
Abstract
Background:
Early intra-abdominal infections (EIAIs) are among the most frequent and life-threatening complications following liver transplantation (LT). Early identification of high-risk patients remains challenging, and no standardized risk stratification tool is currently available.
Objective:
To develop and externally validate interpretable machine learning (ML) models for preoperative and postoperative prediction of EIAIs after LT.
Design:
A multicenter retrospective cohort study.
Methods:
A total of 363 adult LT recipients were included (Center 1: n = 285; Center 2: n = 78). EIAIs were defined as intra-abdominal infections occurring within 30 days after LT. From 120 candidate variables, predictors were selected using random forest, LASSO regression, and univariate logistic regression. Seven ML algorithms were evaluated, and stacking ensemble models were selected as the final preoperative (pre-liver transplantation early intra-abdominal infection forecast tool (LIFT)) and postoperative (post-LIFT) models. Internal testing and external validation were performed. Model interpretability was assessed using SHapley Additive exPlanations (SHAP).
Results:
The stacking models demonstrated superior performance. For pre-LIFT, the areas under receiver operator characteristic curve (ROC) curves (AUCs) were 0.995 ± 0.004 (training), 0.818 ± 0.056 (testing), and 0.796 ± 0.024 (external validation). For post-LIFT, AUCs were 0.996 ± 0.003, 0.847 ± 0.055, and 0.858 ± 0.026, respectively. Both models significantly outperformed model for end-stage liver disease and Child-Turcotte-Pugh scores (all p < 0.05). SHAP analysis revealed that baseline liver dysfunction, inflammatory markers, and immune status were key determinants in the pre-LIFT model, whereas perioperative factors such as intraoperative blood loss, ICU stay, and drainage duration predominated in the post-LIFT model.
Conclusion:
We developed and externally validated interpretable ML-based models (LIFT) for predicting EIAIs after LT. These models enable individualized risk stratification at both preoperative and postoperative stages and may support personalized infection surveillance and management strategies. Prospective validation is warranted.
Plain language summary
Liver transplantation can save the lives of people with severe liver disease, but infections in the abdomen are a common and dangerous problem soon after surgery. These infections can be hard to detect early because symptoms are often unclear, and test results may take time. Doctors often use broad antibiotics to prevent infections, but this can lead to side effects and antibiotic resistance. In this study, we used artificial intelligence-based methods, known as machine learning, to help predict which patients are most likely to develop early abdominal infections after liver transplantation. We collected information from 285 transplant patients at Beijing Friendship Hospital between 2020 and 2024 and 78 patients from Tianjin First Central Hospital. The information included patient characteristics, blood test results, and details from the surgery and recovery period. Two artificial intelligence models were developed: one that predicts infection risk before the operation (called pre-LIFT) and one that predicts risk after surgery (post-LIFT). These models combined data from several advanced algorithms and showed high accuracy in identifying patients at risk. Important factors included whether the patient had a repeat transplant, blood albumin and bilirubin levels, lymphocyte count, and how long the surgical drain remained in place. By using these models, doctors can better identify high-risk patients before and after surgery. This will allow them to adjust antibiotic use, monitor patients more closely, and provide care that matches each patient’s needs. This study provides interpretable artificial intelligence models (LIFT) for predicting early abdominal infections after liver transplantation. It supports more personalized prediction and may help reduce complications and improve patient recovery.
Keywords
Introduction
Liver transplantation (LT) has become a well-established therapeutic option for patients with advanced liver disease, particularly those with decompensated cirrhosis or specific hepatic complications and malignancies.1,2 With advances in surgical techniques and perioperative management, survival after LT has improved significantly. 3 However, postoperative complications remain a major determinant of prognosis. Among these, infections, particularly intra-abdominal infections, are the most common complications after LT and continue to exert a substantial impact on both patient and graft survival.4–6 Infections occur predominantly during the early postoperative period, and those occurring within the first month after LT are collectively referred to as early intra-abdominal infections (EIAIs). 4 Infections account for nearly 50% of all deaths occurring within the first year following LT. 7 Among these, intra-abdominal infections represent the leading cause, responsible for approximately 60% of infection-related mortality in LT recipients. 6 Therefore, reducing the incidence of EIAIs is crucial for improving outcomes in LT recipients.
The underlying liver diseases, the use of immunosuppressive medications, and the procedural complexity of transplantation contribute to a higher incidence of EIAIs, which are primarily caused by bacterial and fungal pathogens.7,8 Establishing a timely diagnosis of EIAIs after LT is challenging. In immunosuppressed patients, clinical symptoms and laboratory findings are often nonspecific. Up to 40% of infections, particularly fungal infections, may occur without fever, while up to 22% of febrile episodes are of noninfectious origin. 9 Moreover, the gold-standard microbial cultures often require considerable time, leading to substantial delays in diagnosis and, consequently, in the initiation of appropriate therapy. 10 Consequently, prophylactic antimicrobial therapy, often comprising multiple antibiotics, is commonly administered after LT, typically on an empirical basis, and has generally proven effective. However, adverse effects of antimicrobial therapy occur more frequently in transplant recipients, and interactions between antimicrobials and immunosuppressive drugs, as well as inappropriate antibiotic use, can result in high-mortality multidrug-resistant bacterial infections.11,12 These challenging issues underscore the urgent need for more refined and individualized antimicrobial strategies.5,11,13
Early identification and accurate prediction of the risk of EIAIs after LT are crucial for developing individualized management strategies and improving transplant outcomes. Despite the identification of established risk factors for EIAIs, methods for early risk prediction remain suboptimal. No standardized risk stratification framework has been developed, and conventional regression-based models may not adequately account for the complex, high-dimensional, and nonlinear interactions that drive the onset of EIAIs.7,11,14,15 Artificial intelligence (AI) approaches have recently emerged as a powerful tool for medical prognostication, especially in the context of transplantation, where they are capable of integrating multidimensional perioperative data to generate individualized risk predictions.16–18 Machine learning (ML) methods offer advantages over conventional statistical approaches by capturing complex, nonlinear relationships and providing insights through feature importance evaluations.16,17 These capabilities are particularly valuable in the context of LT, where they can facilitate individualized risk prediction and stratification of EIAIs, thereby supporting timely detection, personalized prognostic evaluation, and optimized therapeutic decision-making.
Therefore, the present study developed and validated a robust and clinically applicable ML-based prediction model with integrated model interpretability for EIAIs following LT, supporting personalized perioperative management and ultimately improving post-transplant outcomes. Liver Transplantation Early Intra-abdominal Infection Forecast Tool (LIFT) was constructed: a preoperative model, which utilized variables available before transplantation to estimate EIAI risk. The preoperative model is applied before LT to guide preoperative optimization and inform induction immunosuppression strategies, whereas the postoperative model integrates intraoperative and postoperative data to more precisely predict EIAI risk and support early postoperative antimicrobial prophylaxis and immunosuppressive adjustment.
Methods
Patients and data
A total of 328 adult patients underwent LT at Beijing Friendship Hospital (Center 1) between February 2020 and April 2024. All adult (⩾18 years) recipients of a primary or retransplant LT during the study period were eligible for inclusion. All patients underwent comprehensive preoperative infection screening to identify both overt and occult infections. The diagnostic evaluation employed an integrative, multimodal approach incorporating clinical symptoms, physical examination findings, and imaging assessments, supplemented by pathogen-specific detection methods, including molecular diagnostics, conventional microbial cultures, and metagenomic next-generation sequencing (mNGS). 19 To further improve the detection of subclinical infections, inflammatory markers were routinely monitored, whole-body imaging was systematically performed, and polymerase chain reaction testing for respiratory viruses was conducted. In addition, serological testing for Epstein–Barr virus and cytomegalovirus was carried out, along with microbiological cultures of specimens such as anal swabs, sputum, ascitic fluid, and bile. A total of 43 patients were excluded for the following reasons: incomplete clinical data (n = 15), preexisting infections before LT (n = 24), donor-derived infections (n = 2), and multiple organ transplantation (n = 2). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement and Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD).20,21
The patient selection flowchart is presented in Figure 1. All consecutive adult patients who met the inclusion criteria during the study period were included. No monetary or non-monetary incentives were provided. The sample size was determined by the available cohort, and no formal power calculation was performed due to the retrospective nature of the study. Ultimately, 285 patients fulfilled the eligibility criteria and were included in the final analysis, forming the training and test sets. In addition, an independent cohort of 78 patients from Tianjin First Central Hospital (Center 2), enrolled between November 2024 and December 2025 under the same inclusion and exclusion criteria, was included as the external validation set. Patient data included demographic characteristics, clinical information, laboratory results obtained one day before LT, as well as intraoperative and postoperative variables.
