
Abstract
This article examines the issue of professionalism in relation to dental practitioners, and how it impacts upon the range of medico-legal challenges they might face. It provides an overview of professionalism in a healthcare context and explores some of the characteristics that different parties would associate with it.
The mismatch between these different perspectives and the relative importance that each party attaches to different aspects of professionalism, can often sit at the heart of complaints and litigation.
The article also questions whether or not traditional professional values and behaviours are still relevant in a modern healthcare environment that is increasingly digital, consumerist and competitive – or conversely in such a fast-changing world, whether the need for a modern professionalism is greater than ever.
Learning Objectives
To explain how and why clinicians, patients, regulators and others might view professionalism in different ways
To explain the different dimensions of professionalism, and the essential ingredients of professional integrity
To encourage reflection on the nature of professionalism and its relevance at all stages in our career development
Introduction
Professionalism (or the lack of it) is an issue bubbling under the surface of many disagreements between those providing healthcare, and those receiving it – and yet it remains a notoriously difficult and elusive concept to define. It lends itself to the ‘I know it when I see it’ alternative approach made famous by US Supreme Court judge Potter Stewart in the 1960s, 1 not least because it has such a strong subjective dimension. The issue of professionalism arises not only in terms of patient dissatisfaction, complaints and litigation, but also in relation to many other types of medico-legal challenge – the GDC is an obvious example but certainly not the only one.
Healthcare is hardly unique in being populated by ‘professional’ people, but we should find it unsurprising that the qualities required in healthcare are not identical to those considered important in the legal profession, or amongst teachers or religious/faith leaders, or indeed amongst people recognized as having a special level of knowledge and skills in many other fields. There will be core similarities to be found alongside differences in emphasis, interpretation and application. Readers may be interested in some fascinating parallels and contrasts exposed in two pieces of research : the first carried out on behalf of the Health Professions Council by the Medical Education Research Group, Durham University and published in 2014, 2 and the more recently published work (July 2020) by the Association for Dental Education in Europe (ADEE), led by a team from Cardiff University and commissioned by the GDC. 3
It is relevant to acknowledge at the outset, that the term ‘professional’ is defined in subtly different ways according to the context and the viewpoint (and perhaps, subjective bias or special interest) of the person or organisation defining it. The three recurring themes are:
a) being recognised and accepted as a member of a group of people with a particular set of qualifications or special knowledge/expertise. An extension of that recognition is seen in the qualities and values which one would normally associate with members of such a profession, and which may be enshrined in some kind of formal code that those members sign up to and are expected to adhere to;
b) having a level of ‘specialness’ in terms of training, skill and competence that sets them apart from most other people and allows them to carry out the required tasks at a superior level;
c) the fact that their special expertise is valued by others to the extent that they are paid fees for providing their services (as distinct from supplying goods) to a predictably high standard, from which they derive their living (i.e. ‘professional’ as opposed to ‘amateur’).
In his play The Doctor’s Dilemma, 4 George Bernard Shaw wrote to the effect that professions ‘are all a conspiracy against the laity’. The laity appears to be fighting back because more than a century later, the term ‘professional’ has been somewhat hijacked in modern parlance whereby the defining requirement for a professional qualification is conveniently bypassed, and the word is used as an adjective to describe shades of supposed excellence. Perhaps inevitably, those who are unarguably members of a recognized and well-established profession, will attach greater importance to (a) than those who are not. The ensuing paradox persists in the shape of bizarre terms such as ‘a professional foul’ – make of that what you will.
