
Abstract
HIV/AIDS in Bangladesh has historically remained below 0.01% prevalence in the general population; however, recent provisional epidemiological data indicate a concerning shift, with the highest annual increase recorded between November 2024 and October 2025 (1891 new cases; 254 AIDS-related deaths), signaling evolving transmission dynamics. Despite an overall low national prevalence, the epidemic remains highly concentrated among key populations, including people who inject drugs (PWID), men who have sex with men (MSM), female sex workers (FSW), transgender individuals, and migrant workers, where prevention and service coverage gaps have been documented. This narrative review synthesizes evidence published between 2015 and 2025 on HIV epidemiology, prevention strategies, testing infrastructure, treatment outcomes, and structural barriers in Bangladesh. Data were drawn from peer-reviewed studies identified through systematic searches of PubMed/MEDLINE, Google Scholar, and Bangladesh-specific repositories, supplemented by national surveillance reports (National AIDS/STD Programme; Integrated Biological and Behavioral Surveys), international agency documents (UNAIDS, WHO, Global Fund), and recent programmatic reports. Both peer-reviewed and grey literature sources were included to capture the full range of available evidence. Findings reveal significant deficiencies across the HIV response cascade. Geographic availability of testing services is limited to 23 of 64 districts, and prevention coverage is suboptimal, reaching just 26% of MSM and male sex workers. Progress along the treatment cascade shows 82% of people living with HIV diagnosed (approximately 14,334 of an estimated 17,480), 74% of those diagnosed receiving antiretroviral therapy, and 91% of those on ART achieving viral suppression, all falling short of global 95-95-95 targets. Behavioral indicators highlight ongoing vulnerabilities; only 14.4% of MSM report condom use with commercial partners in the past 6 months and 27% of female sex workers reporting no condom use at last sexual encounter. Stigma and discrimination continue to undermine the response, with 68% of people living with HIV reporting feelings of shame and 54% reporting guilt related to their diagnosis, adversely affecting testing, disclosure, and care engagement. Despite these challenges, harm reduction programs and a pilot pre-exposure prophylaxis (PrEP) initiative demonstrate substantial promise. Strengthening targeted prevention, expanding testing and treatment access, and addressing stigma, funding constraints, and structural barriers are essential to sustaining Bangladesh’s low-prevalence status and advancing toward the goal of ending AIDS as a public health threat by 2030.
Plain language summary
HIV/AIDS has remained at a very low level in Bangladesh for many years, affecting less than 0.01% of the general population. However, recent data show a worrying increase in new cases, especially between November 2024 and October 2025. Although the overall number of cases is still low, HIV mainly affects certain high-risk groups such as people who inject drugs, men who have sex with men, sex workers, transgender people, and migrant workers. This review examined research published from 2015 to 2025 on HIV in Bangladesh, including trends in infection, prevention programs, testing services, treatment success, and social challenges. The findings show major gaps in the country’s HIV response. HIV testing services are available in only 23 of the 64 districts, and prevention programs reach only a small portion of people at highest risk. For example, only about one-quarter of men who have sex with men and male sex workers are covered by prevention services. Treatment results show mixed progress. While most people with HIV who receive treatment achieve good control of the virus, Bangladesh has not yet met the global targets for diagnosis, treatment, and viral suppression. Risky behavior remains common, with low condom use among both men who have sex with men and female sex workers. In addition, stigma remains a serious problem. Many people living with HIV feel ashamed or guilty about their condition, which discourages them from getting tested, sharing their status, or continuing care. Despite these challenges, some programs—such as harm reduction services and pilot projects for preventive medicines—have shown strong success. To protect Bangladesh’s low HIV rate and move toward ending AIDS by 2030, the country must expand testing and treatment services, improve prevention programs for high-risk groups, reduce stigma, and address funding and structural barriers.
Introduction
HIV/AIDS in Bangladesh: A growing concern
Bangladesh has been historically recognized as one of the lowest HIV prevalent countries globally, consistently maintaining a reported figure below 0.01% in the general population.1,2 This low-prevalence status has been attributed to early government action, concentrated epidemic dynamics, and sustained harm reduction investments. 1 However, this low-prevalence status is now being challenged by recent epidemiological data that reveal troubling trends.3,4
Between November 2024 and October 2025, Bangladesh recorded its sharpest annual increase in HIV diagnoses, with provisional data indicating 1891 new cases and 254 AIDS-related deaths representing a steeper rise than in any prior year since epidemic monitoring began. 3 For context, the annual incidence prior to this period had been increasing steadily at approximately 600 new cases per year since 2012, from a baseline of 343 new cases in 2010 to 1438 in the preceding year (November 2023–October 2024).4,5 As infections spread beyond conventional hotspots, this notable increase may signal a shift in the dynamics of transmission.3,4
Despite low general population prevalence, Bangladesh faces a concentrated epidemic among key populations. People who inject drugs (PWID) and men who have sex with men (MSM) exhibit higher rates of infection compared to other affected groups, including female sex workers (FSW), transgender individuals, and migrant workers.6,7 As of 2025, approximately 17,480 people are estimated to be living with HIV in Bangladesh, with 14,313 cumulative registered cases since the first diagnosis in 1989 and 2666 cumulative deaths. 5 The 25–49 year age group accounts for 62.61% of cases, representing the majority of cases across all identified age groups.4,5 Since 2010, new cases have risen by over 20%, a trend driven by stigma, reduced international financial support, and insufficient testing facilities serving only 23 out of 64 districts, warranting close monitoring.5,8 Globally, 87% of individuals living with HIV are aware of their condition; Bangladesh lags considerably, as stigma deters people from seeking testing and treatment.2,9 These developments underscore an urgent need for a comprehensive assessment of Bangladesh’s HIV landscape. 9
Historical context and epidemic evolution
Bangladesh’s HIV epidemic began with the first case identified in 1989 in a returning migrant worker, a pattern that would define early epidemic dynamics. 10 Initial surveillance conducted between 1989 and 1996 among 70,676 individuals revealed 80 HIV-positive cases (1.13 per 1000), with a rapid increase starting in 1994. 1 Cases initially concentrated in border districts Sylhet and Chittagong, reflecting the influence of cross-border movement and migrant labor.1,10 The government’s response notably predated the first case, with the National Committee on AIDS established in 1986, making Bangladesh one of the earliest South Asian countries to develop a formal national HIV response.1,11
The epidemic has continued its upward trajectory, with Bangladesh recording 1891 cases between November 2024 and October 2025, bringing cumulative registered cases to 14,313 since 1989. 5 Geographic distribution has expanded beyond Dhaka and Chittagong, with provisional tracking showing 217 new infections emerging among Rohingya refugees in Cox’s Bazar representing a significant new humanitarian dimension to the epidemic. 3 Recent analysis of long-term trends confirm the sustained increase in incidence and forecast rises without strengthened intervention.2,4
Rationale and objectives of this review
The HIV scenario in Bangladesh requires urgent, comprehensive evaluation. The latest increase of 1891 instances indicates a developing trend of transmission patterns that demand examination. 3 Significant gaps remain in the national HIV care cascade. While 82% of individuals living with HIV are aware of their condition, and 74% of those diagnosed are receiving antiretroviral therapy (ART), these accumulated shortcomings leave many individuals unserved. 5 Prevention efforts suffer from key deficiencies: the national testing system operates in only 23 out of 64 districts; prevention tools like PrEP remain largely inaccessible, and condom usage is irregular.5,9
This review addresses a critical gap in the literature. Although there have been recent data-driven analyses of HIV trends in Bangladesh,2,4 there has been no comprehensive narrative review synthesizing the full spectrum of epidemiological, programmatic, and structural evidence in the last several years. This Bangladesh-focused review provides depth necessary for targeted interventions in a concentrated epidemic setting. This review is guided by the Scale for the Assessment of Narrative Review Articles (SANRA) to ensure methodological rigor. 12
Primary objective: Synthesize current evidence on HIV/AIDS epidemiology, prevention and testing in Bangladesh (2015–2025). Secondary objectives: Identify prevention coverage gaps across key populations, assess testing and treatment barriers, evaluate progress toward national/global targets; provide evidence-based recommendations for policymakers and implementers.
