
Abstract
Background
The dorsolateral prefrontal cortex (DLPFC) has been implicated in the modulation of pain-related signals. Given this involvement, manipulation of the DLPFC through transcranial direct current stimulation (tDCS) may influence internal pain modulation and decrease pain sensitivity. Acute stress is also thought to affect pain, with increased pain sensitivity observed following the presentation of an acute stressor.
Methods
A total of 40 healthy adults (50% male), ranging in age from 19 to 28 years (M = 22.13, SD = 1.92), were randomly allocated to one of two stimulation conditions (active and sham). High-definition tDCS (HD-tDCS) was applied for 10 min at 2 mA, with the anode placed over the left DLPFC. Stress was induced after HD-tDCS administration using a modified version of the Trier Social Stress Test. Pain modulation and sensitivity were assessed through the conditioned pain modulation paradigm and pressure pain threshold measurements, respectively.
Results
Compared to sham stimulation, active stimulation produced a significant increase in pain modulation capacity. No significant change in pain sensitivity and stress-induced hyperalgesia was observed following active tDCS.
Conclusion
This research shows novel evidence that anodal HD-tDCS over the DLPFC significantly enhances pain modulation. However, HD-tDCS had no effect on pain sensitivity or stress-induced hyperalgesia. The observed effect on pain modulation after a single dose of HD-tDCS over the DLPFC is a novel finding that informs further research into the utility of HD-tDCS in the treatment of chronic pain by presenting the DLPFC as an alternative target site for tDCS-induced analgesia.
Keywords
Introduction
The experience of pain is affected by a range of biological, psychological, and social factors. 1 One well-established moderator of pain is stress,2,3 a psychophysical response to a real, or potential, threat.4,5 The interrelationship between stress and pain is evident in the high worldwide prevalence of comorbid pain- and stress-related disorders. 6 Stress has been shown, for example, to exacerbate symptoms in various chronic pain conditions including headache,7,8 migraine,8,9 fibromyalgia,10,11 and irritable bowel syndrome. 12 In addition to this comorbidity relationship, experimental methods have also shown a relationship between stress and pain. Specifically, conditioned pain modulation (CPM), an experimental measure of the balance of endogenous pain inhibition and facilitation, 13 is reduced in chronic pain 14 and healthy3,14–17 participants following induced acute stress. Further, perceived stress levels appear to correlate with both pre- and post-stress pain sensitivity and modulation. 15 Taken together, these findings suggest that exposure to an acute stressor may increase pain sensitivity through the disruption of endogenous pain modulation. 6
An intervention that has proved successful in enhancing pain modulatory processes18–21 and reducing physiological and psychological stress responses 22 is transcranial direct current stimulation (tDCS). While the analgesic effects of tDCS have been most widely reported following stimulation of the primary motor cortex, 23 the dorsolateral prefrontal cortex (DLPFC) has been investigated as a potential alternative target. Prefrontal regions have been implicated in the processing of emotional aspects of pain and are thought to be part of corticosubcortical and corticocortical pain modulatory networks. 24 The involvement of the DLPFC in pain processing and modulation suggests that stimulation of this region using tDCS may enhance the efficacy of endogenous pain modulatory responses and reduce stress-induced hyperalgesia. However, to-date, the effects of tDCS over the DLPFC on endogenous pain modulation and stress-induced hyperalgesia have not been investigated.
The current study aims to assess the effects of anodal tDCS over the left DLPFC on pain sensitivity, endogenous pain modulation and stress-induced hyperalgesia. In relation to this aim, we have three primary hypotheses. First, it is hypothesised that active tDCS over the DLPFC will enhance endogenous pain modulatory capacity, demonstrated by increased CPM following active compared to sham tDCS. Second, it is hypothesised that active tDCS will reduce pain sensitivity when compared to sham stimulation. Third, it is hypothesised that active tDCS will decrease stress-induced hyperalgesia, as assessed through changes in pressure pain threshold (PPT) and CPM.
Materials and methods
Design
This study followed a single-blinded, sham-controlled experimental design, with participants attending a single laboratory session and randomly assigned to one of two experimental conditions (active condition and sham condition). Participants were not informed of the stimulation condition that they were assigned; however, researchers were aware of each participant’s assigned condition. The study protocol was approved by the University of Canberra Human Research Ethics Committee (Project Number: 8087) and was conducted in adherence to the standards set by the Declaration of Helsinki.
Participants
Healthy adults aged between 18 and 40 years were recruited. Due to the known influences of age on pain modulation 25 and pain sensitivity,26–28 those younger than 18 and older than 40 years were excluded. Similarly, individuals were excluded if they suffered from a diagnosed psychological disorder, had chronic or acute pain, were currently taking psychoactive medications, had a history of seizures/stroke, had had a serious head injury, had a neurological illness that may have caused brain injury, had metal implants, experienced loss of consciousness, experienced migraines/severe headaches, were pregnant, and had consumed caffeine or alcohol in the past 24 h. These exclusions refer to potential influences on pain modulation and the safety of tDCS.14,29,30
The final sample included 40 healthy adults. This sample ranged in age from 19 to 28 years (M = 22.13, SD = 1.92) and included 20 males (50%) and 20 females (50%).
Materials and measures
Perceived stress
Participants’ perceived stress levels were assessed using a 0–100 stress numerical rating scale (SNRS) with descriptive anchors at 0 (not at all stressed) and 100 (overwhelmingly stressed). The SNRS requires participants to respond verbally to a single question: ‘Can you please indicate on a scale from 0 to 100, with 0 being not stressed at all and 100 being overwhelmingly stressed, how stressed are you feeling at this moment?’ This measure has been shown to allow for valid, reliable, and timely assessment of subjective stress levels within experimental settings.31–34
Depression, anxiety, and stress
To assess whether participants’ psychological states differed significantly across tDCS conditions, baseline mood and stress was assessed using the Depression, Anxiety, and Stress Scale (DASS). 35 The DASS is a 42-item self-report questionnaire that measures an individual’s negative emotional states of depression, anxiety, and stress. The DASS has demonstrated good to excellent reliability within non-clinical samples, with a Cronbach’s alpha (α) of 0.91 for depression, 0.84 for anxiety, and 0.90 for stress subscales. 35 In the present study, the DASS similarly demonstrated excellent reliability, with Cronbach’s α = 0.96, 0.85, and 0.91, for depression, anxiety, and stress subscales respectively.
