
Abstract
Background:
Temporomandibular disorders (TMDs) affect up to 1 in 15 people, significantly impairing daily function and quality of life. Despite clinical guidance recommending a biopsychosocial approach, treatment remains largely biomedical, often relying on occlusal splints or invasive procedures with limited evidence. This study describes a patient-centred, supported, self-management intervention for TMDs co-developed with patients, and its implementation into clinical practice.
Methods:
The intervention was co-developed with patients through syntheses of systematic reviews, qualitative research, and adaptation from a chronic widespread pain intervention. It incorporates a biopsychosocial framework including pain science education, jaw posture control, behavioural activation, cognitive restructuring, and habit reversal. The intervention guide is designed for remote delivery by a trained facilitator. It was evaluated in a proof-of-concept trial and service evaluation.
Results:
The evaluation study (N=104) demonstrates the intervention’s feasibility and efficacy for TMD, reducing pain, interference, and healthcare use. Patients favoured the personalised, remote, guided delivery. Key mechanisms included breaking physical/psychosocial vicious cycles using goal-setting, thus enabling patients to regain control and reverse unhelpful patterns.
Conclusion:
The intervention aligns with biopsychosocial models of care, empowering patients with self-management skills to manage their TMDs. Its flexible, remote format enhances accessibility and environmental sustainability. By addressing key gaps in current pathways, this work also underscores the importance of patient co-design in producing acceptable, scalable, and effective health interventions.
Learning Objectives
To understand the impact of TMD from a patient perspective
To understand the need for a biopsychosocial approach in diagnosis and management of TMD
To demonstrate a supported self-management intervention and its implementation for the management of TMDs
Introduction
Temporomandibular disorders (TMDs) are common painful musculoskeletal conditions affecting up to one in 15 people. 1 Their symptoms are related to the temporomandibular joints (TMJs) and/or the muscles of mastication that move the mandible. Because jaw movements are essential for everyday function, such as talking and eating, TMDs can substantially disrupt daily life, including participation at work and at home. 2 Throughout our translational research work packages on chronic orofacial pain, including TMDs, we have sought to understand the problem from patients’ perspectives and have co-produced an intervention through patient and public involvement and engagement (PPIE).2,3
Our PPIE work underscores both the impact of the condition and the poor quality of current management strategies. 4 Participants described decades of chronic pain and severe functional impairment, often resulting in significant dietary restrictions:
“I have been grinding and clenching my teeth both during the day and night since I was 15 years of age (over 30 years ago). I have suffered from quite intense pain and at times have been left unable to eat solid foods at all. Hard or crunchy foods have been a challenge for many years as the repetitive chewing can be extremely painful in the jaw, so we have tended to avoid these.” (Member of PPIE group)
Furthermore, TMDs are frequently associated with psychological co-morbidities and aspects of illness behaviour that predict onset and persistence and have significant emotional impact on patients.5,6 The emotional burden is compounded by the “invisible” nature of the condition and associated sleep disturbances:
“I have had quite severe sleeping difficulties, waking up multiple times throughout the night and feeling fatigued most days, even after an apparent 8–10 hours’ sleep. No one can ‘see’ my pain so no one understands it, and I have to put up with it.” (Member of PPIE group)
In keeping with these patient experiences and contemporary research, both national and international guidelines recommend a biopsychosocial approach to diagnosis and non-invasive supported self-management as a first line of management for TMD.7,8
That said, in primary dental care treatment usually focuses on biomedical approaches to the exclusion of biopsychosocial factors, with dentists preferring the use of “mouthguards” to cover the teeth (occlusal splints of differing styles) rather than self-management despite equivocal evidence of the former’s efficacy.9,10 The pattern persists into secondary care, where management often escalates to invasive, irreversible treatments such as tooth extraction or surgery. Such interventions are not only poorly supported by evidence but are potentially harmful, frequently exacerbating the patient’s condition and entrenching the chronic pain cycle. 11
