
Abstract
Objective
The aim of this observational longitudinal study was to investigate the impact of lifestyle factors on the prognosis of patients with pain.
Methods
This study was part of a large prospective longitudinal study conducted in general practice (GP). Participants completed questionnaires at baseline (T0) and one year later (T1). Outcomes analysed were the EQ-5D index, presence of pain and the ability to perform a light work for 1 hour without difficulty.
Results
Among 377 individuals with pain at T0, 294 still reported pain at T1. This subgroup had a significantly higher BMI, more painful sites, higher pain intensity, more sleep problems, poorer general self-rated health (GSRH) and higher Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ) score at T0 than pain-free individuals at T1. There were no differences in age, sex, physical activity and smoking. In multivariable analyses, the number of painful sites, GSRH, sleep problems, pain duration, pain intensity and 2 short-form 10-item Örebro musculoskeletal pain questionnaire (SF-ÖMPSQ) items were independently associated with at least one outcome 1 year later. Only GSRH was strongly associated with all outcomes. The accuracy of GSRH at T0 to classify participants according to dichotomous outcomes was overall moderate (0.7 < AUC <0.8).
Conclusions
Lifestyle factors appear to have little influence on the outcome of patients with pain in GP. Conversely, poorer GSRH – which probably integrates the subjects’ perception of several factors – could be considered a negative prognostic factor in patients with pain.
Introduction
Chronic pain is usually defined as ‘pain that persists or recurs for longer than three months’. 1 This highly prevalent condition is challenging and generates high personal, financial and societal costs.2–6
To develop therapeutic management strategies and prevent chronification, it is essential to know the prognostic factors of a disease. Regarding pain, most of the current evidence concerns the role of psychosocial factors (called ‘yellow flags’) in the evolution of low back and musculoskeletal pain.7–10 Nevertheless, these factors do not explain all the observed variability in the prognosis of pain patients, suggesting that other variables contribute to prognosis.
For several years, lifestyle factors have been suggested to influence the prognosis of chronic pain.11–13 They include, but are not limited to, obesity, smoking and sleep habits, physical activity and (un)healthy diet. Some authors recommend multimodal treatments targeting these factors. 13 However, evidence on their presumed impact is still low and even sometimes contradictory. For instance, a recent systematic review found scarce and contradicting evidence for the implication of lifestyle factors as risk factors for pain persistence in patients with acute spinal pain. 14
Therefore, the aim of this 12 month longitudinal study was to identify, among non-cancer pain patients in general practice (GP), lifestyle factors predicting relevant outcomes based on the International Classification of Functioning, Disability, and Health (ICF): Body structures and functions (having pain), Activities (Function – light work) or Participation (quality of life [QoL]).
Materials and methods
Procedures
Research involving human subjects complied with all relevant national regulations, institutional policies and is in accordance with the tenets of the Helsinki Declaration (as amended in 2013), and has been approved by the local medical ethics committee of the Université Catholique de Louvain (2018/19JUI/258). It was part of a large longitudinal study performed in GP in French-speaking Belgium. Details of the study procedures have been published elsewhere. 10 Briefly, fifth-year medical students performing their one-month internship (November 2018, T0) in GP offered to the 3d patient scheduled every day to take part in the study. If the patient refused to participate, the 4th patient was approached, and so on. At T0, patients filled in informed consent and a set of paper questionnaires, including an e-mail address if they agreed to be contacted later. One year later (T1), all patients who provided their email address were sent a link to a secured online survey (LimeSurvey, LimeSurvey GmbH, Hamburg, Germany). Up to two reminders were sent if the patients did not respond within 15 days.
Inclusion and exclusion criteria
All patients scheduled for an appointment with participating GPs could potentially be included in the study. Exclusion criteria were age under 18, inability to answer questionnaires in French, pain caused by active cancer and absence of a valid e-mail address. We also excluded people with missing values from the analyses.
Questionnaires
The questionnaires completed at T0 (Appendix 1 – initial questionnaires) assessed demographic data, lifestyle-related variables, and pain-related variables.
Demographic questions included age, gender, weight, height, professional status (employed, student, retired, invalidity, unemployed) and postal code.
Lifestyle-related variables were assessed by 1 inquiring if the patient currently smoked (yes/no), 2 asking about sleep problems (‘During the last month, have you had any problems falling asleep or sleep problems?’ with possible responses being ‘never, sometimes, often, almost every night’) 15 and 3 the Exercise Vital Sign (EVS, ‘On average, how many days per week do you engage in moderate to strenuous exercise (like a brisk walk)?’ × ‘On average, how many minutes per day do you engage in exercise at this level?’). 16 General health perception (or general self-rated health, GSRH) was assessed using the first item of the SF-36 questionnaire (‘In general, would you say your health is…,’ with categorical responses including ‘excellent, very good, good, fair, poor’). 17 We used the eighth question from the long Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ) to assess work perception (‘Is your work heavy or monotonous?’ with answers from 0 = not at all to 10 = extremely). 18 Answers < 4 were considered to indicate light work, between 4 and 6 moderately heavy, and 7–10 heavy work.
Patients who reported pain at T0 were asked additional questions to assess whether their pain was the reason for the consultation, whether it was related to active cancer (exclusion criteria), where the pain was located, and how many body sites were painful. Finally, they also filled in the French version of the short-form 10-item Örebro musculoskeletal pain questionnaire (SF-ÖMPSQ).10,19 This version was derived from the original 25-item ÖMSPQ, a validated tool that assists clinicians in assessing the risk of persistent pain in people with musculoskeletal injury (Linton et al. 2003). It focuses mainly on ‘yellow flags’, which are good predictors of the risk of chronification in musculoskeletal pain and is nearly as accurate as the original extended version.10,19
At T1, the participants filled in the same questionnaires, along with the EQ-5D-5L questionnaire, a validated measure of QoL (EQ-5D User Guides – EQ-5D n.d. https://euroqol.org/publications/userguides, accessed Jul 8, 2022).
Data analysis
Statistical analyses were conducted using IBM SPSS Statistics 27. The number of painful sites (NPS) was computed from pain localization data and categorized into 4 items (0, 1, 2, or 3 + pain sites). The EQ-5D index was computed according to the recent EQ-5D-5L value set for Belgium. 20 Statistical significance was set at α = 0.05.
We used descriptive statistics to present the participants’ demographics, clinical characteristics and EQ-5D-5L data. Continuous variables were summarized using medians and interquartile ranges and compared between groups with a Wilcoxon test. Categorical variables were summarized using numbers and percentages and were compared between groups with a Pearson’s Chi-squared test.
We examined the following outcomes: EQ-5D index, presence of pain at T1, and having no difficulty doing light work for 1 hour (Function – light work) at T1. This latter was based on the ÖMPSQ item of the same name and dichotomized as having issues (1 to 9) vs. no issues (10 on a 10-point scale).
To identify potential prognostic factors, we first performed univariable binary logistic regressions or generalized linear models, according to the type of outcome. We also performed ordinal logistic regression for each dimension of EQ-5D-5L, available in Supplementary file 1 (‘Supplementary file 1 - Prognostic factors for each dimension’).