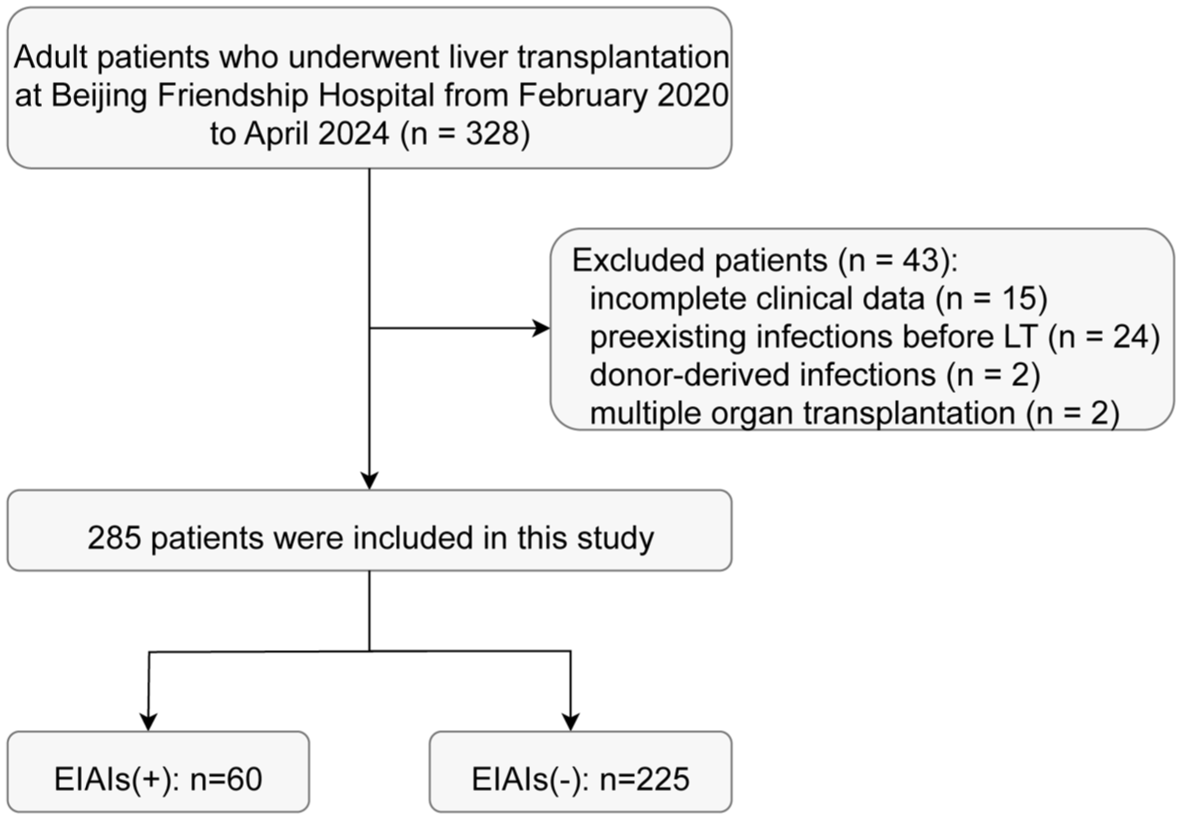
Flowchart of patient selection and exclusion criteria for the study cohort.
Definition and diagnostic criteria of EIAIs
EIAIs were defined as those occurring within the first 30 days after LT. The diagnostic criteria for EIAIs were as follows: (1) Clinical manifestations of acute abdominal pain accompanied by local and/or systemic signs of inflammation; and/or (2) imaging findings (ultrasound, CT, and MRI) suggesting an intra-abdominal infectious focus.22,23 Negative microbiological results do not exclude infection. 24 Microbiological evidence, when available, was obtained from peritoneal drainage fluid or percutaneous aspiration specimens and included positive conventional cultures and/or pathogen identification by mNGS.19,24 The LT population represents a complex clinical setting in which immunosuppression often blunts typical signs and symptoms of infection, leading to atypical presentations. Therefore, infections were not further subclassified. The diagnosis of EIAIs was based on a comprehensive assessment integrating clinical manifestations, laboratory and imaging findings, and microbiological evidence when available.22,23,25 This composite approach reflects real-world practice and improves diagnostic accuracy in this immunocompromised population (see Supplemental Table S1 for details).
Surgical and perioperative management
All LT surgeries were performed by the surgical teams at each participating center. After surgery, all recipients received intensive care in the transplant care unit. Immunosuppressive induction therapy with basiliximab was administered selectively according to the patient’s condition. The postoperative immunosuppressive regimen mainly consisted of tacrolimus (initial dose 0.05–0.10 mg/kg/day, adjusted according to target trough concentrations at different postoperative stages), methylprednisolone (initial intravenous dose 4–5 mg/kg/day, gradually tapered and converted to oral methylprednisolone at 5–10 mg/day by postoperative day 7), and mycophenolate mofetil (0.50–0.75 g twice daily). The dosages of immunosuppressants were individualized based on infection status and rejection episodes.
All recipients received empirical antimicrobial therapy postoperatively. For recipients of livers donated after cardiac death or brain death, the prophylactic antimicrobial regimen generally consisted of a combination of meropenem or imipenem, vancomycin, and micafungin. For living donor LT recipients, third-generation cephalosporins or carbapenems were routinely used for prophylactic antimicrobial therapy. Antibiotic therapy was subsequently de-escalated based on the clinical course and culture results.
Peritoneal drainage fluid was routinely collected for culture within 24 h after LT, every 2–3 days during post-LT days 1–7, and once or twice weekly thereafter until drain removal. In cases of confirmed EIAIs, drainage cultures or mNGS were repeatedly obtained as clinically indicated to identify the causative pathogens and to monitor the response to antimicrobial therapy.
Statistical analysis
The AI models were developed in three main steps. First, baseline characteristics were compared between the infected and non-infected groups. Variables showing statistically significant differences (p < 0.05) were identified as candidate predictors. All preprocessing steps, including normalization and feature selection, were performed exclusively within the training set and subsequently applied to the test and validation cohorts. For model development, the dataset (Center 1, n = 285) was randomly split into training and test sets at a 7:3 ratio. Second, feature selection was performed exclusively within the training set to prevent data leakage. Three complementary variable selection approaches were applied: random forest (RF), LASSO regression, and univariate logistic regression (LR). For the RF, variables with a non-zero decrease in Gini impurity were retained; for LASSO regression, predictors with non-zero coefficients were selected; and for LR, variables with statistical significance were included. Predictors identified by at least two of the three methods were integrated and retained as the final feature set for constructing both the preoperative and postoperative models. Third, seven ML algorithms were independently employed to develop predictive models, including LR, RF, extreme gradient boosting (XGBoost), support vector machine (SVM), neural network (NNET), AdaBoost (homogeneous ensemble learning), and stacking (heterogeneous ensemble learning). We add AdaBoost to each machine learning model, including LR, SVM, and NNET, to reveal the ensemble learning’s effect on performance improvement. Model performance was systematically compared across algorithms. The best-performing models, based on discrimination and calibration metrics, were selected as the final predictive models for the preoperative (pre-LIFT) and postoperative (post-LIFT) stages. The entire modeling procedure, including feature selection and model training, was repeated 1000 times. After each iteration, all intermediate variables and models were cleared to minimize potential information leakage, and performance metrics were summarized as mean ± standard deviation. Center 2, an independent external validation cohort, was subsequently used to evaluate model generalizability and was not involved in any stage of model construction. Considering the commonly recommended sample size requirement of 8–10 events per predictor variable, up to 20 variables could be accommodated in the training set. Accordingly, 8 and 12 predictors were included in the pre-LIFT and post-LIFT models, respectively. All analyses were conducted using R software (version 4.2, https://cran.r-project.org/), and a two-sided p value < 0.05 was considered statistically significant.