The current management landscape for TMD is characterised by clinical fragmentation and a high volume of unproductive referrals.2,4,11 This systemic failure is substantiated by both our PPIE work and health economic data. 12 Patients frequently report being “passed from pillar to post” between primary and secondary care providers, enduring significant delays in receiving personalised, appropriate care. 4 Research demonstrates that consultation costs in primary and secondary care are likely to be between £237–£333 per patient per annum accounting for 76–81% of the total cumulative cost per care per annum. 12 These direct costs are further compounded by broader societal economic impacts, including significant productivity losses – estimated between £1,698 and £2,574 per annum – and substantial out-of-pocket costs for private treatment and related healthcare charges (£578–£754 per annum).12,13 Patients with TMDs frequently consult their general (medical) practitioner (GP) in preference to dentists and a recent study has shown an increase in consultation rates to GPs. 14 However, GPs often lack the specialised training required to manage TMDs and do not understand the nuances of managing the dental aspects of this condition. Furthermore, there is lack of communication between GPs and dentists with patients passed between them without improved clinical outcomes. 2
Therefore, a critical requirement exists for a non-invasive, evidence-based intervention that is effective and scalable across diverse healthcare settings, including both dental and non-dental primary care. This article describes a biopsychosocial intervention, co-developed with patients and grounded in the contemporary TMD evidence base designed to address the existing care gap and the high economic burden of fragmented management. 15
Specific objectives include:
Description of intervention development including links to an online guide.
Demonstration of clinical application utilising illustrative case studies to show how the intervention can be integrated into routine clinical practice across multidisciplinary settings.
Intervention development
The development of the intervention was underpinned by a systematic review conducted by our group, which evaluated self-management interventions for adults with TMD. 15 The analysis of nine high-quality studies confirmed that self-management is effective in achieving long-term improvements in both pain intensity and depressive symptoms.
Building on this evidence, we utilised a co-production model with a PPIE group to design the pain intervention guide. 3 A central feature of this guide is the integration of patient ‘stories’ within relevant sections. These stories illustrate lived experiences of the “vicious cycles of pain”, provide peer-led examples of technique application (e.g. posture control, behavioural activation, cognitive restructuring), and offer strategies for relapse prevention. We adapted the psychosocial elements, specifically behavioural activation and cognitive restructuring, from a telephone-delivered intervention for chronic widespread pain which showed long-term clinical and cost-effectiveness (24-month follow-up period). 16 The adaptation process involved a synthesis of our systematic review, 15 qualitative findings, 2 and PPIE feedback. To ensure the intervention met the unique clinical needs of TMD patients, we integrated specific jaw posture control and habit reversal techniques, which are necessary for management of TMDs and which differentiate our intervention from other living well with pain self-management programmes, such as Ten Footsteps. 17 The resulting intervention guide is structured into four steps. 3 It is easy to read, achieving a Flesch-Kincaid Grade Level of 6.4 (equivalent to a reading age of 12–13 years). This design allows for a highly personalised approach, enabling patients to tailor the self-management tools to their specific needs.
The four-step self-management framework
The intervention is structured into four progressive steps, designed to transition the patient from a passive recipient of care to an active manager of their condition.
Step 1: Understanding chronic orofacial pain
This foundational stage explains the pathophysiology of TMDs and psychological processes involved in pain pathways, specifically utilising the gate control theory of pain to illustrate how psychological and physical factors influence pain perception. It introduces self-management, emphasising the role of the patient as the primary “agent of change”, fostering self-efficacy and the motivation to take control of their recovery.
Step 2: Impact assessment and goal setting
Patients conduct a holistic evaluation of how TMD affects their daily function, emotional well-being, and social interactions. This impact assessment facilitates personalised goal setting, ensuring the subsequent techniques are tailored to the patient’s specific needs.
Step 3: The biopsychosocial programme
The core of the intervention implements a biopsychosocial triad consisting of three evidence-based strategies:
Step 4: Sustaining progress and recovery
The final stage provides patients with tools for continued symptom management and “recovery techniques” to handle their pain and potential flare-ups. This ensures that patients have a relapse prevention plan, maintaining the gains achieved during the active phase of the intervention.