Methods
Literature search strategy
This study is a narrative review conducted to synthesize current evidence on HIV/AIDS epidemiology, prevention strategies, testing infrastructure, and treatment outcomes in Bangladesh. This approach was selected to facilitate the triangulation of findings across diverse data types including peer-reviewed studies, national surveillance, and grey literature which is necessary to capture a comprehensive and timely picture of the epidemic in the local context. The search was performed in December 2025, covering January 2015 to December 2025 to capture the most recent decade of evidence, with exceptions made for seminal earlier works providing historical context (e.g., initial surveillance studies from 1989 to 1999).
Four categories of databases and repositories were systematically searched: (1) Peer-reviewed databases: PubMed/MEDLINE and Google Scholar; (2) Bangladesh-specific repositories: Bangladesh Journals Online (BanglaJOL) and institutional databases of the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b); (3) Grey literature sources: reports from the National AIDS/STD Programme (NASP), Integrated Biological and Behavioral Surveys (IBBS 2020), National Strategic Plans (2018–2022 and 2024–2028), mapping and size estimation studies, and surveillance bulletins, as well as international agency documents from UNAIDS, WHO, UNFPA, and the Global Fund; and (4) Recent media: news reports from major Bangladeshi media outlets (Dhaka Tribune) were searched specifically for 2024–2025 statistics not yet available in formal publications.
Search terms combined using Boolean operators included: “HIV” OR “AIDS” AND “Bangladesh” AND specific terms including “prevalence,” “incidence,” “key populations,” “people who inject drugs,” “men who have sex with men,” “sex workers,” “transgender,” “prevention,” “testing,” “treatment,” “antiretroviral therapy,” “stigma,” and “barriers.” No language restrictions beyond English were applied, as per our inclusion criteria. Reference lists of included articles were manually searched for additional relevant sources.
Study selection and reporting flow
Literature identified through the search strategy was screened for relevance based on the inclusion and exclusion criteria defined in the Section Inclusion and exclusion criteria. The selection process prioritized the most recent epidemiological data (2015–2025) while ensuring that foundational historical works were retained for context. Data were extracted from the final set of sources using a standardized thematic framework covering epidemiology, prevention, testing, and treatment to ensure a comprehensive narrative synthesis. As noted in Limitations section, this study is a narrative review rather than a systematic review, and the synthesis focuses on triangulating findings across diverse data types to capture the full range of available evidence.
Inclusion and exclusion criteria
Inclusion criteria: (1) contained Bangladesh-specific data; (2) addressed HIV/AIDS epidemiology, risk behaviors, prevention, testing, treatment, or care barriers; (3) focused on general population, key populations (PWID, MSM, FSW, transgender individuals, migrants), or specific subgroups; (4) published January 2015–December 2025, with exceptions for seminal earlier works providing historical context; (5) available in English.
Exclusion criteria: (1) studies without Bangladesh-specific data; (2) opinion pieces or commentaries without original data; (3) individual case reports unless illustrative of important issues; (4) duplicate publications, retaining the most recent version.
Evidence hierarchy and critical appraisal
The review synthesizes diverse source types, which were differentiated according to an evidence hierarchy. The highest-quality evidence was assigned to (1) National surveillance systems including the Integrated Biological and Behavioral Survey (IBBS 2020), NASP surveillance bulletins, and National Strategic Plans are considered authoritative for epidemiological data given their systematic methodology and national representativeness; (2) Peer-reviewed observational studies such as cross-sectional surveys, cohort studies, and systematic reviews published in indexed journals were considered the strongest source for behavioral and clinical data.
Moderate-quality evidence was assigned to (3) International agency reports (UNAIDS, WHO, Global Fund) considered reliable for program coverage and global comparative data but subject to reporting delays. Lower-quality evidence was assigned to (4) Grey literature and news media. Programmatic reports and newspaper sources (Dhaka Tribune) were used exclusively for 2024–2025 data not yet available in formal publications, and these sources are clearly identified in citations throughout the text.
For peer-reviewed articles, an informal quality assessment was conducted considering study design, sample size, potential for selection bias, and methodological rigor. Studies with nationally representative samples (e.g., IBBS 2020 with population-level data) were weighted more heavily than single-city or small convenience-sample studies. Where multiple sources provided data on the same indicator, we prioritized the most recent and methodologically rigorous source and noted discrepancies where they existed.
Data extraction and synthesis
Data were systematically extracted using a standardized framework covering: (1) epidemiological indicators (prevalence, incidence, mortality, demographics); (2) geographic distribution; (3) key population-specific data (size estimates, HIV prevalence, risk behaviors); (4) prevention interventions and coverage; (5) testing infrastructure; (6) treatment cascade data; (7) barriers to testing and treatment; (8) policy and programmatic context.
For quantitative data, we extracted point estimates, confidence intervals where available, sample sizes, and sources. For qualitative information, we extracted key themes and illustrative examples. Data synthesis employed a narrative approach given heterogeneity across sources and the breadth of the review’s scope. We organized findings thematically: epidemiological trends, prevention strategies and gaps, testing infrastructure and barriers, treatment cascade, and structural factors. Findings from multiple sources were triangulated where possible, and tables and figures were developed to present key quantitative findings systematically.
The synthesis was guided by three established frameworks: (1) the HIV testing and treatment cascade model, 13 (2) the socio-ecological framework for multi-level barriers, 14 and (3) UNAIDS 95-95-95 targets, 6 which provide a standardized benchmark for epidemic control, while situating Bangladesh’s epidemic within the South Asian regional context and global HIV trends.
