
Abstract
This report discusses a rare case of a 75-year-old male presenting with a large lipoma of the tongue. It examines the investigations carried out to aid in diagnosing the lesion and the management options. Since oral lipomas rarely cause symptoms, there tends to be a general delay in seeking treatment. This case report aims to help dental practitioners diagnose intra-oral soft tissue lesions and provide appropriate management for their patients.
Learning Objectives
To raise awareness on the diagnosis of lipomas
To raise awareness of the management options for lipomas
Introduction
Lipomas are among the most common benign tumours and account for 50% of all soft tissue neoplasms. 1 They are defined as adipose (fat) cells which are usually encapsulated by a thin layer of fibrous tissue. 2 They lie in subcutaneous tissues and tend to develop in patients between the ages of 40 and 60 years. 3 Lipomas are typically asymptomatic and are relatively uncommon in the oral cavity; however, when they do occur there, lipomas are likely to affect the cheek, tongue, lips, gingiva, and rarely the floor of the mouth. While intra-oral lipomas are benign in nature, depending on their size and location, they can have a detrimental effect on a patient’s quality of life. Management options include no treatment and surgical excision, and are largely influenced by anatomical location and patient preference.
Case report
A 75-year-old Asian male was referred to the Oral and Maxillofacial Surgery (OMFS) department with a tongue lesion. The patient, an irregular dental attender, was referred on a routine pathway after registering with a dental practice and visiting a General Dental Practitioner (GDP). The patient’s complaint was dental pain from an unrelated tooth, the lower left second premolar. The patient’s “very asymmetrical tongue” and “raised floor of the mouth on the left” was noticed by his GDP, who made a referral to secondary care for a second opinion. The referral was triaged by one of the clinicians in the OMFS department and the patient was asked to attend for an urgent assessment. The change in the appearance of the tongue was not originally noticed by the patient and this, combined with a lack of previous GDP attendance for several years, made it difficult to gauge the duration the lesion was present for. While the lesion was not causing the patient any pain or discomfort and was described as “completely asymptomatic”, it was noted that the patient’s tongue deviated to the left on protrusion. The lesion did not, however, have any impact on the patient’s swallow or speech function.
Medically, the patient suffered with hypertension for which he took ramipril and atenolol medication daily. The patient did not report to smoke nor drink alcohol.
Extra-oral clinical examination revealed no cervical lymphadenopathy or facial asymmetry (see Figure 1a–c). Oral examination revealed a soft non-tender mass on the left posterolateral tongue. It did not encroach onto the floor of the mouth and did not cross the midline. The overlying tongue mucosa appeared to have normal colour and surface texture without signs of ulceration or induration. No discrete lesions were noted. The tongue deviated to the left side on protrusion (see Figure 1d) which suggested a hypoglossal nerve injury. All other cranial nerves were intact, including the lingual nerve with no signs of paraesthesia, and the swelling did not impact on the patient’s swallow function.

Differential diagnoses for this mass included collection of lymphoid tissue or lipoma of the tongue. With the presumed short history and possible hypoglossal nerve injury, however, a more sinister pathology needed to be excluded.
To further evaluate the lesion a magnetic resonance imaging (MRI) of the head and neck was requested.
MRI examination
The MRI scans (see Figure 2) revealed almost the whole left side of the tongue to be abnormal. There was increased signal on both T1 and T2-weighted scans, which is usually seen with fat and is consistent with a lipoma. The left side of the tongue was also lax posteriorly, bulging into the vallecula. This appearance can be seen secondary to a hypoglossal nerve palsy with subsequent atrophy, but no cause of a hypoglossal nerve lesion was seen at the skull base to explain this.