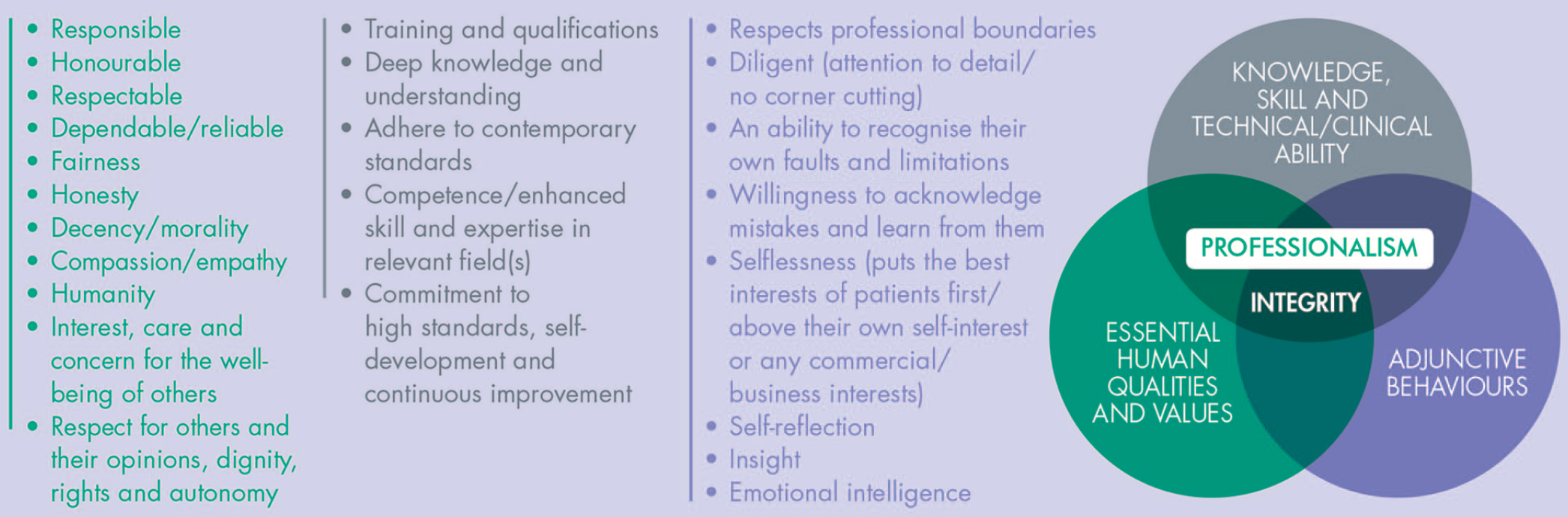
Figure 1 illustrates some of the qualities normally associated with professionalism. For the purposes of this discussion they have been grouped into three broad and overlapping ‘domains’ and the underlying premise offered here is that a fully rounded professionalism requires a balance of the qualities spanning all three of them.
The Ingredients of Professionalism
Integrity is an equally intangible concept but most people would associate it primarily with the qualities and values domain in Figure 1, while also drawing from the other two domains. Taken literally, the term describes the kind of ‘wholeness’ which underpins true professionalism. In this sense integrity is necessarily binary in that you can’t have partial integrity: it is as nonsensical as being ‘a little bit pregnant’. Conversely, an individual may act unprofessionally on a particular occasion, but this is not necessarily indicative of their professionalism – or lack of professionalism – more generally.
A couple of the descriptions in Figure 1 merit closer examination for the purposes of our present discussion:
Responsible – the person takes responsibility for their actions (and omissions) and demonstrates a commitment to putting things right when necessary. They do not seek to blame, gratuitously criticise or denigrate others. They are also socially responsible and understand the part they play in wider society;
Honourable – they behave appropriately and properly: they are principled and ethical and can be relied upon to ‘do the right thing’ even when (and especially when) others might be tempted to take an easier or more self-serving course – and even when nobody is looking or nobody would ever find out;
Respectable – they recognise and respect the rule of law and set a good example to others. In doing so they help to maintain public confidence in the profession and its reputation as being ‘upright’ and trustworthy;
Competence – this implies the ability to provide care and treatment safely, and to an acceptable standard. Public confidence in a profession always relies upon trust that appropriate standards will be maintained: there is a further expectation that a professional person will by virtue of their special knowledge and training be able to provide their services to a significantly higher standard than other members of the public. Dentistry enjoys the further privilege of being a legally protected activity, reserved under the Dentists Act 1984 for dental registrants only, so the comparison with lay people does not apply. But the law5,6 does expect dentists to provide care and treatment to a standard that would be considered proper, by a responsible body of their peers.