Stress induction protocol
To induce acute psychosocial stress, a modified version of the Trier Social Stress Test (TSST) 36 was employed. Unlike the standard TSST, which consists of a 10-minute preparation phase, followed by a five-minute speech presentation phase and a five-minute surprise mental arithmetic task,36,37 this modified version of the TSST consisted only of the speech preparation phase.3,38 Participants were taken to a separate room at the beginning of the stress induction protocol. They were provided with a notepad and pen and given verbal instructions adapted from Birkett. 37 Participants were then given an opportunity to ask questions or voice concerns before being left alone for 10 min to prepare for the speech presentation. After 10 min, participants were brought back into the laboratory and asked to stand in front of a desk behind which the two researchers were seated, ready to listen to the prepared speech. Participants were then told that they would not be required to perform their speech. This modified version of the TSST was chosen to induce acute psychosocial stress as it is characterised by unpredictability and uncontrollability, characteristics that have been shown to induce robust stress responses in humans.39–41
Pain measurement
Pain sensitivity
Pain sensitivity was assessed through pressure pain threshold measures. Participants were instructed to place their left hand flat on a table, with their palm facing down. The researcher then pressed the tip of a handheld algometer (Wagner Force Dial FDK 20, Wagner Instruments, Greenwich, CT) down upon the index finger at a rate of approximately 1 kg/s. Participants were instructed to indicate when the pressure was first perceived as painful. At the onset of pain, pressure was released and PPT was recorded in kilograms of force. Two measurements were taken at the same site, with a 30 s interval separating each. Final PPT scores were calculated as the mean of these two trials. Prior to the first of the two trials, participants were provided with a familiarisation trial on their ring finger. One minute separated the familiarisation trial and the first experimental trial.
Endogenous pain modulation
The CPM protocol was used to assess endogenous pain modulation. This involved a painful test stimulus (TS) being presented before and after a painful conditioning stimulus (CS). This sequential design with the TS presented prior to and immediately after the CS was chosen as it has been shown to be a more valid assessment of endogenous modulatory capacity since it removes the potential for the CS to distract attention from the TS if presented simultaneously. 13 For the TS in the CPM protocol, PPT was used as outlined above. Therefore, PPT measurements were recorded prior to (pre-conditioning PPT) and after the CS (post-conditioning PPT). Pre-conditioning PPTs were used in both the calculation of CPM and as a measure of pain sensitivity.
Cuff occlusion of the participant’s right arm was used as the CS. The use of cuff occlusion as a CS has been supported in previous research.42,43 A sphygmomanometer cuff was positioned around the distal end of the participant’s right bicep brachialis and slowly inflated (approximately 20 mm Hg/s) until the participant reported the onset of pain. Once pain was reported, the researcher stopped inflating the cuff. While at this level of inflation, the participant reported pain intensity based on a visual analogue scale (VAS) with 0 (no pain at all) and 10 (the worst pain imaginable), participants were asked at 10 s intervals to report their pain intensity according to the VAS. If participants reported a decrease in pain or the same pain intensity on two consecutive intervals, the cuff was inflated by approximately 20 mm Hg. Once the participant reported a pain intensity of ‘5’ or higher, the cuff was deflated. Immediately following deflation, post-conditioning PPTs were measured. Pre-conditioning PPT and post-conditioning PPT measurements were used to obtain baseline and post-stimulation CPM scores.
Direct current stimulation
Transcranial direct current stimulation was applied using a 4 × 1 HD-tDCS multi-channel stimulation interface (Model 4X1-C2, Soterix Medical, New York, NY) connected to a conventional 1 × 1 tDCS device (Model 1300, Soterix Medical, New York, NY). High-definition tDCS (HD-tDCS) is a form of tDCS that has been shown to induce more focal stimulation of target regions by using a 4 × 1 ring configuration.44,45 Electrodes were fitted into plastic casings which were secured using an EEG cap. The centre anode electrode was placed in accordance with the International 10/20 EEG system over the F3, which is the approximate location of the left DLPFC. Cathodal electrodes were placed in a ring configuration 2 cm from the centre electrode, at the approximate locations of C3, Fz, Fp1, and F7.
Underneath each electrode, hair was parted to ensure greater contact between the electrodes and scalp. A conductive gel (Signa Gel, Parker Laboratories Inc., Fairfield NJ) was inserted into the plastic casings underlying the electrodes. Impedance values were assessed through the HD-tDCS device to determine sufficient contact quality. If presented with impedance values greater than 1.50 quality units, electrodes were taken out and readjusted.
In the active condition, 2 mA was delivered for 10 min. This protocol is supported by previous applications of tDCS and has been shown to induce changes in underlying brain regions for up to 6 hours.46,47 An automated ramp-up period gradually increased current intensity from 0 mA to 2 mA over 30 s. Following the ramp-up period, 10 min of stimulation occurred with a 30 s ramp-down period gradually decreasing the intensity back to 0 mA.
In the sham condition, the same protocol for electrode placement was employed. However, the 30 s ramp-up period was immediately followed by the 30 s ramp-down period to 0 mA. After 10 min of sham stimulation at 0 mA, a 30 s ramp-up period occurred again, immediately followed by a ramp down. This allowed the participants to experience initial sensations of tDCS such as itchiness, without inducing changes in cortical excitability. 48 This sham protocol has been shown to be effective at blinding participants to their condition. 49
Procedure
Participant recruitment occurred during May 2021. Prior to participation, individuals were instructed to complete appropriate COVID-19 forms to ensure they presented no symptoms of illness and were not close contacts to the virus. Those indicating any symptoms or recent travels to hot-spot areas were excluded from participation. Individuals eligible for participation were directed to wear masks during the experiment. Researchers wore surgical masks and gloves throughout the entirety of experimental sessions.