Then, in multivariable analyses, we systematically adjusted for age, sex and variables with a p-value <0.20 in the preceding univariable analysis. Results are reported as standardized regression coefficient (βStd), unstandardized regression coefficient (β), 95% confidence interval of the unstandardized coefficient (95% CI) and p-value. Odd ratios were computed based on unstandardized β. Professional status was coded using worker status as the baseline. Regarding the assumptions for statistical tests, multicollinearity (VIF > 4) was tested for each outcome. For binary logistic regression, we tested the goodness of fit of the model (using the Hosmer and Lemeshow test). For ordinal logistic regression, we checked the test of parallel lines. For GLM, we tested the equality of variances with Levene’s test. We reported each abnormal test with the results.
Finally, we performed Receiver Operator Characteristic (ROC) curve analyses to assess the ability of the GSRH item to predict QoL at T1. We dichotomized the 5 dimensions of EQ-5D-5L according to levels 1–2 (no or slights problems) vs. levels 3 to 5 (moderate to extreme problems). We reported the best cut-off value according to the Youden index (highest value with sensibility + specificity – 1) and computed the positive predictive value (PPV) and negative predictive value (NPV) in our cohort.
Results
Demographic and clinical characteristics at T0
Figure 1 shows the study flowchart. Flowchart of the study.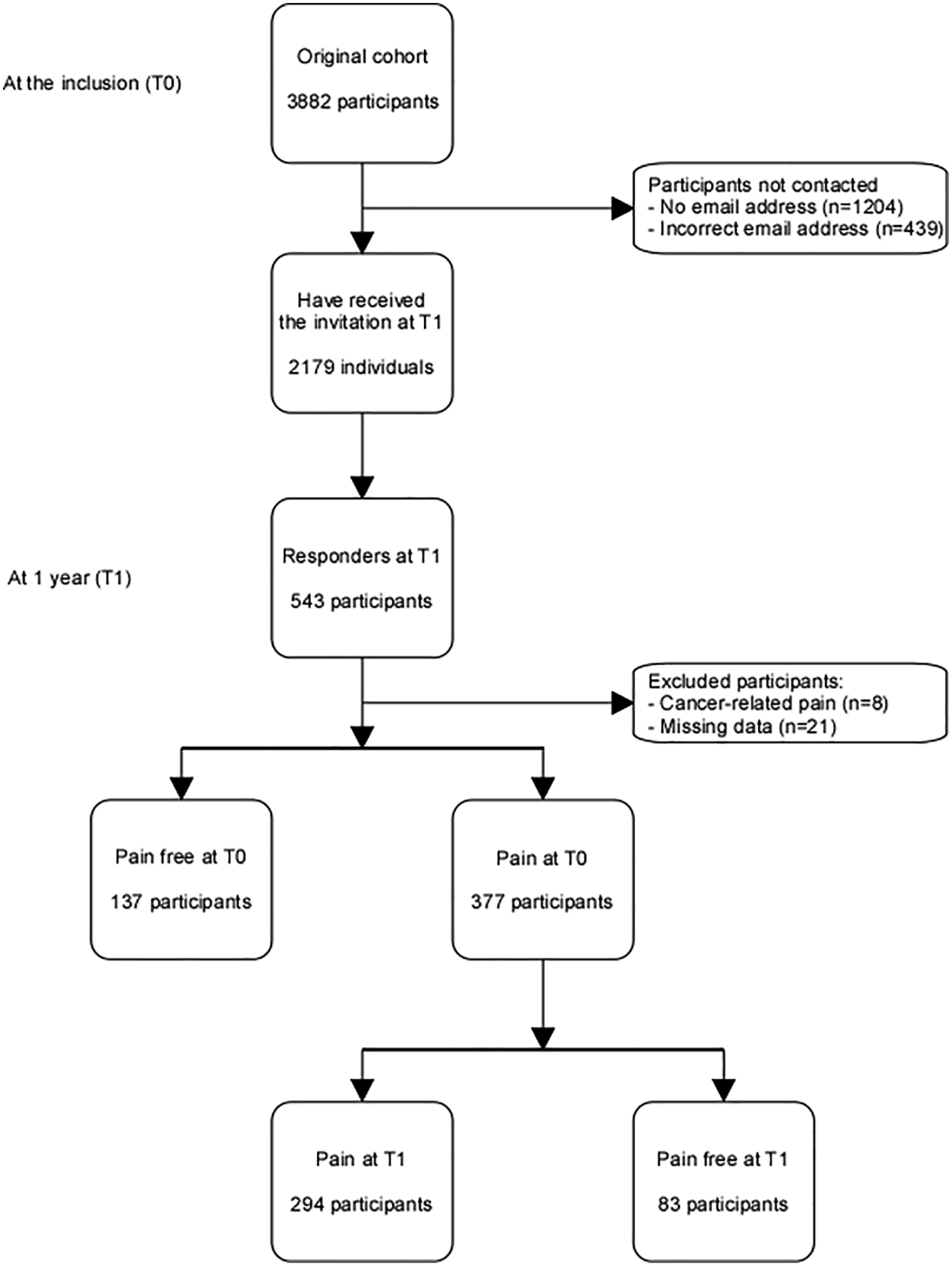
Among 3882 participants at T0, 543 filled in the online questionnaire at T1. After excluding participants suffering from cancer-related pain (n = 8) and cases with missing data (n = 22), 377 (73%) already reported pain at T0. Cases with missing values accounted for 3.9% of the whole cohort, and 4.8% of the analysed sample (participants with pain at T0). For further details about missing values, see Supplementary File 2 (“Supplementary file 2 - Missing data”).
Demographical and clinical characteristics at T0 of patients with and without pain at T1.