Results
Patient characteristics
The study included 363 liver transplant patients: 285 from Center 1 (training/test) and 78 from Center 2 (external validation). Overall cohort: 64.2% male, mean age 50.8 ± 12.3 years, laboratory MELD 13.7 ± 7.9. Main etiologies: liver cancer (32.5%), HBV (20.7%). Center 2 patients had more severe disease than Center 1, with higher rates of moderate/severe ascites (37.2% vs 18.2%), gastrointestinal bleeding (30.8% vs 13.7%), hepatic encephalopathy (29.5% vs 17.2%), and significantly elevated laboratory MELD, lactic acid, INR, and CRP (all p < 0.05, see Table 1 and Supplemental Table S2).
Characteristics and clinical information of patients with and without early intra-abdominal infections in center 1.
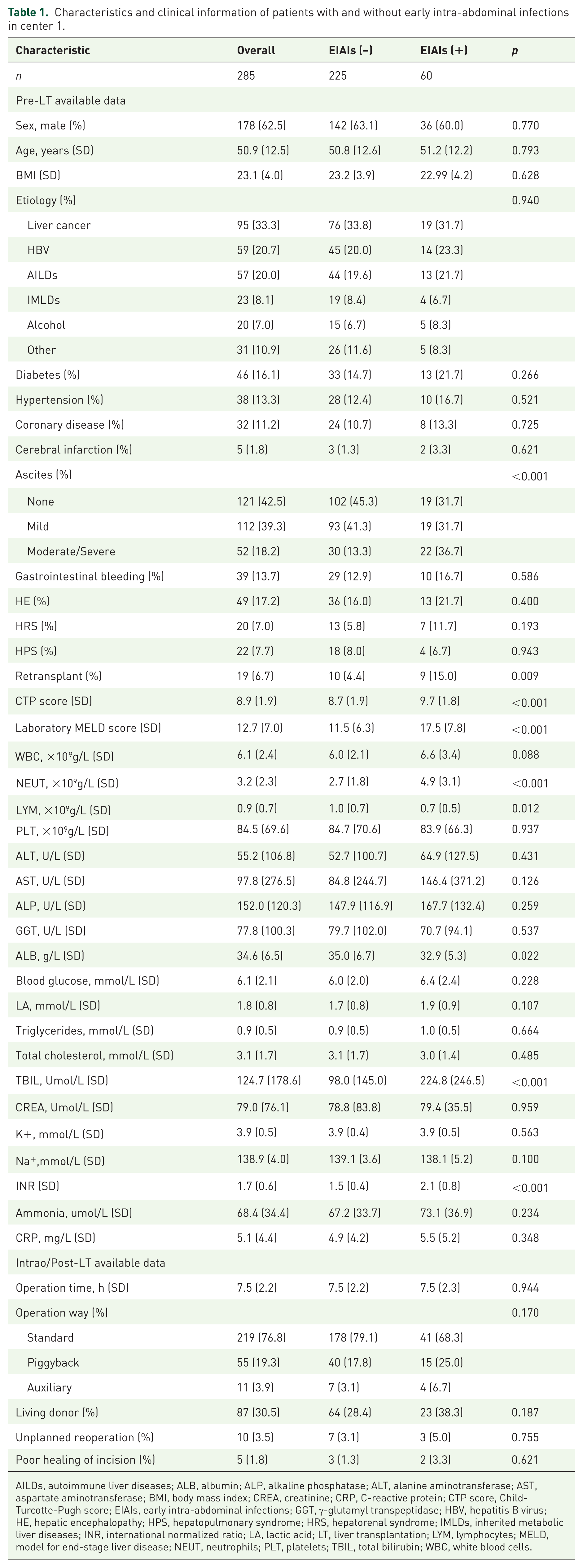
AILDs, autoimmune liver diseases; ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; CREA, creatinine; CRP, C-reactive protein; CTP score, Child-Turcotte-Pugh score; EIAIs, early intra-abdominal infections; GGT, γ-glutamyl transpeptidase; HBV, hepatitis B virus; HE, hepatic encephalopathy; HPS, hepatopulmonary syndrome; HRS, hepatorenal syndrome; IMLDs, inherited metabolic liver diseases; INR, international normalized ratio; LA, lactic acid; LT, liver transplantation; LYM, lymphocytes; MELD, model for end-stage liver disease; NEUT, neutrophils; PLT, platelets; TBIL, total bilirubin; WBC, white blood cells.
Screening clinicopathologic variables
Factors were categorized into preoperative and postoperative variables, as presented in Table 1. From a total of 120 candidate variables, the top 8 and 12 predictors were identified for the pre-LIFT and post-LIFT models, respectively (Figure 2(a)–(f)). Figure 2 illustrates the relative importance of each variable within the corresponding feature selection methods.
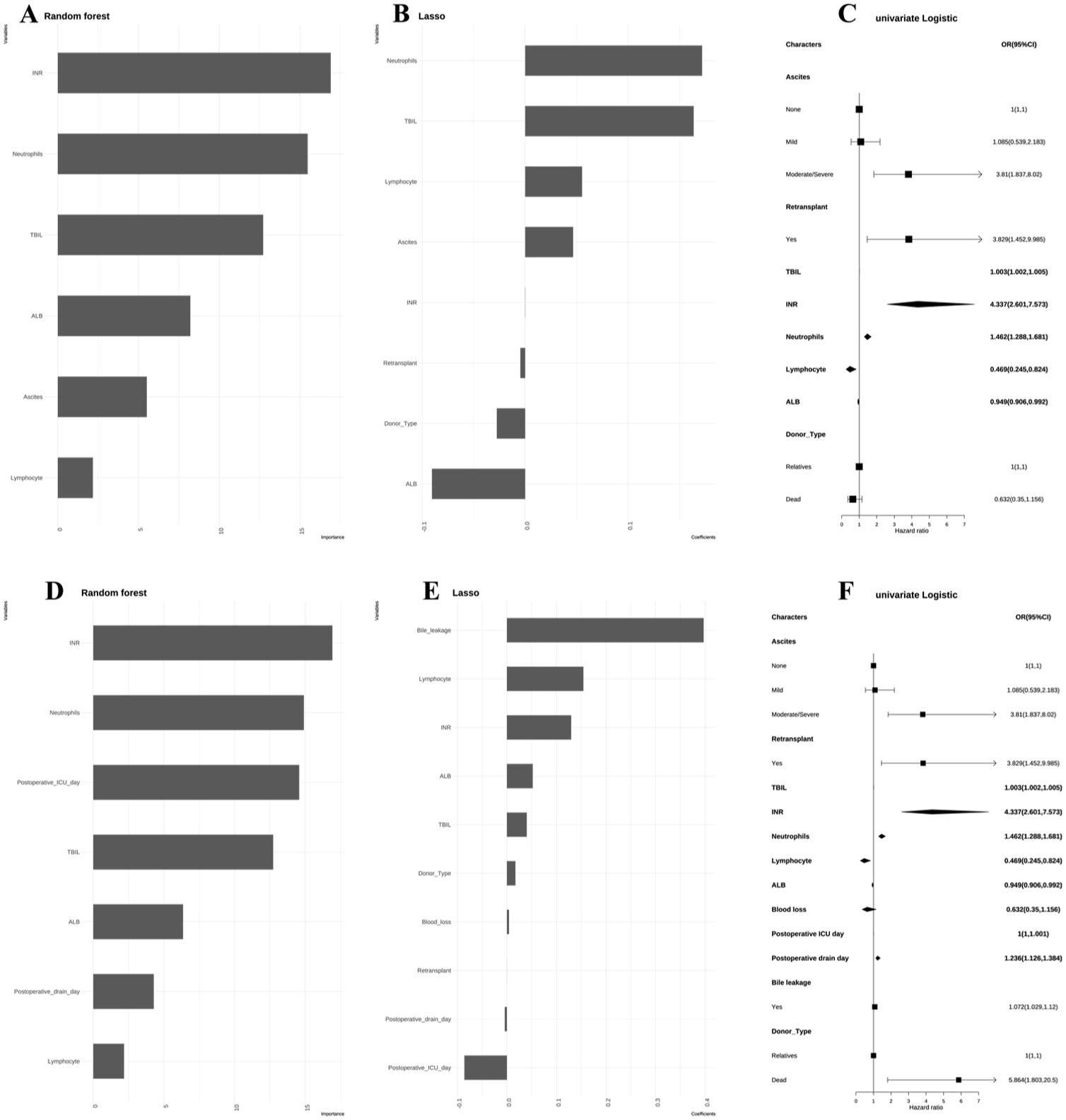
Identification of key predictive features for the pre-LIFT and post-LIFT models using three feature selection approaches (random forest, LASSO regression, and univariate logistic regression). (a–c) Pre-LIFT variable importance and (d–f) Post-LIFT variable importance.
