
Abstract
Introduction
The Covid-19 pandemic required rapid substitution of in-person Pain Management Programmes (PMP) delivery with delivery via videoconferencing technologies (VCT). No prior published VCT-PMP effectiveness findings were found, so an evaluation was conducted to explore effectiveness of this method and to compare psychometric outcomes with pre-pandemic, in-person- PMPs, delivered in routine clinical settings.
Methods
Participants were routinely attending PMPs. A consecutive series of six in-person-PMPs (n = 61) immediately prior to the pandemic were compared with the first series of six VCT-PMPs (n = 64) delivered in the same services. A within-subjects comparison of clinical outcomes (pre-post for VCT-PMP and in-person PMP) and a between-subjects comparison of delivery type was conducted (two-way mixed ANOVA). Reliable change indices examined reliable improvements and deteriorations by delivery type.
Results
Both PMP delivery format groups made significant improvements in anxiety, depression, pain self-efficacy, chronic pain acceptance and pain catastrophising. No significant difference was found between VCT-PMP and in-person-PMP on each of the measures. Reliable change indices indicated similar levels of improvement and deterioration with each delivery format with improvements far outweighing deteriorations. Attrition was greater in the VCT format (33%) versus in-person-PMP (18%).
Conclusion
This study indicates that meaningful change as measured by standard psychometric questionnaires can occur in PMPs delivered via VCT and appear broadly equivalent to that achieved through in-person delivery. Physical performance outcomes such as quality and amount of movement were not measured or explored.
Keywords
Introduction
The Covid-19 pandemic meant that face-to-face group-based interventions were an infection transmission risk. Pain services underwent rapid transformation to adapt their Pain Management Programmes (PMPs) for Video Conference Technology delivery (VCT). In-person PMPs have been widely studied, typically reporting small to moderate effect sizes for treatment outcomes in various quality of life domains. 1 More specifically, studies of Acceptance and Commitment Therapy (ACT) PMPs, have also been shown to yield outcomes improving factors such as pain-related disability, anxiety and depression. 2 Increasingly, internet-based behavioural interventions for chronic pain, including Cognitive Behaviour Therapy (CBT) and ACT have been developed. These include internet-based instruction in behaviour change methods with or without the support of a therapist. They show some promise in reducing catastrophising and pain interference and disability as examples. 3 However, these methods do not yet appear to have included VCT-delivery of a multi-disciplinary PMP. A rapid review published in 2020 found no studies examining VCT-PMP effectiveness 4 and a further literature search by the authors of this study found nothing further prior to conducting this study.
PMPs are typically multi-disciplinary and psychologically based interventions. Therefore, the literature was then searched for precedent around VCT-group-based psychological interventions. Again, surprisingly little was found. One study used VCT to deliver group therapy to military veterans for Post-Traumatic Stress Disorder (PTSD) and anger management. 5 In both conditions, group members attended the session together in-person. However, there were treatment arms with the therapist attending via VCT versus in-person. Both treatment modalities were effective in reducing anger scores. A Cochrane review 6 of interactive telemedicine included a subset of studies evaluating VCT-delivery effectiveness. Many of the reported studies comprised chronic condition monitoring and outcomes were mainly focused on physiological measures. However, a subset of seven studies included psychological interventions designed to enhance mental health outcomes (e.g., CBT for bulimia, counselling for substance misuse, anger management therapy, Post-Traumatic Stress Disorder coping skills). VCT and in-person were of equivalent effectiveness.
More specifically, the literature search for individual psychological therapy delivered using VCT yielded two notable systematic reviews. One examined the effectiveness of one-to-one VCT-CBT and behavioural activation (BA) for depression 7 and the other for VCT-CBT for anxiety. 8 Both reviews excluded studies where psychotherapy was in conjunction with treatment for chronic pain. Twenty-one of 33 studies reported statistically significant improvements in depression with median effect sizes ranging from medium to very large. 7 14 of 21 studies found statistically significant improvements in anxiety and 11 reported clinically significant improvements. Anxiety reduction effect sizes ranged from small to very large. 8 Most controlled studies showed no statistically significant difference between VCT and in-person for depression 7 and all seven controlled studies found no difference between VCT and in-person for anxiety. 8
This evaluation was conducted due to the aforementioned gap in the literature around effectiveness for VCT-PMP at a time when it was unsafe for patients to access in-person groups. It was imperative to ensure that the intervention was not causing harm in a group of patients who may be vulnerable due to their complex biopsychosocial needs, already exacerbated by the stress of the pandemic. Prior to working with VCT, clinicians reported concerns about the effectiveness of VCT as a modality for PMP delivery. These particularly focused around reduced ability to detect non-verbal cues of participants, group cohesion and the challenges of using technology to interact, in addition to the demands of clinical delivery. Determining that meaningful positive change could be effected via VCT-PMP, was also necessary to support clinician morale and guide future service delivery decisions as the pandemic unfolded. To provide a finer grained analysis of both improvement and possible harm (deterioration), Reliable Change Indices were also examined alongside parametric statistics. The evaluation aimed to answer two main questions:
Can VCT-PMP lead to improved clinical outcomes (increases in pain self-efficacy and acceptance of pain and reductions in pain catastrophising, anxiety and depression)?
Are VCT-PMP and in-person PMPs equivalent in clinical outcomes (increases in pain self-efficacy and acceptance of pain and reductions in pain catastrophising, anxiety and depression)?
Methods
The study was conducted after local institutional approval had been gained (reference number SE-0369).
Design
The design employed a within-subjects pre-post comparison for outcome of attending a PMP and a between-groups comparison for comparison of the two modalities, VCT versus in-person.
Intervention content
The PMPs use ACT as their therapeutic model and are co-delivered by clinical and counselling psychologists, senior CBT therapists, clinical specialist physiotherapists and nurses, with support from assistant psychologists and an exercise rehabilitation instructor. All clinicians are trained and experienced in using ACT. PMP sessions comprise pain education, activity management, mindfulness skills (defusion, acceptance, contact with the present moment, observer self), values-based goal setting, movement and exercise. The aim is to improve patient quality of life alongside pain and empowerment in self-management of chronic pain.