In accordance with SANRA guidelines, we acknowledge that the inclusion of sources involved selection judgment and that potential selection bias exists. 12
Epidemiological trends in Bangladesh
Current HIV burden and temporal trends
Bangladesh maintains a national HIV prevalence below 0.01% in the general population. 5 As of 2025, an estimated 17,480 people live with HIV, with 14,313 cumulative registered cases since 1989 and 2666 cumulative deaths recorded. 5 The country witnessed its steepest annual increase between November 2024 and October 2025, with provisional data indicating 1891 new cases and 254 AIDS-related deaths. 3 This figure contrasts sharply with the preceding year, when 1438 new cases were recorded, and with the 2010 baseline of 343 new cases, representing a more than five-fold increase over 15 years. 5
New infections have risen by more than 20% since 2010 and have been steadily increasing since 2012, with an annual increment of approximately 600 cases. 4 This upward trajectory stands in contrast to global trends in several regions. For instance, new HIV infections declined by 39% in Eastern and Southern Africa between 2010 and 2023, and by 16% in Western and Central Europe and North America over the same period. 13 In South Asia more broadly, countries such as India have reported declining incidence, though concentrated epidemics persist in certain states. 2
The demographic profile of cases shows that more than 65% of cases occur in the 25–49 age group, with a male-to-female ratio of approximately 2:1. 5 Treatment disparities are notable: although men constitute the majority of diagnosed cases, women and transgender individuals have lower ART coverage. 4 The treatment cascade as of 2025 shows that approximately 14,334 of an estimated 17,480 people living with HIV (82%) are aware of their status; of those diagnosed, approximately 10,607 (74%) are on ART; and of those on ART, approximately 9652 (91%) have achieved viral suppression, all falling short of the global 95-95-95 benchmarks. 5
Geographic distribution and hotspots
Dhaka Division accounts for 35.44% of cases, followed by Chittagong Division at 27.51%. 4 Within Dhaka, microgeographic aggregation is evident: among male PWID, prevalence reaches 27.3% in Old Dhaka compared to 8.9% in other locations. 7 Border regions have emerged as rising hotspots. In Hili, adjacent to West Bengal, India, a 1.6% prevalence rate has been recorded among occasional FSW. 15 The border regions near Myanmar are experiencing elevated HIV rates, a direct consequence of ongoing migration patterns. 1 Recent provisional monitoring shows geographic expansion beyond conventional urban areas, with cases currently noted in an increasing number of districts.3,5 Nonetheless, only 23 out of 64 districts possess testing facilities, establishing access obstacles and possibly concealing the true geographic range of the epidemic.3,5 The Rohingya refugee population in Cox’s Bazar recorded a provisional 217 new infections between November 2024 and October 2025, representing a significant new humanitarian dimension requiring a dedicated response 3 —this is discussed in further detail in the section Rohingya refugees.
HIV among key populations
This section presents HIV epidemiological data for each key population, including sexually transmitted infection (STI) co-infection data. Syphilis is included as an epidemiological outcome because active syphilis infection is a recognized biological cofactor that facilitates HIV transmission by disrupting mucosal barriers and increasing HIV viral shedding, making syphilis co-infection data an important component of understanding HIV transmission risk among key populations. 16 Syphilis data are drawn from the IBBS 2020, which included syphilis serology as part of its key population surveillance protocol. Detailed quantitative indicators for population estimates, prevalence rates, and specific risk behaviors for these groups are summarized in Table 2.
People who inject drugs
PWID remain a primary focus of the country’s concentrated epidemic, with specific urban hotspots historically documented as having prevalence rates that reach or exceed critical thresholds.6,7 Molecular analysis of circulating viral subtypes has further validated the concentrated nature of transmission within this population. 17 While there has been a notable decline in the proportion of new HIV diagnoses among PWID, highlighting the impact of sustained harm reduction efforts, current service coverage requires geographic expansion beyond existing urban centers to maintain this progress.7,18 Detailed population estimates and specific prevalence indicators for this group are summarized in Table 2.
Men who have sex with men
MSM represent the most rapidly growing transmission route in Bangladesh.4,9 High rates of active syphilis co-infection within this group reflect the presence of high-risk sexual networks, while condom use with commercial partners remains critically inconsistent.16,19 Beyond behavioral risks, structural barriers rooted in the criminalization of same-sex acts under Section 377 generate a pervasive fear of arrest and disclosure, which significantly deters testing and prevention uptake.20,21 Detailed epidemiological shifts and behavioral indicators for this population are provided in Table 2.
Female sex workers
FSW exhibit significant geographic vulnerability, with prevalence rates notably higher in border regions compared to the national average.6,22 Active syphilis co-infection within this group reflects the high-risk environments and sexual networks present in specific divisions. 16 Condom use remains critically inconsistent across both brothel-based and street-based settings. 22
FSW face compounded vulnerability: half entered the profession before age 20; average client volume is approximately 23 per week and nearly 27% report active STI symptoms. 22 While knowledge and prior testing rates are relatively high (88% knowing about testing; 83% having been tested at least once), consistent prevention coverage and accessible, ongoing services remain critical. 22 Detailed population estimates, prevalence rates, and specific behavioral indicators for FSW are summarized in Table 2.
Transgender individuals (Hijra)
Transgender individuals (Hijra) bear a disproportionate burden of STI co-infections, exhibiting the highest active syphilis prevalence among all key populations in the country.6,16,22 In 2013, the Bangladesh government formally recognized hijra as a third gender, representing legal progress. 23 Despite this, substantial healthcare barriers persist, including criminalization of same sex sexual acts and systemic discrimination. 20 Many hijra engage in sex work for economic survival, creating multiple overlapping vulnerabilities.3,10 Detailed prevalence data, population estimates, and behavioral indicators—including specific condom use patterns are summarized in Table 2.
Migrant workers
Migrant workers have historically played a significant role in Bangladesh’s HIV epidemic. As of December 2015, approximately 50% of all cumulative cases reported were migrants deported from Gulf countries, and the first documented HIV case in 1989 involved a returning migrant worker. 10 While recent data indicate a declining yet significant proportion of returnees among new cases, they continue to face severe vulnerabilities; specifically, job loss upon diagnosis, economic hardship, and social stigma remain formidable barriers. 3 No HIV testing policy currently exists for returning migrants, and no structured prevention program specifically targets this population. The absence of couples counseling and testing mirrors the systemic neglect of this group, a gap that has direct implications for the heterosexual transmission chain. 10 Historical cumulative figures and specific regional vulnerability trends are detailed in Table 2.
