
Abstract
Temporomandibular disorders (TMDs) comprise a heterogeneous group of conditions affecting the temporomandibular joints, masticatory muscles, and associated structures. Occlusal splint therapy remains one of the most prescribed conservative interventions for the management of TMD. However, considerable debate persists regarding its mechanism of action, clinical indications, and comparative effectiveness relative to other conservative management strategies. This article provides an overview of splint therapy in the management of TMD, focusing on stabilisation splints, anterior repositioning splints, and Nociceptive Trigeminal Inhibition Tension Suppression System (NTI-tss) appliances.
Keywords
Learning Objectives
To understand the proposed mechanisms of action of occlusal splints in the management of temporomandibular disorders
To obtain an overview of the use of occlusal splint appliances in the management of TMDs
To identify potential complications associated with partial-coverage appliances and the importance of clinical monitoring
Introduction
Temporomandibular disorders (TMDs) encompass a range of conditions affecting the masticatory muscles, temporomandibular joints (TMJs), and associated structures. Among the conservative management options available, occlusal splint therapy remains a commonly prescribed and widely studied intervention. However, given the diversity of proposed mechanisms and treatment protocols, it is imperative that clinicians adopt an informed approach, balancing clinical expertise with the best available research and individual patient values. 1
Contemporary approaches to TMD management
Modern dental care must be rooted in robust scientific evidence. As Carlsson emphasised, long-standing clinical dogmas in prosthodontics and occlusion often lack empirical support. 2 Echoing this, the Swedish Council on Technology Assessment in Health Care warns against disregarding evidence in patient care. 3
Indeed, while randomised controlled trials (RCTs) and systematic reviews with meta-analysis offer the highest level of evidence, many clinicians rely on outdated or weakly-supported approaches.
Clinical guidelines should be informed by the integration of high-quality evidence, clinician expertise, and patient preferences. However, methodological challenges in TMD research (e.g. inconsistent diagnostic criteria, variable outcome measures, and heterogeneity in patient populations) have hampered the development of definitive treatment algorithms. 4
Mechanisms of splint therapy
Occlusal splints are designed to alter the occlusal environment and masticatory muscle function, with proposed mechanisms including:
Stabilisation splints: myofascial pain and muscle activity
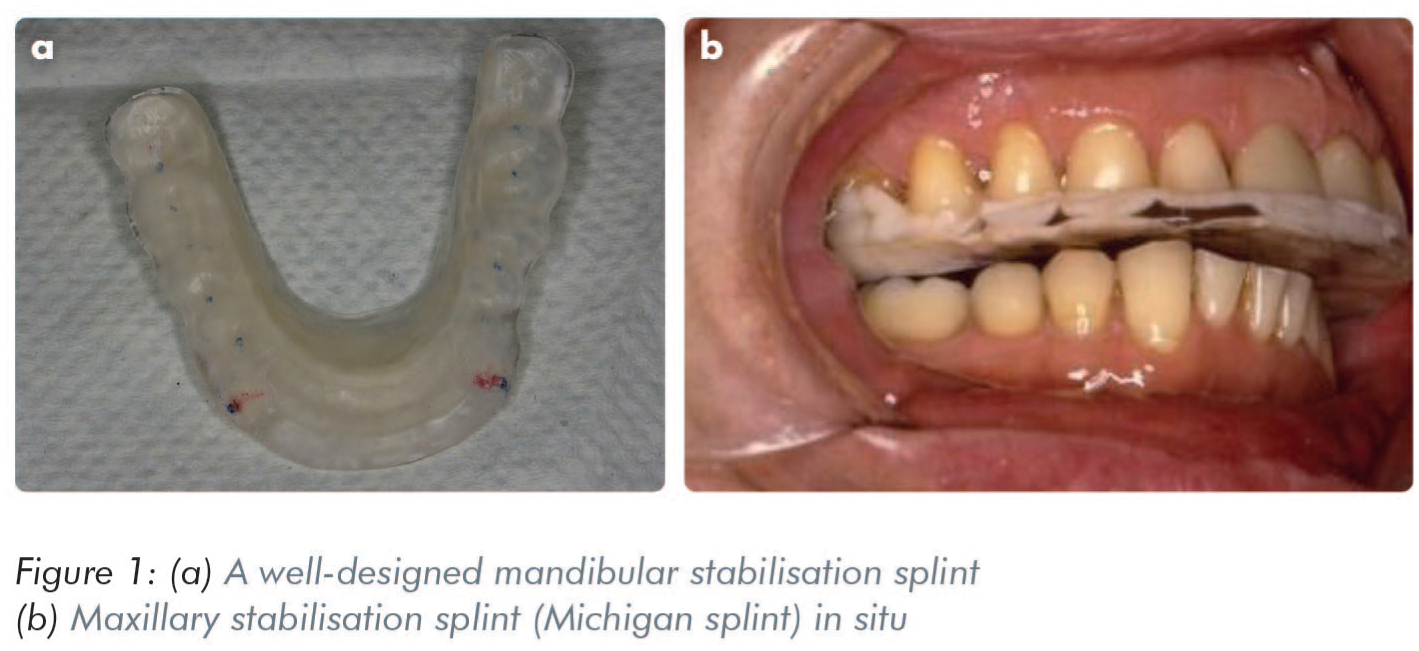
Stabilisation splints (SS) (Figure 1) are flat-plane appliances designed to promote neuromuscular relaxation and occlusal stability. Davies and Gray reported that properly adjusted SS can reduce pain and improve function in patients with myofascial pain, a myogenous form of TMD. 8