The VCT course covered the same topics as the in-person course but adapted for VCT-delivery. VCT adaptations comprised increased provision of powerpoint slides covering key concepts. In-person sessions relied more on live or pre-prepared write-up of content on interactive whiteboards or flip charts. VCT sessions included video clips from a range of internet sources to illustrate key points and provide variety. Interactive group discussions on VCT were captured using the whiteboard function or by screen sharing of power point slides created live in response to group generated content. The equivalent was captured on in-person-PMP using flip charts or interactive whiteboards. Virtual breakout rooms were used for small group discussions.
Depending on in-person-PMP delivery setting, some groups had access to gym equipment, whereas others in community room settings had none. All groups included regular stretch and gentle movement practices such as Tai Chi. The VCT-groups comprised physiotherapist or exercise rehabilitation instructor led movement and stretch practices similar to in-person-PMPs but no live gym-based or live equipment-based exercise. VCT sessions were adapted with the movement instructor requiring sufficient space and set up of camera angle to enable full body view. Similarly, participants were instructed in the optimal positioning of their camera for movement sessions (included in the VCT orientation session described below) and were required to keep their cameras on for safety and movement monitoring reasons.
An additional 2-hour session was offered to VCT participants to enable orientation to the group experience on the VCT platform. This included some ice breaking exercises and an opportunity to explore VCT-group etiquette (e.g., use of camera functions, mute/unmute), practical aspects such as how to set your room up to enable movement practise and use of breakout rooms for small group work.
The same programme manual was provided to VCT and in-person-PMP participants. In the VCT condition this was posted or emailed according to participant preference. The manual covers all aspects of the course and exercises and practices discussed on the course. For both conditions, supporting weblinks to other resources including mindfulness audio recordings were provided.
Intervention duration
Out of the six PMPs in each arm (VCT and in-person), five were 9-week programmes with sessions lasting 2.5 h and one was a 10-week programme with sessions lasting 2.5 h. These differences were due to differing service specifications with the 10-weeks programme including a medication session.
Measures
Patients routinely complete a battery of standardised self-report questionnaires prior to attending PMP (normally within 2 weeks of commencement) and again at the end of the weekly course. The seven-item Generalised Anxiety Disorder-7 (GAD-7) questionnaire screens for anxiety. 9 The nine-item Patient Health Questionnaire-9 (PHQ-9) screens for depression. 10 The Pain Self-Efficacy Questionnaire (PSEQ), assesses patients’ confidence in managing different aspects of their life despite pain. 11 The Pain Catastrophising Scale (PCS), measures the extent to which patients worry about and fear their pain. 12 The Chronic Pain Acceptance Questionnaire (CPAQ), 13 measures activity engagement (engagement in life activities despite being in pain) and pain willingness (awareness that avoidance and control can be unhelpful in adapting to chronic pain). All the measures employed have excellent or good internal consistency and test-retest reliability 9,10,14–16 and are widely used as outcome measures in chronic pain services.
Objective physical outcome measures were not taken during the VCT-PMP and are therefore not reported.
Participants
Means, standard deviation (SD) and effect sizes for the questionnaires pre- and post-VTC-PMP and in-person-PMP.
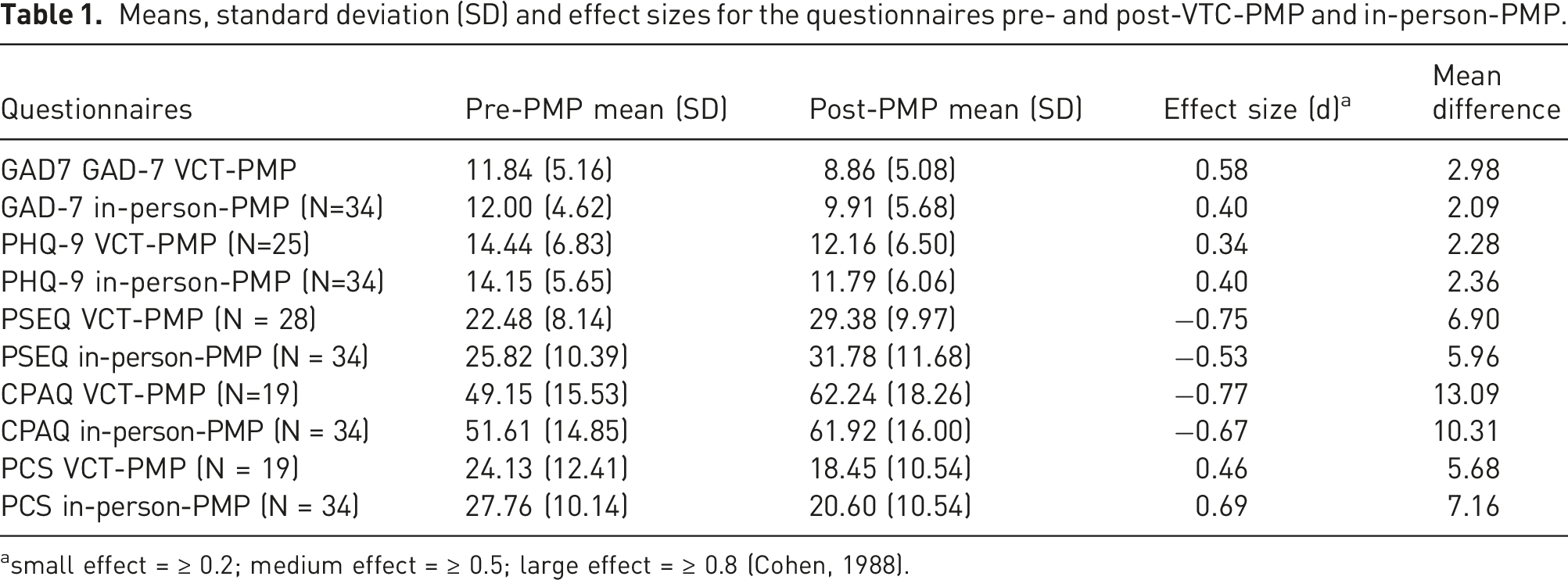
small effect = ≥ 0.2; medium effect = ≥ 0.5; large effect = ≥ 0.8 (Cohen, 1988).