Self-reflection and insight
Self-reflection has been described as a process whereby you develop and refine your understanding of who you are, why you think and act the way you do and what your values are. Sharing many of the facets of emotional intelligence, it is a form of personal analysis that can be a valuable tool in aligning the reality of your life with what you wish it to be.
Insight is the possession of a clear, deep and perhaps profound understanding of something. Although it is often as valuable to have insight into one’s strengths as one’s deficiencies, the term is often used in the countersense: that is, describing someone as ‘lacking insight’. Individuals are often criticised for appearing to lack insight into some previous deficiency, ‘offending’ or underperformance and this creates an awkward moral dilemma for those who have consistently denied or maintained their innocence of the allegations previously made against them. It is difficult to show insight into something you genuinely believe not to have happened, but as the famous American comedian George Burns once observed: ‘The key to success is sincerity; if you can fake that, you’ve got it made’. Joking aside, there is no doubt that an essential quality for a professional person is to be able to see themselves as others see them, and to demonstrate that fact: perhaps that is the key to solving the moral dilemma mooted above.
One aspect of insight that is particularly relevant to this discussion, arises when a clinician is adamant that they have treated the patient to a high standard, and believes that the patient is acting unreasonably in complaining about the care they have received. Very often in such cases, the clinician appears to have a blind spot and is measuring the quality of the treatment by narrow, technical/clinical standards alone, and vigorously defending it on that basis. Meanwhile, the patient’s dissatisfaction is about their overall experience and they are measuring the quality of their care by very different criteria, many of which feature in Fig 1. This mismatch in perspectives tends to entrench views and feelings on both sides.
This leads us conveniently to examining how the quality of care is measured.
Quality and standards
Standards are central to any kind of professionalism. As highlighted in Figure 1, professionalism requires adherence to acceptable contemporary standards, which in turn implies an up-to-date awareness and understanding of them. Philip (‘Phil’) Crosby is widely recognised as having been one of the most influential contributors to the field of quality and its management in organisations – not only in his native America, but internationally. His background was largely in manufacturing industries but he developed principles which had a much wider application. Crosby maintained that quality relied on the consistent achievement of defined standards – but he emphasised that this is too simplistic a view. The following short extract from one of his many books
7
elegantly summarises a key theme of his approach and has a particular resonance for general dental practitioners:
True quality is determined not by the person providing the product, but by the end customer.
Too many businesses have a self-indulgent, inward-facing perception of quality in a technical sense, and too few of them measure quality in terms of how well the product or service meets the needs, expectations and demands of the customer.
They are preoccupied with their own parameters of quality and they will place the highest value on whatever they think they are best at.
People who have unusual, rare or highly specialised skills will understandably place a high value upon them, but the downside is that they might dismiss or under-value equally important but more commonplace skills. More dangerously, they might assume that they already have these skills in greater abundance than is actually the case. In healthcare – and the law, interestingly enough – communication skills are undoubtedly crucially important and both the GDC and the Solicitors Regulation Authority (SRA) have moved their required CPD approach to self-directed learning based on a personal development plan and a personal assessment of training needs and priorities. Many dental registrants view communication skills as somewhat basic and somehow implied into their dental degree; they prefer to believe that their time would be better spent on other, more ‘advanced’ clinical topics. In any event, tracking down relevant CPD courses or more structured training in basic and advanced/applied communication skills (e.g. listening, questioning, non-verbal and other such skills) is much more difficult than finding courses on cosmetic dentistry or implant dentistry or on medical emergencies, infection control, safeguarding or other recommended CPD topics – which is quite revealing in itself. Consequently, while communication issues feature prominently in so many dentolegal cases,15,19,20 training in applied communication skills very rarely features in the CPD activity of the majority of dental registrants.