Construction and evaluation of predictive EIAIs models
We subsequently developed predictive models for EIAIs using seven ML algorithms, as summarized in Table 2. Among these, the stacking models demonstrated the best performance and were ultimately selected as the LIFT. After training, testing, and external validation, the AUCs of the pre-LIFT model were 0.995 ± 0.004, 0.818 ± 0.056, and 0.796 ± 0.024, respectively. Correspondingly, the post-LIFT model achieved AUCs of 0.996 ± 0.003, 0.847 ± 0.055, and 0.858 ± 0.026. Both the pre-LIFT and post-LIFT models enabled individualized risk estimation, with higher predicted scores corresponding to an increased risk of EIAIs. Patients were stratified into high- and low-risk groups based on optimal cutoffs derived from the training set’s Youden index (0.199 for pre-LIFT and 0.347 for post-LIFT). Calibration curves and additional performance details are presented in Figures S1–S3. In the external validation cohort, both the pre-LIFT (Figure 3(a)) and post-LIFT (Figure 3(b)) models were further compared with the Child-Turcotte-Pugh score (CTP) and the MELD score, showing superior discriminatory performance of the LIFT models.
Comparison of machine learning pre- and post-model performance in predicting early intra-abdominal infections (training, test, and external validation cohorts).
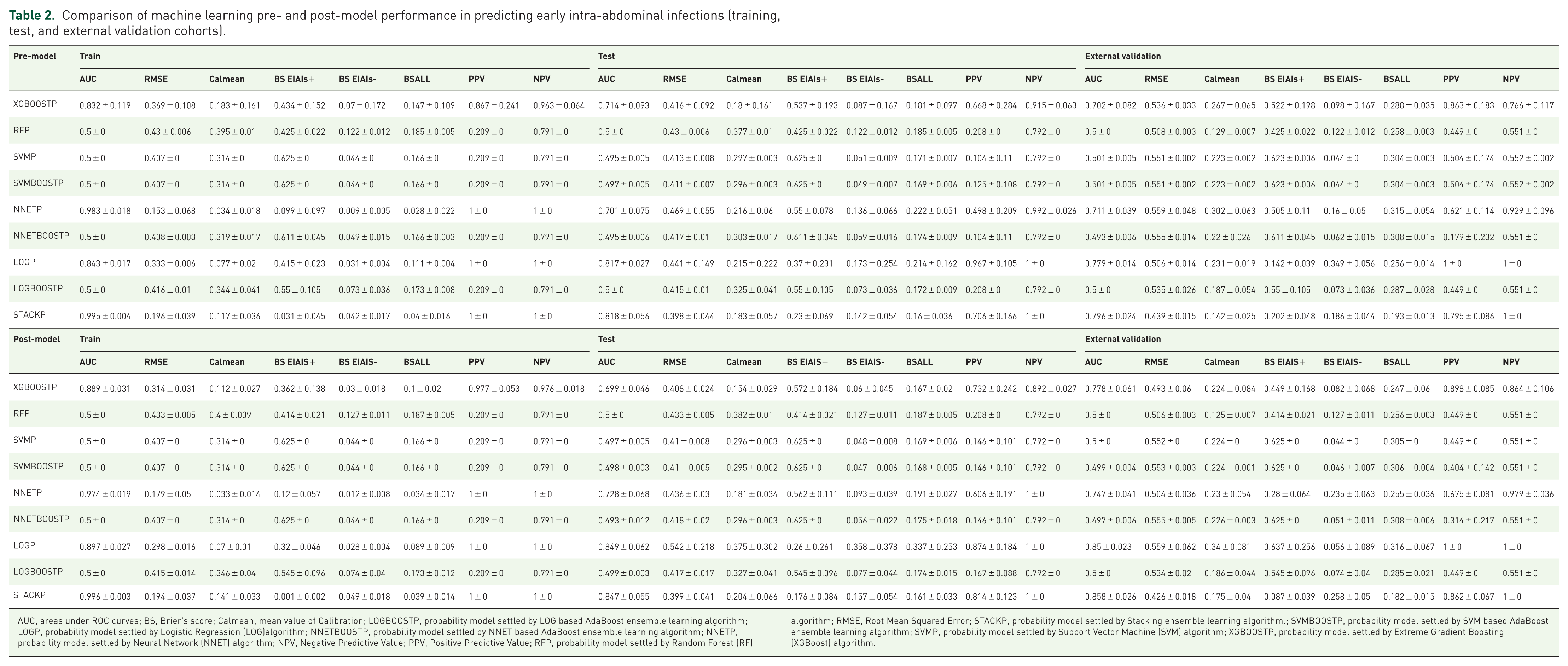
AUC, areas under ROC curves; BS, Brier’s score; Calmean, mean value of Calibration; LOGBOOSTP, probability model settled by LOG based AdaBoost ensemble learning algorithm; LOGP, probability model settled by Logistic Regression (LOG)algorithm; NNETBOOSTP, probability model settled by NNET based AdaBoost ensemble learning algorithm; NNETP, probability model settled by Neural Network (NNET) algorithm; NPV, Negative Predictive Value; PPV, Positive Predictive Value; RFP, probability model settled by Random Forest (RF) algorithm; RMSE, Root Mean Squared Error; STACKP, probability model settled by Stacking ensemble learning algorithm.; SVMBOOSTP, probability model settled by SVM based AdaBoost ensemble learning algorithm; SVMP, probability model settled by Support Vector Machine (SVM) algorithm; XGBOOSTP, probability model settled by Extreme Gradient Boosting (XGBoost) algorithm.