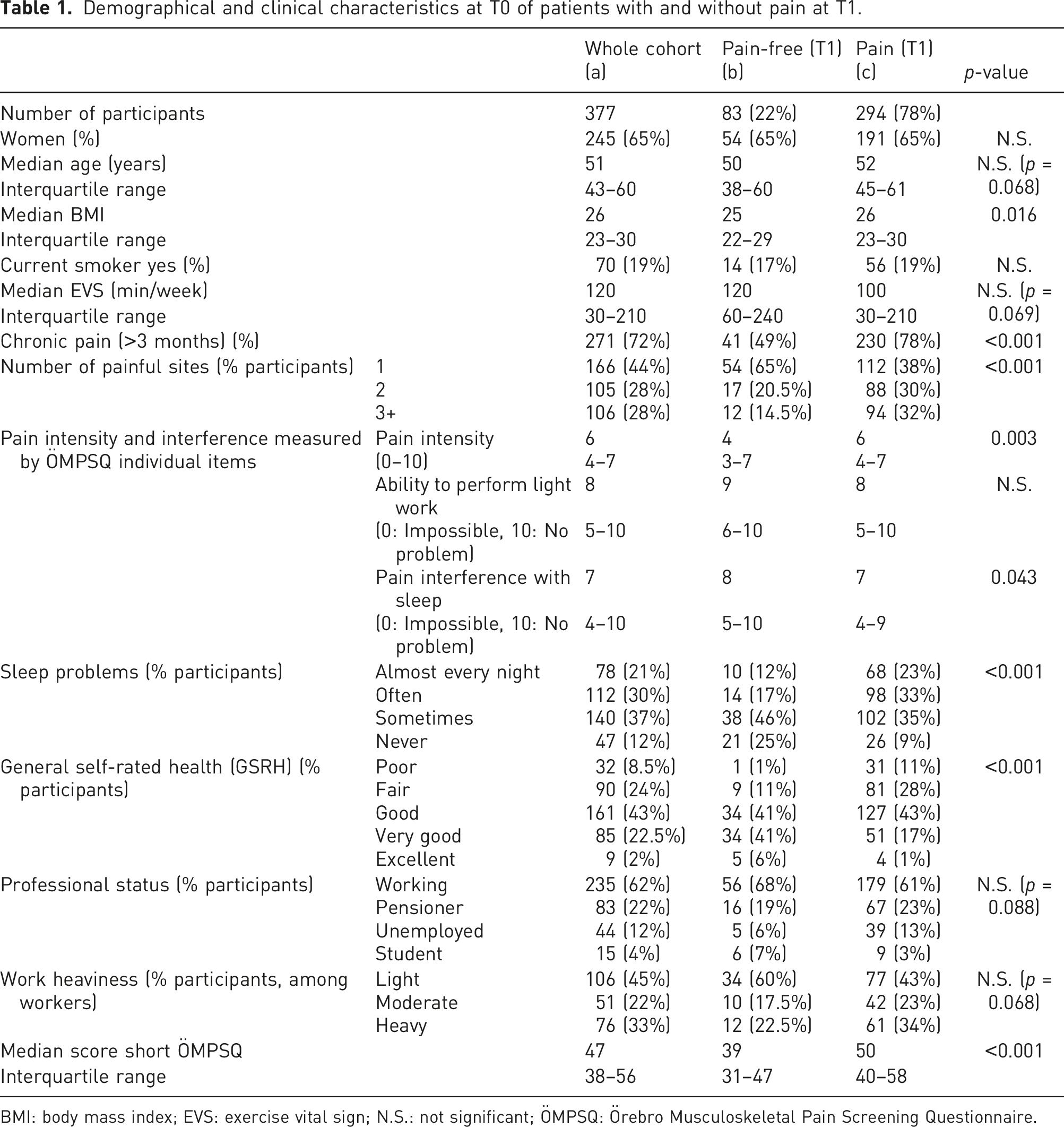
BMI: body mass index; EVS: exercise vital sign; N.S.: not significant; ÖMPSQ: Örebro Musculoskeletal Pain Screening Questionnaire.
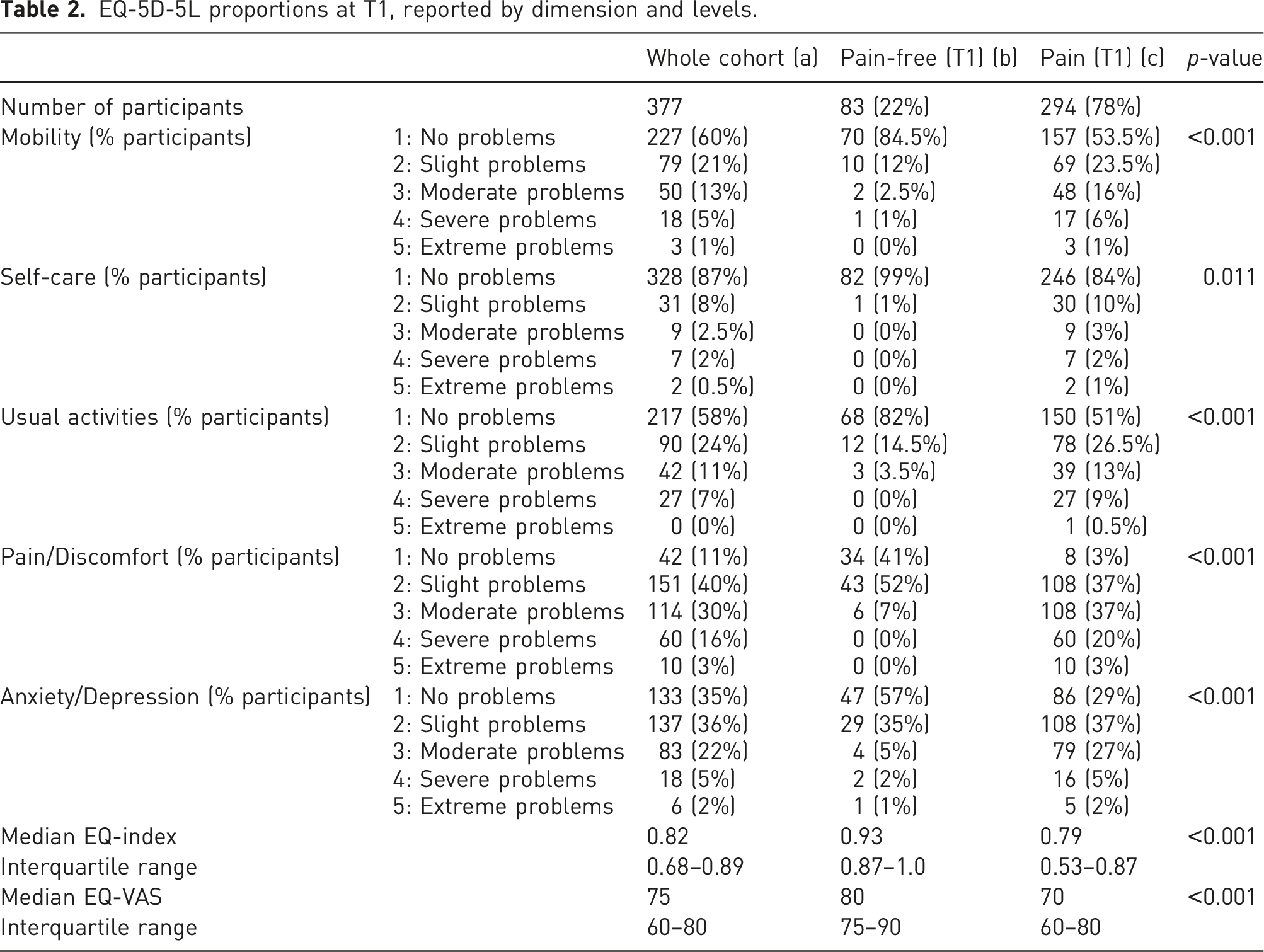
Quality of Life at T1
EQ-5D-5L proportions at T1, reported by dimension and levels.
Prognostic factors
Collinearity for each variable was low in all following analyses (VIF <2).
EQ-5D index – health state
In univariable analysis, age, BMI, smoking status, NPS, professional status (worker or unemployed), work heaviness, GSRH, sleep problems and all ÖREBRO items were associated with EQ-5D index.
Prognostic factors for EQ-index.
