
Abstract

Introduction
In the ever-changing world of dentistry dental practitioners must keep pace with scientific and technological advancements, alongside the changing needs and expectations of patients. To this effect, dental implants have become a game-changer for the replacement of missing teeth, offering a durable and predictable alternative to conventional dental prostheses. As clinical implant dentistry is not widely taught at undergraduate level those just starting out in their dental career may find it challenging breaking into this field. A plethora of postgraduate short and long courses, and academic programmes with substantial practical/clinical components are available and promoted through various channels. The length and intensity of such postgraduate education opportunities vary greatly, influencing the experience of the trainee in terms of both clinical experience and knowledge gained. While nothing can substitute for clinical experience, diving straight into implant dentistry without appropriate support through a personal mentor is far from ideal. This article outlines how having a mentor makes a significant difference for dental professionals learning the ropes of implant placement, and why those who have had this support might consider mentoring others.
Why mentoring matters in dental implantology
Implant dentistry is a very different treatment modality compared to regular dentistry and requires a completely new set of skills and knowledge. When new skills are introduced or enhanced in other dental areas, for example restorative dentistry, the clinician is building on what they have already learned during the process of becoming a dentist. New information must be acquired, but the academic and hands-on basics are already in-built. However, with dental implants many things are new, from assessment and planning through to clinical performance.
Although implant dentistry is increasingly taught in undergraduate dental schools in the UK and across the world, the extent of clinical implant education is limited.1,2 Consequentially, most dentists train in implant dentistry after their initial dental training, in postgraduate courses of different lengths and with varying content; 3 some attend weekend study sessions, while others take full-time MSc degrees4,5 or embark on specialist clinical training programmes that include implant dentistry, i.e. restorative dentistry. What is clear, however, is that those learning to be implant surgeons feel they need someone to advise, assist, and generally be there for them during the early stages of their practical career. 6 This is especially relevant during surgical procedures, as it is not uncommon to need to make decisions ‘on the spot’, so there is no time to wait for later discussions with more experienced clinicians. This makes having in-person support during surgery especially valuable, particularly in those early cases when everything can feel a bit overwhelming. 7
This article uses one of the authors’ real-life example of mentorship in implant dentistry to demonstrate why having a mentor is so important in turning theoretical knowledge into practical skills. This story will share personal experiences, talk about challenges faced, and show how mentorship can transform someone into an expert in this exciting field. When the mentee feels able to become the mentor, future dentists continue to benefit from this initial mentoring experience.
The mentee’s journey: navigating the maze of dental implant training
It is likely that, if asked, every clinician would have a slightly different story of their route into implant dentistry. The following first-hand experience is written from the perspective of one of the co-authors (B.S-I) and contains elements which many other aspiring implant dentists can relate to, but equally has its own unique set of circumstances impacting on the final outcome. It is worth highlighting at this point that most individuals will bring a unique set of both professional and personal circumstances which may influence the development of their surgical skills. It should not be overlooked that the mentee, as well as the mentor, has much to contribute.
“Embarking on the journey into implant dentistry in 2012 marked a significant juncture in my professional life. Relatively fresh from completing my undergraduate studies in 2009 and after a one-year postgraduate training in restorative dentistry and another one-year course in oral surgery, I anticipated that a one-year dental implant training programme would seamlessly combine these two together and equip me for this new trajectory. However, reality unfolded quite differently.
“Dental implants were not merely an expansion of my existing skill set: they demanded an entirely new practice setting. Beyond acquiring fresh knowledge and skills, the challenge encompassed adapting to a new environment – with new equipment, staff requirements, and, especially in the UK, an environment where the NHS does not support dental implant treatment in primary care. This necessitated the establishment of novel work routines and environments, adding layers of complexity to the learning curve.