The in-person-PMP data sample was drawn from a database of PMPs that took place prior to the pandemic. The most recent, consecutively run, 6 in-person-PMPs were examined in order that course content and staff delivering might be as closely matched as possible to that of the VCT-PMP. Of these groups, 61 participants started a programme and 50 (82%) completed a programme (defined as attendance at 7 or more sessions). Of those who completed a programme 35 (70%) patients completed questionnaires at both pre- and post-programme and were included in the analyses. Table 1 includes the number of participants whose data was complete by questionnaire. The average age was 48 (SD, 16.86) with a range of 21–78 years. Thirty were female (88.2%) and 4 were male (11.8%). The primary sites of pain were classified as follows: widespread pain (50%), back (41.2%), head/face (2.9%), lower limb (2.9%) and abdomen (2.9%). The duration of pain was recorded as follows: 1–5 years (41%), 5–10 years (24%), more than 10 years (35%).
Service inclusion and exclusion criteria for attendance on either PMP type were as follows:
Inclusion criteria: – English speaker – Unremitting, non-malignant pain. – No indication for further medical investigations or treatment – There is significant disruption of lifestyle where chronic pain is the primary diagnosis, of ≥6 months duration, including: – Widespread disruption of daily activities – Interference with ability to work – Habitual under/over-activity resulting in frequent flare-ups – Excessive medication without adequate effect – Distressed by pain – Extensive de-conditioning – Sleep disturbance – Poor understanding of chronic pain – Wishing to learn about self-management
Exclusion criteria: – If a severe intractable mental health condition is interfering with ability to cope with pain and/or programme demands. – Substance misuse history and an ongoing issue with opioids – Functional disorder with a high symptom load such as dizziness, falls, fits or vomiting, and pain is just one of the symptoms treatment is sought for
At the time when the VCT-PMPs were run, there were no in-person-PMPs offered in the service. For those who declined or could not access this format, in-person or telephone 1:1s were made available as appropriate, or the individuals were discharged back to their GP to avoid indefinite unsupported waiting times. Where digital access (e.g., lack of wifi access or unavailability of digital devices) was the barrier to attendance, a separate work stream was set up to source wifi-enabled devices for loan. Individuals supported in this manner do not feature in this cohort as this offer was not instantly available.
Procedure
Questionnaires were posted or emailed to participants according to preference prior to attendance on either type of PMP (normally within 2 weeks prior to commencement). Participants then attended either a VCT-PMP or in-person-PMP. Questionnaires were re-administered via post or email in the week prior to the final VCT-PMP session or were handed out for completion during the final in-person-PMP session.
Data analysis
All data were pseudonymised for purposes of database creation and analysis. Data were analysed using SPSS and Excel. Descriptive statistics and effect sizes (Cohen’s d) were calculated. A two-way mixed analysis of variance (ANOVA) was run to examine pre- to post-PMP change (within-subjects factor) in each condition and to compare the effectiveness of VCT-PMP with in-person-PMP (between-subjects factor).
Reliable change indices were calculated to determine the number of participants who met criteria for reliable change (improvements and deteriorations) following treatment using the Leeds RCI calculator. 17
Information was also drawn from patient systems records on attendance and attrition for the PMPs.
Results
Table 1 displays the mean (SD) questionnaire scores for patients who completed both pre- and post-PMP outcome measures for the VCT-PMP and in-person delivery conditions together with effect sizes.
A two-way ANOVA (mixed) was conducted for each questionnaire. The results of the ANOVAs showed the same patterns across all questionnaires, with a significant main effect of time (pre-post) on questionnaire scores which were as follows: GAD-7, F (1, 57) = 15.860, p < .05; PHQ-9, F (1, 57) = 13.146, p < .05; PSEQ, F (1, 60) = 29.258, p < .05; CPAQ, F (1, 51) = 24.968, p < .05 and PCS, F(1, 51) = 18.439, p < .05. Post-PMP scores were significantly improved from pre-PMP scores.
There was no significant main effect of PMP delivery format: GAD-7, F (1, 57) = 0.255, p > .05; PHQ-9, F (1, 57) = 0.048, p > .05; PSEQ, F (1, 60) = 1.531, p > .05; CPAQ, F (1, 51) = 0.073, p > .05, PCS, F (1, 51) = 1.059, p > .05. Furthermore, the interaction between time (pre-post) and treatment modality was not statistically significant across all the questionnaires: GAD-7, F (1, 57) = 0.491, p > .05; PHQ-9, F (1, 57) = 0.003, p > .05, PSEQ, F (1, 60) = 0.156, p > .05; PCS, F(1, 51) = 0.245, p > .05 and CPAQ, F (1, 51) = 0.351, p > .05 indicating that the VCT and in-person delivery had equivalent effectiveness on these outcome measures.
Given the novelty of VCT delivery reliable change indices were also calculated for a finer grained understanding of the effects of treatment including possible deteriorations. 18 We were unable to assess clinically significant change (CSC) due to an absence of benchmarks reported in the literature for CSC on the outcome measures used.
To calculate reliable change, we used the definition which states that following treatment, if the participant’s mean is closer to that of the “functional” population than the “dysfunctional" population, then a reliable improvement has happened. 18 Published reliable change values were not found for the PSEQ, CPAQ and PCS questionnaires. Therefore, we used Criterion A on the Leeds RCI calculator which uses Cronbach’s alpha as a reliability measure, and were found from several large studies as follows: PSEQ = 0.94, 11 CPAQ = 0.90, 15 and PCS = 0.87. 16 Previous research had proposed reliable change values of 4 and 9 for the GAD-7 and PHQ-9 questionnaires 19 and test-retest reliability values of 0.83. 9 and 0.84, 10 respectively. These were used for GAD-7 and PHQ-9 analyses.