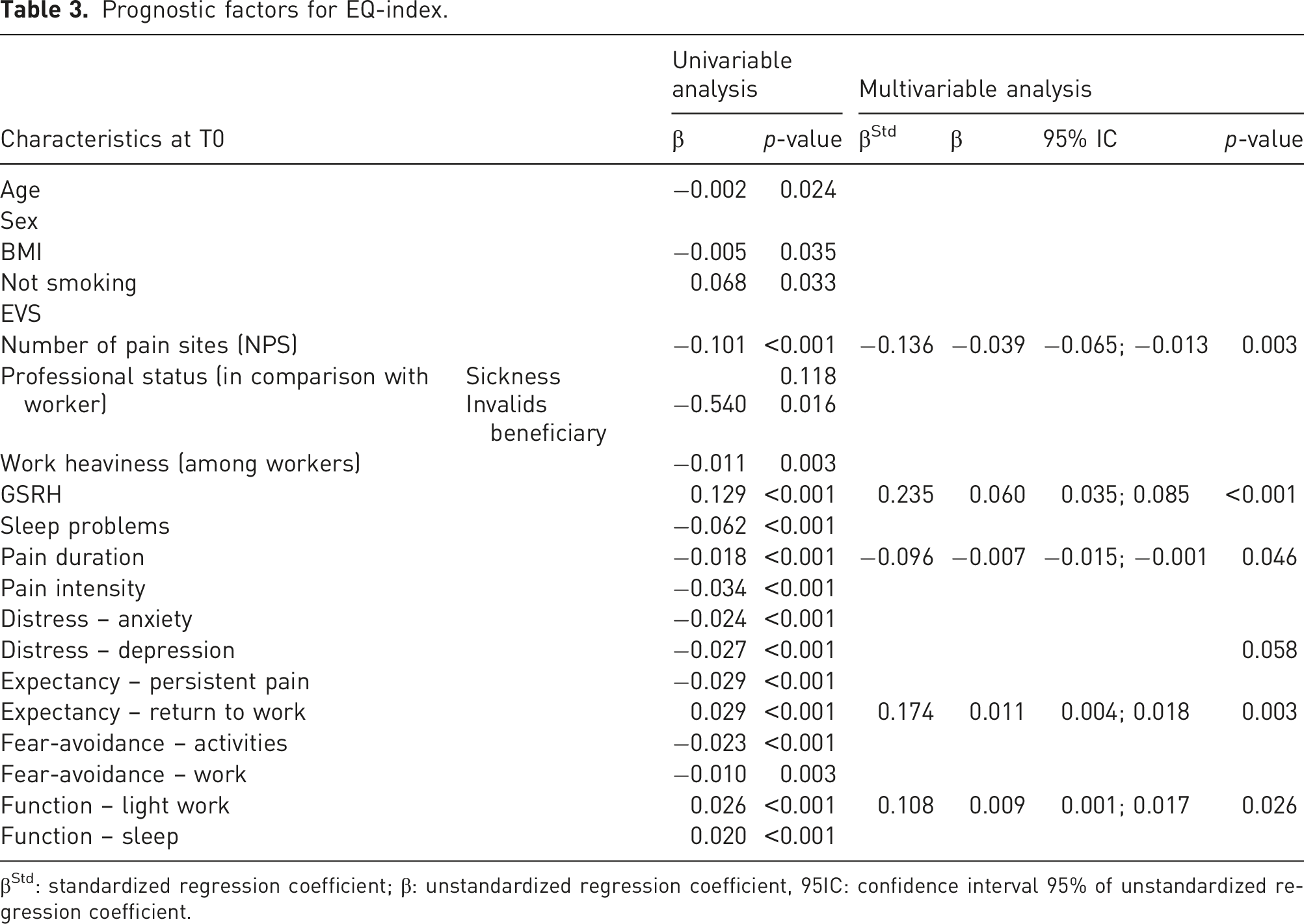
βStd: standardized regression coefficient; β: unstandardized regression coefficient, 95IC: confidence interval 95% of unstandardized regression coefficient.
Prognostic factors EQ-5D index at T1.
Having pain
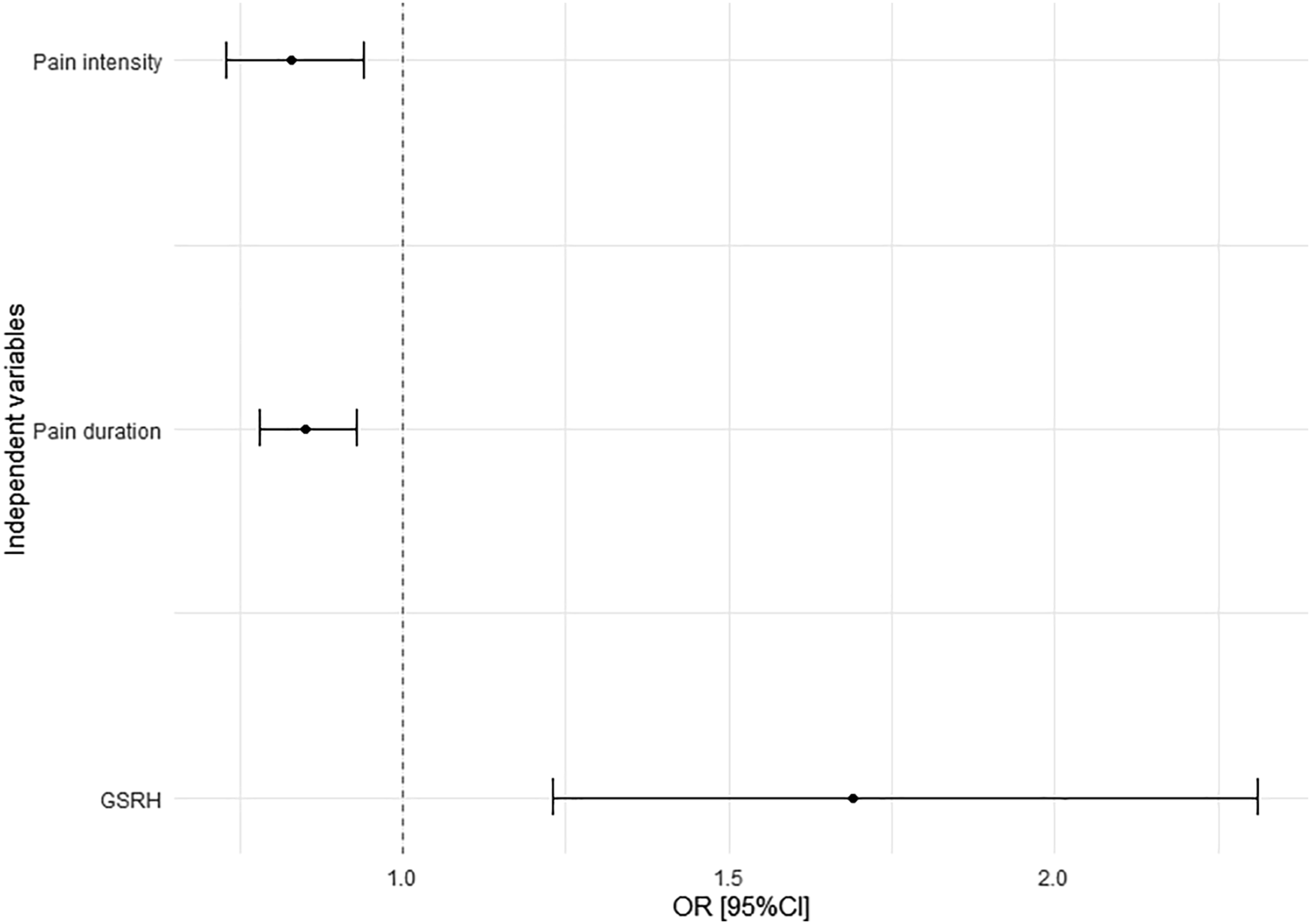
Using univariable binary logistic regression, we identified that age, NPS, perceived work heaviness, GSRH, sleep problems, pain duration, pain intensity, Distress – anxiety, Distress – depression, Expectancy – persistent pain, Expectancy – return to work and Function – sleep were associated with the probability of suffering from pain at T1.