Numerous electromyography (EMG) studies have confirmed reduced activity in the masseter and temporalis muscles during SS therapy.9,10
Emshoff and Bertram further demonstrated that short-term SS use can decrease muscle cross-sectional dimensions, reinforcing its physiological impact. 11
A systematic review by Al-Ani et al. examined the effectiveness of SS therapy in the treatment of temporomandibular myofascial pain. 4 The review analysed RCTs and controlled clinical studies to determine the clinical outcomes associated with SS use. The findings indicated that SS were generally more effective than no treatment or placebo appliances in reducing myofascial pain in the short term. However, when compared with other conservative treatments such as counselling, physiotherapy, and behavioural therapy, the superiority of SS was not consistently demonstrated.
The review also highlighted significant variability across studies in terms of design, outcome measures, and follow-up periods, limiting the ability to draw strong conclusions. Overall, the authors concluded that while SS may be a beneficial component of conservative TMD management, they should not be regarded as a universally superior treatment. Further high-quality research with standardised methodologies is necessary to clarify their long-term efficacy and comparative advantage.
An RCT by Niemelä et al. showed that SS therapy significantly alleviated pain in patients with myofascial TMD over a 12-month follow-up period. 12 However, Cochrane reviews and subsequent meta-analyses suggest that while SS may provide short-term benefits, its long-term superiority over other conservative treatments is less clear.13 -15
In their systematic review of randomised controlled trials, Zhang et al. examined the efficacy of occlusal splints in the treatment of TMDs. 15 The review analysed a wide range of studies involving both myogenous and arthrogenous forms of TMD and found that occlusal splints, particularly hard SS, were generally effective in reducing pain and improving jaw function in the short term. The authors reported statistically significant improvements in pain intensity and maximum mouth opening in patients treated with splints compared to control groups. However, they emphasised that the magnitude of benefit varied across studies due to differences in diagnostic criteria, splint design, treatment duration, and follow-up periods. Importantly, the review also highlighted that while splint therapy was more effective than no treatment or placebo, it was not consistently superior to other conservative interventions such as physiotherapy or behavioural therapy. The same authors concluded that occlusal splints are a valid treatment option for TMD, but called for further high-quality, large-scale RCTs with standardised methodologies to strengthen the evidence base and guide clinical decision-making.
