
Abstract
Accurate working impression is an essential requirement for the fabrication of implant prosthesis, and digital impressions have recently become more popular. In this case report, a completely digital workflow is introduced for the fabrication of three single-unit screw-retained implant crowns on the posterior maxilla by a dental student, under supervision. This approach involved the use of an intraoral scanner to capture a digital impression of the three implants and their surrounding mucosa, the opposing arch, and occlusion. The use of intraoral scanners and digital impressions illustrated an efficient and patient-friendly method of capturing the necessary data to fabricate a well-fitted prothesis. The aim of this case report is to examine a fully digital approach in the production of multiple single-unit implant crowns.
Learning Objectives
To describe how to use an intraoral scanner for digital implant impression
To discuss advantages and disadvantages of digital and analogue workflows for implants
To describe the steps for fabrication of implant-supported crowns
Introduction
Dentistry has recently undergone a shift from traditional fabrication methods to digital procedures, including different intraoral scanners (IOS) and software programmes.1,2 Such an advancement allows for better communication between the clinician and the laboratory technician. This improvement has proven to yield superior results for patients, eliminating errors commonly associated with conventional dentistry. 3 There are no longer concerns related to distortion of impression material or the transport of cases to the laboratory. Research indicates a preference for intraoral scanning compared to the conventional method, including shorter appointments and greater patient satisfaction. 1 The use of IOS provides enhanced comfort for patients, particularly those dealing with certain conditions such as severe gag reflex, limited jaw opening or breathing challenges.
Another positive aspect of the digital procedure is its ease of adjustment or rescanning, contrasting with the conventional method where an entirely new impression would be necessary. Additionally, the precision of these devices has been demonstrated to meet clinical standards and is particularly advantageous for implant impressions. Unlike subgingival crown margins, the software easily detects the scan bodies utilised, facilitating a streamlined digital workflow for the fabrication of implant-supported prostheses. However, it is important to note that using an IOS also comes with its drawbacks, including its sensitivity to the clinician’s skills, the need for a saliva-free and blood-free environment, and obstacles such as the movement of the tongue or cheek. 4 The aim of this report is to present a case with three implant crowns by using a digital workflow.
Case report
A 48-year-old male with no significant medical history presents to the dental clinic with concerns about his posterior dentition, with his chief complaint “I have missing teeth in the back and I want to chew again”. A comprehensive clinical and radiographic examination was completed and showed partially dentate maxilla and mandible. All maxillary and mandibular molars, as well as the right maxillary second premolar, were missing. Implants were present in edentulous sites of the right maxillary second premolar (UR5) and first molar (UR6) and the left maxillary first molar (UL6). Different treatment options were given, and the patient decided on fixed restorations. This treatment plan involved the insertion of screw-retained implant-supported crowns on implants in edentulous sites of the UR5, UR6 and UL6, to restore form and function.
Under local anesthesia, three dental implants were placed without any problems. The patient returned after six months of proper healing and osteointegration for stage 2. Each implant was exposed, and healing abutments were screwed on the implants.