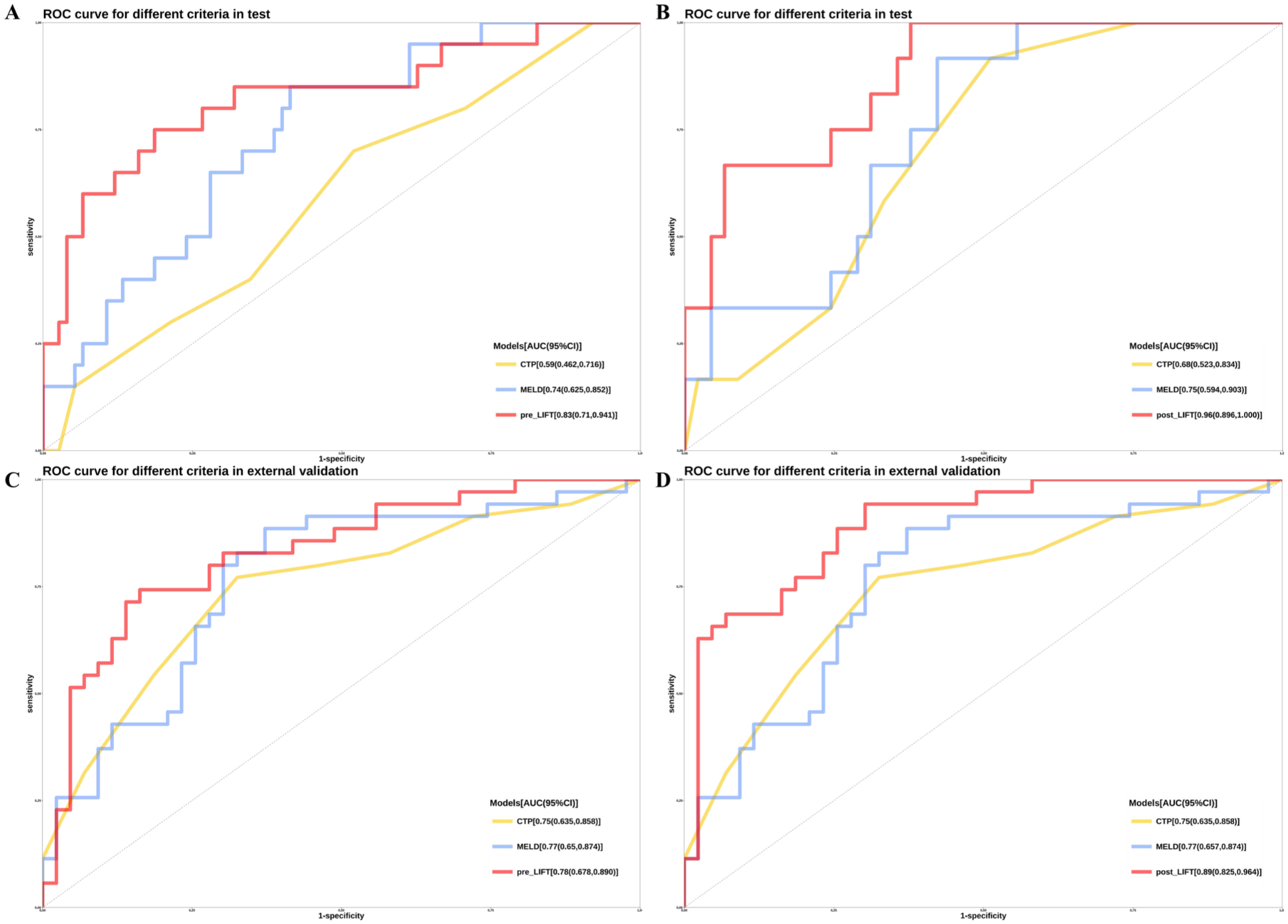
Receiver operator characteristic curve(ROC) curve comparison of LIFT models with conventional scoring systems in the testing and validation set. (a) Pre-LIFT versus CTP and MELD scores in testing set (b) Post-LIFT versus CTP and MELD scores in testing set (c) Pre-LIFT versus CTP and MELD scores in extermal validation set and (d) Post-LIFT versus CTP and MELD scores in external validation set.
Furthermore, we analyzed 30-day EIAIs-free survival curves for high- and low-risk groups across the training (Figure 4(a) and (b)), test (Figure 4(c) and (d)), and external validation cohorts (Figure 4(e) and (f)), applying the cutoffs derived from the training set; these results demonstrate that the LIFT models effectively stratify patients into distinct risk categories.
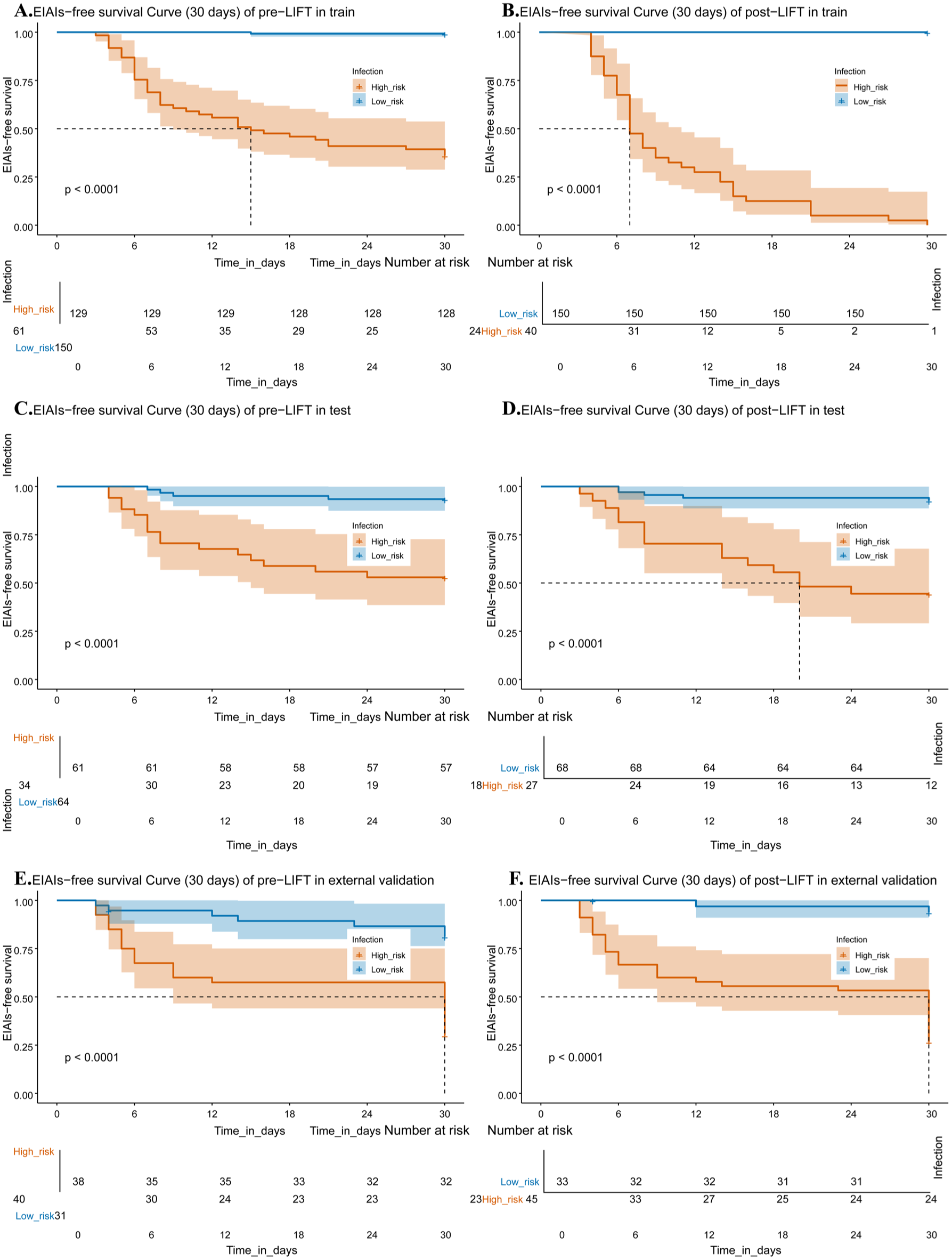
Kaplan–Meier curves for 30-day EIAIs-free survival in the training (a, b), test (c, d), and external validation cohorts (e, f), stratified by risk groups using cutoffs derived from the training set. The LIFT models demonstrated significant discrimination between high- and low-risk patients across all cohorts.