Before experimental sessions took place, the randomisation of conditions was pre-determined through an online random number generator (Calculator.net). Thus, researchers were aware of the participants’ allocated condition while participants were blinded. Twenty participants were allocated to the active condition (50% male) and 20 participants to the sham condition (50% male).
On arrival, participants were presented with an overview of the experiment and the tasks involved. The exclusion criteria were reassessed and thoroughly described to the participants to ensure eligibility. Written informed consent was then provided after participants clearly understood the experiment.
The experimental protocol began with participants completing the DASS. Upon its completion, participants verbally rated their current level of perceived stress according to the stress-NRS (baseline perceived stress). Participant’s baseline pain sensitivity and pain modulation measurements were then recorded (baseline CPM). This involved PPT measurements before (baseline pre-conditioning PPT) and after the CS (baseline post-conditioning PPT) of cuff occlusion. Participants were then moved to an adjacent room and provided a comfortable chair to sit on and receive active or sham tDCS. Following the 10 min of stimulation, participants were brought back to the first room to undergo post-stimulation pain sensitivity and CPM measurements (post-stimulation CPM). This involved the same PPT measurements before (post-stimulation pre-conditioning PPT) and after (post-stimulation post-conditioning PPT) the CS of cuff occlusion.
Participants were then led into an adjoining room and instructed to sit at a desk. The stress induction protocol then commenced. Once the 10-minute speech preparation phase was completed, participants were collected from the adjoining room and instructed to stand in front of a desk behind which both researchers were seated. Once participants were in front of the desk, they were asked to indicate on the stress-NRS their level of perceived stress at that moment (post-TSST perceived stress). Participants were then thanked for preparing their speech and informed that they were not required to present anything. The third (post-TSST) PPT and CPM assessments were then conducted. Finally, participants were debriefed, thanked for their participation, and given both researchers’ contact information in case of future questions or concerns.
Results
Data screening
All processing, screening, and analysis of data was conducted using IBM SPSS (Version 27, IBM Corp, Armonk, NY). Two participants withdrew before the beginning of the TSST, and the corresponding data was considered incomplete and not used in the analyses. A visual inspection of Z-score distributions of all variables revealed no univariate outliers greater than 3.29 standard deviations from the mean. Visual inspection of relevant histograms supported the assumption of normality. The final sample consisted of 38 participants: 20 (10 female) in the active condition and 18 (9 female) in the sham condition.
As per the recommendations of Yarnitsky, Bouhassira, 13 CPM was calculated as both absolute and relative changes in PPTs from pre- to post-conditioning. To calculate absolute CPM, post-conditioning PPTs were subtracted from pre-conditioning PPTs (lower scores represent greater endogenous modulatory functioning). Relative CPM was calculated as (post-conditioning PPT − pre-conditioning PPT)/pre-conditioning PPT, multiplied by 100. Therefore, relative CPM values represent the relative (percentage) change in PPTs from pre- to post-conditioning, with higher percentages representing greater pain inhibition to the TS when followed by the CS.
Prior to analysis, assumptions for parametric tests were assessed and confirmed. To assess potential differences in age and DASS scores between conditions at baseline, independent samples t-tests were conducted. Separate 2 × (3) mixed factorial ANOVAs were conducted to assess the effects of tDCS on endogenous modulatory capacity. The first factor in this analysis was condition (two levels: active and sham) and the second factor was time (three levels: baseline CPM, post-stimulation CPM, and post-TSST). Additionally, a 2 × (3) mixed factorial ANOVA was used to investigate the effects of tDCS on PPTs. In this analysis, the first factor was condition (two levels: active and sham) and the second factor was time (three levels: baseline pre-conditioning PPT, post-stimulation pre-conditioning PPT, and post-TSST pre-conditioning PPT). Finally, a 2 × 3 mixed factorial ANOVA was used to investigate the effects of tDCS and exposure to an acute psychosocial stressor on perceived stress levels. In this analysis, the first factor was condition (two levels: active and sham) and the second factor was time (three levels: baseline perceived stress, post-stimulation perceived stress, and post-TSST perceived stress). Simple effects analyses were conducted using independent samples t-tests to investigate significant interaction effects with Bonferroni corrections to reduce Type I errors (α of 0.017). Effect sizes are reported as Cohen’s d and partial eta squared (η p 2 ). Alpha levels <0.05 were considered statistically significant.
Baseline differences
Descriptive statistics for age and DASS subscale scores across tDCS conditions.
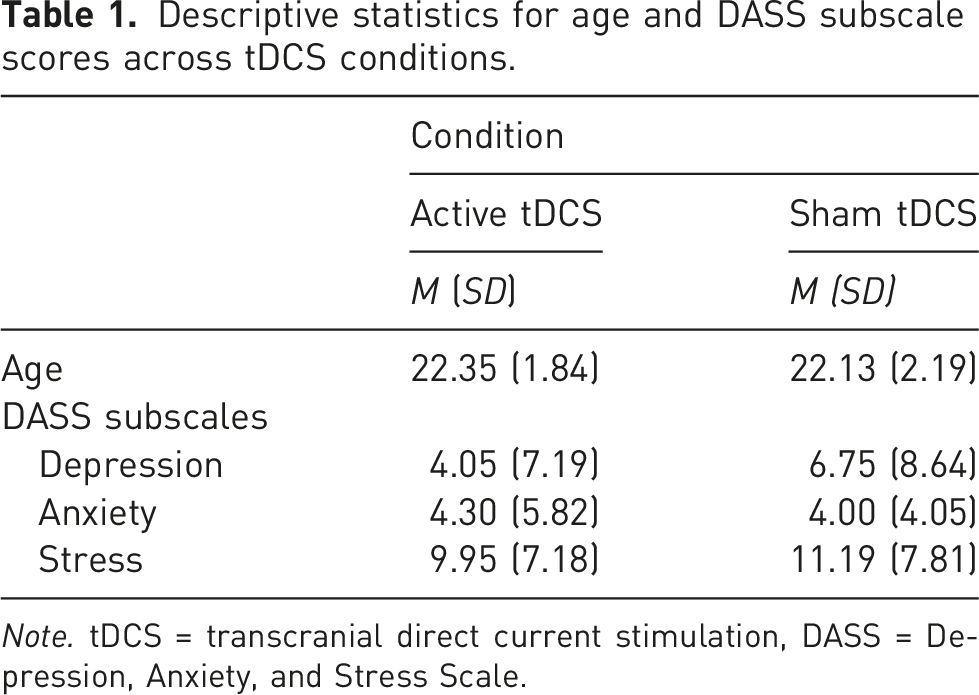
Note. tDCS = transcranial direct current stimulation, DASS = Depression, Anxiety, and Stress Scale.