“After my initial year of implant dentistry training, I found myself lacking the confidence to independently provide implants. Attributing this to a perceived deficiency in training, I sought a more extensive solution, enrolling in a three-year part-time MSc programme dedicated to dental implants. I was sure that this was the solution to all my problems and would provide me with the practice I needed. However, challenges persisted.
“At that time, my struggle was exacerbated by difficulties in patient recruitment for treatment, especially in a predominantly NHS practice where advising patients on the merits of dental implants proved to be an uphill battle. In a bid to augment my practical experience, I sought a programme that included a clinic with its own patient pool. While this addressed certain gaps (and I did treat a few patients), I still did not feel the confidence building as I had hoped, and a crucial element remained elusive – my own work environment.
“Back in my own workplace, I grappled with a dearth of confidence, a scarcity of willing patients for practice, and the substantial financial investment required for both training and equipment procurement. The intricacies of treating complex cases compounded my insecurities, with the added challenge of triaging cases in the absence of readily available guidance.
“As the years passed, my academic knowledge expanded through the MSc programme, culminating in the completion of a systematic review. Yet, the gap between academic prowess and practical proficiency remained pronounced, leaving me with a sense of unreadiness to independently provide implant treatments in my daily practice.
“In a quest for guidance, I initially shadowed an implant surgeon, but the limitations of passive observation soon became evident. I also engaged with an implant surgeon to assist in my practice which also proved unproductive as, without any formal discussion of mentoring, this quickly transitioned to yet another situation where I was the observer, and I was unable to actively participate in the treatment process.
“The turning point arrived when I secured a position as a General Dental Practitioner (GDP) in a private specialist practice where dental implants constituted a significant portion of the patient base. Although I did not initially start placing implants myself, I immersed myself in various stages of implant dentistry – diagnosis, planning, second stages, photography, and handling implant-related emergencies. This multifaceted involvement significantly contributed to the development of both confidence and practical knowledge. Moreover, I found an experienced clinician willing to mentor and guide me, transforming me into the competent implant dentist I now am.
“While I was extremely grateful that I was finally able to receive the clinical support and guidance I had been lacking, it is well worth considering what mentees have to offer when approaching potential mentors. I was able to take on a large degree of implant-related work (as detailed above) meaning the time I ‘took’ from my supervisor I was in some part ‘giving back’ in kind.
“As I progressed, I was presented with the opportunity to get involved in teaching – a prospect I embraced wholeheartedly as teaching is one of the most powerful tools for maintaining personal learning and a very fulfilling activity, as well as a fantastic complement to clinical work.
“Although I acknowledge the uniqueness of my situation, I believe it could serve as inspiration for colleagues seeking new development options. Many colleagues from my MSc programme did not achieve similar milestones, with only a minority placing implants by the course’s end, mainly those colleagues who had prior experience before the course began.”
Becoming the expert: transitioning from mentee to mentor
“After several years of improving my skills as an implant surgeon, with a focus on the surgical aspects of implant and oral surgery, I found myself drawn to the prospect of guiding others in their professional journey. It was a natural evolution, a transition from being mentored to assuming the role of a mentor. This phase marked a mindset shift – from absorbing knowledge to sharing acquired wisdom with those embarking on their own paths in implant dentistry.
“In aligning with this new mission, I decided to contribute to a mentorship programme. In 2015, the practice in which I now work and teach, in partnership with a global implant company, established its own standardised mentoring initiative. This programme delineated clear conditions and fees, operating with a network of verified mentors who shared similar principles.
“Mentoring is a significant investment of time, often involving travel and a notable jump in responsibility. The responsibilities associated with guiding others differ substantially from the challenges encountered in one’s own professional growth – an evolution from the possibility of creating a mess to sorting out one! Nevertheless, armed with the eagerness to share my experience, I embraced this role.