A comprehensive network meta-analysis by Al-Moraissi et al. evaluated the comparative effectiveness of various occlusal splints and conservative therapies in the management of TMDs. 16 The analysis concluded that hard SS were significantly more effective than non-occluding appliances and no treatment in reducing TMD-related pain and dysfunction. However, when compared to counselling therapy, a low-cost behavioural intervention, the additional therapeutic benefit of hard SS was minimal. Furthermore, the combination of counselling therapy with splint use did not yield superior outcomes compared to counselling alone. Soft splints and non-occluding appliances were found to be less effective than hard splints. These findings support the recommendation that counselling therapy should be considered the first-line treatment in patients with myogenous TMD, reserving splint therapy for cases that do not respond to initial conservative measures. The study also emphasised the need for well-designed RCTs with consistent diagnostic criteria, standardised outcome measures, and adequate follow-up durations to more definitively determine the long-term efficacy of splint interventions.
A recent systematic review by Orzeszek et al. evaluated the impact of splint therapy on muscle-related TMD pain. 17 The review synthesised findings from multiple clinical studies and concluded that occlusal splints, particularly hard SS, were effective in significantly reducing orofacial muscle pain, especially in patients diagnosed with myofascial pain. The greatest improvements were typically observed within the first few weeks of therapy, indicating a prompt clinical response. However, the review also noted that while splint therapy reduced pain intensity and improved function, the magnitude and duration of these effects varied depending on splint type, patient compliance, and the presence of contributing factors such as parafunctional habits or psychological stress. Overall, the study supports the inclusion of occlusal splints as a non-invasive, first-line treatment option for patients with muscle-based TMD, while highlighting the need for further standardised, long-term trials to confirm sustained benefits and optimal usage protocols.
Anterior repositioning splint (ARPS)
ARPS aim to recapture anteriorly displaced discs by guiding the mandible forward (Figure 2). Early evidence and more recent studies suggest that ARPS can be effective in treating disc displacement with reduction (DDwR) when worn continuously.7,18 -20

Kurita et al. and Eberhard et al. used magnetic resonance imaging (MRI) to confirm successful disc recapture in the majority of patients using ARPS.21 -23 However, long-term stability remains a concern. Chen et al. and Hiyama et al. showed that spatial disc-condyle relationships are often lost once splint use ceases, suggesting that ARPS may serve primarily as a diagnostic and short-term therapeutic tool.24,25
Recent evidence underscores the efficacy of ARPS in managing TMJ DDwR.
An RCT by Pihut et al. demonstrated that patients using ARPS for approximately 20 hours daily over four months experienced significant reductions in TMJ pain compared to those receiving laser therapy and self-exercises, as measured by the verbal numerical rating scale (VNRS). 26
Further supporting these findings, a systematic review by Maheshwari et al. compared ARPS with other occlusal splints, such as SS. 27 The review found no significant differences in short-term outcomes for TMJ clicking and pain. However, a slight advantage was observed for other splints in reducing TMJ clicking over the long term. The authors noted that the overall certainty of evidence was low to very low, highlighting the need for more rigorous studies.
Additionally, a retrospective study by Jin and Chi 28 evaluated the effectiveness of digitally designed and 3D-printed ARPS compared to traditional splints. Patients using the digital splints reported greater pain reduction and improved mouth opening over a six-month period, suggesting that advancements in splint fabrication may enhance treatment outcomes.
In summary, current research supports the short-term benefits of ARPS in managing DDwR, particularly in pain reduction and functional improvement. However, considerations regarding long-term stability and the quality of evidence necessitate further investigation to optimise treatment protocols.
Do occlusal contacts change after splint therapy?
A study by Al-Ani et al. explored occlusal contact patterns pre- and post-splint therapy in TMD patients. 29 Results indicated no significant change in contact number in myofascial pain and bruxism groups. However, in patients with DDwR treated with ARPS, a significant increase in occlusal contacts was observed after disc recapture, underscoring the need for caution before initiating irreversible occlusal adjustments during acute disc displacement.