Prognostic factors for having pain at T1 (yes/no).
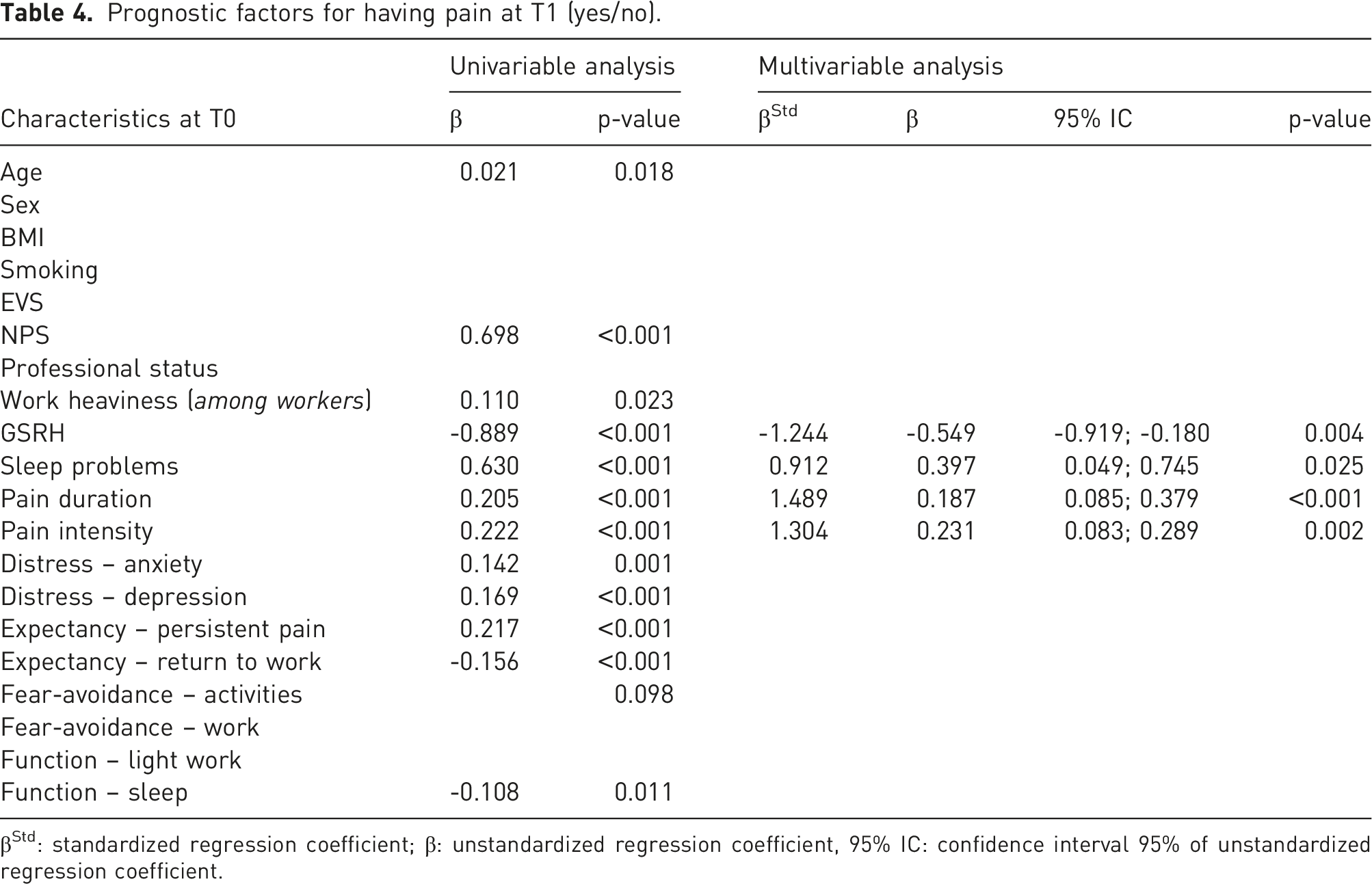
βStd: standardized regression coefficient; β: unstandardized regression coefficient, 95% IC: confidence interval 95% of unstandardized regression coefficient.
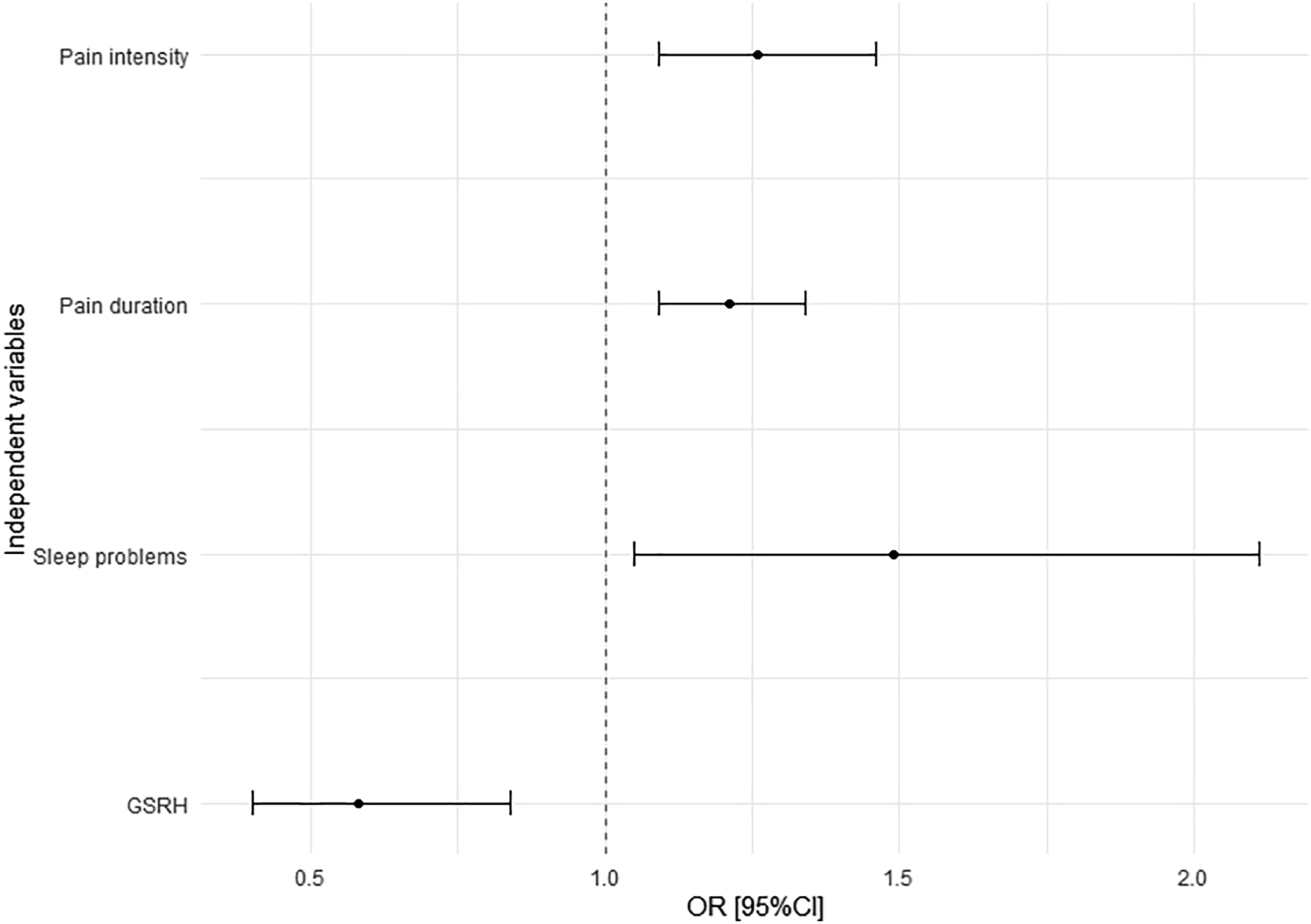
Prognostic factors Having pain at T1.