Complaints and/or legal proceedings are not served upon us by teeth, but by people. If we concentrate on treating people rather than teeth, we will experience far fewer dentolegal problems (see section below). Similarly, when selecting areas for improvement or the measures we might use as part of clinical audit, we should ensure that the focus of our efforts will be relevant and beneficial in a currency that patients will recognise and benefit from. Even the highest quality treatment, in a technical sense, is of questionable quality if it is not necessary, not what the patient wants, or not in the patient’s best interests.
Defining quality in healthcare has long been a contentious issue in many parts of the world,8–11 due once again to the widely differing perspectives of clinicians, patients, managers of health services and third party funders – amongst others.
Professionalism and litigation
The inherent and/or claimed ‘specialness’ of a recognised professional in any field, does raise the bar of expectation and can fuel a heightened sense of being let down when things don’t go to plan. There is a large body of evidence, albeit mostly from studies involving our medical colleagues, that a disproportionately high share of all litigation involves a relatively small minority of doctors. This is also true of dentists. In broad terms, a UK dentist is likely to be the subject of a negligence claim once every ten years – a frequency greater than for UK medical GPs. But in fact some will go through their entire career without a single claim, while a small minority will suffer a much higher ‘strike rate’ than the average. One would expect a standard normal distribution (bell) curve to apply anyway and anecdotally we all hear tales of ‘good’ and ‘bad’ colleagues or get occasional glimpses of their clinical work and base our conclusions upon that. Where our assumptions come unstuck, however, is in the reasons for the extremes in that distribution.
We might guess that some procedures (and by extension, some specialties) involve more inherent risks than others. 12 Such surmise would be correct to an extent, but even within the same specialty, and/or amongst a group of general practitioners carrying out a similar mix of procedures, some clinicians will experience a disproportionate share of the resulting claims. Some specialists will argue that certain procedures are an accident waiting to happen when they are attempted by general dental practitioners/non-specialists – and in many cases they will be right. But such generalisations are an imprecise science and there are many exceptions to disprove the theory, even though we would probably all agree that recognising our own limitations is one of the hallmarks of professionalism.
However, clinical negligence claims experience is a particularly crude and clumsy measure of the quality of care because the legal test of negligence5,6 requires the patient to have suffered avoidable harm, as a result of care which has fallen below an acceptable standard in some respect(s). For this and other reasons surprisingly few adverse outcomes result in litigation anyway. Some dissatisfaction surfaces as a complaint (direct to the clinician, or to the practice, or involving other bodies up to and including the GDC), some enters the public domain as negative online feedback, while some ‘goes away’ for reasons that are not always clear at the time.
Individual variation between patients is the single most important determinant of where things finish up; the same clinical scenario can unfold for several patients and what happens next will be different for each of them reflecting their personality, past experience, expectations, and not least what happened, how they feel about it and what kind of remedy or reparation they are seeking.13–17 Most important of all, however, is the relationship and interactions between the patient and the clinician18,19 before, during and after the events in question – and that is where all the non-clinical aspects of professionalism enter the picture and arguably assume even greater importance.
Most patients understand that clinicians are human and mistakes will happen. They are also surprisingly forgiving of sub-standard treatment, as long as you respond appropriately, put things right or assist in that process. But a mistake or sub-standard treatment when coupled with perceived shortfalls in our communication, attitude or behaviour, compounds the ‘injury’ and often proves to be a powerful driver for taking things further. 20
Professionalism and the GDC
Anyone reading the GDC’s published guidance Standards for the Dental Team, 21 may well be struck by how little time is spent talking about clinical /technical standards. Indeed, the nine core principles outlined by the GDC appear at first sight to be almost silent on such standards, being much more preoccupied with ethical standards and what we might call ‘behaviours’. The document is written through the lens of ‘what members of the public expect’ and Principle 7 (one of the shortest sections in the guidance) simply states that patients expect to receive ‘good quality care’ and that all members of the dental team:
are appropriately trained and qualified;
keep their skills up to date;
know their limits and refer patients as appropriate;
work within current laws and regulations.