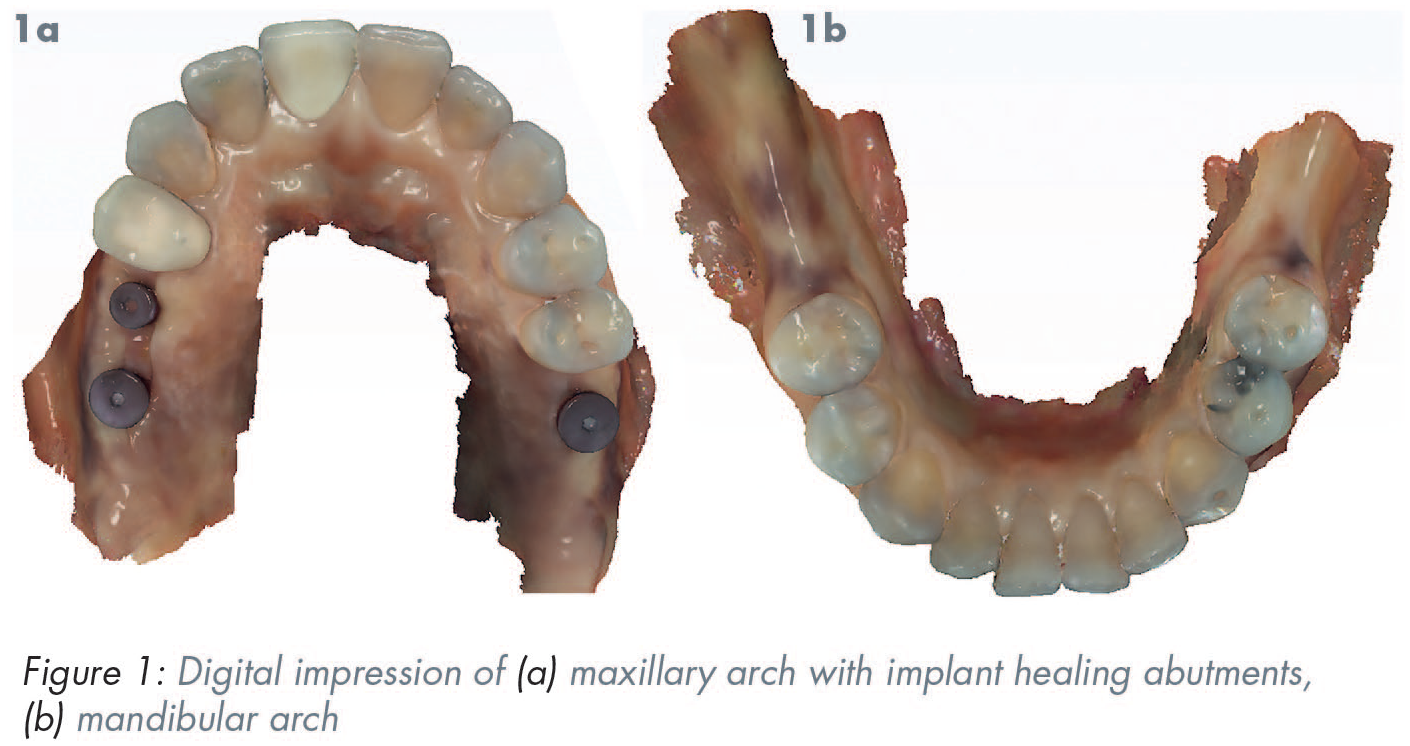
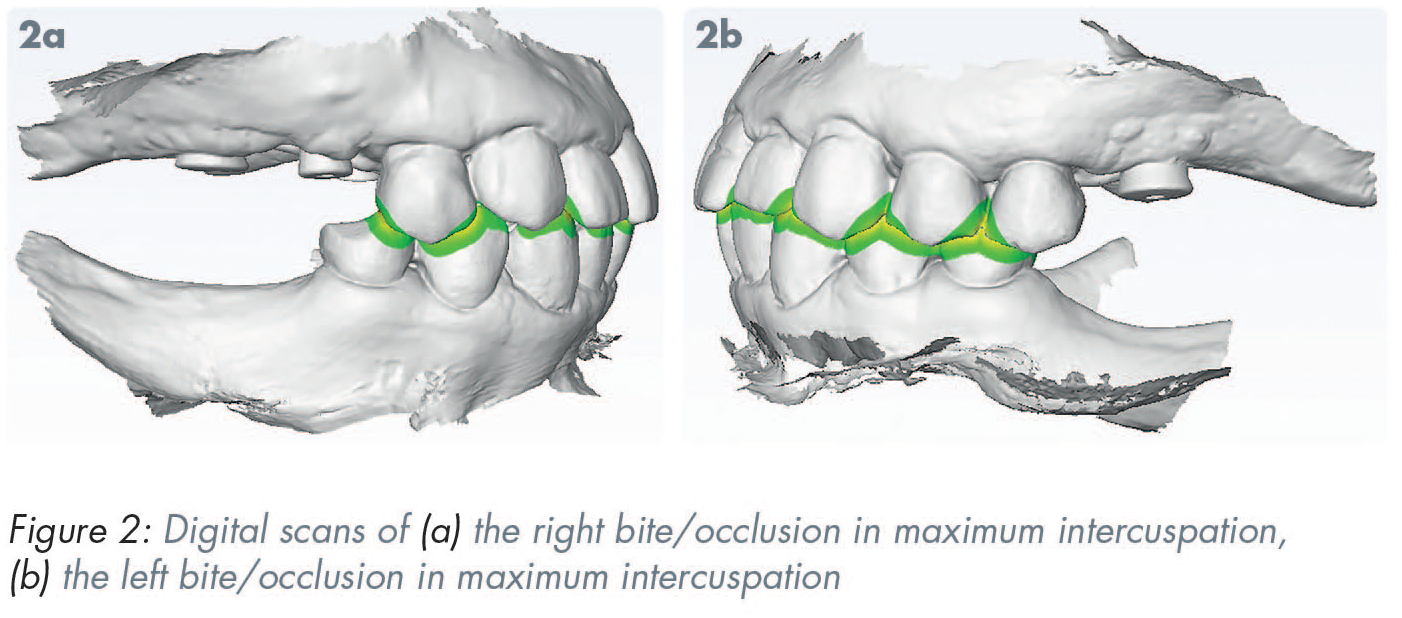
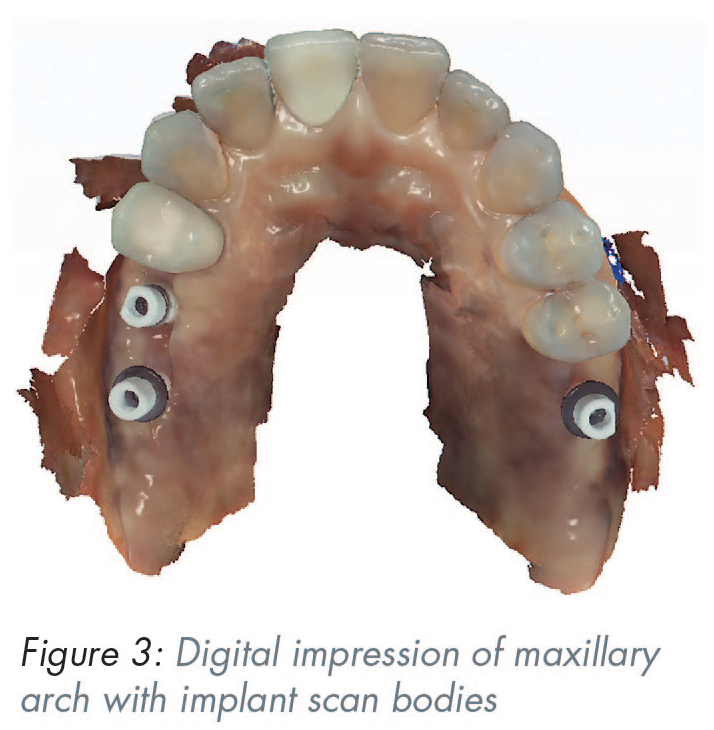
During the restorative stage, the digital workflow was utilised for the maxillary single-unit screw-retained implant crowns. Using an IOS (Planmeca Emerald S, D4D Technologies LLC, Richardson, TX, USA), the maxillary arch was scanned, including the remaining dentition, healing abutments and surrounding soft tissue. The IOS followed the scanning path recommended by the manufacturer, starting with the occlusal surface (the tip of the scanner pointing towards the distal) and moving mesially to capture the healing abutments, surrounding soft tissue and proximal surfaces of adjacent teeth. Afterwards, the opposing mandibular arch was captured, and the patient’s bite was recorded by scanning the buccal of the dentition while in maximal intercuspation (Figures 1 and 2). The healing abutment of each implant was unscrewed and replaced by a scan body. The 10mm-long scan body was screwed into the implant and torqued to 5Ncm. A radiograph was taken to confirm seating of each scan body. The cylinder-shaped scan bodies had one flat proximal surface, allowing the IOS to determine the exact position of each implant. The maxillary arch was then scanned a second time using the IOS to capture the scan bodies and surrounding structures (Figure 3). The digital impression of the scan bodies and the healing abutments, the opposing arch impression, and bite registration were sent to the laboratory where a three-dimensional (3D) model was printed. A digital laboratory prescription was placed requesting the fabrication of three screw-retained implant crowns in selected shade. All healing abutments were hand-screwed back on the implants.