Rohingya refugees
The Rohingya refugee population concentrated in Cox’s Bazar represents an increasingly significant humanitarian dimension of Bangladesh's HIV epidemic. As detailed in Tables 1 and 2, recent provisional monitoring indicates that this population bears a disproportionate burden of the country’s new infections. 3 Earlier research documented that HIV and STI awareness and testing uptake among young Rohingya refugees was limited, with stigma, displacement-related trauma, and lack of culturally appropriate services identified as key barriers. 24 The Rohingya population’s restricted access to formal healthcare, limited freedom of movement, and high rates of gender-based violence create a complex web of HIV vulnerability that requires a dedicated humanitarian response framework distinct from the national prevention program.3,24,25
HIV epidemiological indicators in Bangladesh (2024–2025).
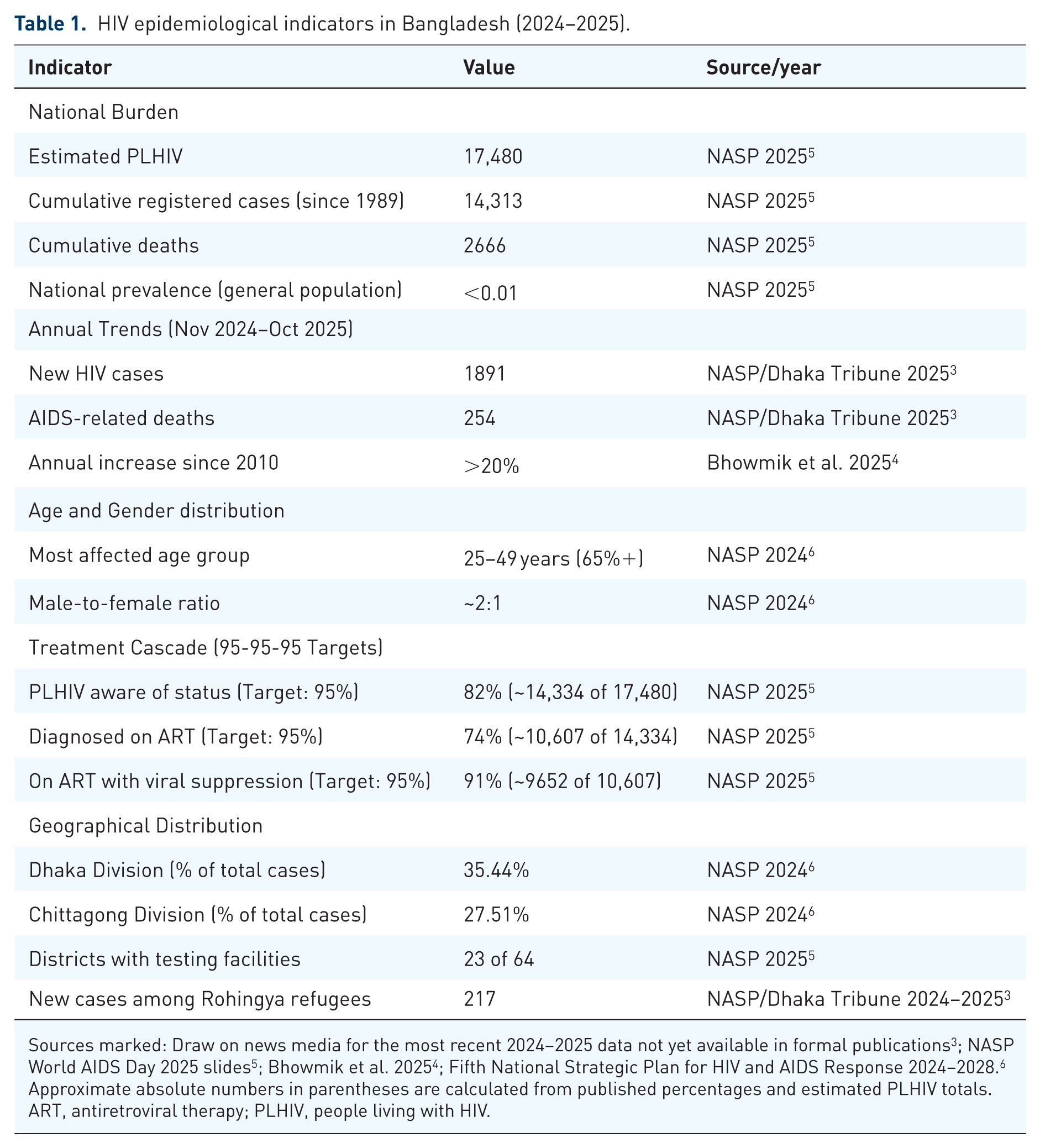
Sources marked: Draw on news media for the most recent 2024–2025 data not yet available in formal publications 3 ; NASP World AIDS Day 2025 slides 5 ; Bhowmik et al. 2025 4 ; Fifth National Strategic Plan for HIV and AIDS Response 2024–2028. 6
Approximate absolute numbers in parentheses are calculated from published percentages and estimated PLHIV totals.
ART, antiretroviral therapy; PLHIV, people living with HIV.
HIV prevalence and risk behaviors among key populations in Bangladesh.