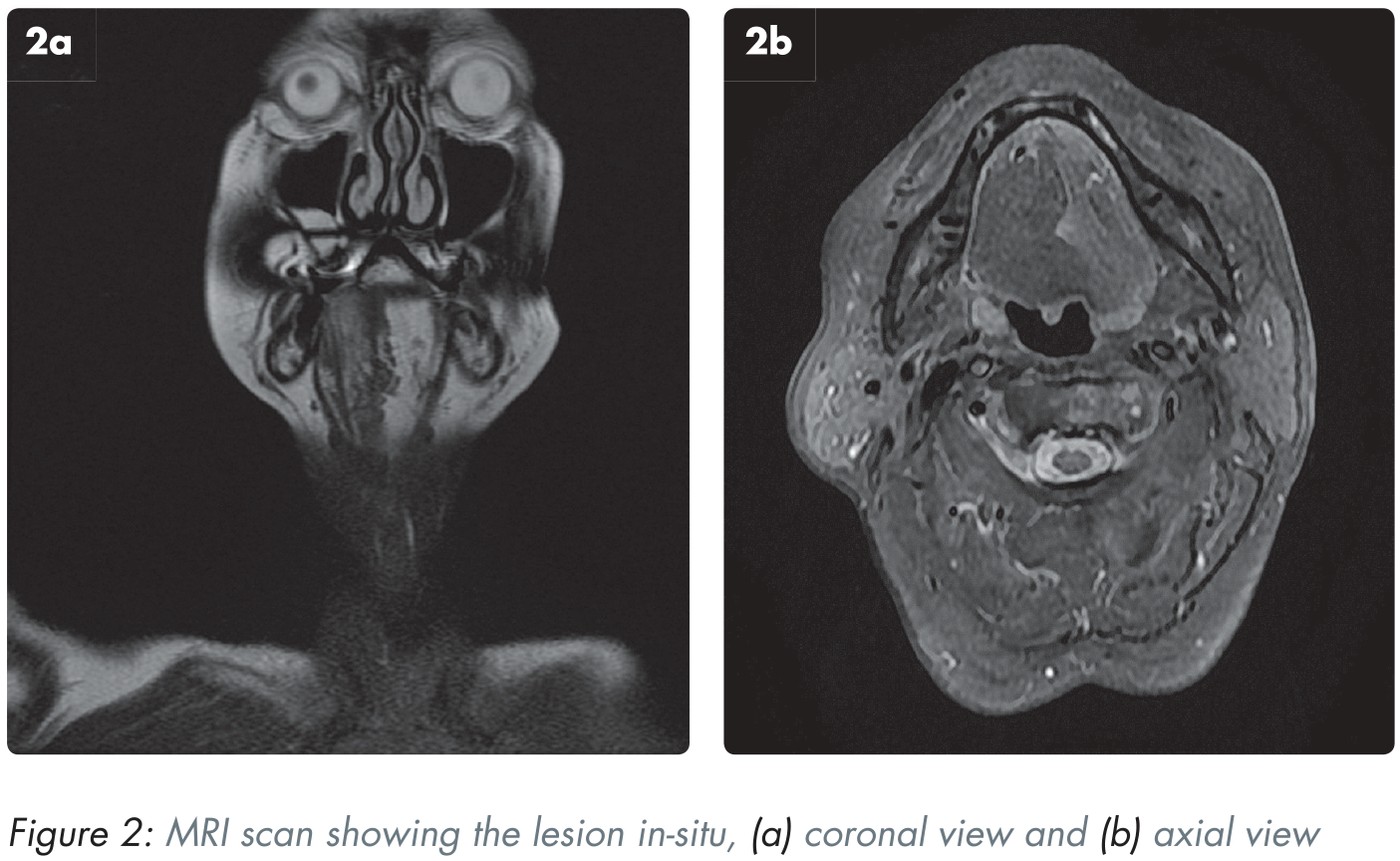
Tumour infiltration with secondary hypoglossal nerve involvement would be an alternative explanation which might better account for the unilateral tongue swelling. No lymphadenopathy was reported.
A prominent Level 1B lymph node was identified on the MRI. However, sonographic appearances and fine needle aspiration supported a reactive lymph node.
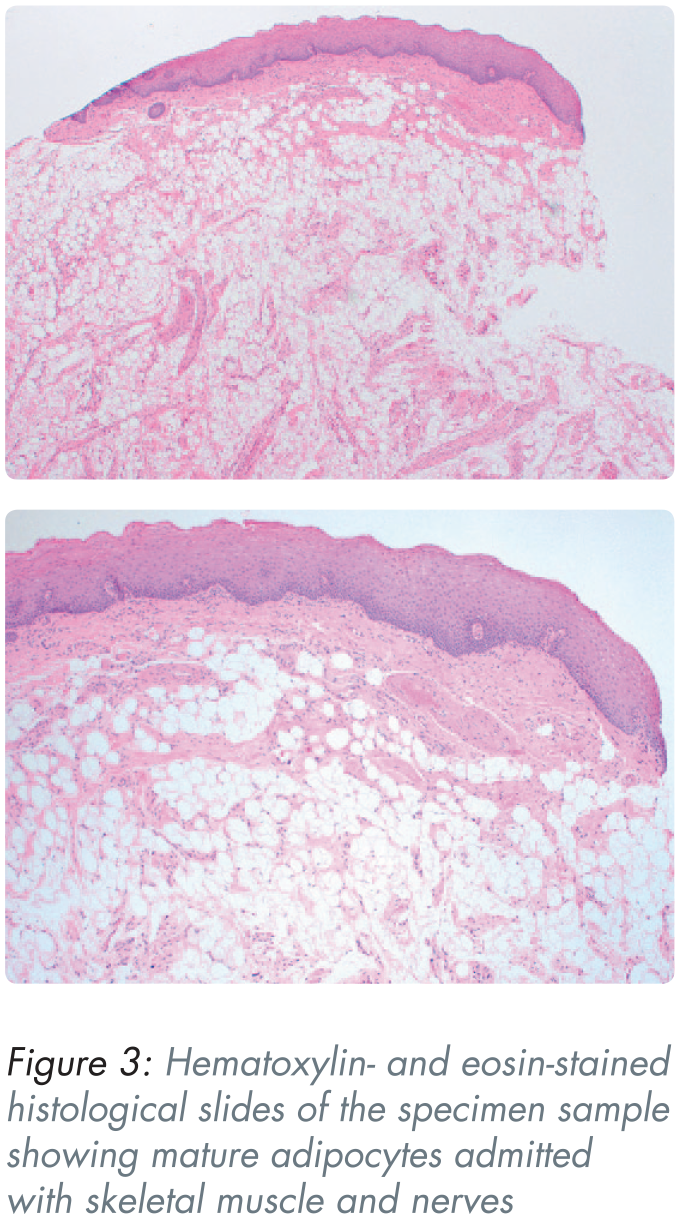
Biopsy
An incisional biopsy of the mass was carried out under local anaesthetic. Microscopic analysis of the sample showed tongue squamous mucosa containing lobules of mature adipose tissue, admixed with skeletal muscle and nerve fibres, consistent with a lipoma (see Figure 3).