Absolute CPM
Mean and standard deviations for participant’s absolute CPM scores across condition and time.
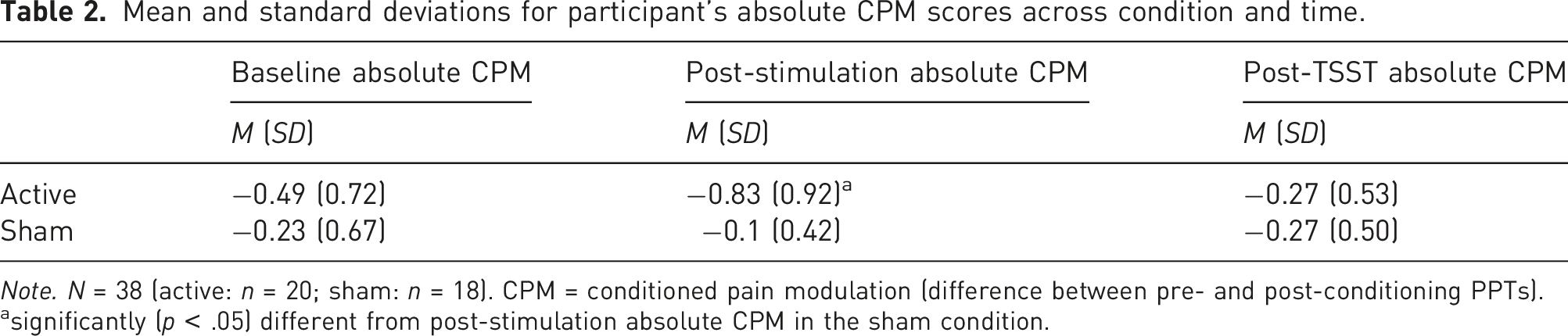
Note. N = 38 (active: n = 20; sham: n = 18). CPM = conditioned pain modulation (difference between pre- and post-conditioning PPTs).
asignificantly (p < .05) different from post-stimulation absolute CPM in the sham condition.
Simple effects analyses revealed a significant difference in post-stimulation absolute CPM scores across conditions t(29.02) = −3.45, p = 0.002, with a large effect size (d = 0.73), and a non-significant difference in baseline absolute CPM scores across conditions t(38) = −1.27, p = 0.211, and post-TSST absolute CPM t(36) = 0.02, p = 0.99 (see Figure 1). Absolute CPM scores of active and sham conditions across time. Lower scores represent greater endogenous pain modulatory capacity. Error bars represent standard error. CPM = conditioned pain modulation. TSST = Trier Social Stress Test. *significantly (p < .05) different from post-stimulation absolute CPM in sham condition.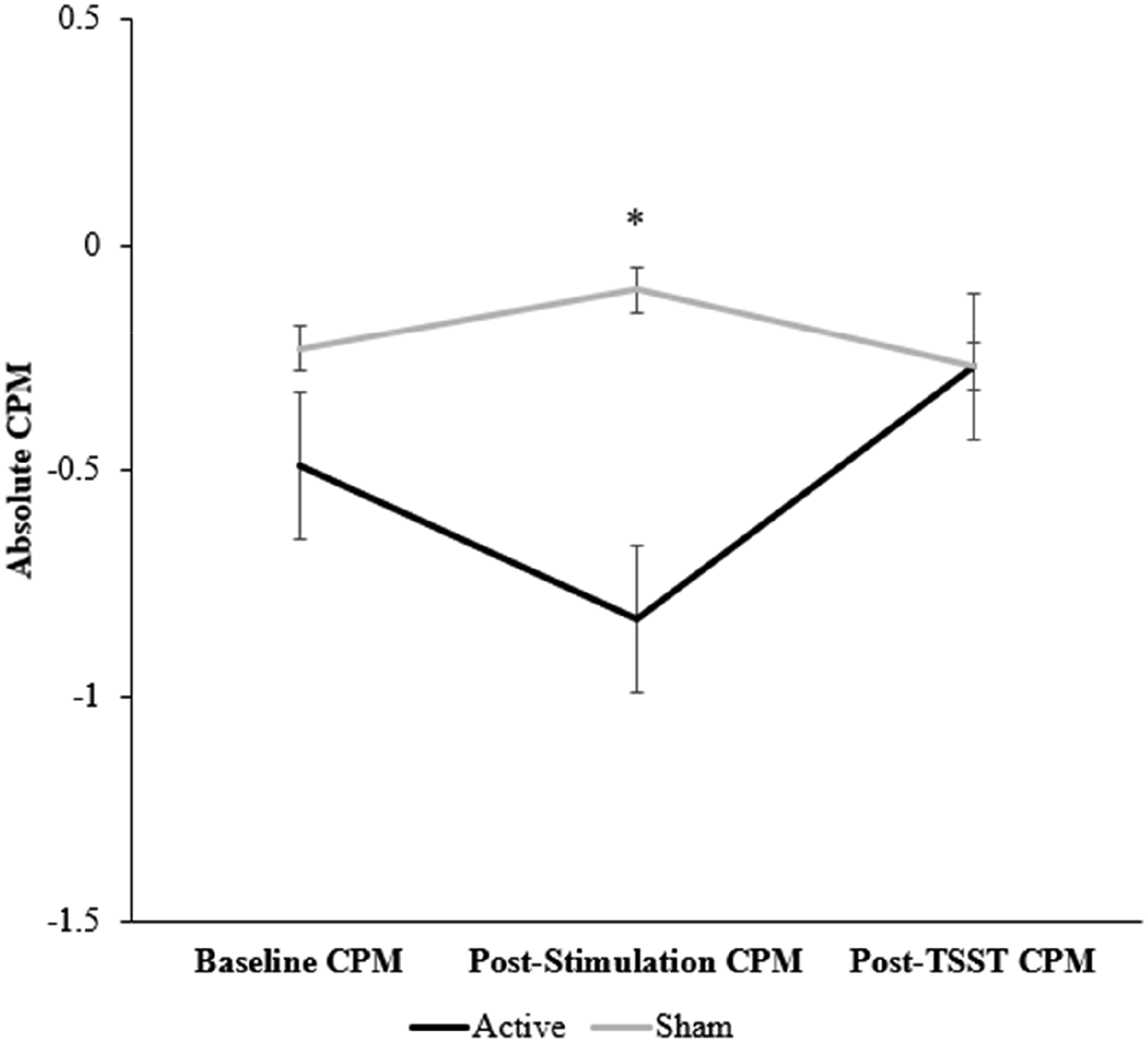
Relative CPM
Mean and standard deviations of relative CPM scores across conditions and time.