Bruxism and splint therapy
The use of occlusal splints in managing sleep bruxism is contentious. Macedo et al. found that there is insufficient evidence to support their effectiveness for improving sleep outcomes, although protection against tooth wear remains a plausible benefit. 13 Further high-quality RCTs are needed with standardised diagnostic criteria and outcome measures.
Notably, Bertram et al. demonstrated that SS reduce muscle asymmetry during clenching, supporting the notion that biomechanical effects play a role in symptom relief. 30
A recent systematic review provided an in-depth evaluation of the clinical effectiveness of oral splints in the management of both TMD and bruxism. 31 The review found moderate evidence supporting the short-term efficacy of SS in reducing pain and improving function in patients with myogenous TMD. However, it emphasised that the long-term benefits remain inconclusive due to variability in study design, small sample sizes, and inconsistent outcome measures across trials. For bruxism, the evidence was even less robust; while splints may help prevent tooth wear and reduce muscle activity during sleep, there was insufficient data to support their effectiveness in improving sleep quality or reducing the frequency of bruxism episodes. The review concluded that while splints may offer symptomatic relief in some patients, they should be used as part of a broader, individualised treatment plan rather than as a standalone intervention. Further high-quality, long-term RCTs are needed to clarify the role of oral splints in both conditions.
Laser and combined therapies
A clinical trial by Molina-Torres et al. evaluated the effects of SS and low-level laser therapy in patients with TMD and fibromyalgia. 32 Both therapies were effective in reducing pain and joint sounds. This highlights the potential benefit of multimodal approaches, though cost-effectiveness and long-term outcomes require further exploration.
Counselling and cost-effectiveness
A network meta-analysis by Al-Moraissi et al. concluded that while SS can be beneficial, its added value over low-cost interventions such as counselling may be limited. 16 The authors recommend beginning treatment with conservative behavioural strategies before progressing to appliance therapy, a stance that aligns with broader evidence-based frameworks.
Role of calcitonin gene-related peptide (CGRP) in splint therapy
Emerging evidence suggests that neuropeptides may mediate the effects of splint therapy. A clinical trial by Nitecka-Buchta et al. revealed that calcitonin gene-related peptide (CGRP) levels declined significantly in patients treated with SS, indicating a potential biochemical pathway for symptom relief. 33 This finding complements earlier pharmacological studies on CGRP receptor antagonists. 34
Efficacy of Nociceptive Trigeminal Inhibition Tension Suppression System (NTI-tss) and Sleep Clench Inhibitor (SCI) devices in the management of TMD and bruxism
In recent years, alternative occlusal devices such as the NTI-tss and SCI have been introduced with the aim of managing parafunctional habits and related orofacial pain.
These devices are typically smaller than traditional full-coverage splints and are designed to cover only the anterior teeth, thereby inhibiting posterior occlusal contact and reducing elevator muscle activity.
Several studies have investigated the effects of NTI-tss and similar anterior bite appliances on bruxism and TMDs.35 -39 Despite their growing popularity, there is currently insufficient high-quality evidence to support the routine use of NTI-tss or SCI appliances over conventional full-arch splints for the long-term management of TMDs or bruxism. Most available studies are limited by small sample sizes, short durations, and methodological variability. Further well-designed RCTs are needed to establish their comparative efficacy, optimal indications, and long-term safety profile.
An RCT conducted by Baad-Hansen et al. found that the NTI-tss significantly reduced EMG activity in the masseter muscle during sleep compared to SS. 35 This suggests a potential short-term benefit in reducing nocturnal muscle hyperactivity. Similarly, Hasanoglu Erbasar et al. reported that NTI-tss therapy led to a significant reduction in TMD-related symptoms, including pain and joint clicking, over a three-month period. 36
However, the long-term safety and effectiveness of NTI-tss remain subjects of debate.