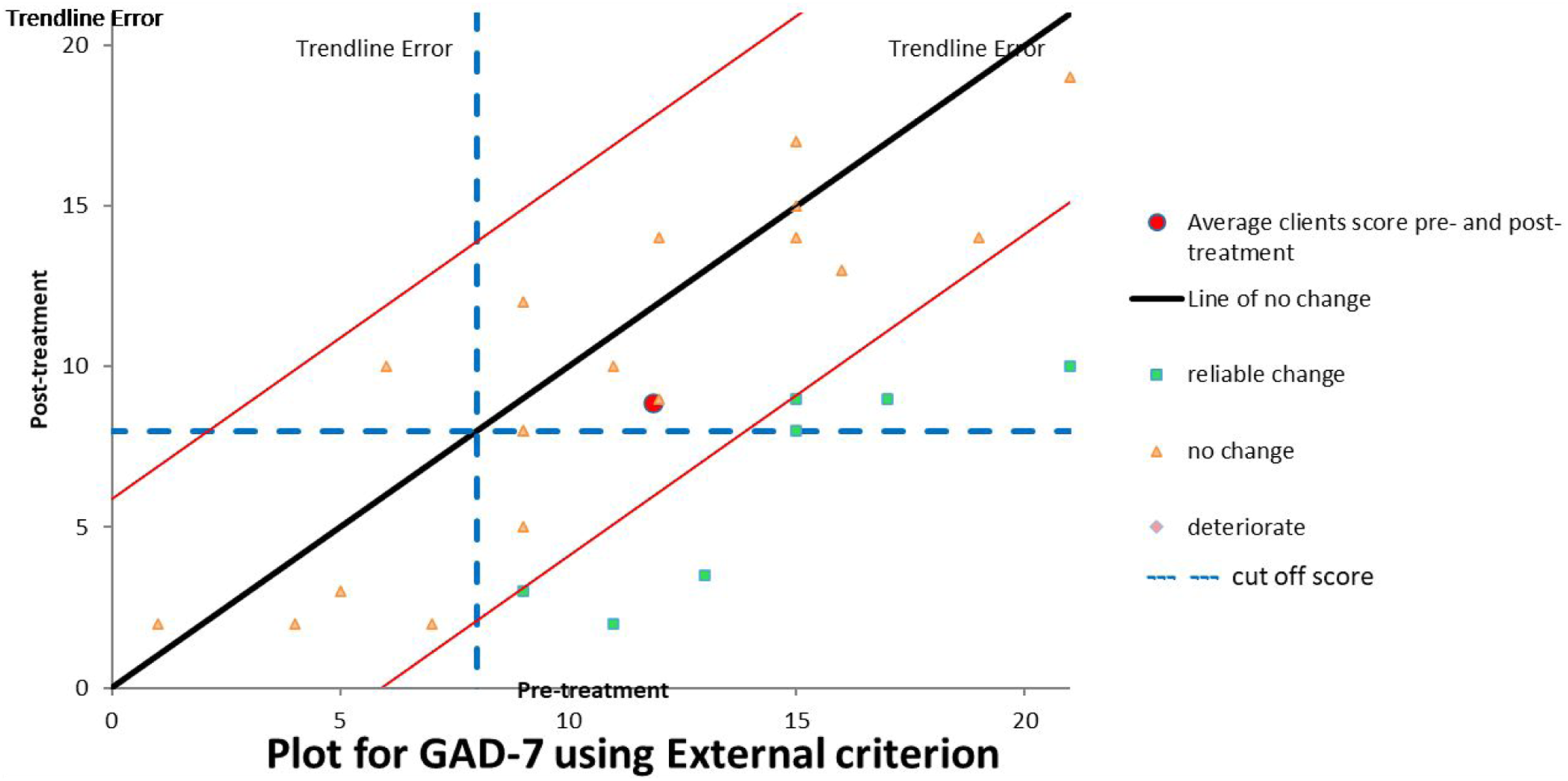
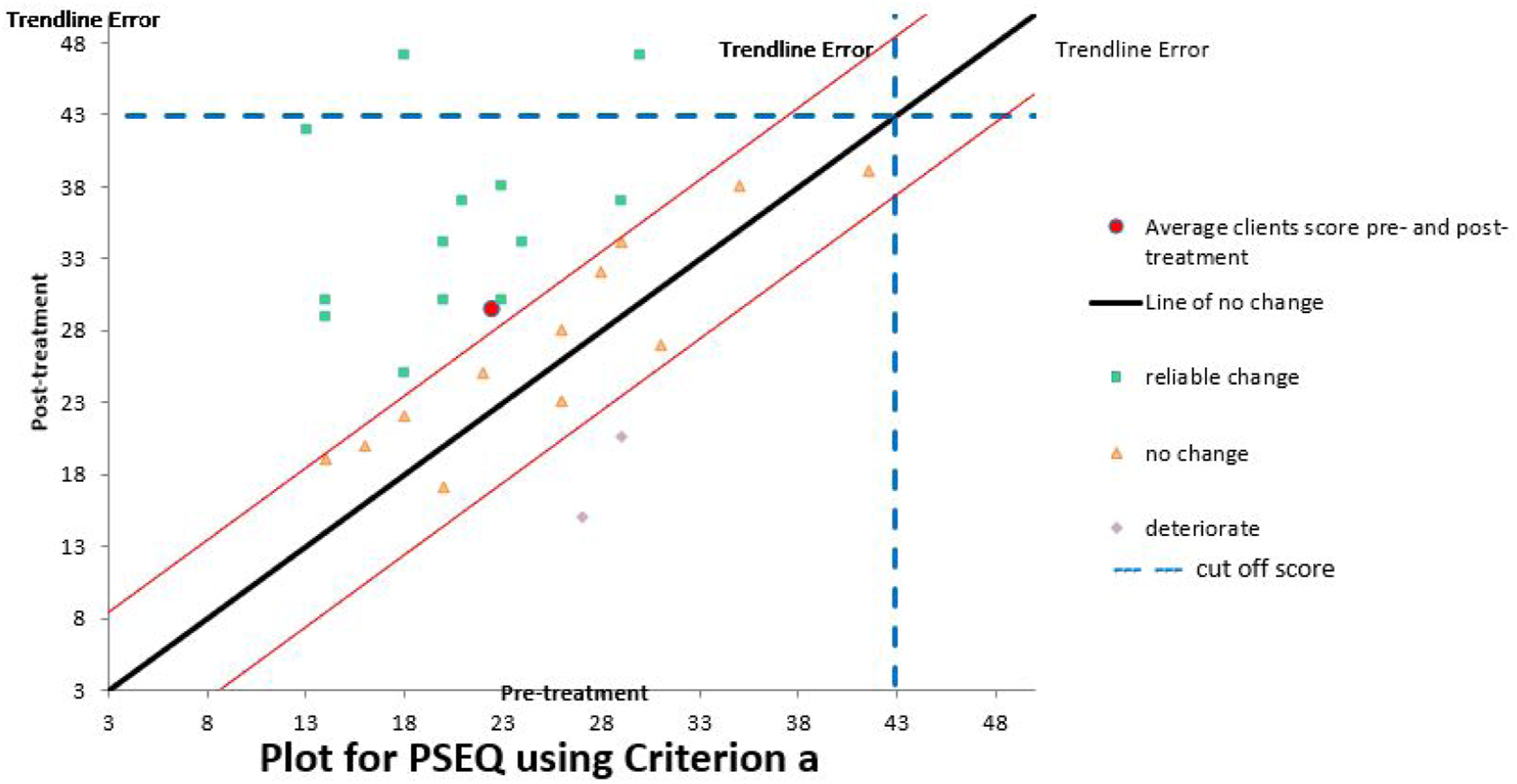
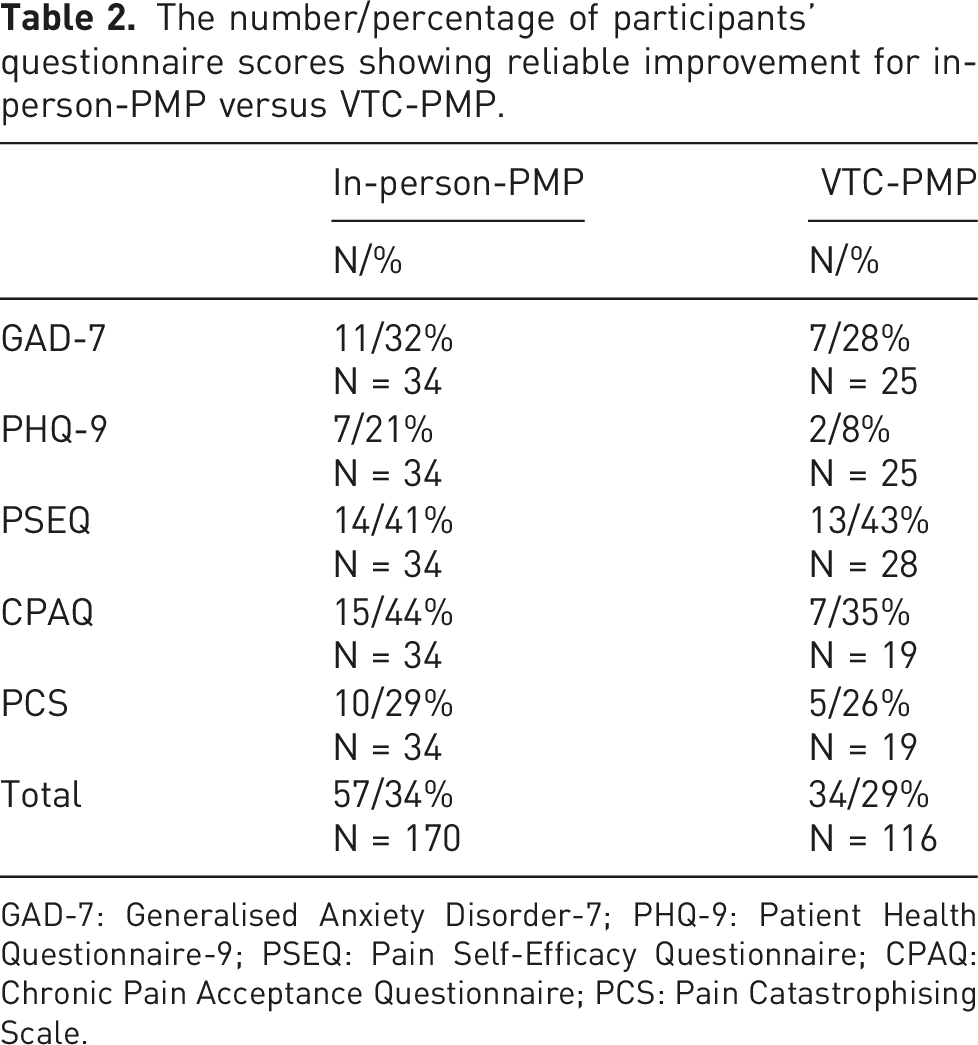
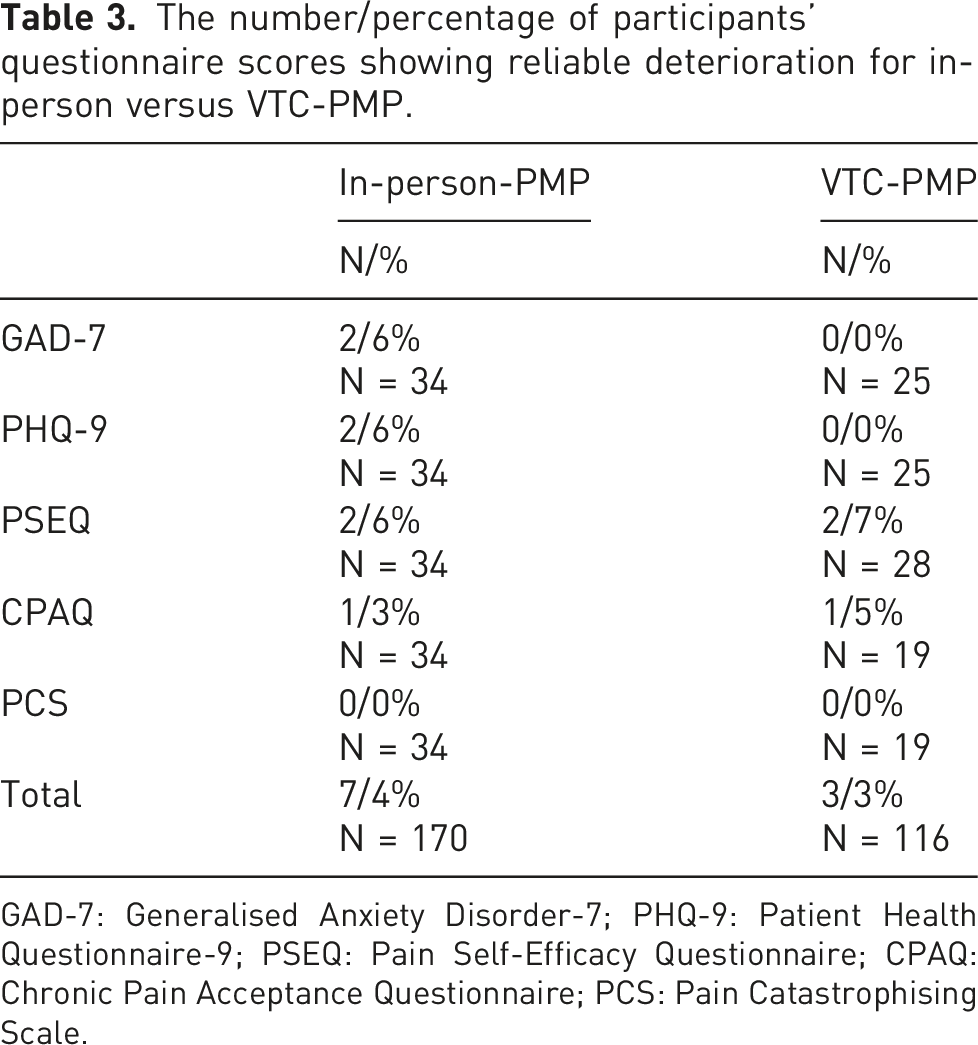
For purposes of illustration scatter plots are displayed for the VCT condition for PHQ-9, GAD-7 and PSEQ (Figures 1–3). The graphs depict the number of participants who showed no change, reliable improvement and reliable deterioration. Table 2 summarises the RCI (improvement) for each outcome measure by treatment modality. Table 3 summarises the RCI (deterioration) for each outcome measure by treatment modality. The Leeds RCI tool
17
was used to compute these graphs and tables. Scatter plot of participants’ pre- and post- VTC-PMP PHQ-9 scores. Scatter plot of participants’ pre- and post- VTC-PMP GAD7 scores. Scatter plot of participants’ pre- and post- VTC-PMP PSEQ scores. The number/percentage of participants’ questionnaire scores showing reliable improvement for in-person-PMP versus VTC-PMP. GAD-7: Generalised Anxiety Disorder-7; PHQ-9: Patient Health Questionnaire-9; PSEQ: Pain Self-Efficacy Questionnaire; CPAQ: Chronic Pain Acceptance Questionnaire; PCS: Pain Catastrophising Scale. The number/percentage of participants’ questionnaire scores showing reliable deterioration for in-person versus VTC-PMP. GAD-7: Generalised Anxiety Disorder-7; PHQ-9: Patient Health Questionnaire-9; PSEQ: Pain Self-Efficacy Questionnaire; CPAQ: Chronic Pain Acceptance Questionnaire; PCS: Pain Catastrophising Scale.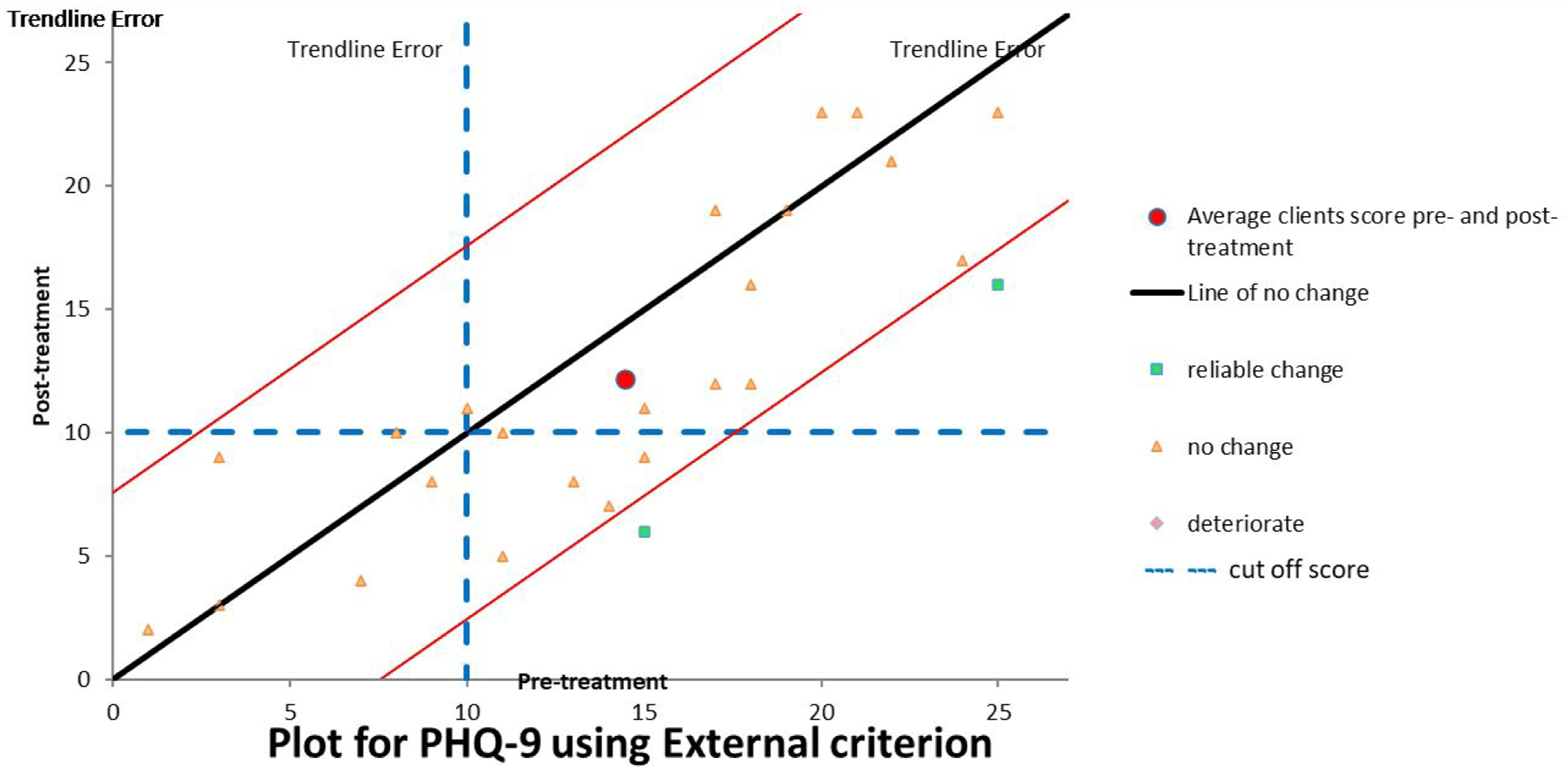