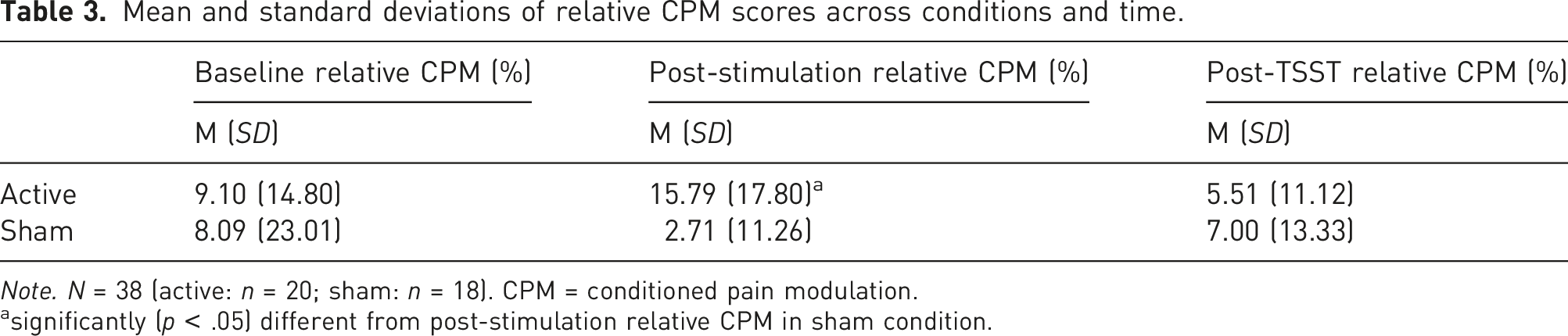
Note. N = 38 (active: n = 20; sham: n = 18). CPM = conditioned pain modulation.
asignificantly (p < .05) different from post-stimulation relative CPM in sham condition.
Simple effects analyses of the significant interaction revealed a significant difference in post-stimulation relative CPM scores across conditions t(31.42) = 2.72, p = 0.01, with a large effect size (d = 0.86), and a non-significant difference in baseline relative CPM scores across conditions t(38) = 0.19, p = 0.85, and post-TSST relative CPM t(36) = −0.37, p = 0.72 (see Figure 2). Relative CPM scores across conditions and time. Higher values represent greater pain inhibition to the testing stimulus (pressure) following the conditioning stimulus (cuff occlusion). Error bars represent standard error. CPM = conditioned pain modulation. TSST = Trier Social Stress Test. * significantly (p < 0.05) different from post-stimulation relative CPM in the sham condition.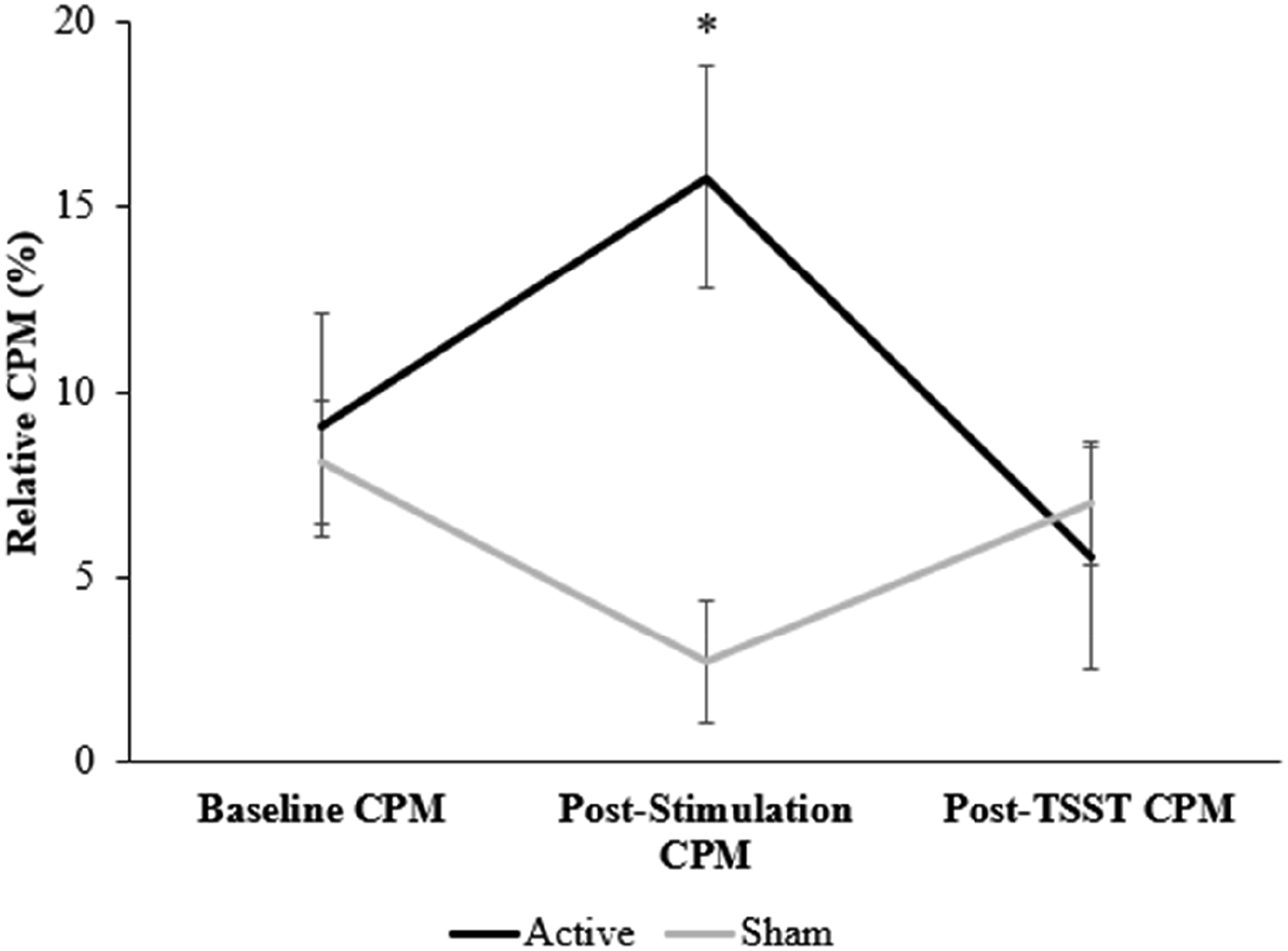
PPT
Mean and standard deviations of participant’s PPT across conditions and time.