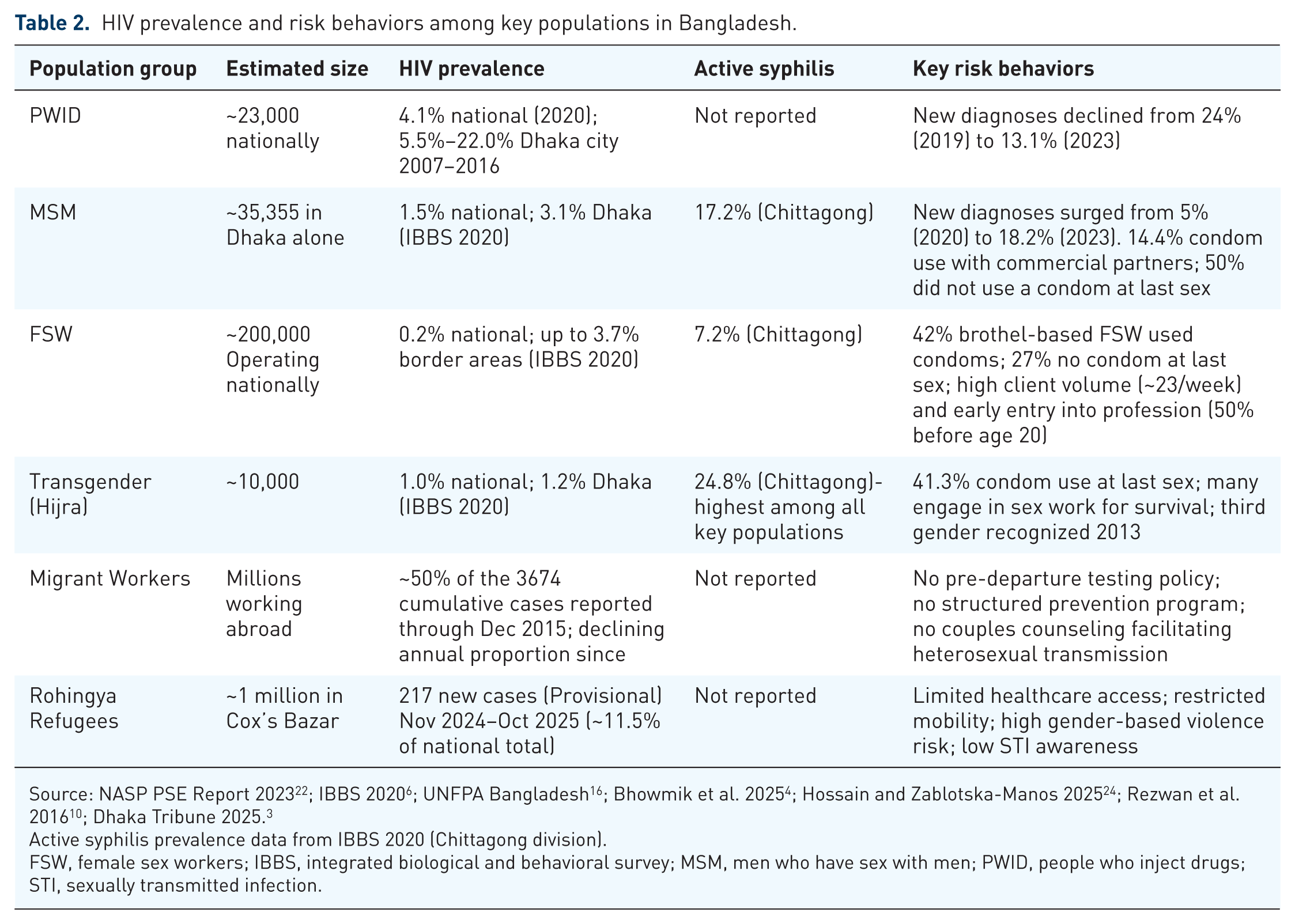
Source: NASP PSE Report 2023 22 ; IBBS 2020 6 ; UNFPA Bangladesh 16 ; Bhowmik et al. 2025 4 ; Hossain and Zablotska-Manos 2025 24 ; Rezwan et al. 2016 10 ; Dhaka Tribune 2025. 3
Active syphilis prevalence data from IBBS 2020 (Chittagong division).
FSW, female sex workers; IBBS, integrated biological and behavioral survey; MSM, men who have sex with men; PWID, people who inject drugs; STI, sexually transmitted infection.
Prevention strategies and interventions
National HIV prevention framework
Bangladesh’s HIV response operates under NASP leadership, implementing successive National Strategic Plans, with the Fifth NSP (2024–2028) representing the current framework. 6 The foundation for a structured response was laid in 1985, before the first case, with the establishment of the National AIDS Committee, leading to the establishment of the National AIDS/STD Programme in 1997, making Bangladesh the first South Asian country to adopt a comprehensive national HIV/AIDS policy. 11
Despite this strong foundation, significant challenges persist. According to the Fifth NSP, only 26% of the estimated 165,192 MSM and MSW are covered by prevention services as of June 2023, leaving 74% unreached. 6 For female sex workers, service gaps have emerged following the closure of operations supporting brothel-based FSWs in January 2023. 6 The country’s HIV program faces ongoing challenges including maintaining political will and investment, integrating HIV services into the healthcare system, coordinating multisector partnerships, and addressing governance issues. 6
Behavioral interventions
Information, education, and communication campaigns
Information, education, and communication (IEC) campaigns have been a cornerstone of Bangladesh’s HIV prevention strategy since 1986. 8 International development agencies have supported tailored messaging for both general and key populations. However, activities to counter stigma and discrimination against high-risk populations have remained limited in scope and funding compared to biomedical interventions, and targeted campaigns risk further labeling vulnerable groups as carriers of HIV infection. 8
Peer education and community outreach
Peer education has appeared as an effective strategy for delivering accessible and relevant HIV prevention information by leveraging social networks to reduce transmission risk. 26 The Fifth National Strategic Plan (NSP, 2024–2028) formalizes this mandate, specifying diversified training resources for peer educators working with PWID, FSW, MSM, MSW, transgender individuals, PLHIV. 6
Biomedical prevention approaches
Condom promotion and distribution
Since 1986, condom promotion has been consistently funded as a key biomedical intervention for high-risk groups. 8 In Bangladesh, condoms are distributed by government health workers and sold through retail channels primarily supplied by the Social Marketing Company. 27 Differentiated Service Delivery includes targeted distribution of condoms and water-based lubricants in varying specifications for different key populations, though persistent concerns exist regarding the quality and consistency of these services. 6
Harm reduction for people who inject drugs
Harm reduction interventions began in 1998, with CARE Bangladesh initiating needle/syringe exchange programmes in Dhaka, which expanded geographically over the next 5 years. 28 By the end of 2006, programmes operated in 21 districts with 20 drop-in centers in Dhaka, providing needle/syringe distribution, abscess and STI management, counseling, and recreational facilities with additional services at Integrated Health Centres including drug detoxification, STI treatment, voluntary counseling and testing, condom distribution, and vocational training. 28 The proportion of newly diagnosed cases among PWID declined from 24% in 2019 to 13.1% in 2023, suggesting programme effectiveness, though geographic expansion of harm reduction services remains essential.7,18
Pre-exposure prophylaxis
Pre-exposure prophylaxis represents a newer addition to Bangladesh’s prevention toolkit. In 2023, icddr,b piloted a PrEP initiative for MSM and male sex workers in Dhaka, supported by the Global Fund. 11 By December 2023, 232 clients had initiated PrEP, with follow-up data showing encouraging results: high retention rates, improved condom use, better mental health, and notably, zero new HIV infections among those who consistently used PrEP during the 22-month intervention. 11 This pilot demonstrates PrEP’s potential effectiveness in Bangladesh’s context. However, availability remains extremely limited to this pilot program in Dhaka. Scaling up requires national guidelines, expanded service delivery points, sustainable supply chains, and demand generation activities. 11
Prevention of mother-to-child transmission
Bangladesh has implemented ART to prevent mother-to-child transmission, reducing transmission risk from 15% to 45% without intervention to below 5% with treatment. 4 National programs have promoted antenatal HIV screening and PMTCT measures, with some evidence suggesting relative effectiveness among married individuals. 4 However, comprehensive data on coverage and outcomes remain limited in publicly available literature. 6 Only 12 antenatal care sites currently offer HIV testing, covering a fraction of the country’s ANC needs. 6
Prevention coverage and existing gaps
Substantial coverage gaps persist across all prevention modalities. The Fifth NSP reveals that 74% of MSM and male sex workers are not reached by services, and similar gaps exist for other key populations. 6 Significant geographic gaps still exist with prevention services concentrated in major urban centers. 4 Poverty limits acquisition of preventive technologies. High levels of stigma and discrimination persist, with anti-stigma activities limited in both scope and funding. 8 The lack of a facilitative legal environment creates additional barriers, as do gender inequality and low education levels. These dimensions of social exclusion lead to risky behaviors that biomedical and behavioral interventions alone cannot adequately address. 8
HIV testing and counseling in Bangladesh
HIV testing services and facilities
Bangladesh’s testing infrastructure reveals critical gaps. Only 23 of the country’s 64 districts have functioning HIV testing facilities, creating enormous geographic barriers, particularly for rural populations. 9 NASP has established 28 HIV Testing Services centers in government medical colleges and district hospitals, and 27 AIDS detection centers operate, though medical services are available at only 11 centers. 6 Most diagnostic facilities are NGO-provided and concentrated in Dhaka, leaving rural areas and cross-border regions severely underserved. 4
Community-based testing through outreach programs targets key populations, though scale and coverage remain limited. HIV self-testing is minimally available. 9 icddr,b has operated VCT units in Dhaka, Chittagong, and Sylhet, providing HIV testing alongside counseling services. More recently, icddr,b has introduced ICT-based interventions including mobile applications, SMS, and web-based platforms to expand HIV testing access for marginalized populations hesitant to seek care in traditional healthcare settings. 11
Testing coverage and uptake patterns