“As part of the programme, clear expectations are set, and communication channels are established: this includes shared secure access to all relevant patient files (cone beam computed tomography [CBCT], Wax up STL [standard tessellation language] file, photos, checklists and any other planning documents), and using a work-based communication platform for one-to-one discussions, but avoiding extending this into personal contacts excluding the potential to extend discussions well into the evening. Discussions/meetings pre-surgery to go through planning and materials can be undertaken at a pre-set time during work hours, either face-to-face or by video call. My personal commitment is limited to one day a month, either in a full-day session or two half-days, striking a balance that maintains an enjoyable workload.
“Clarity in fees proved pivotal; it ensures that mentors are compensated adequately for relinquishing a day of their own clinical practice to assist others. Determining the value of a mentoring session, both in realistic and worthwhile terms for the mentee, becomes a critical aspect of this process. In my workplace mentors charge a fee per session (half day or full day). This fee covers case discussion and surgical planning as required by the mentee, and face-to-face support on the day. We generally advise that up to four implants and two guided bone regeneration (GBR) procedures can be done in a full day session. Post-surgical discussions, feedback, and assessment of any complications is included in this arrangement. Online case discussion sessions are also available for ad hoc mentoring, charged at an hourly rate.
“It’s also important to consider patient communication – our mentoring programme has mentees in charge of communication with the patient and organising the surgical day, as this is an important part of the learning process. When it comes to treatment planning, we advise a straightforward case for all first cases undertaken under supervision in the mentee’s practice: at this point it is not only the mentee who is learning but also their team who need to learn a new surgical set up and become familiar with a new range of equipment and materials. As the mentee progresses, arrangements can be made for more complex cases (e.g. sinus grafting, advanced GBR). These can be done in the mentee’s practice, but we prefer to oversee these in our own practice at least initially, again due in part to the whole team’s familiarity with materials and equipment.
“Working with an array of remarkable clinicians has been a source of immense joy. Each mentoring session, a journey in itself, offered a unique opportunity to contribute to the growth of aspiring implant dentists. The camaraderie established in the mentorship programme was grounded in mutual understanding, and the satisfaction derived from seeing mentees progress was immeasurable.
“Most of the individuals seeking mentorship emerge from our practice’s own academic training programme, providing a valuable continuity. Having previously taught them, I possessed an intimate understanding of their knowledge base, fostering a seamless transition into the mentor-mentee relationship. Thus far, the progress of all mentees has been commendable, instilling confidence in the effectiveness of structured mentorship programmes.
“For those where geographic location has been more of a challenge, we have leveraged our network to identify suitable mentors within the mentorship programme. This network-based approach facilitated connections for those who previously lacked local mentors. Encouraging mentees to establish clear and fair conditions in their mentoring relationships became a recurrent theme, ensuring a mutually beneficial and sustainable engagement.”
The journey from mentee to mentor, as delineated in this section, illuminates the transformative nature of mentorship in implant dentistry. It not only signifies personal growth but also underscores the responsibility that comes with guiding the next generation of implant surgeons. Of note, since the journey outlined here, the College of General Dentistry have published Mentoring in Implant Dentistry: Good practice guidelines. 8 This will be of great benefit to mentors and mentees and assist in standardising the mentoring process, while still allowing for individual variation in the relationship.
What makes a mentor great and a mentee successful?
As the mentorship journey unfolds, it becomes paramount to reflect on the qualities that elevate a mentor from being good to great, and the attributes that distinguish a mentee on the path to success.9,10 Outlined below are the pivotal aspects that shape a thriving mentor-mentee relationship in implant dentistry.
Talking at the same level
Effective communication is the bedrock of any mentorship dynamic. A great mentor understands the significance of dialogues that avoid any implication of hierarchy. By engaging in open and candid conversations, mentors will foster an environment of trust and collaboration. This ensures that mentees feel comfortable sharing their concerns, uncertainties, and triumphs.