Note. N = 38 (active: n = 20; sham: n = 18). PPT = pain pressure threshold (force required to elicit perceived pain).
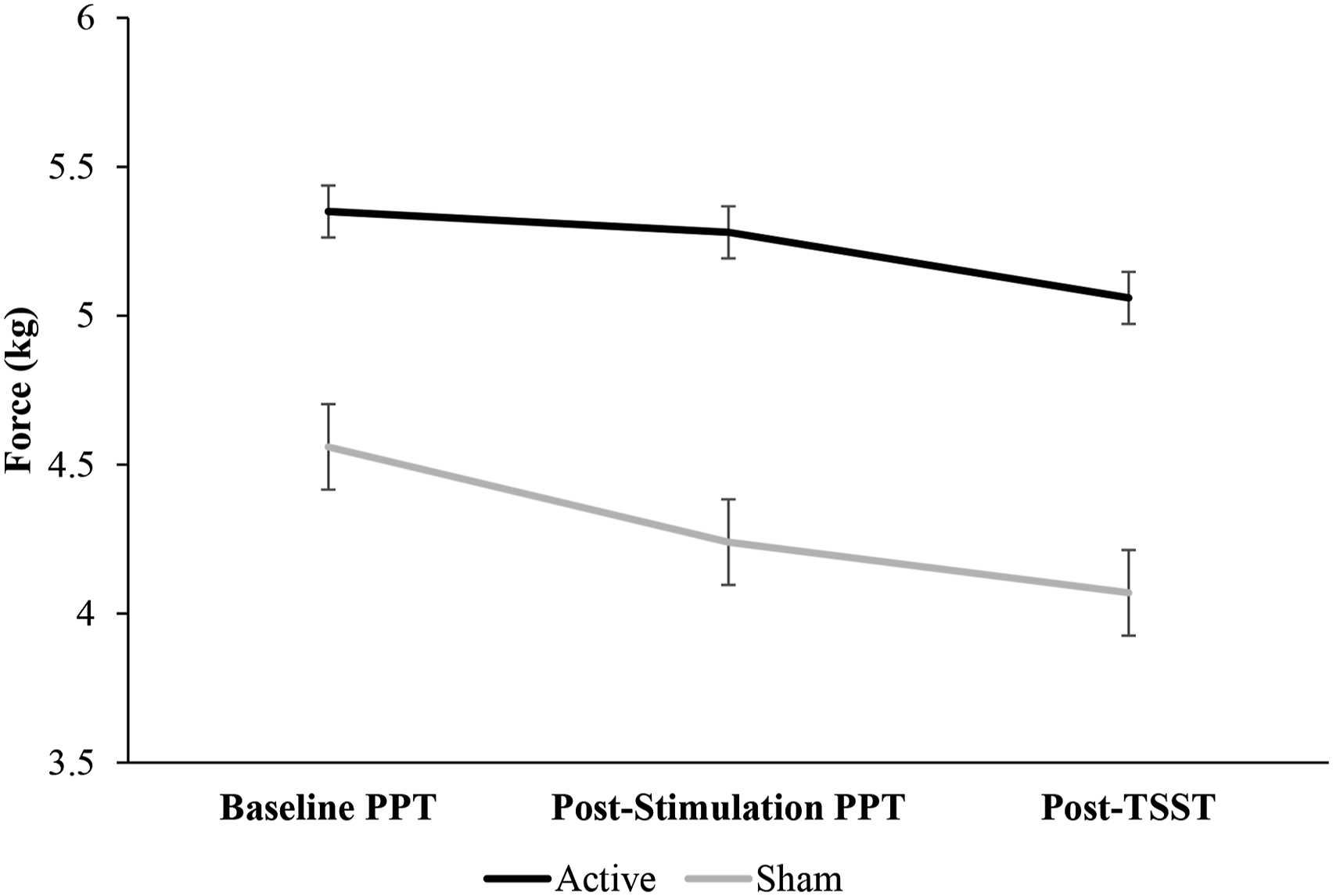
Mean PPT scores across conditions and time. Higher values represent greater pain thresholds measured in kilograms of force applied to the index finger. Error bars represent standard error. PPT = pain pressure threshold. TSST = Trier Social Stress Test.
Perceived stress
The analysis of perceived stress levels revealed a significant main effect of time F(1.68, 60.52) = 84, p < 0.001, η p 2 = 0.76. Post hoc analysis with a Bonferroni adjustment revealed that post-TSST perceived stress levels were significantly higher than baseline (pre-tDCS) perceived stress levels (p < 0.001). Post-TSST perceived stress levels were also significantly higher than post-tDCS perceived stress levels (p < 0.001).