Testing coverage remains suboptimal across all populations. Among female sex partners of HIV-positive PWID in Dhaka, knowledge about HIV and sexually transmitted infections was limited, and uptake of routine HIV testing and prevention services was inadequate. 18 Youth-friendly services remain scarce, and adolescents frequently have incomplete or incorrect knowledge about HIV. 3 Women who inject drugs face compounded barriers to testing, as they are further marginalized and stigmatized compared to male counterparts. 8 Similarly, migrants returning from abroad often lack systematic screening, despite evidence that many contract HIV while working in higher-prevalence countries. 10
The testing cascade and diagnostic gaps
As of 2025, approximately 18% of people living with HIV in Bangladesh (an estimated 3146 of 17,480 individuals) remain undiagnosed and cannot access treatment or prevention services. 5 Late presentation is common, with many individuals diagnosed only when presenting with opportunistic infections or advanced disease which compromises clinical outcomes, increases treatment complexity and costs, and prolongs potential transmission periods. 3
Barriers to HIV testing
Multiple interconnected barriers constrain the uptake of testing at individual, healthcare system, and structural levels.
Individual-level barriers
Stigma and fear constitute the most significant individual-level barriers.8,29 Widespread social stigma discourages individuals from seeking testing or treatment, with documented evidence that stigma deters testing, disclosure, counseling, and safer sex adoption. 8 Approximately 68% of people living with HIV report feeling ashamed and 54% feel guilty because of their HIV status, with more than half blaming themselves for their condition. Fear of such stigmatization deters many from seeking testing even when aware of potential exposure. 30
Healthcare system barriers
Testing facilities operate in only 23 of Bangladesh’s 64 districts, severely hindering early diagnosis and care. 11 Youth-friendly services are notably absent. 3 No dedicated department for HIV services exists in most healthcare facilities to provide psychological support, and existing staff numbers are insufficient; since 2017, the shift of community services to hospitals has created a substantial access gap. 9
Structural and legal barriers
Key populations (KPs) are reluctant to seek healthcare because their behaviors and identities are legally prohibited. Legal barriers are rooted in Section 377 of the Penal Code (same-sex behaviors), the Narcotics Control Act 1990 (drug use), and laws criminalizing sex work, including the Human Trafficking Act 2012 and Section 373 of the Penal Code 1860. 21 Poverty constrains access by transportation affordability and ability to take time off work. Gender inequality restricts women’s autonomous healthcare decisions. Low education levels leave many unaware of testing availability. 8
Linkage to care and treatment
Antiretroviral therapy infrastructure
Bangladesh provides antiretroviral therapy through government healthcare facilities with support from international partners, including the Global Fund, UNAIDS, WHO and UNFPA. 11 The Global Fund’s Bangladesh Programme has significantly boosted ART coverage, with ART coverage reaching 89.11% among diagnosed individuals in 2023, representing substantial improvement from earlier periods. 11 However, the overall treatment cascade figure of 74% of all diagnosed individuals on ART as of 2025 reflects ongoing linkage gaps. 5 Facilities remain concentrated in major urban areas, requiring rural patients to travel considerable distances for medication refills, clinical monitoring, and consultations. 4 Only 11 viral load testing sites currently operate nationally, limiting routine monitoring capacity. 11
Antiretroviral therapy failure due to drug resistance
Drug resistance represents an emerging threat to treatment success in Bangladesh. A 2025 cross-sectional study examined people living with HIV experiencing ART failure, revealing concerning patterns of resistance mutations that compromise treatment effectiveness. 19 The National AIDS/STD Programme follows a “test and treat strategy,” with standard first-line treatment regimens combining three drugs: Tenofovir plus Lamivudine (or Emtricitabine) plus Dolutegravir, or Tenofovir plus Lamivudine (or Emtricitabine) plus Efavirenz. During special situations, alternative combinations using Zidovudine or protease inhibitors are employed. 19 Resistance mutations emerge primarily from inconsistent adherence or poor treatment support, rendering standard regimens ineffective and necessitating a shift to costly second-line therapies. This situation is particularly concerning given Bangladesh’s limited treatment infrastructure. 19
Progress toward the 95-95-95 targets
Bangladesh has made progress toward the UNAIDS 95-95-95 targets but remains short of these goals. 6 As of 2025, approximately 82% of people living with HIV know their status (approximately 14,334 of 17,480); 74% of diagnosed individuals are on ART (approximately 10,607 of 14,334); and 91% of those on ART have achieved viral suppression (approximately 9652 of 10,607). 5 These improvements reflect the success of community-based approaches, peer-led outreach, and the integration of key population services within the public healthcare system. 11 However, the cascading effect of shortfalls at each stage means that the proportion of all people living with HIV who are virally suppressed is substantially lower than 91%.5,13
Impact of global health funding changes
A significant threat to Bangladesh’s HIV response is the shifting landscape of global health financing. The Global Fund remains the primary international donor for HIV programs in Bangladesh, and its contributions have been central to sustaining ART coverage, harm reduction, and key population services. 11 However, international donor funding is approximately 17% below what is needed, and the trajectory of major funding mechanisms including UNAIDS and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) is uncertain amid broader debates about foreign assistance budgets.6,11
Reductions in PEPFAR funding globally are of concern because, while Bangladesh is not a direct PEPFAR recipient country, PEPFAR funding supports UNAIDS operations and regional capacity-building programs that indirectly benefit Bangladesh’s surveillance and programmatic efforts. Similarly, any reduction in Global Fund allocations could jeopardize the sustainability of ART supply chains, PrEP scale-up, and key population outreach programs. 11 Bangladesh’s domestic government allocation to HIV remains insufficient, and the transition to greater domestic financing a goal of both the Fifth NSP and the Global Fund transition framework remains incomplete.6,11 Without sustained international support and accelerated domestic investment, the hard-won gains in ART coverage and harm reduction risk being reversed. These financing uncertainties represent one of the most significant structural threats to epidemic control in Bangladesh for the period 2025–2030.6,11
Barriers to treatment access and adherence
Barriers to ART adherence operate at individual, community, and institutional levels. 29 Barriers at individual levels include forgetting the doses, lack of positive family support, missing doses due to being away from home, financial constraints in continuing treatment (despite free ART, the CD4 count test requires self-funding), and a lack of a positive approach toward life all hinder adherence. 29 At the community level, stigma is the main culprit, which leads to discrimination, fear of disclosure, and depression. 29 At the institutional level, medicine-related barriers (side effects and insufficient or irregular supply), treatment related barriers (substandard counselling, inadequate service delivery), and facility-related barriers (insufficient diagnostic capacity) all contribute to non-adherence. 29