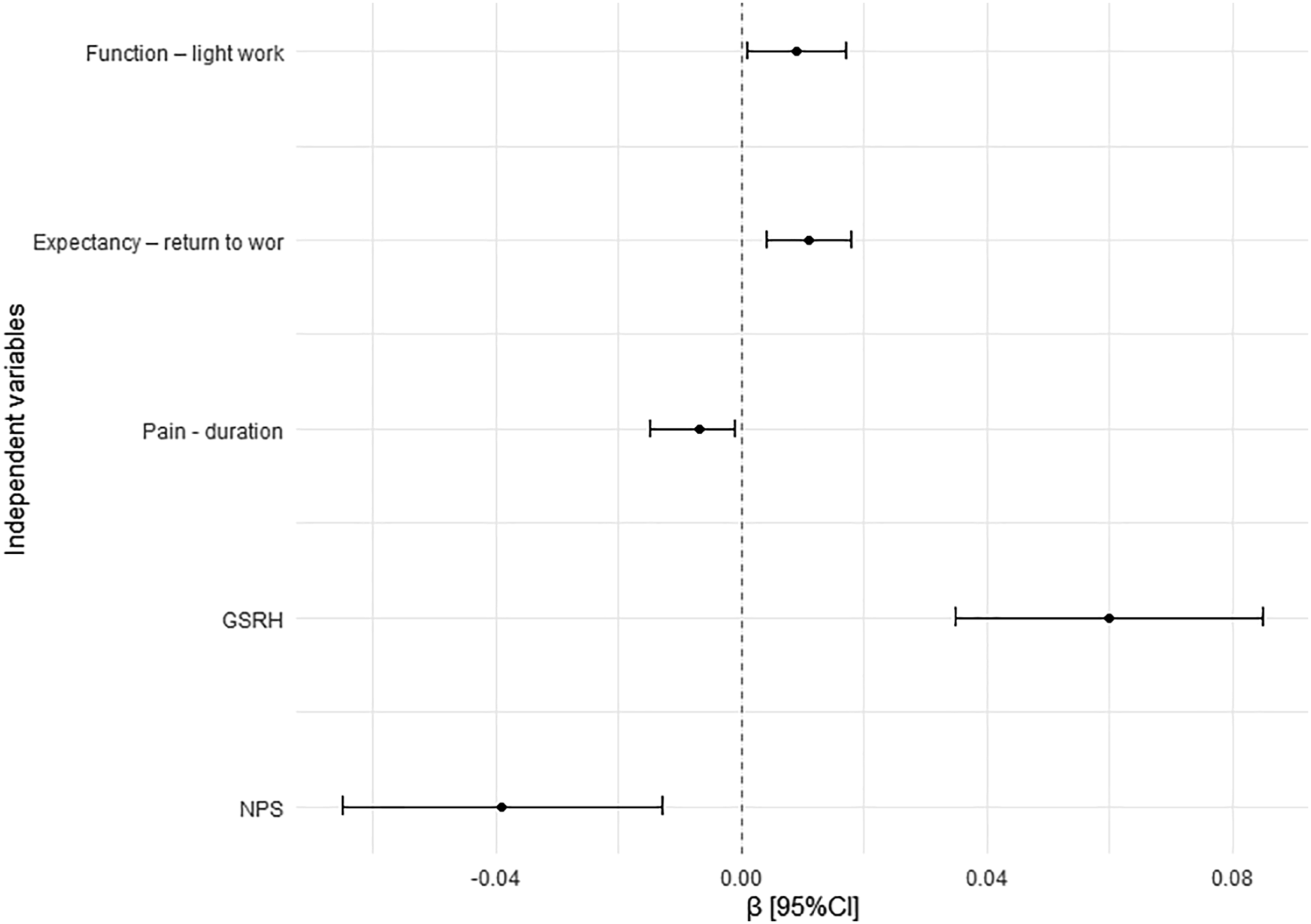
Function – light work
Using univariable binary logistic regression, age, BMI, NPS, professional status, EVS, perceived work heaviness, GSRH, sleep problems, pain duration and intensity, Distress – anxiety, Distress – depression, Expectancy – persistent pain, Expectancy – return to work, Fear-avoidance – work, Function – light work and function-sleep impacted the probability of not having problems performing light work during 1 hour at T1.
Prognostic factors for having issue performing light work during 1 hour at T1 (yes/no).