Delegating and correcting
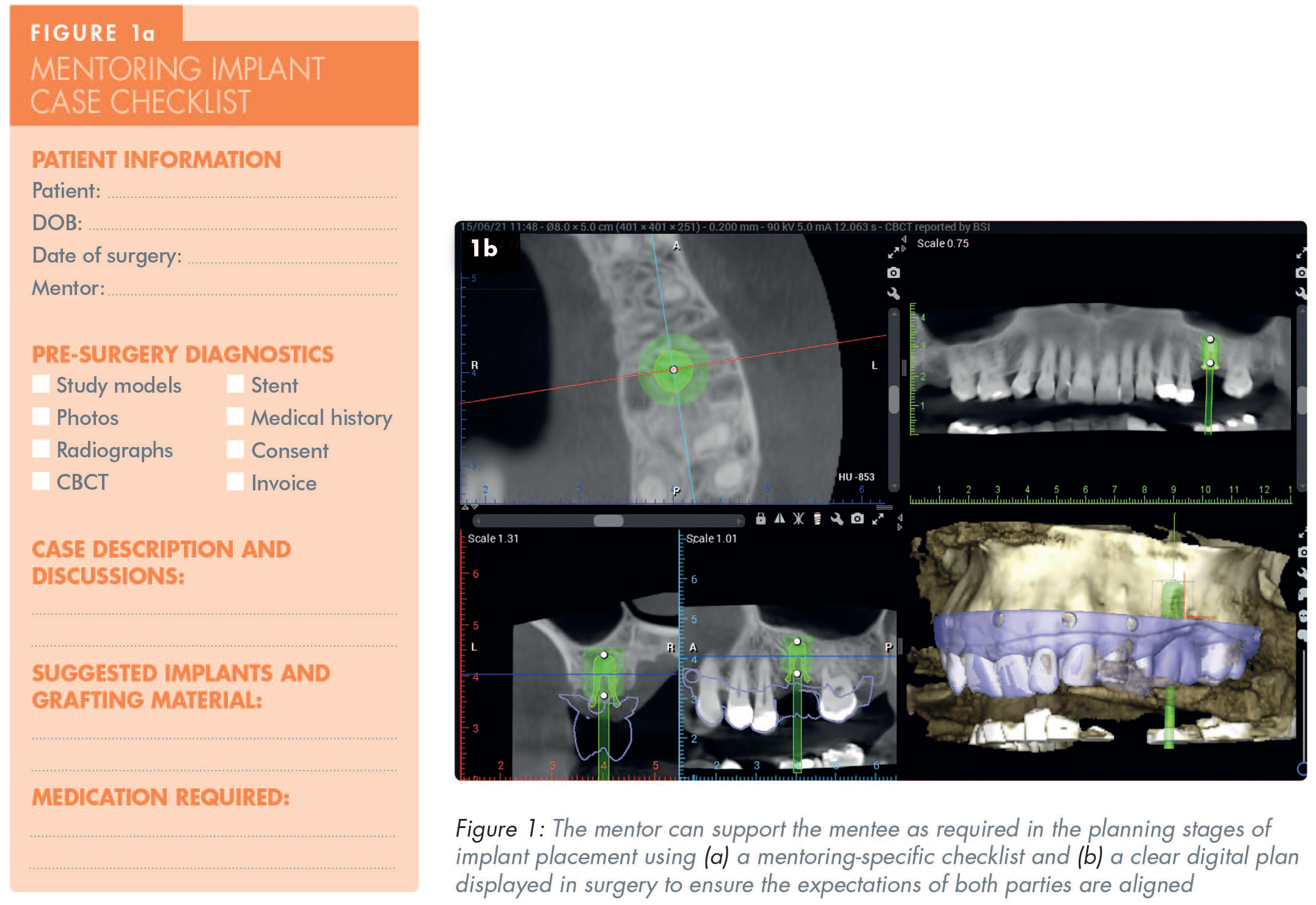
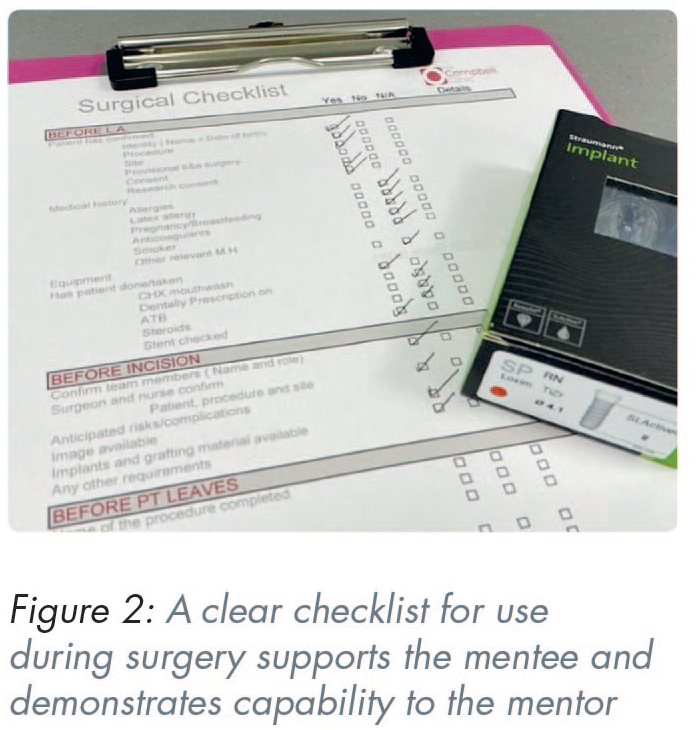
A great mentor recognises the importance of letting the mentee take charge. This involves delegating tasks, allowing them to plan, organise, and even make mistakes (Figures 1 and 2). However, the mentor’s role is not passive; it involves a keen eye for identifying areas that need correction. Offering timely guidance and constructive feedback is essential in refining the mentee’s skills and promoting continuous improvement.
Multiple opportunities to check
Checklists ensure work is consistent and organised, and are a huge benefit in a learning environment. They help to make sure cases are properly prepared, nothing is missed, and that both parties know what to expect. A mentoring-specific checklist (Figure 1a) can be used by both mentee and mentor for all case planning and discussions. This can be supported by a surgery checklist (Figure 2) to document and check that all required materials are available. This is vital in a mentoring situation where at least one party will be working out of their own environment, and with a different team.
Developing the clinician within