In addition, DeLong’s tests were performed to compare the AUCs between the LIFT models and conventional clinical scores. For the preoperative model, significant differences were observed in the test set (CTP vs pre-LIFT: Z = −2.86, p = 0.004; pre-LIFT vs MELD: Z = 2.06, p = 0.039) and were confirmed in the external validation cohort (CTP vs pre-LIFT: Z = −2.90, p = 0.0037; pre-LIFT vs MELD: Z = 2.21, p = 0.027). Similarly, for the postoperative model, statistically significant improvements were found in the test set (CTP vs post-LIFT: Z = −3.16, p = 0.002; post-LIFT vs MELD: Z = 3.23, p = 0.001) and in the external validation cohort (CTP vs post-LIFT: Z = −3.70, p < 0.001; post-LIFT vs MELD: Z = 2.64, p = 0.008).
Predicted risk scores were calculated for all patients using the pre-LIFT model, and the optimal cut-off value (0.199) was determined based on Youden’s index derived from the training set. Patients were subsequently stratified into high- and low-risk groups. At this predefined threshold, the model demonstrated a sensitivity of 0.80, specificity of 0.76, positive predictive value (PPV) of 0.471, and negative predictive value (NPV) of 0.934 in the test set. In the external validation cohort, the corresponding values were 0.80, 0.721, 0.70, and 0.816, respectively.
Similarly, for the post-LIFT model, the optimal cut-off value (0.347) was determined using Youden’s index derived from the training set, and patients were subsequently stratified into two risk groups. At this predefined threshold, the model achieved a sensitivity of 0.75, specificity of 0.84, PPV of 0.556, and NPV of 0.926 in the test set. In the external validation cohort, the corresponding values were 0.943, 0.721, 0.733, and 0.939, respectively. Detailed LIFT models are provided in https://LIFT.aean.net/.
SHAP-based interpretability analysis of the pre-LIFT and post-LIFT models
To enhance transparency and facilitate clinical interpretability, SHapley Additive exPlanations (SHAP) were applied to both the pre-LIFT and post-LIFT models to quantify the contribution of each predictor to the risk of EIAIs (Figures 5 and 6).
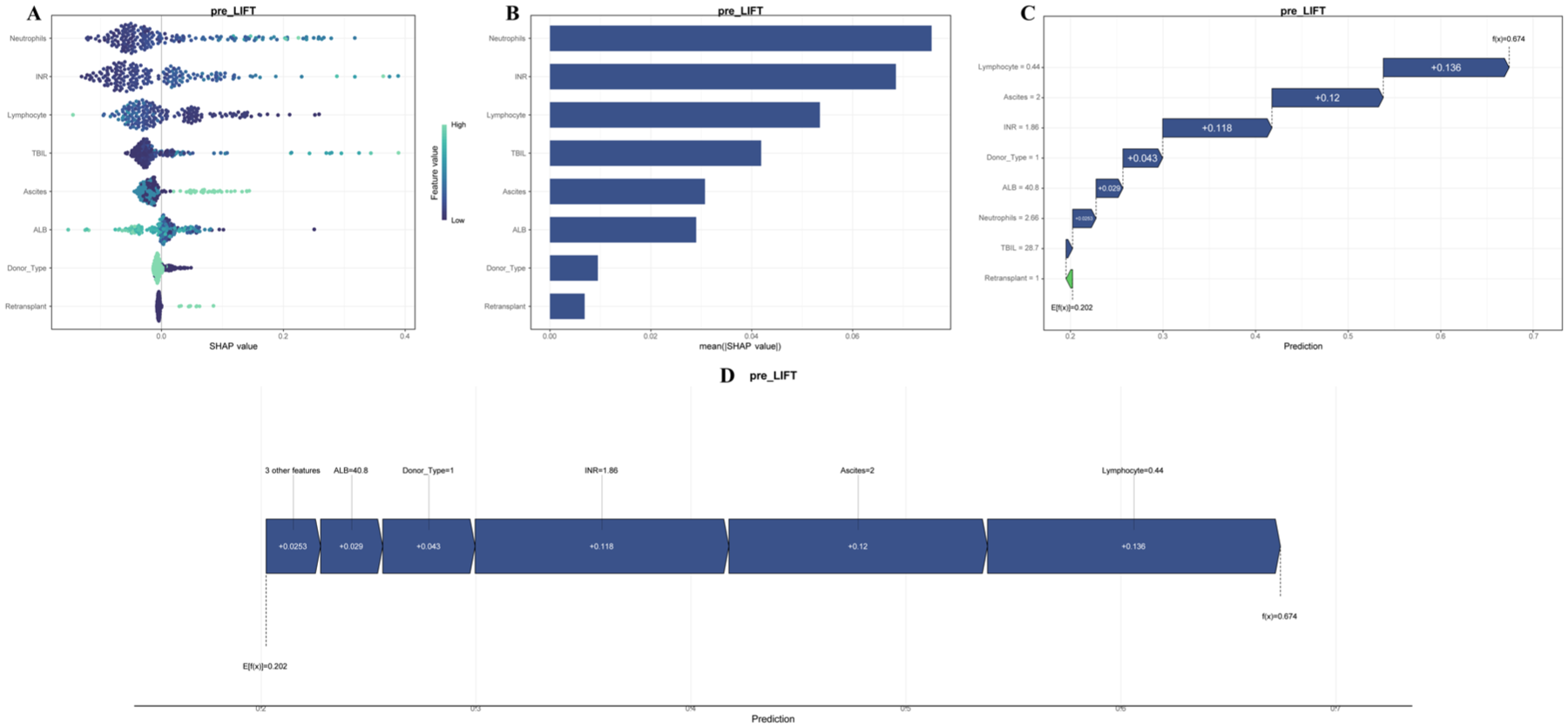
SHAP interpretability analysis of the pre-LIFT model based on preoperative variables. Baseline liver function, inflammatory status, and host immunity are key determinants of infection risk in the pre-LIFT model. (a) SHAP summary plot. Each row represents one preoperative variable and each dot represents an individual patient. The x-axis shows the SHAP value, which quantifies the contribution of that variable to the predicted infection probability. Positive values (right side) indicate increased risk, whereas negative values (left side) indicate decreased risk. Dot color reflects the original feature magnitude (red = high value; blue = low value). Variables are ordered from top to bottom according to their overall importance. Liver dysfunction markers, inflammatory indices, and impaired nutritional or immune parameters predominantly show positive risk contributions, whereas favorable baseline conditions demonstrate protective effects. (b) Mean absolute SHAP value bar plot. Displays the average magnitude of SHAP values for each variable across all patients, providing a quantitative ranking of feature importance. Larger bars indicate stronger global influence on model predictions. (c, d) Individual force plot. Shows patient-specific prediction decomposition. Starting from the baseline risk, red segments represent variables that increase predicted infection probability, and blue segments represent protective variables. The cumulative effects determine the final output.