While perhaps a glaring omission at first sight, the GDC is not (and must not be) the arbiter of clinical standards: that is the proper role of the profession itself. The Standards reflecting Principle 7 continue, stressing the need for registrants to familiarise themselves with and follow the evidence base and ‘best practice’, and to ensure that they only carry out a task or a type of treatment if they are appropriately trained, competent, confident and indemnified to do so. The section concludes with the need for career-long professional development.
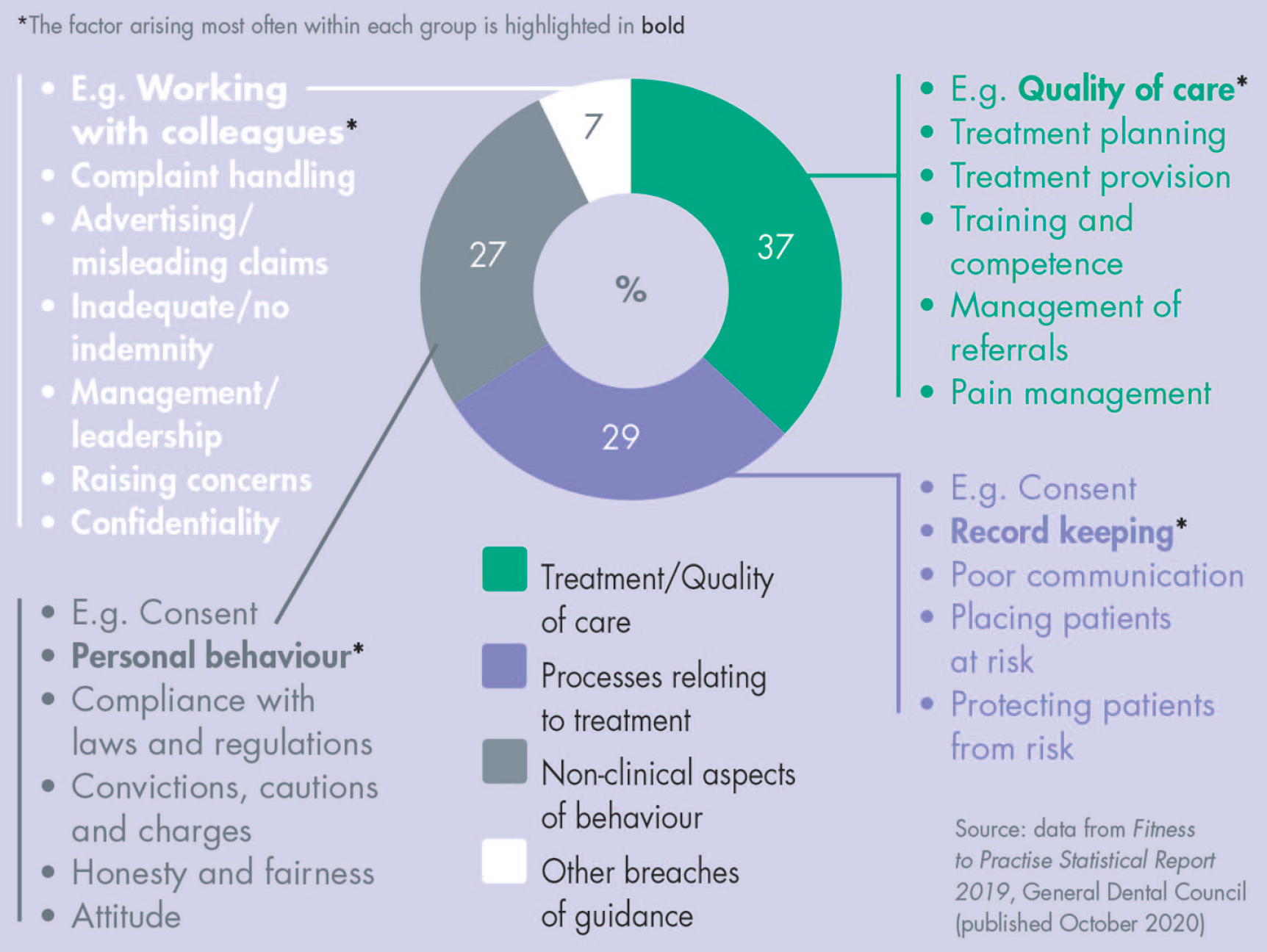
The GDC publishes details of the various categories of what it terms the ‘consideration’ involved in the cases which are dealt with under its Fitness to Practise procedures, by the Professional Conduct and Professional Performance Committees respectively. 22 Several ‘considerations’ might arise from a single case. The spread of the issues involved (see Figure 2) supports the contention that professionalism is not simply a matter of clinical/technical quality.