An exceptional mentor understands that each mentee is unique, possessing distinct aspirations and visions for their clinical practice. Nurturing individuality is crucial. Encouraging the mentee to develop into the clinician they aspire to be involves providing tailored guidance that aligns with their professional goals. This approach ensures that mentees don’t merely replicate the mentor but evolve into practitioners with their own distinct identities.
Growing, developing, and letting go
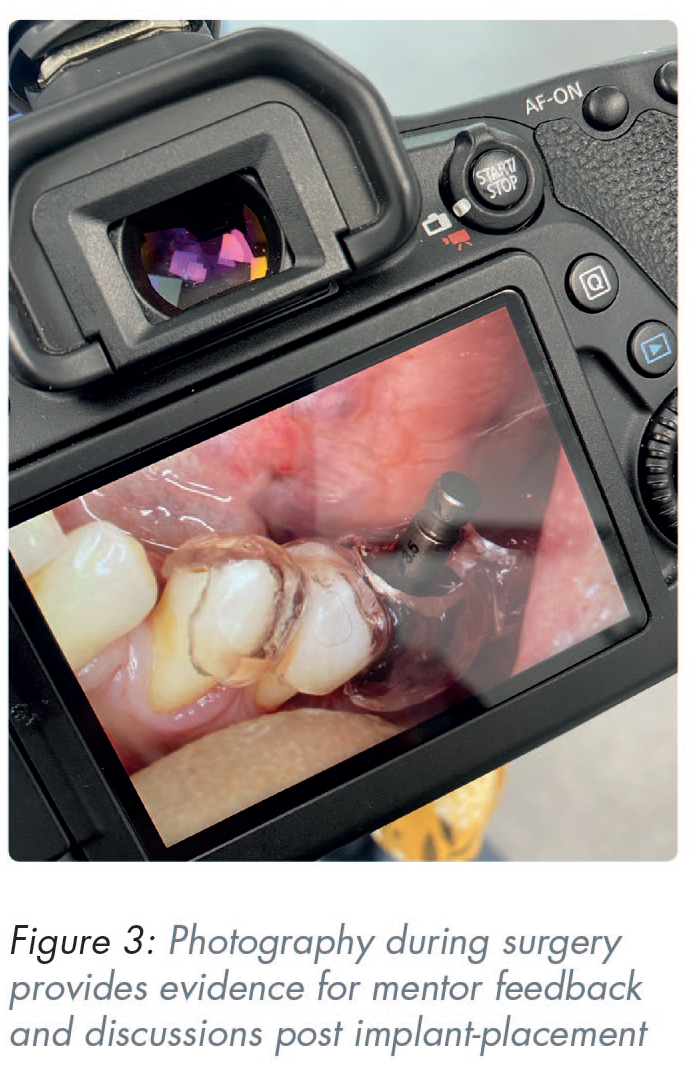
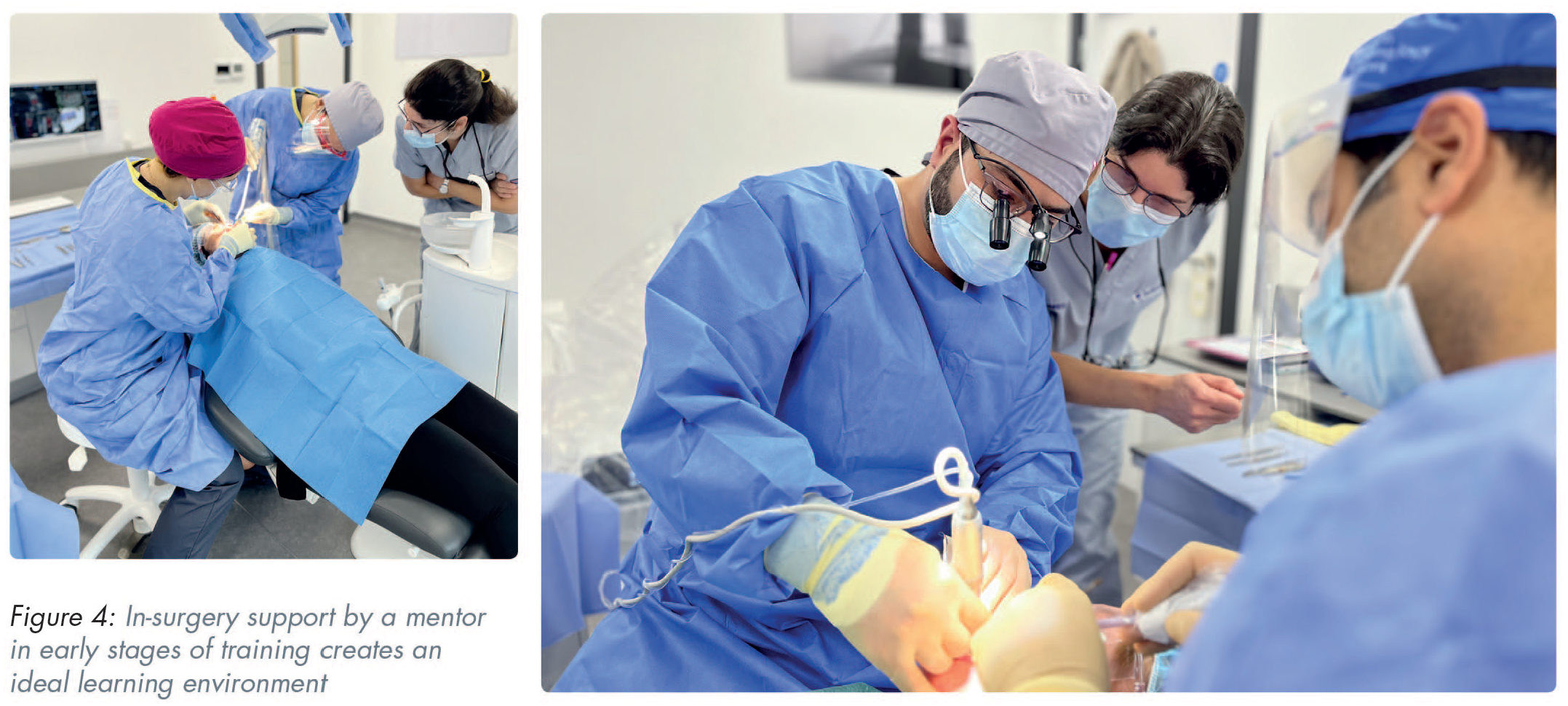
A hallmark of a great mentor lies in their ability to foster growth, facilitate development, and eventually let the mentee spread their wings independently. While continuous guidance is indispensable, a mentor recognises the importance of encouraging mentees to become self-reliant practitioners. The mentor’s role shifts from active guidance to a supportive presence, instilling confidence in the mentee’s ability to navigate the complexities of implant dentistry (Figures 3 and 4).
Sustaining the mentor-mentee relationship
The mentor-mentee relationship is not bound by a specific timeframe; rather, it is an ongoing journey of mutual growth. Beyond face-to-face mentoring sessions, embracing digital avenues for continued support is essential. Online mentoring platforms offer a space for regular case discussions, collaborative treatment planning, and quick checks on decision-making processes. This virtual engagement ensures that the mentor remains a valuable resource even as the mentee advances to more complex cases.