Mean and standard deviations of participant’s perceived stress across conditions and time.
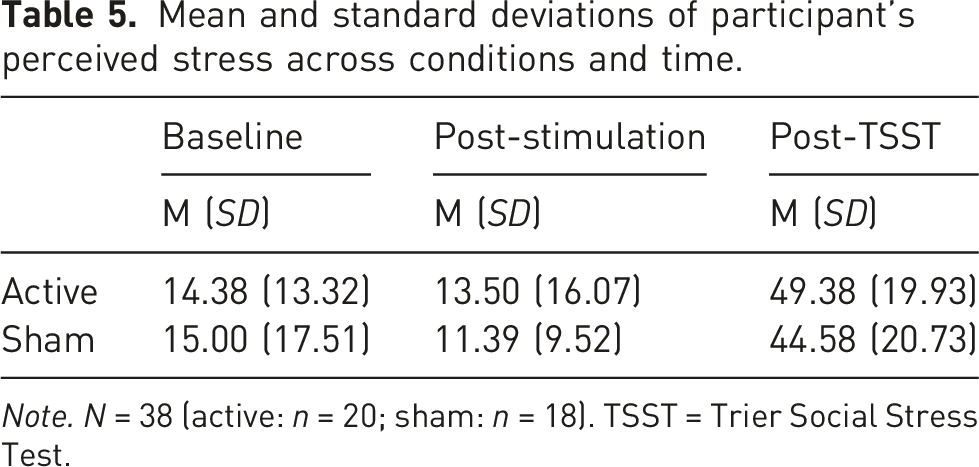
Note. N = 38 (active: n = 20; sham: n = 18). TSST = Trier Social Stress Test.
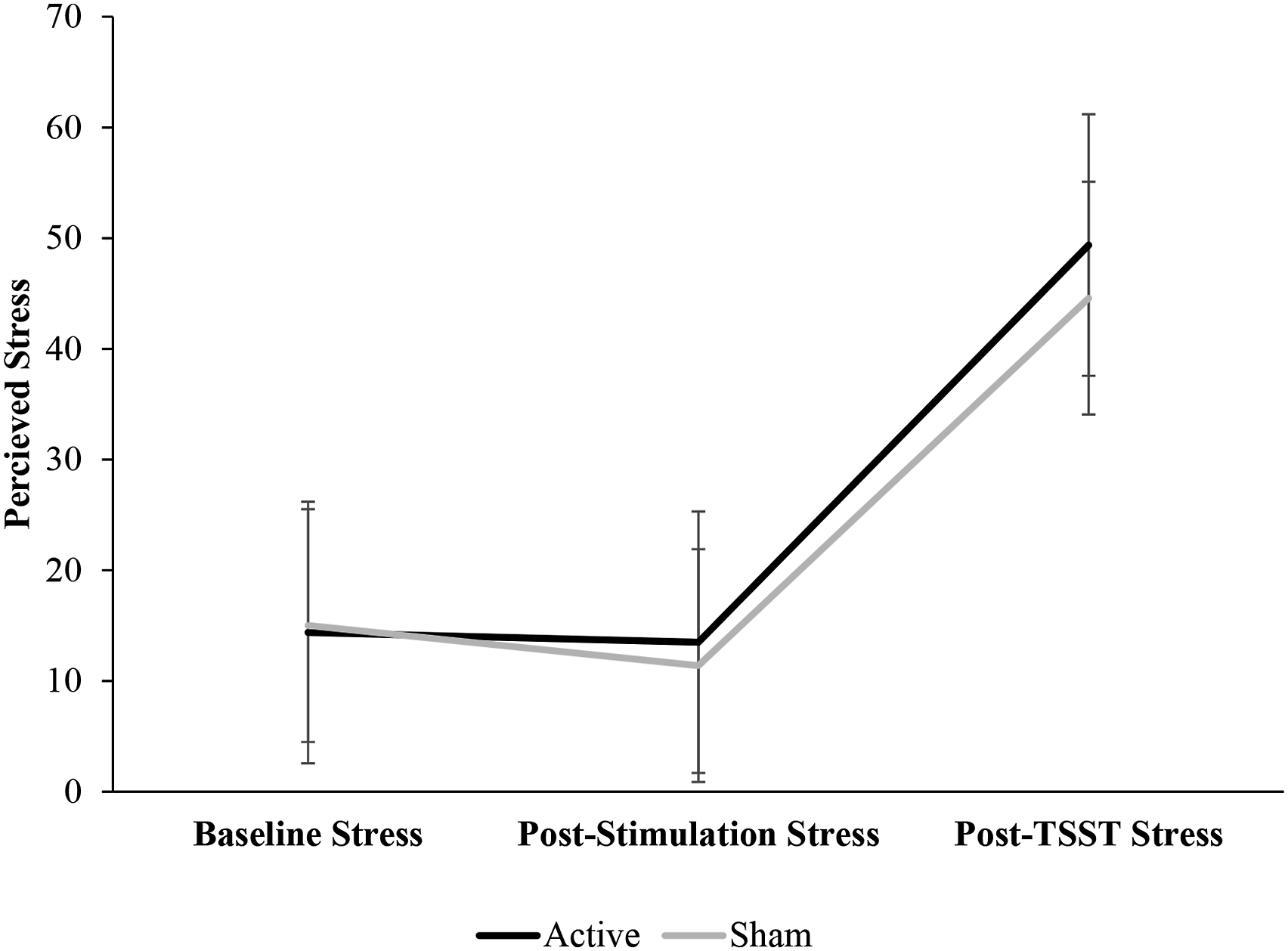
Mean perceived stress across conditions and time. Stress was measured using a visual analogue scale, with participants verbally indicating their level of perceived stress. Higher values represent greater perceived stress. Error bars represent standard error. TSST = Trier Social Stress Test.