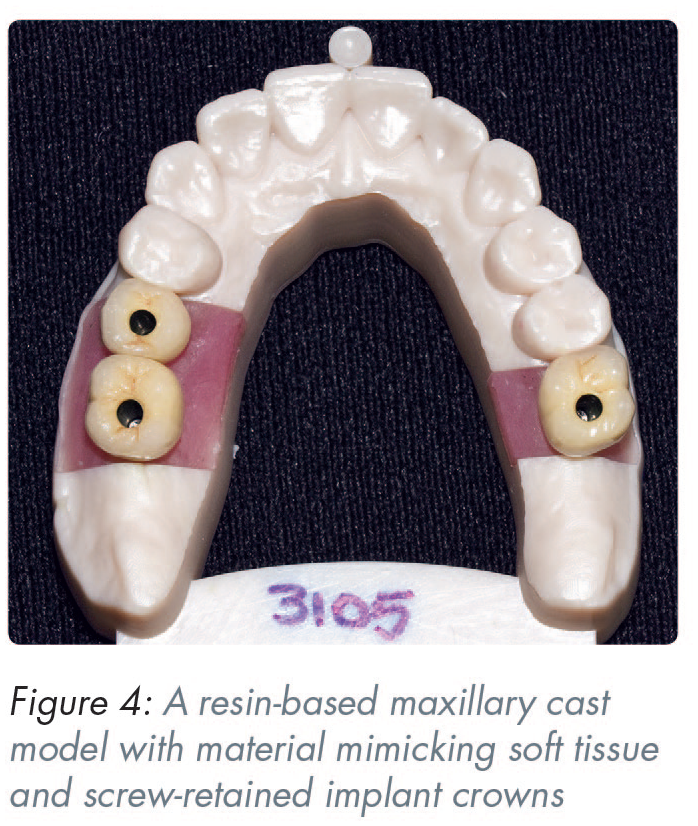
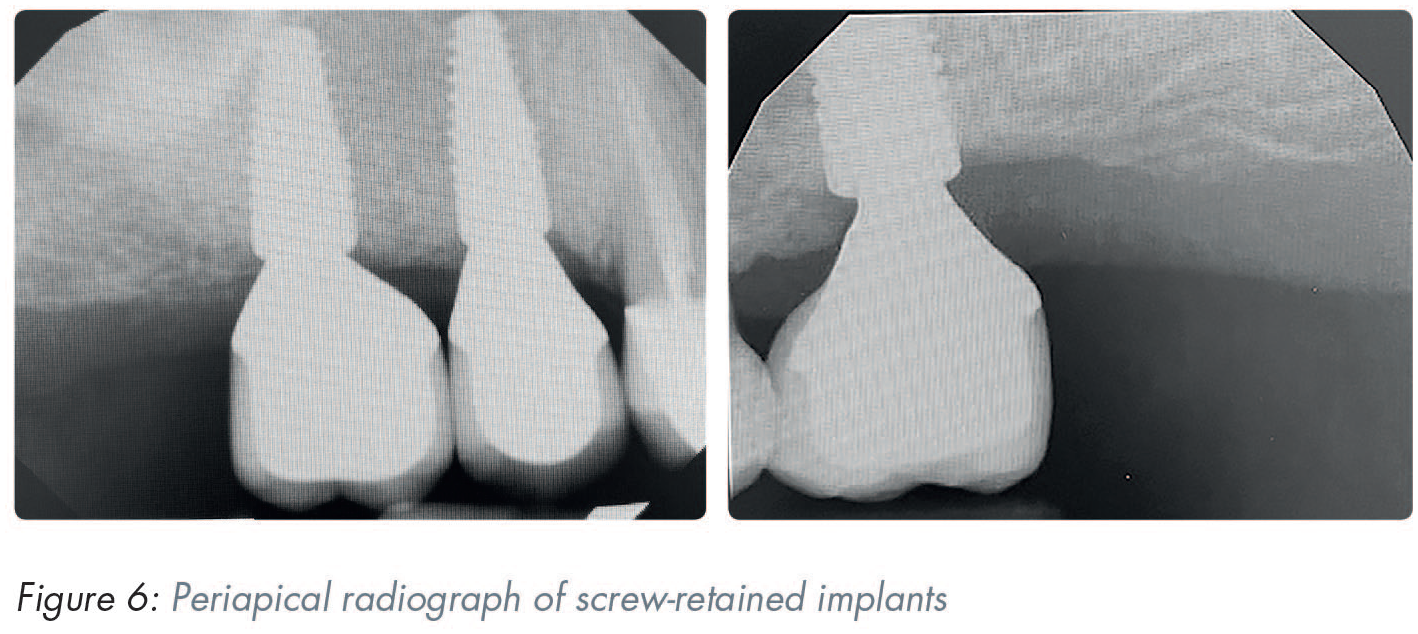
The laboratory received the digital data necessary to produce the desired crowns. A resin-based maxillary cast model with material mimicking soft tissue around the analogue and the opposing arch were printed. The library of scan bodies allowed for the creation of a virtual cast with the corresponding implant analogue. Using the lab prescription, the requested crowns were fabricated with porcelain baked onto the custom-milled metal abutments, glazed and polished to achieve an aesthetic appearance (Figure 4). The patient returned after two weeks. The screw-retained implant crowns for the UR5, UR6 and UL6 were fitted, and a periapical radiograph was taken to confirm the seating of each crown (Figures 5 and 6). The placement of the crowns was completed without any challenges. No adjustment was needed in the proximal areas. The implant crowns were tightened to 35Ncm using a torque wrench. Teflon tape and composite resin were placed in the screw access channel and light cured. The patient was satisfied with the crowns and was provided with hygiene instructions.

Discussion
This case report aimed to assess the digital workflow of maxillary single-unit screw-retained implant crowns. When comparing such a digital method to the traditional use of impressions materials, there are many advantages to consider. First, a digital workflow is more cost-effective due to the decreased chairside time and reduced usage of traditional materials including stone and impression material.5,6 In addition, digital methods tend to result in less distortion compared to traditional casting methods which involve uneven cooling rates and contraction of the different materials. Digital workflow uses a computer-aided design to create a virtual model of the desired prothesis and 3D milling methods to carve the final prothesis from a block of selected material. Such