Assistance with challenges and failures
The mentor’s role extends beyond successes: it encompasses providing support during challenges and failures. A great mentor understands that setbacks are inevitable in the learning process. Whether a mentee is facing difficulties with a complex case or encountering unexpected complications, the mentor offers a helping hand. This assistance is not just about problem-solving; it also involves imparting the resilience and problem-solving skills necessary for overcoming obstacles.
Conclusions
In the dynamic field of implant dentistry, the journey from mentee to mentor is truly transformative and empowering. Recognition of the unique challenges posed by implant dentistry is key, and the crucial role that mentorship plays in shaping competent professionals underlines the necessity for guidance during the early stages of professional development. The qualities that make a mentor great and a mentee successful are intertwined in a symbiotic relationship. The mentor’s ability to communicate effectively, delegate and correct, nurture individuality, facilitate growth, and sustain ongoing support sets the stage for the mentee’s success. Simultaneously, a successful mentee is characterised by their receptivity to guidance, proactive involvement in their development, aspiration for individuality, readiness to embrace independence, and an understanding that the mentor-mentee journey is an enduring collaboration.
The personal journey shared here reflects the intricacies of transitioning from a learner to a mentor including the challenges faced during implant training, such as adapting to a new environment and the financial intricacies of practice. The fact that the narrative’s turning point lay in securing guidance from an experienced clinician, supports the clear need for a mentorship pathway. In addition, continuation of the mentor-mentee collaboration beyond face-to-face interactions using online platforms is key to ensuring ongoing development.
Perhaps the most important message is the recognition that mentorship not only fosters professional growth for all involved, but also instils responsibility for guiding the next generation of implant surgeons, shaping a community of empowered and proficient dental professionals.
Footnotes
Acknowledgements
The authors would like to thank Dr Kath Hare, Research Manager at The Campbell Clinic, for her constructive review and editing of this article. Thanks also to Straumann for their support and partnership to establish the standardised mentoring programme as outlined in the above first-hand account.