Discussion
Summary of key findings
This review reveals Bangladesh’s paradoxical HIV situation: nationally low prevalence below 0.01% masks a concentrated epidemic among key populations with alarming recent acceleration. The 1891 new cases between November 2024 and October 2025 represent the sharpest annual increase in the country’s epidemic history, signaling a potential transition from concentrated to generalized transmission patterns. 3
Epidemiologically, the burden has shifted dramatically. While people who inject drugs historically drove transmission, their proportion among new diagnoses declined from 24% in 2019 to 13.1% in 2023, suggesting harm reduction success.7,18 Men who have sex with men now constitute 18.2% of new cases in 2023, up from just 5% in 2020, indicating rapidly evolving transmission dynamics requiring urgent attention. 4 Geographic concentration persists in Dhaka (35.44%) and Chittagong (27.51%), though border regions and refugee populations present emerging hotspots, with 217 new infections among Rohingya refugees.3,5
Prevention coverage exhibits critical deficiencies. Only 26% of the estimated 165,192 MSM and male sex workers receive services, leaving three-quarters unreached. 6 Condom use remains dangerously low among both MSM (14.4% with commercial partners) and FSW (27% no condom at last sex).22,19 The testing and treatment cascade falls short of 95-95-95 benchmarks, and testing infrastructure serves only 23 of 64 districts.5,9
Achievements and persistent challenges
Bangladesh has achieved notable successes warranting recognition. The country maintained general population prevalence below 0.01% for over three decades through early prevention investments beginning before the first case in 1989. 1 Harm reduction programs contributed to declining PWID prevalence.7,18 Treatment outcomes demonstrate progress, with 91% of those on ART achieving viral suppression, reflecting successful integration of community-based approaches and peer-led outreach.5,11 The PrEP pilot program in Dhaka demonstrated remarkable effectiveness, with zero new HIV infections among 232 consistent users during a 22-month intervention period. 11 ICT-based interventions using mobile applications, SMS, and web-based platforms represent promising innovations for reaching marginalized populations. 11
However, persistent challenges threaten these gains. Coverage gaps remain substantial, with 74% of MSM and male sex workers unreached by services. 6 The January 2023 closure of operations supporting brothel-based FSWs created new service gaps. 6 Women who inject drugs remain particularly marginalized, with intervention programs largely failing to reach them. 8 Behavioral challenges persist despite prevention efforts reflecting deeper structural issues including violence risks when negotiating condom use, economic vulnerabilities, and gender inequality constraining protective decision-making.19,22
Funding constraints present ongoing challenges. Activities to counter stigma and discrimination remain limited in both scope and funding compared to biomedical interventions, allowing stigmatization to persist as a dormant barrier. 8 The uncertain trajectory of international financing for HIV programs discussed in detail in section Impact of global health funding changes represents a significant threat to the sustainability of current achievements.
Bangladesh in the regional context
Bangladesh’s HIV situation must be understood within the broader South Asian context. The country shares cultural similarities and a porous border with India and Nepal, both of which have higher HIV prevalence, creating cross-border transmission risks. 8 Migration patterns significantly influence epidemic dynamics, with returning migrants historically comprising 50% of all HIV cases reported through December 2015. 10
The country faces unique vulnerabilities within the region. Bangladesh’s dense population means that even 1% general population prevalence would translate to approximately 1.7 million people living with HIV, a burden that the current health system simply could not manage. 8 New infections in Bangladesh have risen by more than 20% since 2010, contrasting sharply with declining incidence in several neighboring countries. 4 The dramatic surge in MSM cases from 5% to 18.2% of new diagnoses signals shifting transmission patterns that demand urgent regional and domestic attention. 4
Data gaps and surveillance needs
A critical but underappreciated dimension of Bangladesh’s HIV response is the significant gap in surveillance data quality and coverage. Several populations and outcome domains remain poorly characterized. First, women who inject drugs are rarely captured in behavioral surveillance, with most PWID surveys focusing predominantly on male respondents, leading to a systematic underestimate of this population’s burden. Second, HIV incidence data as distinct from reported diagnoses are not routinely estimated, making it difficult to assess whether transmission is truly accelerating or whether improved case-finding explains recent increases. Third, pediatric HIV surveillance data are sparse, with limited published information on mother-to-child transmission rates and outcomes. Fourth, among Rohingya refugees, population-based HIV surveillance is nascent, and the true prevalence is likely underestimated given restricted access to formal healthcare. Fifth, drug resistance surveillance outside of the 2025 cross-sectional study remains limited. 19
Strengthening HIV surveillance infrastructure including establishing a sentinel surveillance system with standardized, regular IBBS rounds across all divisions, implementing routine viral load monitoring, and developing community-based surveillance mechanisms for hard-to-reach populations should be treated as a foundational priority recommendation alongside the programmatic recommendations outlined in the section Priority recommendations for action.
Limitations
First, as a narrative review rather than a systematic review with a pre-registered protocol, the inclusion of sources involved a degree of selection judgment; therefore, potential selection and confirmation bias cannot be entirely excluded, particularly concerning the reliance on provisional media reports for 2024–2025 data. Second, reliance on available literature means that some recent programmatic developments may not yet be captured in formal publications; we addressed this partially through the inclusion of grey literature and news sources, but these carry lower evidentiary weight. Third, potential underreporting is substantial stigma and limited surveillance infrastructure mean that the true burden among key populations is likely higher than reported figures suggest. Fourth, heterogeneity in data quality across sources complicates direct comparison; for instance, IBBS 2020 data reflect population conditions five years ago and may not fully characterize current epidemic dynamics. Fifth, the narrative synthesis approach, while appropriate given the breadth of the review, does not permit statistical pooling of estimates. These limitations should be considered when applying the findings to policy and program planning.