Attrition was greater for VCT-PMP (33%) than in-person (18%). However, the percentage of complete data sets received out of the possible number of treatment completers was similar across each condition (VCT, 65% versus in-person, 70%).
Discussion
This study indicates that of those PMP participants who completed outcome measures both prior to and after PMP, there were statistically significant improvements across all outcome measures, irrespective of treatment modality (VCT or in-person). The majority of these changes produced moderate effect sizes with the remainder being small (Cohen’s d). These effect sizes were in line with existing literature on in-person PMP effectiveness.1,2 Reliable change indices 18 provided finer grained detail with a minimum of 15 (44%) in-person participants achieving reliable improvement on at least one measure (CPAQ) and a minimum of 13 (43%) VCT-participants achieving this on at least one measure (PSEQ). There was also some reliable deterioration noted with a likely minimum of 2 (6%) in-person participants experiencing this on at least one measure (GAD, PHQ-9, PSEQ) and a minimum of 2 (7%) participants in the VCT condition on at least one measure (PSEQ). Visual inspection of the reliable improvement and deterioration data suggests that in-person and VCT were broadly equivalent.
These findings are clinically relevant as they provide initial reassurance about the effectiveness of VCT-PMP. Pre-post intervention psychometric questionnaire score differences were comparable with our in-person data. In addition, reliable deterioration was relatively low (and outweighed by improvements) in both conditions. We were unable to formally evaluate clinically significant change in the present study due to the lack of published minimal clinically important difference (MCID) values derived from mixed chronic pain samples, for the psychometric questionnaires used in this study. However, two studies of the PSEQ in people with low back pain suggest a change of greater than 5.5 20 or 8.5 21 points constitutes a MCID. The mean pre-post pain score difference was 5.96 and 6.90 for in-person and VCT groups respectively in the present study. These mean values alone exceed the suggested MCID of 5.5 recommended by one study. 20 Additionally, visual inspection of the Reliable Change graphs reassures that scores recorded by several participants in each condition exceeded one or both of these MCID values on the PSEQ. VCT appears to be a viable and effective delivery modality for PMP. This creates potential to increase patient choice and improve PMP accessibility for patients who find it difficult to access in-person PMPs or where infection prevention is paramount.
Study limitations
This is a real-life clinical evaluation with no opportunity to apply the standardisation and bias-reduction processes that would be seen in a randomised controlled trial. In the present study, the VCT condition was inextricably linked to living through the first winter of the Covid-19 pandemic with chronic pain. The in-person groups took place prior to the pandemic. Thus, the remote delivery versus in-person is not the only treatment context difference. Furthermore, groups were not matched on variables such as pain location, duration or initial distress severity. Instead, the decision was taken to study consecutive in-person groups run immediately prior to lockdown compared with the VCT-PMPs first run by the service during the legally enforced social distancing stage of the Covid-19 pandemic. This was an attempt to maximise the chance that the same staff members were delivering the programmes and that the content delivered in VCT and in-person was similar, as content tends to evolve over time as clinicians refine their approaches.
The small sample size (28 patients for VCT-PMP and 35 for in-person-PMP) is a significant limitation and results should be interpreted cautiously as preliminary indicators of effectiveness. Further research is needed, for example, randomised controlled trials on larger samples with both treatment arms delivered outside of the acute stages of a pandemic. The lack of follow-up is also a weakness, providing no information on maintenance or loss of gains for either group and whether these differ between modalities. Finally, both the VCT and the in-person-PMP data were heavily biased towards female membership (75% and 88%, respectively) reducing sample representativeness.