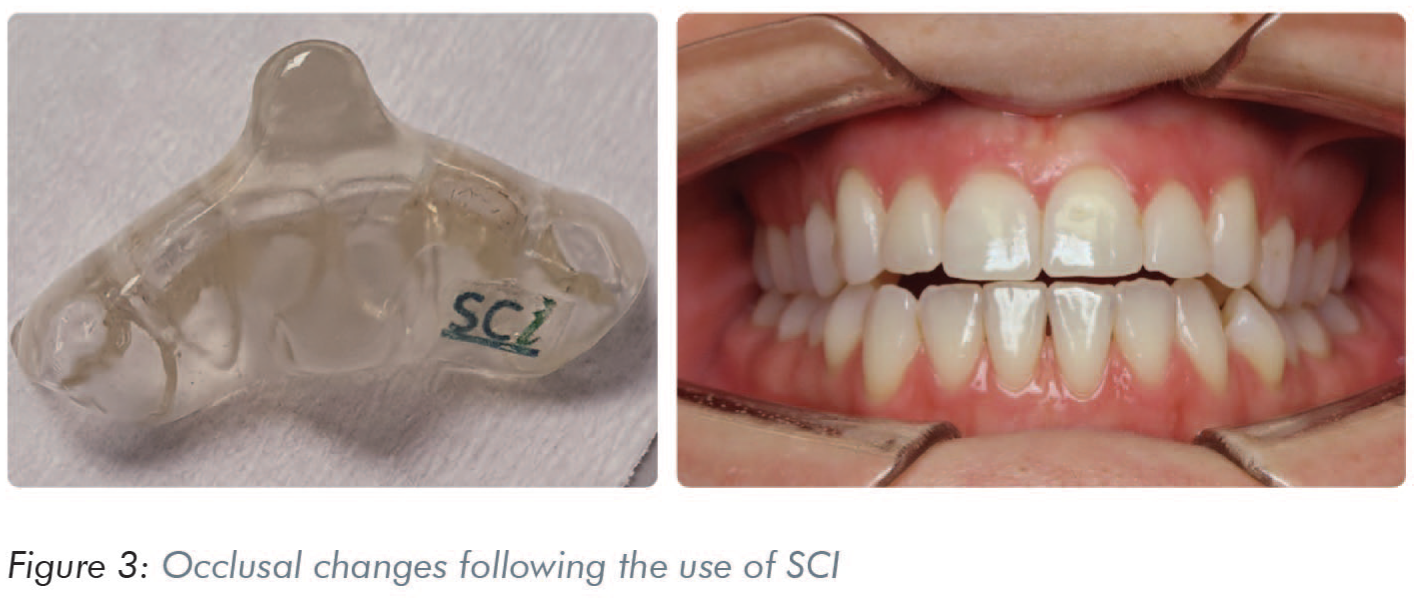
Lukic et al. warned of potential adverse effects, including the risk of irreversible occlusal changes such as the development of an anterior open bite (Figure 3). 37 Furthermore, a systematic review by Stapelmann and Türp concluded that evidence from RCTs suggest that the NTI-tss device can be effective for managing bruxism and TMDs, but it should only be used when patient compliance with follow-up is assured. 38 It is particularly indicated for reducing jaw muscle activity or as a short-term option in acute temporomandibular pain.
Additionally, the American Academy of Orofacial Pain (AAOP) has advised that anterior bite appliances should be used only under close professional supervision and typically for limited durations ranging from a few days up to approximately 2–6 weeks, depending on the clinical indication due to the risk of unwanted occlusal changes. 39
According to the AAOP guidelines, patients wearing occlusal appliances, particularly partial-coverage appliances such as anterior bite appliances, should be closely monitored for changes in occlusion. An initial review should occur within 1–2 weeks after insertion to evaluate occlusion when the appliance is removed and to check for early signs of occlusal alteration. A second follow-up at 2–4 weeks should specifically assess the stability of intercuspation, posterior tooth contacts, and any changes in overbite or overjet, as well as the development of posterior open bite or premature contacts. If any occlusal alterations or bite changes are detected during these reviews, the appliance should be discontinued promptly to prevent permanent occlusal modifications.