Evaluation, feasibility and refinement
This supported self-management guide 3 based on a biopsychosocial approach to manage TMDs and chronic orofacial pain was evaluated in a proof-of-concept study 18 where it was delivered by two trained facilitators by telephone or face-to-face. The guide was further developed and refined during our evaluation in the proof-of-concept trial which showed high levels of patient acceptability and established the feasibility of remote delivery via telephone.18,19 The intervention was successfully delivered by facilitators from both dental and psychological backgrounds by telephone.18,19
Identifying and reversing unhelpful patterns specific to TMDs (e.g. bruxism, clenching, and nail biting) are critical drivers of clinical improvement as identified in our process evaluation. 19 Posture control and habit reversal were therefore incorporated into the intervention guide to target these along with the psychosocial approaches of behavioural activation and cognitive restructuring which targeted underlying stressors that led to these unhelpful habits. Subsequent evaluation of the refined intervention in a case-series of 66 patients presenting to a secondary care NHS clinic demonstrated reduction in pain intensity and functional interference with daily life, suggesting that the transition to a biopsychosocial, self-management model directly addresses the debilitating nature of chronic TMD. 4 In addition, this resulted in cost savings owing to reduced consultation for TMDs. The intervention achieved strong clinical and patient “buy-in”, which facilitated a secondary phase of co-production. During this stage, the guide was further enriched with additional patient narratives to enhance peer-led validation. Critically, a member of our PPIE group reformatted the guide to optimise readability, ensuring the content remained accessible and patient-centred.
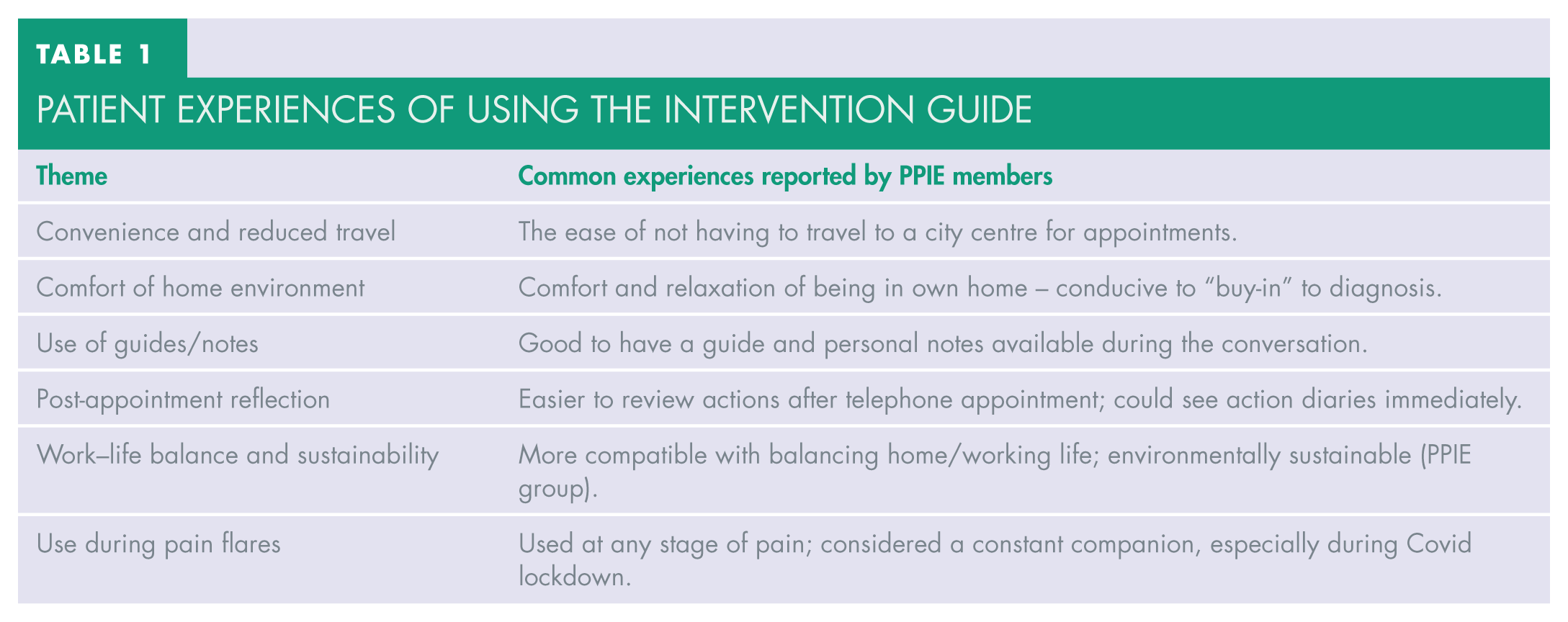
Patient “buy-in” indicated a preference for remote service delivery which was used during the Covid lockdown and now continues to be sustained post-lockdown due to its significant logistical and therapeutic advantages. Furthermore, the remote model aligns with emerging priorities in environmental sustainability. Patient and clinician travel are recognised as the greatest contributors to the carbon footprint of dental services. 20 The burden of TMD is historically exacerbated by high-frequency travel across primary and secondary care dental services;2,4,11 therefore, a remote-first pathway offers a measurable reduction in the service’s environmental impact while simultaneously improving the patient experience (see Table 1).
Patient experiences of using the intervention guide
Case study
The following case study shows how the intervention can be used to manage patients with TMD using a biopsychosocial approach.
Diagnosis
While the purpose of this paper is focused on biopsychosocial management, it is first necessary to understand and have a systematic approach to diagnosis without which management cannot be appropriate at the outset. In approaching the diagnosis