Fitness to Practise Considerations
What is less obvious from this analysis is that a complaint might itself relate primarily to some kind of dissatisfaction with the care and treatment provided, but it could raise other concerns when viewed through the eyes of a GDC caseworker. Furthermore, these other concerns may well be viewed more seriously than the clinical issues raised in the original complaint. One of the reasons for this is that while one can be seen to be addressing clinical or technical shortfalls, the other aspects of professionalism do not all lend themselves equally well, or as easily, to effective remediation. Even more fundamentally, a perceived lack of insight or an apparent absence of any evidence of reflective learning, undermines the confidence of committee members in a registrant’s commitment to (and ability to) turn things around so that a future similar situation is avoided.
Patient safety is a primary concern for the GDC and patients alike. The quality of clinical/technical dentistry arises as a specific consideration more than twice as often as any other issue. Yet the technical aspects of quality are a much hotter topic for dentists and other registrants, than for patients. There are echoes here of Phil Crosby’s work (see above) but the GDC’s most recent research 3 found that patients also expect technically good care (as a “given”) and on balance this appears to be more important to them than other aspects of professional behaviour. Strikingly, patients seem far less concerned than registrants (or the GDC) about how a dentist behaves in their personal life.
Thus, maintaining high standards of professionalism may not only make it less likely that we will find ourselves subject to a complaint to the GDC in the first place, and/or being investigated by the GDC; it will materially reduce the likelihood of any serious adverse sanction or other consequences even if the GDC does become involved. Professionalism can come to our rescue even after the event.
Professionalism in a consumerist society
There is a view in some quarters that patients in today’s world are simply consumers of healthcare, thinking and behaving like customers and using the same digital tools to choose their dentist and make their treatment decisions just as they would for any other consumer purchase. The same observers will have us believe that patients view their encounters with the dental profession as just another commercial transaction, and that cheapest is best.
If we allow it to do so, such a depressing view may prevail and some dentists and practices are unwittingly encouraging the commoditisation of dentistry in this way. The specialness of the dentist: patient relationship lies in our professionalism, not our sales patter, and we abandon that at our peril. Several years ago 23 I posed the rhetorical question of whether people would really prefer to feel like a customer or a consumer as the anaesthetic was taking effect, or like a patient.
I would contend that patients want all the access, information, choice and consumer protection that they would enjoy anywhere else in the modern high street, but they want all those ‘old fashioned’ professional values too. We are the custodians of the trust and confidence that patients regularly report themselves as having in the dental profession, and we should not relinquish that, nor allow it to be stolen from us.
Summary
Professionalism is not just a question of qualifications nor of a ‘steady state’ de facto membership of a recognised ‘learned’ profession. It manifests itself in terms of
Our patients don’t want our technical skills alone (however good they are): they want, expect and deserve the rounded totality of our professionalism. As to the value of that, I cannot improve upon the words of the legendary Texan firefighter Paul Neil (“Red”) Adair whose iconic reputation was built upon his role in extinguishing many of the world’s most terrifying gas and oil well fires of the 1960s and 1970s:
“If you think it’s expensive to hire a professional to do the job, wait until you hire an amateur.”