A qualitative systematic review by Stapelmann and Türp evaluated the efficacy and safety of the NTI-tss device in managing bruxism, TMDs, and headaches. 38 The review analysed five RCTs out of 68 relevant publications. Two RCTs focused on EMG activity in patients with TMDs and bruxism, finding that the NTI-tss device significantly reduced EMG activity compared to occlusal SS. However, clinical outcomes varied: one study reported greater improvement with SS, while another found no difference between the NTI-tss and stabilisation splints. An additional RCT indicated that patients with tension-type headaches or migraines responded more favourably to the NTI-tss device than to a bleaching tray. Notably, some complications were associated with the NTI-tss, primarily affecting single teeth or occlusion. The authors concluded that while the NTI-tss device may be effective in reducing jaw muscle activity, its use should be limited to patients who can adhere to regular follow-up appointments to monitor for potential adverse effects.
A controlled clinical study by Conti et al. investigated the effectiveness of different intraoral devices combined with counselling in managing painful TMJ clicking. 40 The study compared three groups of patients: those treated with NTI-tss, those with an ARPS, and those receiving counselling alone. All groups showed a significant reduction in pain intensity and frequency of joint clicking over the course of treatment. Notably, the ARPS group exhibited the most substantial improvement in reducing joint sounds.
A study by Hasanoglu Erbasar et al. investigated whether the NTI device could serve as an effective first-line therapy for patients with TMD myofascial pain. 36 In this RCT, patients using the NTI-tss device were compared to those using conventional SS over an eight-week period. Both groups demonstrated significant reductions in pain intensity and muscle tenderness, with no statistically significant difference between the two treatment modalities. The results indicated that the NTI-tss device was as effective as SS in managing myofascial pain symptoms in the short term. The authors suggested that, with appropriate case selection and clinical monitoring, the NTI-tss could be considered a viable first-line treatment option for myofascial TMD. However, they also emphasised the importance of further long-term studies to evaluate potential occlusal changes and sustained therapeutic outcomes.
An RCT by Bruno and Krymchantowski evaluated the effectiveness of the NTI-tss device in the preventive treatment of migraine. 41 The study compared three groups: patients receiving 25 mg/day of amitriptyline, those using the NTI-tss device, and those using a non-occlusal (sham) intraoral splint. Results indicated that the amitriptyline group experienced a significant reduction in migraine attack frequency (60% at six weeks and 64% at 12 weeks). In contrast, the NTI-tss and sham splint groups showed reductions of 39% and 30% at six weeks, respectively, and both groups exhibited a 48% reduction at 12 weeks.
The study concluded that while the NTI-tss device did provide some benefit in reducing migraine frequency, it was not superior to the sham device and was less effective than amitriptyline. These findings suggest that the NTI-tss may not be more effective than placebo in the prophylactic treatment of migraine.
A comprehensive network meta-analysis conducted by Al-Moraissi et al. evaluated the effectiveness of various occlusal splint therapies, including the NTI-tss device, in managing TMDs. 16 The study analysed 48 RCTs encompassing different splint types and treatment modalities. Findings indicated that while the NTI-tss device showed some efficacy in reducing pain intensity for myogenous TMDs, its effectiveness was comparatively lower than that of hard SS and ARPS. Specifically, the NTI-tss ranked below SS and ARPS in terms of post-treatment pain reduction and improvement in mouth opening. The evidence supporting NTI-tss was categorised as very low to low quality, suggesting limited confidence in its clinical benefits. Consequently, the authors recommended prioritising SS and ARPS over NTI-tss for TMD management, emphasising the need for further high-quality research to substantiate the efficacy of NTI-tss devices.
Conclusion
Occlusal splint therapy remains a cornerstone in the conservative management of temporomandibular disorders. Both SS and ARPS have demonstrated clinical utility, particularly for myofascial pain and DDwR. However, the evidence underscores the need for personalised, evidence-based treatment planning and cautious interpretation of outcomes. High-quality RCTs with standardised criteria, rigorous methodology, and long-term follow-up are essential to better define splint therapy’s role within a broader therapeutic framework. In the meantime, clinicians must maintain transparency with patients regarding treatment goals, expected outcomes, and alternative modalities.