Attrition was greater for VCT-PMP (33%) versus in-person (18%). However, the percentage of complete data sets received out of the possible number of treatment completers was similar across each condition (VCT, 65% versus in-person 70%). The higher dropout in the VCT-PMP is of concern and could be indicative of a less acceptable treatment. A recent qualitative study found acceptability of remotely delivered PMPs varied across patients. 22 Thus, for some, acceptability was linked to being able to receive high quality care from home, improved treatment accessibility, overcoming social distancing requirements and virtual peer support. Those who found this format less acceptable cited an unsuitable home environment for remote therapy, communication difficulties with the virtual format and technological problems and concern that care was lower quality. The reasons for dropout were not explored in this sample. Past efforts by this service to understand reasons for dropout from in-person PMPs have met with extremely low response rates. Nonetheless, it would be of value to seek feedback from those who dropout in future.
The questionnaire return rates at the end of both in-person and VCT-PMP meant that approximately one third of treatment completers did not provide outcome data. The service does its best to remind patients and provide time within the final session for questionnaire completion. Factors that impede questionnaire return include participants not attending the final in-person or VCT-PMP session (although they may have attended 7 sessions or more) and therefore not having this protected time. Even with protected time on PMP some participants do not wish to complete all measures in one sitting, and we are reliant on them returning them later. These are participant choices and behaviours which are difficult to influence.
Other than the difference in attrition rates between the two conditions, the patient outcomes seem broadly equivalent. The measures used target psychological aspects. No direct assessment of outcomes such as movement, exercise and quality of movement were made and therefore participant progress in these areas is not reported and is a further limitation.
Advantages and disadvantages of VCT-PMP versus in-person-PMP
There are a mixture of advantages and disadvantages to each delivery modality. VCT-PMP improves accessibility and comfort for some (caring responsibilities, cost of and/or ability to travel, reduced time pressures, health problems, anxiety), 22 but not others (digital poverty and/or illiteracy, conditions making use of screens difficult or impossible). 23 For others, the home environment may provide more, or different, distractions compared to an in-person environment and may lack the privacy needed for open discussions about an individual’s psychological state. 22 In-person PMP may be more conducive to group cohesion and networking amongst participants compared to VCT as has been shown in other psychologically based interventions. 24 Finally, VCT-PMP provides a safe option for intervention delivery in conditions where meeting as a group is unsafe, either for the individual (e.g., the immunocompromised) or more generally (e.g., in a pandemic).
From our service perspective, VCT-PMP arguably required more administrative efforts (e.g., sending and return of programme materials and outcome measures), but less clinician time (reduced travel, room set up, etc). Reduced travel also decreases service and staff costs as well as carbon footprint. Due to variations in our treatment facilities, VCT-PMP allowed for increased options for audiovisual content (e.g., use of short films/cartoons, etc), but fewer options for supervised movement practice (e.g., no access to exercise equipment and reduced opportunity for tailored, discrete feedback). VCT-PMP format made it easier to coordinate the attendance of our patient volunteers.
Clinically, it can be argued that VCT-PMP provides less opportunity to modify and reduce safety-seeking and other avoidance behaviours that are common in this patient group. 25 Speculatively, in-person group attendance may provide greater opportunity to reduce avoidance and build confidence in areas such as travelling, leaving the house on a regular basis, interacting with others in real-life and exploring idiosyncratic barriers to normal movement.
Future research
Future research would benefit from exploring treatment effectiveness of VCT-PMP compared to in-person PMP in a randomised controlled trial outside of a pandemic to clarify whether the findings reported here are robust. Rigorous exploration of patient experience would also help guide clinical decisions made in collaboration with patients around the most suitable format for that individual. Model-based research into the reduction of avoidance versus approach behaviours in each PMP modality would be of value in understanding the relative clinical impact of interventions in each modality on individuals presenting with high levels of avoidance. Staff experience would also be usefully examined to enable enhanced quality of delivery and to identify areas where staff may need more support to deliver interventions in an alternative evidence-based format. Finally, exploration of the reasons for attrition in either format could also provide important feedback to develop accessible and acceptable intervention offers.
Conclusions
This real-life clinical service evaluation comparing VCT with in-person-PMP provided some reassurance of the comparable effectiveness of each approach in relation to improving patient outcomes in areas of anxiety, depression, pain self-efficacy, pain catastrophising and acceptance of pain. It also provided reassurance that VCT-PMP did not appear to be more harmful than in-person-PMP as deterioration was small and comparable to that found in the treatment-as-usual in-person PMP. This is a small-scale service evaluation and the comparison of VCT with in-person PMP needs further replication and improvements using more robust methodologies such as randomised controlled trials and post-intervention participant follow-up over time. Future research might also begin to tease out which clinical presentations are most appropriate for which modality, for example, whether working with entrenched or more severe levels of avoidance that are forming barriers to improved health and wellbeing is more effective in an in-person setting. Finally, further examination of patient and staff experience may also shape our understanding of which modality is most suitable for whom.
Footnotes
Acknowledgements
We would like to thank The Solent NHS Trust pain teams and Mark Heywood, Samuel Pidduck and Lauren Noya for their contributions to this service evaluation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contribution
DJ reviewed literature and planned the service evaluation. AC conducted the data analysis and write-up with contribution from DJ. DJ wrote and completed all drafts and revisions to the manuscript.
Ethical approval
The project was submitted for review as a service evaluation of a necessary clinical development to Solent NHS Trust’s Clinical Effectiveness and Improvement department where it was approved (reference number SE-0369), and further ethical approval was not deemed necessary.
Informed consent
Consent to use outcome measure data for purposes such as service evaluation is already routinely obtained as a part of the routine administration of these questionnaires. This is gained via an information sheet on the front of the PMP patient questionnaire pack. It is also routinely reinforced verbally by clinicians. Returned and completed questionnaires were taken as consent for the information to be used for the purposes described.
Trial registration
N/A
Guarantor
DJ