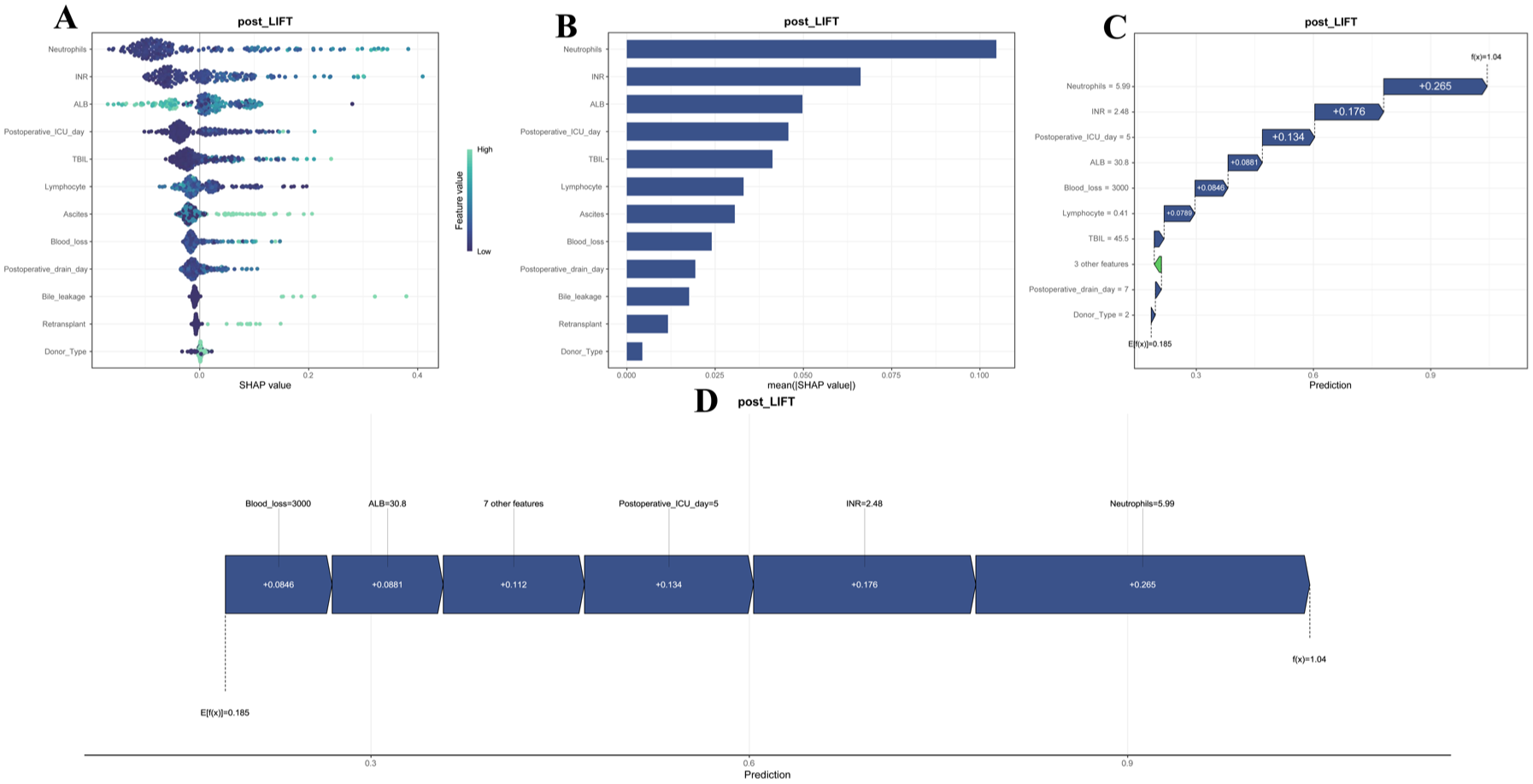
SHAP interpretability analysis of the post-LIFT model incorporating both preoperative and postoperative variables. Perioperative and postoperative clinical events are the primary drivers of early infection development in the post-LIFT model. (a) SHAP summary plot. Each dot corresponds to one patient and each row represents a predictor. The horizontal position indicates the SHAP value (magnitude and direction of contribution). Positive values increase predicted infection risk, while negative values reduce risk. Dot color denotes the feature magnitude (red = high; blue = low). Variables are ranked by importance. Postoperative and perioperative variables show larger SHAP distributions, indicating stronger predictive effects. (b) Mean absolute SHAP value bar plot. Quantifies the relative importance of all predictors. Compared with the pre-LIFT model, postoperative variables exhibit higher mean absolute SHAP values, suggesting a greater impact on model output. (c and d) Individual force plot. Provides a case-specific explanation. Risk-promoting variables such as greater surgical trauma, prolonged invasive support, or delayed recovery appear as red segments that shift the prediction upward, while protective variables appear in blue and shift the prediction downward.
In the pre-LIFT model, the SHAP summary plot demonstrated that several preoperative clinical and laboratory variables exerted substantial influence on infection risk. Features related to liver dysfunction and systemic inflammation showed predominantly positive SHAP values, indicating increased predicted probabilities of EIAIs. In particular, elevated total bilirubin, prolonged coagulation parameters (e.g., increased INR), and neutrophil-predominant inflammatory markers were associated with higher risk contributions. Conversely, indicators reflecting better physiological reserve, such as higher albumin levels and preserved lymphocyte counts, tended to exhibit negative SHAP values and were associated with lower predicted infection risk.
The SHAP bar plot further confirmed the relative importance of these features, with liver function indices, nutritional markers, and immune cell counts ranking among the top contributors. These findings indicate that baseline hepatic function, inflammatory status, and host immunity are major determinants of postoperative infection susceptibility even before surgery.
After incorporating perioperative and postoperative information, the post-LIFT model showed a marked shift in feature importance. The SHAP summary plot revealed that postoperative management and surgery-related variables contributed more prominently to the prediction. Variables such as greater intraoperative blood loss, longer postoperative drainage duration, and prolonged intensive care unit (ICU) stay exhibited large positive SHAP values, indicating strong associations with increased infection risk. These variables consistently pushed predictions toward higher probabilities of EIAIs.
In contrast, indicators of favorable recovery or less invasive postoperative courses showed negative SHAP contributions, suggesting protective effects. Compared with the pre-LIFT model, the magnitude of SHAP values for postoperative variables was generally larger, demonstrating their stronger influence on early infection outcomes.
Force plots for representative patients illustrated how multiple variables jointly influenced the final prediction. Risk-enhancing factors cumulatively increased the predicted probability, whereas protective variables reduced it. These patient-specific explanations provided intuitive visualization of the additive decision process underlying the models.
Overall, the SHAP analyses identified distinct patterns of risk determinants: preoperative physiological status predominated in the pre-LIFT model, whereas perioperative and postoperative factors played a dominant role in the post-LIFT model.
Discussion
In this study, to our knowledge, we developed and validated the first ML–based prognostic models for EIAIs applicable to both the pre- and post-transplant stages. The pre-LIFT model, based on readily available preoperative data, may enable early risk stratification and assist in preoperative optimization as well as in planning immunoinduction strategies. The post-LIFT model, incorporating intraoperative and postoperative variables, provides an individualized risk assessment that may support clinicians in tailoring antimicrobial and immunosuppressive regimens, facilitating shared decision-making, and enhancing infection surveillance. The models have the potential to support improved postoperative outcomes by identifying high-risk patients who may benefit from tailored interventions. However, further validation is warranted.
LIFT provides a novel perspective for understanding EIAIs. The risk of severe infections in transplant recipients is shaped by the interplay between a patient’s epidemiological exposures and their overall state of immunosuppression. Notably, the variables incorporated into LIFT primarily reflect three key dimensions: the severity of the underlying liver disease, the patient’s immune status, and the extent of postoperative microbial exposure. Ascites represents a hallmark of hepatic decompensation and is commonly accompanied by electrolyte imbalance. Beyond serving as a marker of disease severity, ascites predisposes patients to intra-abdominal infections by providing a favorable environment for bacterial translocation and growth, thereby contributing to poorer survival outcomes in patients with advanced liver disease. 26 Ascites, elevated INR, hypoalbuminemia, and hyperbilirubinemia constitute key components of widely used prognostic scoring systems.27,28 Their incorporation into these validated models underscores their ability to reflect hepatic functional reserve, quantify disease severity, and predict patient survival.29–34 INR, a key indicator of hepatic synthetic function, indirectly reflects impaired liver functional reserve in patients with cirrhosis; elevated INR levels are associated with clinically significant portal hypertension, and an INR ⩾ 1.5 is widely recognized as one of the diagnostic criteria for liver failure.35,36 Furthermore, albumin directly affects the efficacy of antimicrobial therapy through its binding capacity. 37 Although hypoalbuminemia was not significantly associated with an increased risk of intra-abdominal infection in our cohort, we retained this variable given its established clinical relevance and its recognized role as an indicator of hepatic dysfunction and overall nutritional status.