of this case study patient, it is important to consider a biopsychosocial approach as outlined by the International Diagnostic Criteria for TMD (DC/TMD) which consider both physical symptoms (Axis 1) and psychosocial factors (Axis 2). 21 We have developed a structured clinical examination which can be accessed via a YouTube video. 22 This includes a one-minute examination using a checklist which maps onto DC/TMD diagnoses and incorporates a red flag checklist adapted from the Manchester 3-minute examination. 23 It includes a nine-item patient health questionnaire (PHQ-9) used for depression screening to assess psychosocial factors and, therefore, as a package provides a biopsychosocial approach to diagnosis of TMD. 24
According to the video and checklist, the Axis 1 symptoms relate to both the joint (internal derangement) and muscles of mastication. 22 Radiation is also beyond the muscles of mastication. Specific diagnoses are therefore disc displacement with reduction and myofascial pain. 22 Axis 2 factors include anxiety and OCD which may be manifesting as bruxism/occlusal parafunction.
Biopsychosocial supported self-management
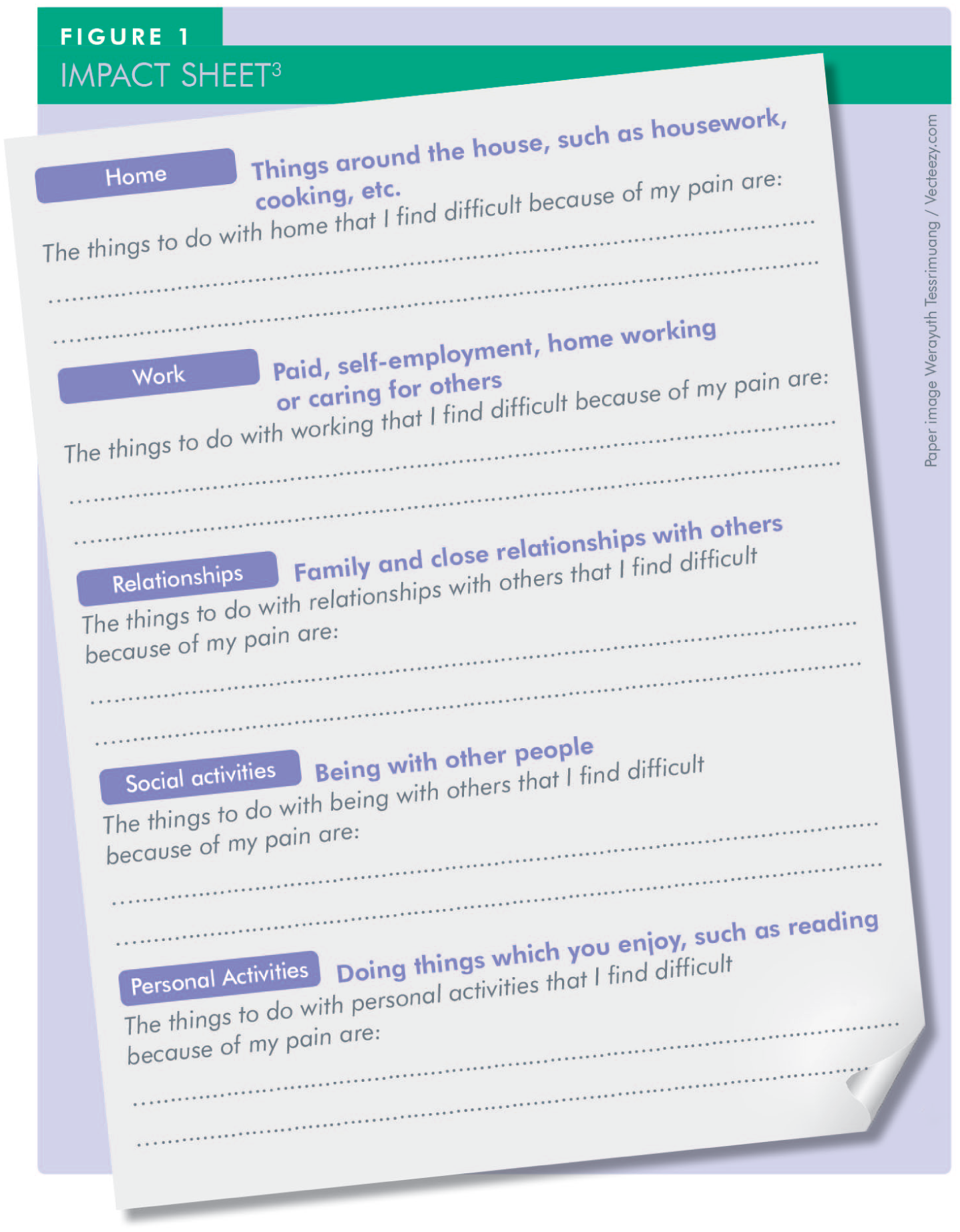
The key to successfully managing this case study patient is to develop a shared understanding of the problem from the patient’s perspective. To aid this process our intervention guide includes an impact sheet on page 8 of the pain guide which can be completed with the patient (Figure 1). 