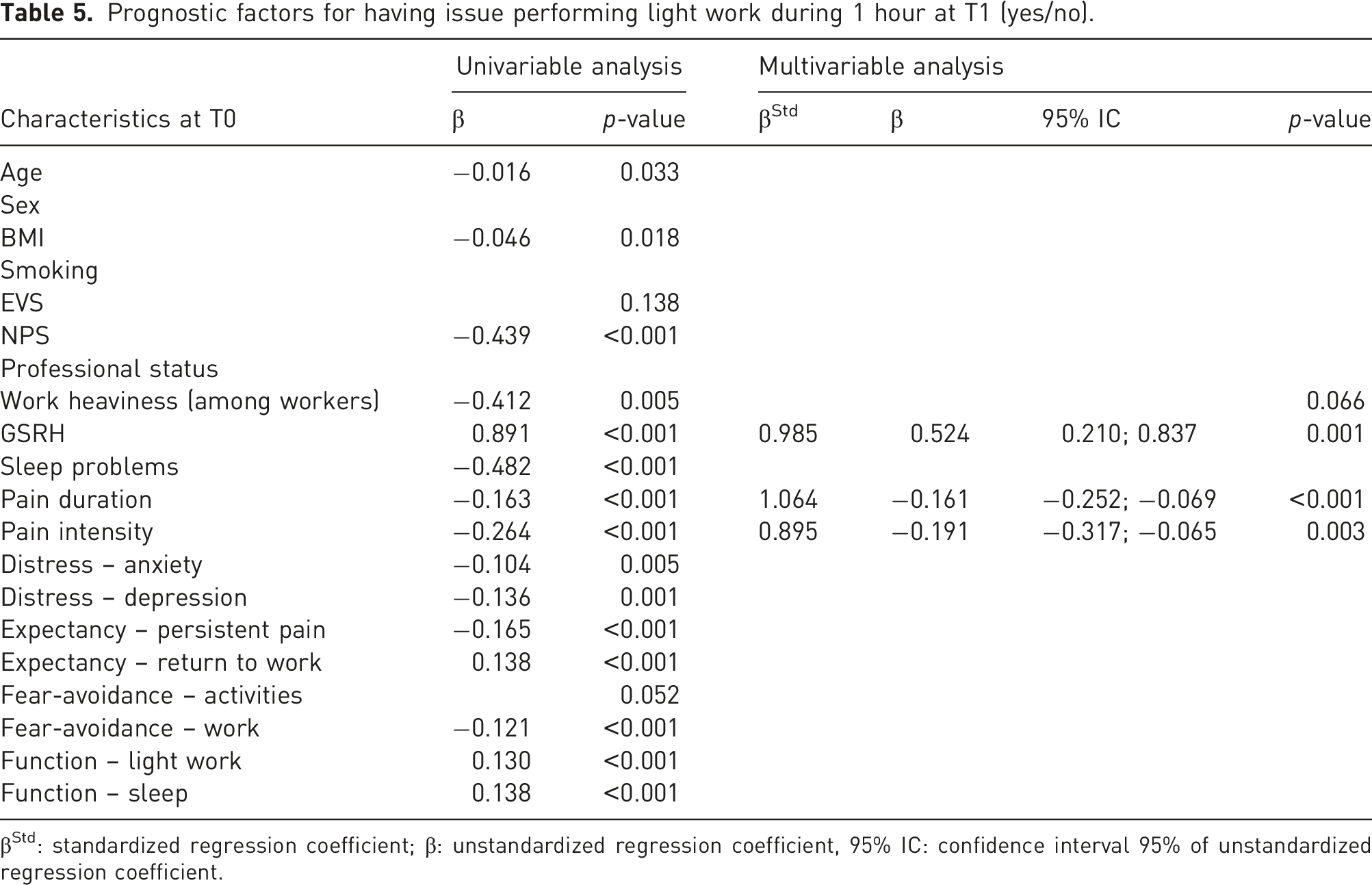
βStd: standardized regression coefficient; β: unstandardized regression coefficient, 95% IC: confidence interval 95% of unstandardized regression coefficient.
Prognostic factors Function – light work at T1.
Individual EQ-5D dimensions
Results for each EQ-5D dimension are available in supplementary data. Prognostic factors were similar to those observed with the EQ-5D index, but with some specificities. For example, BMI was independently associated with poorer mobility, self-care and pain/discomfort. Smoking was associated with poorer mobility. Except for self-care, GSRH was strongly associated with each dimension.
Receiver Operator Characteristic analyses
General Self-Rated Health: ROC analyses.
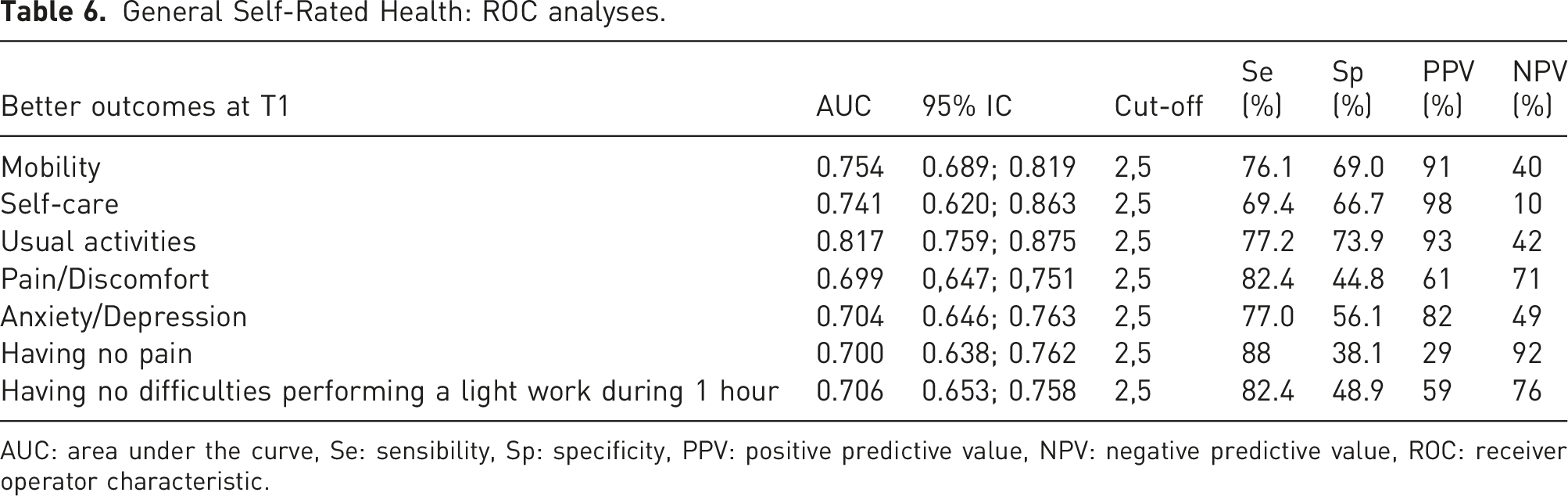
AUC: area under the curve, Se: sensibility, Sp: specificity, PPV: positive predictive value, NPV: negative predictive value, ROC: receiver operator characteristic.
For instance, the best accuracy was obtained with the Usual Activities outcome (AUC = 0.817, [0.759–0.875]). Using a value of 2.5 value as a cut-off (Sensitivity: 77.2%; Specificity: 73.9%), this question would have predicted participants with better outcomes at T0 with PPV = 93% and NPV = 42%.
Discussion
Demographic and clinical characteristics
Among participants with pain in GP, individuals reporting pain one year later had higher BMI, higher NPS, described more chronic pain, higher pain intensity, higher sleep problems, poorer GSRH and had higher ÖMPSQ score at T0 than pain-free individuals at one year.
At one year, they also described poorer QoL than pain-free individuals. In comparison with the respondents of the EQ-5D-5L value set for Belgium, 20 participants with pain at T1 reported poorer GSRH (63% vs. 75% of good to excellent self-rated health), had on average lower EQ-5D index (0.74 vs. 0.84), and lower EQ-5D VAS (69.0 vs. 77.6). Only 6.6% of the participants with pain reported no problems in the 5 dimensions (vs. 34.6%). These results were expected, given that chronic pain negatively impacts QoL. 2
Predictive factors
We identified several factors predicting QoL: NPS, GSRH, Distress – depression, Expectancy – persistent pain and Function – light work independently influenced EQ-5D index at T1. Regarding having pain at T1, only GSRH, sleep problems, pain duration and pain intensity were independently associated with this outcome. Finally, four factors influenced the probability of having no difficulties performing light work for 1 h: smoking, GSRH, pain duration and pain intensity.