Hyperbilirubinemia has also been reported to show the expansion of immunosuppressive regulatory T cells, thereby contributing to impaired host defense and increased susceptibility to bacterial infections in patients with liver cirrhosis. 38 Neutrophils serve as the first line of defense against infection, while neutrophilia and lymphopenia are common immunological alterations reflecting disruption of the host immune system.39,40 Increasing evidence suggests that lymphopenia, involving depletion of T, B, and natural killer cells, commonly develops during sepsis and leads to immunoparalysis, thereby impairing host defense; consequently, a high neutrophil-to-lymphocyte ratio (NLR) has been linked to worse outcomes and higher sepsis-related mortality. 41 Patients undergoing retransplantation are at particularly high risk of infection owing to cumulative immunosuppression and increased surgical complexity. Extensive intra-abdominal adhesions prolong operative time and necessitate greater hepatobiliary manipulation, thereby heightening perioperative complication rates and microbial exposure.42,43 Consistently, previous studies have reported that infection represents a major cause of mortality following re-transplantation. 44 Deceased-donor liver transplantation (DDLT) has been associated with a higher risk of infection compared with living-donor liver transplantation (LDLT).13,45 This disparity may be explained by the poorer baseline condition and higher MELD scores of DDLT recipients, as well as the limited time and technology available for donor infection screening.46,47
The volume of intraoperative hemorrhage may reflect surgical complexity and prolonged operative exposure, thereby increasing opportunities for pathogen contamination. Moreover, excessive blood loss can lead to severe immune dysfunction and heightened susceptibility to infection. 48 Extended ICU stay often indicates slower recovery and more severe clinical status, and is associated with increased cumulative exposure to hospital-acquired pathogens, especially multidrug-resistant organisms.49,50 Moreover, drainage tubes compromise the natural skin and mucosal barriers, providing direct entry routes for microorganisms and thereby predisposing patients to infection. Early removal of drainage tubes is important for reducing infectious complications within the first month after transplantation. 6 Bile leakage has been identified as a significant risk factor for postoperative infectious complications, and biliary tract complications have been shown to significantly increase mortality after liver transplantation. 6 Our findings suggest that surgical factors may play an important role in infection development, underscoring the potential value of minimizing intraoperative injury and reducing opportunities for microbial invasion.
The development of postoperative EIAIs is a complex process influenced by multiple interrelated factors. Modern ML algorithms—such as RF, gradient boosting, and support vector machines-can automatically capture nonlinear relationships, manage multicollinearity, and better simulate real-world clinical settings, thereby improving predictive accuracy and robustness.16,51 Our model represents a significant advancement over previously published models based on conventional statistical approaches, which rely on linear assumptions and often fail to capture the complex biological interactions underlying clinical outcomes.52–54
In this study, for the sake of transparency and to promote further investigation, we introduced ML methods and employed cross-validation, feature interpretation tools (such as SHAP), and external validation to overcome the limitations of conventional approaches. Although ML approaches can provide more powerful predictive models, their opacity-often referred to as the “black box”-poses a challenge in understanding the specific variables contributing to model predictions.55,56 Consequently, we developed LIFT models with potentially improved accuracy, stability, and interpretability for predicting the risk of EIAIs.
The LIFT models developed in this study may help facilitate individualized postoperative management according to different risk levels. Early identification and timely intervention play pivotal roles in achieving favorable outcomes for patients with intra-abdominal infections.5,11 However, in current clinical practice, the absence of specific and individualized post-LT surveillance protocols impedes the early diagnosis and management of intra-abdominal infections, resulting in considerable heterogeneity in patient outcomes.5,11 Antimicrobial agents are more likely to cause adverse effects in transplant recipients and may interact with immunosuppressive drugs. The prevalence of multidrug-resistant organisms is increasing.11,12 This challenge, among others, underscores the urgent need for individualized therapeutic strategies. To address these challenges, we explored the use of AI–based approaches to provide additional clinically relevant information for risk stratification. For patients identified as high-risk by the pre-LIFT model, clinicians might consider enhanced preoperative supportive care and optimized prophylactic antimicrobial therapy to theoretically improve clinical stability. Individualized immunoinduction strategies could also be explored for those with elevated baseline risk. The post-LIFT model further underscores the potential relevance of vigilant perioperative management, particularly regarding the minimization of intraoperative blood loss and meticulous biliary tract handling. While high-risk classification provides a rationale for intensified monitoring and tailored immunosuppression, we acknowledge that the therapeutic benefit of acting on these predictions remains to be proven. Rather than confirming improved outcomes, these models currently offer a statistical framework for risk stratification. Future prospective studies are essential to validate whether deploying these model-guided interventions translates to a tangible reduction in EIAI rates or improved patient survival.
This study has several limitations. First, as a retrospective cohort study, it is inherently subject to selection bias and residual confounding, which may not have been fully addressed despite strict inclusion criteria and multivariable adjustments. In addition, the relatively small sample size may limit statistical power and model generalizability. Second, although both internal and external validations were performed, prospective multicenter studies—such as large-scale cohort studies or interventional clinical trials—are still warranted to further assess the robustness, stability, and real-world clinical utility of the LIFT models, particularly to determine whether model-guided prophylactic strategies can translate into improved postoperative outcomes and reduced infection-related complications. Finally, bacterial infections constituted the majority of cases in our cohort, whereas fungal infections were relatively uncommon. Therefore, the applicability of the models to fungal infections remains uncertain, and further studies focusing on fungal infectious complications are needed for additional validation.
In summary, LIFT, as an interpretable ML‑based model, represents a substantial advance in predicting EIAIs after LT. The LIFT models offer a precise and practical tool for early risk prediction, providing valuable guidance for individualized diagnosis, prevention, and therapeutic decision-making in LT recipients. These strategies require further clinical validation.
Supplemental Material
sj-docx-4-tai-10.1177_20499361261453152 – Supplemental material for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study
Supplemental material, sj-docx-4-tai-10.1177_20499361261453152 for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study by Shuang Cao, Hua-Bin Peng, Xin-Zhe Wei, Lei Wang, Ying Liu, Wei Qu, Zhi-Gui Zeng, Hai-Ming Zhang, Lin Wei, Hao-Feng Xiong, Fei Hou, Zhi-Jun Zhu, Wei Gao and Li-Ying Sun in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-pdf-1-tai-10.1177_20499361261453152 – Supplemental material for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study
Supplemental material, sj-pdf-1-tai-10.1177_20499361261453152 for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study by Shuang Cao, Hua-Bin Peng, Xin-Zhe Wei, Lei Wang, Ying Liu, Wei Qu, Zhi-Gui Zeng, Hai-Ming Zhang, Lin Wei, Hao-Feng Xiong, Fei Hou, Zhi-Jun Zhu, Wei Gao and Li-Ying Sun in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-pdf-2-tai-10.1177_20499361261453152 – Supplemental material for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study
Supplemental material, sj-pdf-2-tai-10.1177_20499361261453152 for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study by Shuang Cao, Hua-Bin Peng, Xin-Zhe Wei, Lei Wang, Ying Liu, Wei Qu, Zhi-Gui Zeng, Hai-Ming Zhang, Lin Wei, Hao-Feng Xiong, Fei Hou, Zhi-Jun Zhu, Wei Gao and Li-Ying Sun in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-pdf-3-tai-10.1177_20499361261453152 – Supplemental material for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study
Supplemental material, sj-pdf-3-tai-10.1177_20499361261453152 for Interpretable machine learning models for pre- and postoperative prediction of early intra-abdominal infections after liver transplantation: a multicenter retrospective cohort study by Shuang Cao, Hua-Bin Peng, Xin-Zhe Wei, Lei Wang, Ying Liu, Wei Qu, Zhi-Gui Zeng, Hai-Ming Zhang, Lin Wei, Hao-Feng Xiong, Fei Hou, Zhi-Jun Zhu, Wei Gao and Li-Ying Sun in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.