milling does not require the same amount of heat associated with traditional methods, resulting in less distortion, and thus, a more accurate and precise fitting prothesis. In a previous study by Abduo at el., 7 the authors investigated the trueness, precision, inter-implant distance deviation and angle deviation between parallel and tilted implants when using conventional and digital techniques. The findings of their study indicated an overall tendency for digital impressions to exhibit greater accuracy compared to the conventional impressions. There was a notable difference for the divergent implant model where the use of conventional impressions was more susceptible to errors than the digital impression. In this fully digital approach, there is also no need for storage of stone models. Moreover, it provides more comfort for patients, particularly those with limited jaw movement and severe gag reflex. In a previous study by Yuzbasioglu at el., 8 the authors compared the provider and patient perspectives using digital scanning and conventional impressions. They demonstrated that the majority favoured the digital method.
This case was completed by a fourth-year dental student under the supervision of a prosthodontist. Thus, if any adjustment needed to be made due to the student clinician error, additional scanning could be completed instead of taking an entirely new traditional impression. Additionally, in the event of the clinician needing to remake the prothesis, all information was digitally stored, allowing for a replica of the original product to be rapidly fabricated. Limitations of the digital technique include the need for a saliva-free and blood-free setting, and challenges presented with different obstructive anatomical structures.
Conclusion
This case report showed the efficiency of a fully digital approach of maxillary single-unit screw-retained implant crown fabrication in a partially dentate patient.