Discussion
The current study aimed to investigate the effects of tDCS over the DLPFC on pain sensitivity, endogenous pain modulation, and stress-induced hyperalgesia. It was hypothesised that active tDCS would enhance endogenous pain modulatory capacity and reduce pain sensitivity when compared to sham tDCS. Active tDCS was also expected to significantly reduce stress-induced hyperalgesia when compared to sham stimulation. Findings in relation to these hypotheses are discussed below, with reference to existing literature.
Supporting the first hypothesis, the application of anodal HD-tDCS over the left DLPFC induced a significant increase in endogenous pain modulation. This finding aligns with previous research, with reports of anodal tDCS over the M1 significantly enhancing CPM in healthy populations.19,20 However, a more recent study by Jiang, Wang 50 reported that tDCS over the DLPFC does not induce any significant change in CPM, whereas M1 stimulation does. The inconsistency between the current findings and those of Jiang, Wang 50 may relate to the differences in the method of tDCS application. Specifically, Jiang, Wang 50 applied HD-tDCS at an intensity of 2 mA for 20 min, with electrodes placed in a 3 × 1 ring formation. In contrast, we applied 2 mA stimulation for 10 min using a 4 × 1 ring formation. These variations in stimulation duration and electrode montage may be significant,51,52 and comparisons of the efficacy of these differing approaches should be further investigated.
Beyond the findings relating to the effects of tDCS on endogenous pain modulation, no significant difference in pain sensitivity was observed when comparing active and sham tDCS conditions. While this finding is consistent with previous research which has reported no effect of tDCS over the left DLPFC on pain sensitivity in healthy populations, 53 it contradicts other research supporting the analgesic effects of tDCS over the left DLPFC. 54 The discrepancy between these findings may be explained by the methodological differences across these investigations, namely, in the application of tDCS itself. For instance, Kold and Graven-Nielsen 53 found no significant influence of DLPFC stimulation on pain sensitivity following the application of HD-tDCS. In contrast, significant reductions were reported after the application of conventional tDCS. 54 Computational modelling has shown that there are large focality differences between HD-tDCS and conventional tDCS, demonstrating conventional tDCS to induce widespread stimulation effects across the brain. 44 Therefore, significant reductions in pain sensitivity following conventional tDCS over the DLPFC may be explained by the inadvertent stimulation of neighbouring cortical sites, including the M1, which has previously been shown to reduce pain sensitivity.55,56
The third hypothesis of the current study related to the expected effect of tDCS on stress-induced hyperalgesia. This is the first study to consider the analgesic effects of tDCS on pain thresholds and modulation following an acute psychosocial stressor. Our findings indicate that while stress-induced hyperalgesia was established, indicated through reduced pain thresholds after the stress induction, active tDCS did not affect this hyperalgesic response. Analysis of these data showed no effect of active tDCS on perceived stress induced through the TSST, which contradicts previous research.22,57 These findings can be interpreted as evidence that tDCS over the left DLPFC may not effectively buffer the hyperalgesic effect of stress. One explanation for the current findings can be found in the perceived stress data. Analysis of these data showed no effect of active tDCS on perceived stress induced through the TSST. This is notable since existing research has proposed that the degree of hyperalgesia induced via a stressful task is dependent on the amount of stress experienced.15,58,59 Therefore, the current findings of no change in stress-induced hyperalgesia may be because stress was unaffected by the tDCS intervention.
The current findings offer both theoretical and clinical implications for the manipulation of pain through tDCS. First, the current findings support previous neuroimaging studies, which have observed the involvement of the DLPFC in pain inhibitory pathways through functional connections to the midbrain–medial thalamic pathway.24,56 We propose that the tDCS intervention used in the current study allowed for the targeted manipulation of DLPFC excitability, resulting in downstream effects on endogenous pain inhibitory systems. By extension, these findings inform the clinical utility of tDCS protocols in the treatment of chronic pain by presenting the DLPFC as an alternative target site for tDCS-induced analgesia. However, it is important to note that research to-date has not investigated the effects of tDCS over the DLPFC on pain modulation in chronic pain conditions. Therefore, the findings of this study should be interpreted with caution when generalising effects from a healthy population to chronic pain populations.
Although promising, the current findings need to be considered in the context of the study’s strengths and limitations. Firstly, HD-tDCS is an advanced form of tDCS which has been shown to induce more focal stimulation than conventional tDCS. 44 Using this form of tDCS allows for greater certainty about targeting the DLPFC, which ultimately produced significant changes in pain modulation. Further, the novelty of applying HD-tDCS over the DLPFC to induce changes in pain modulation is also considered a strength of this study and advances current knowledge in this field.
Despite these methodological strengths, several limitations of the current study should be acknowledged. As the current study included only young and healthy participants, care should be taken when attempting to generalise our findings to other populations, such as chronic pain sufferers and older adults. This is important given the widely documented differences in pain modulation profile observed across age ranges 25 and in chronic pain groups. 60 Thus, while tempting, the findings of the current study should not be solely used to inform the clinical utility of DLPFC stimulation via tDCS for the treatment of chronic pain. Indeed, we encourage further work to extend the current findings into other populations.
Conclusion
The current study provides novel insight into the effect of tDCS over the DLPFC on pain sensitivity, pain modulation, and stress-induced hyperalgesia. While active stimulation appeared to enhance pain modulatory capacity, no effects on pain sensitivity and stress-induced hyperalgesia were observed. The observed effect on pain modulation after a single dose of tDCS over the DLPFC is a novel finding that informs further research into the utility of tDCS in the treatment of chronic pain by presenting the DLPFC as an alternative target site for tDCS-induced analgesia. Future research should continue to investigate the analgesic potential of tDCS over the DLPFC.
Footnotes
Author contributions
CT recruited participants, developed the research question and hypotheses, collected and analysed data, and prepared and edited draft of manuscript. MM developed the research question and hypotheses, as well as collected and analysed data. AL performed statistical analyses and prepared draft of manuscript. AF developed the research question and hypotheses, devised protocol, edited draft of manuscript, and approved final manuscript. All authors discussed the results and commented on the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Ethical approval for this study was obtained from University of Canberra Human Research Ethics Committee (Project Number: 8087).
Informed consent
Written informed consent was obtained from all participants before the study.