Management
Due to the benign nature of the lesion and its asymptomatic features, the patient wished to monitor the lipoma. We discussed the options of surgical excision; however due to the risks to the lingual and hypoglossal nerves the patient did not feel as though the benefits outweighed the risks and preferred to adopt a conservative approach. The patient had been warned of the potential risk that the lesion may increase in size and interfere with function. The patient has been booked for an annual review in the oral and maxillofacial clinic; however he has also been given the option to attend sooner should he have any concerns.
Discussion
Lipomas commonly present as slow growing with a soft consistency, yellow in colour (when superficial), and generally asymptomatic. In rare instances, however, the sheer size of the lipoma can apply pressure onto the surrounding nerves and cause muscle dysfunction or sensory changes. 4
In the oral cavity, lipomas are more commonly located in the buccal mucosa, but lipomas of the tongue, gingiva, retromolar pad, and the floor of the mouth have also been reported. 5 While the site predilection is still under consideration, it has been hypothesised that this is related to the availability of adipose tissue, which would explain the high incidence in the buccal mucosa due to the proximity to the buccal fat pad. 6 Lipomas of the tongue represent only 0.3% of all tongue neoplasia5,7,8 and these are rare as the tongue is usually totally devoid of any fat cells. While Naruse et al. (2014) reported that tongue lipomas account for 16.6% of all oral lipomas, a more recent study by Osterne et al. (2019) recorded a lower prevalence of tongue lipomas, accounting for 6.93% of oral lipomas.9,10 This study also found that almost half of all cases (44.5%) were accounted for in the buccal mucosa, followed by the lower lip (12%) and retromolar area (10%). 10 The reduced prevalence of oral lipomas located in the tongue could be due to a larger number of cases included in this study which may be more representative of the true population. While lipomas are twice as common in females over the whole body, there is little gender predilection when it comes to lipomas of the oral cavity. Rafieiyan et al. (2010) reported a slightly higher prevalence of fibrolipomas in females and simple lipomas in males. 11
Liposarcoma is a common differential diagnosis of lipoma due to the similarities in clinical presentation. However, histologically, liposarcomas feature lipoblasts, cellular pleomorphism, marked vascularisation, and increased mitotic activity. 4 Additionally, there is no evidence to suggest the formation of liposarcoma from lipomas. 12
While the aetiology of lipomas is still unclear, a number of causative factors are known to play a role in the pathogenesis of these lesions. These factors range from trauma, chromosomal abnormality, hereditary, chronic irritation, hormonal imbalance, and metabolic conditions. 5
Several treatment options are discussed in the literature, such as liposuction or injections of intralesional steroids combined with isoproterenol (a beta-2 adrenergic agonist), with surgical excision of the lipoma seeing the greatest success. 4 The general prognosis of surgical excision is good, with a low recurrence rate. It is vital that the fibrous capsule surrounding benign lipomas, like the one discussed in this case, is entirely removed to reduce the risk of recurrence.
The benefit of surgical excision is to prevent the lesion enlarging and encroaching on surrounding anatomical structures, potentially compromising function. The lesion in this case was asymptomatic and considered too large for excision without considerable risk of patient morbidity. It is therefore currently being monitored in accordance with the patient’s wishes.
Conclusion
Lipomas in the oral cavity may grow unnoticed by the patient. GDPs and other dental healthcare professionals involved in examining the oral cavity are ideally placed to identify intra-oral soft tissue lesions, such as lipomas, and refer patients to secondary care for specialist opinion and/or investigation. The case presented in this report should aid dental healthcare professionals in considering a lipoma as a differential diagnosis when encountering patients presenting with similar lesions.