Priority recommendations for action
Based on the synthesis of epidemiological trends, programmatic deficiencies, and multilevel barriers identified throughout this review, the following priority actions are recommended to strengthen Bangladesh’s HIV response. These interventions are strategically designed to address the critical gaps in the prevention and treatment cascades while tackling the structural factors necessary to sustain the country’s low-prevalence status and achieve the 2030 goal of ending AIDS as a public health threat (Table 3).
Priority recommendations for action in the Bangladesh HIV response.
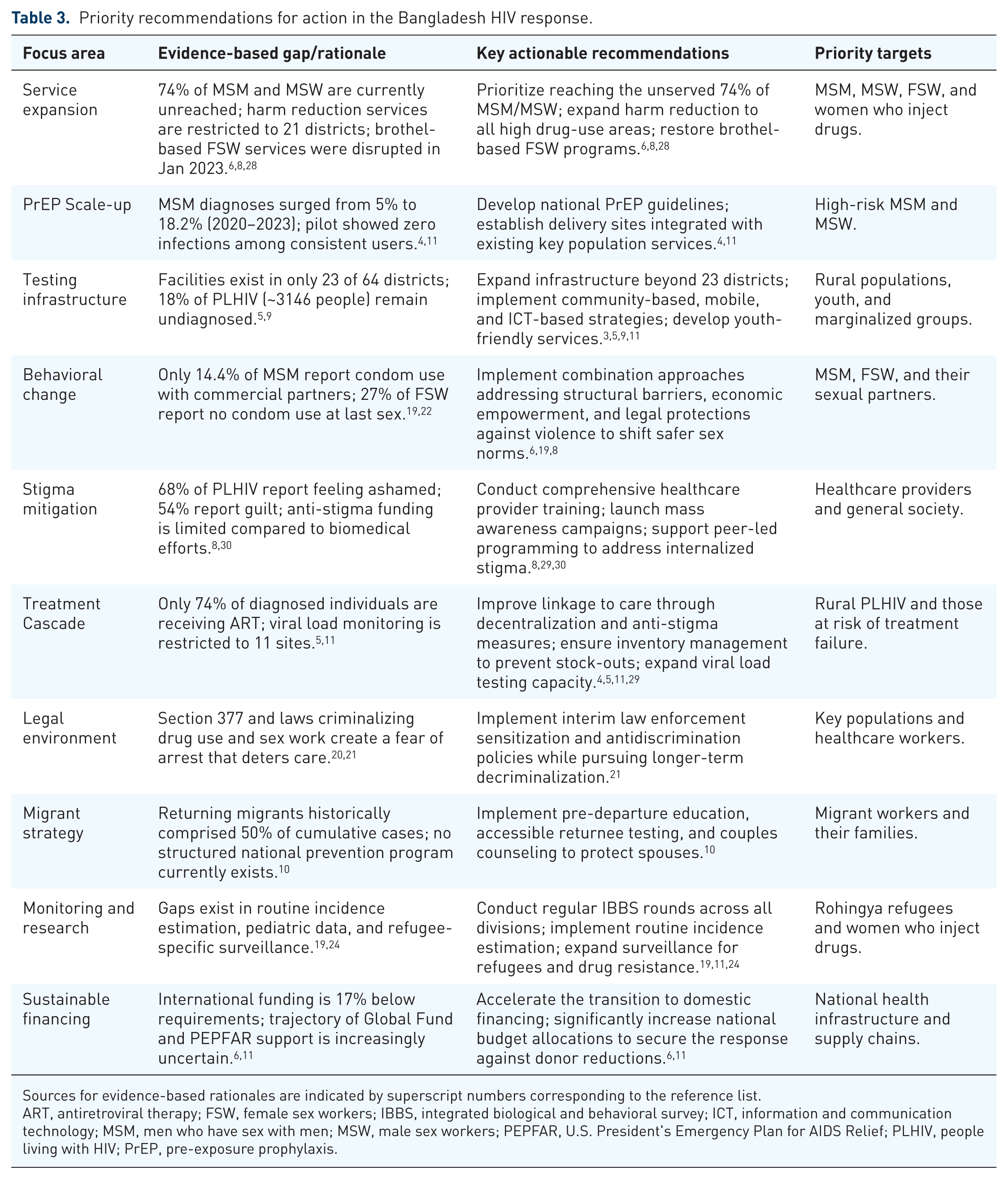
Sources for evidence-based rationales are indicated by superscript numbers corresponding to the reference list.
ART, antiretroviral therapy; FSW, female sex workers; IBBS, integrated biological and behavioral survey; ICT, information and communication technology; MSM, men who have sex with men; MSW, male sex workers; PEPFAR, U.S. President's Emergency Plan for AIDS Relief; PLHIV, people living with HIV; PrEP, pre-exposure prophylaxis.
Conclusion
Bangladesh faces a critical juncture in its HIV response. Recent epidemiological shifts, characterized by the steepest annual increase in new diagnoses since monitoring began, signal a potential transition from a concentrated to a more generalized transmission pattern. 3 While the country successfully maintained a low-prevalence status for over three decades, these evolving dynamics demand urgent, adaptive, and comprehensive strategies to prevent further escalation.3,4
Critical gaps span the entire response cascade, from a testing infrastructure that leaves rural and border populations underserved to suboptimal prevention coverage among the most vulnerable key populations.6,9 The national treatment cascade currently falls short of global benchmarks, highlighting significant bottlenecks in diagnosis and linkage to care. 5 These challenges suggest that biomedical approaches alone cannot achieve epidemic control without addressing the underlying structural barriers, including poverty, gender inequality, the criminalization of key identities, pervasive stigma, and the increasingly uncertain global health funding landscape.6,11,19,22,30
Stigma and discrimination emerge as dominant barriers across all response aspects. Internalized shame and fear of judgment continue to deter individuals from seeking testing, disclosure, and long-term treatment engagement. 30 These individual-level barriers are reinforced by institutional challenges, such as inadequate HIV training for healthcare providers and limited funding for antistigma advocacy.8,29,30
The path forward requires multisectoral strategies that address prevention, testing, and structural inequities simultaneously. The documented success of harm reduction, high rates of viral suppression among those receiving care, and the efficacy of recent pilots prove that epidemic control is achievable when interventions are properly resourced and implemented. With sustained political will, robust community support, and the transition to sustainable domestic financing, Bangladesh can reclaim its trajectory toward ending AIDS as a public health threat by 2030.4,11