In our cohort, we did not find a strong association between the different outcomes and individual lifestyle factors, such as physical activities, overweight, sleep problems and smoking. In the literature, the influence of these factors on pain is not clarified. A recently published systematic review investigating the role of lifestyle risk and protective factors for the development of chronic spinal pain in longitudinal studies found conflicting evidence for several factors such as BMI, smoking, and physical activity. 14 Another systematic review synthesized evidence of risk factors for new episodes of back pain in emerging adults. 21 The authors reported conflicting evidence for lifestyle factors. Eventually, another systematic review found no association between these factors and non-specific neck pain in young adults. 22 Conversely, in a Norwegian longitudinal cohort including adolescents (n = 1824), participants with persistent musculoskeletal pain at baseline and reporting >4 adverse lifestyle behaviours described more persistent musculoskeletal pain at 11-year follow-up than those with only 0 or 1 adverse lifestyle behaviour (OR: 2.23). 23 Nevertheless, each individual factor was not associated with a worse outcome (with the exception of smoking), whereas none were associated with future persistent pain in adolescents without pain at baseline. Over a 2-year period, adherence to an ‘optimal lifestyle’ (3 to 4 components [OR: 0.44 and 0.69, respectively], including physical activity, smoking, alcohol use and consumption of fruits and vegetables) was shown to reduce the incidence of back pain in a cohort of active employees (n = 6848). 24 Again, individual components of optimal lifestyle were not associated with the incidence of back pain. In the same way, reporting several healthy lifestyle behaviours (3 or 4 in comparison with 0 or 1) was associated with lower incidence of neck pain in women (RR: 0.52). 25 The incidence of low back pain and neck pain in men did not differ between the 2 groups. We could therefore hypothesize that lifestyle factors only slightly influence the pain prognosis, but the accumulation of several healthy habits could affect the outcomes.
Among the identified prognostic factors, only GSRH was strongly associated with all outcomes. As explained by DeSalvo et al. this single item probably ‘serves as a proxy for the array of important covariates known to predict health and resource needs’. It ‘may also function as a dynamic evaluation reflecting judgments about trajectory of health, rather than just the current level of health’. 26 In a prospective cohort study that followed up 21,732 veterans for one year, GSRH at baseline predicted important outcomes (mortality, hospitalization) as well as SF-36 and Seattle index of comorbidity (SIC). 27 It has been associated with lifestyle factors such as overweight and obesity, dietary habits and physical activity.28–30 In prospective studies, poorer GSRH predicted higher type 2 diabetes incidence, 31 and mortality.26,32 In cross-sectional studies, it has been associated with a higher level of inflammatory markers (erythrocyte sedimentation rate, C-reactive protein and interleukin-6),33,34 sleep problems, 35 anxiety – depressive disorders 30 and pain.30,36,37 In a Finnish cross-sectional cohort study (n = 4542), the prevalence of chronic pain was independently associated with self-rated health status. For example, those describing poor GSRH had more daily chronic pain (OR: 11.82) than other participants. 37 Among a Swedish elderly cohort (n = 1360), the pain was independently associated with poorer GSRH (OR: 3.8). Physical activity (OR: 1.5) also impacted the health perception in the multivariable model but the result was at the limit of being not significant. 30 To the best of our knowledge, only one longitudinal study investigated the link between mortality and poorer self-rated health. 32 The England Longitudinal Study of Ageing (n = 6324) followed adults aged 50 years or older. Poorer self-rated health was found to mediate the relationship between troubling pain and mortality.
Compared to our previous analyses of this cohort, 10 the accuracy of the GSRH in predicting outcomes in participants with pain was broadly similar to that of the SF-ÖMPSQ. The AUC for EuroQol 5 dimensions were between 0.699 and 0.817 in the present study vs. 0.583 and 0.781 for SF-ÖMPSQ in our former analysis. To predict presence/absence of pain at T1, AUC for GSRH was 0.700 vs. 0.674 (acute-subacute pain) and 0.732 (chronic pain). Two reviews evaluated the performances of the STarT Back Screening Tool and the ÖMPSQ to discriminate pain outcomes in back pain.38,39 These questionnaires do not appear to perform better than the GSRH assessment in our study (AUC between 0.55 and 0.80).
Strengths and weaknesses
This work has several strengths. Few longitudinal studies have focused on primary care and even fewer on lifestyle factors yet general practitioners have to manage acute and chronic pain on a daily basis, 37 while the vast majority of pain patients will never be seen by secondary or tertiary care. 40 Our results are probably closer to ‘real life’ because we recruited patients directly through their GP, without restrictions in terms of conditions or reasons of consultation. In addition, there were little missing data in our analysed cohort.
Some limitations should also be noted. First, participants filled in the first questionnaires (T0) with different interviewers. This may have increased variability between participants’ responses. Second, the ‘having pain’ outcome at T1 could have been more accurate. It did not indicate whether the participants still had the same pain 1 year later. Third, the EVS and smoking variables could be considered inaccurate. The former was misunderstood by some participants (indicating ‘30 days per week’ as the exercise frequency, for example), whereas the latter was dichotomous and did not capture the quantity or the duration. Fourth, our cohort at T1 was not as large as expected. Many participants at T0 chose not to reply to our invitation one year later. In addition, only people with an email address were invited to this second part, which could constitute a selection bias. Our sample (n = 535) was, for instance, younger (1.8 years on average) than the original cohort but was similar in terms of sex, body mass index, smoking, EVS and presence of pain at T0.
Clinical implications
Given the accuracy of the GSRH in predicting QoL and pain, this single item could be used as a screening question, where poor answers would be considered as indicating an increased risk of pain persistence.
In addition, our results suggest that lifestyle factors only slightly influence the prognosis of patients in pain. While the benefits of lifestyle interventions are well established in many conditions, including chronic pain,41–44 these interventions should perhaps not be the core of pain secondary preventions strategies. Stratified approaches targeting psychosocial factors have demonstrated their interest.45,46
Conclusion and perspectives
The influence of lifestyle factors (physical activity, BMI, sleep problems, and smoking habits) on the prognosis of pain patients in pain in primary care was smaller than expected. More longitudinal studies are needed to clarify their role.
Conversely, GSRH might be an interesting predictive factor in this setting. Subjects evaluating their global health probably integrate several objective and subjective variables such as existing diseases, lifestyle, representations and beliefs about health and pain, emotions or occupational factors. Therefore, in a clinical setting, patients reporting low GSRH should be assessed in detail to identify individual risk factors that could be the target of specific (multimodal) interventions.
Supplemental Material
Supplemental Material - Do lifestyle factors influence pain prognosis? A 1-year follow-up study
Supplemental Material for Do lifestyle factors influence pain prognosis? A 1-year follow-up study by Marc-Henri Louis, Anne Berquin and Arnaud Steyaert in British Journal of Pain
Footnotes
Author contributions
AS and AB participated in protocol design, data extraction, data analyses, and manuscript preparation. MHL participated in data analyses and manuscript preparation. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the local medical ethics committee of the Université Catholique de Louvain (2018/19JUI/258). We certify that that this work has not been published previously, that it is not under consideration for publication elsewhere, that its publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the MHL is supported by a grant from the Fondation Saint-Luc [grant number: 326E].
Informed consent
Each participant provided written informed consent.
Trial registration
The study was not registered because it is an observational study.
Guarantor
AS but corresponding author is MHL
Article type
Observational cohort studies. We followed the STROBE guidelines.
Supplemental material
Supplemental material for this article is available online
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.