3 The impact sheet allows a clinician to assess what it means for the patient to be in pain, which is often a better indicator of pain severity than a visual analogue scale (VAS) that gives a 0–10 pain intensity but does not establish what that means to the patient. Moreover, every individual experiences pain differently based on their previous pain experiences and learned environment (i.e. psychosocial factors). 25 Therefore, a 7/10 report on a VAS can have very different meanings from one individual to the next, for example a stoical person might report the same pain as 2/10. As per the patient video, which can be viewed online (see reference 26, “TC Project Agata edit 15 05”), the impact of the pain on this patient was on all areas of her quality of life including sleep, eating hard foods, walking her dog, and leisure activities such as attending the gym. 26
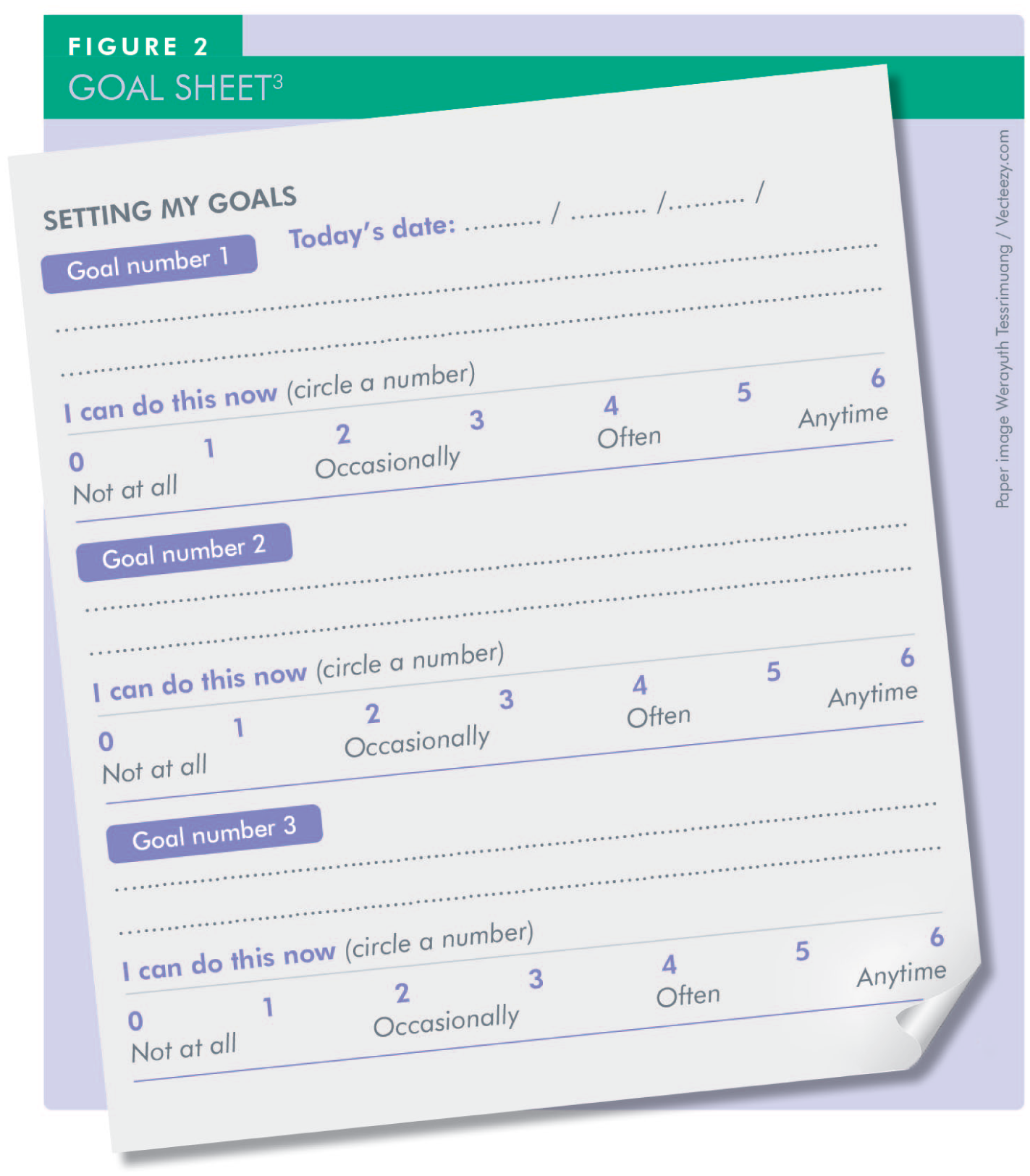
Having understood the impact, it is then easy to work with the patient to set goals for her pain management which can be targeted by the intervention. An example of a goal sheet (page 14 of pain guide 3 ) is illustrated in Figure 2. For this patient, her goals were to improve her sleep and stop the pain from impacting on her daily functional activities, such as walking her dog and going to the gym.
The key areas for intervention were to break vicious cycles both from the physical aspects (i.e. “clenching – muscle tension – pain” cycle) and psychosocial aspects related to negative thoughts about the pain and fear avoidance of activities. An example of a vicious cycle related to this patient is shown in Figure 3.
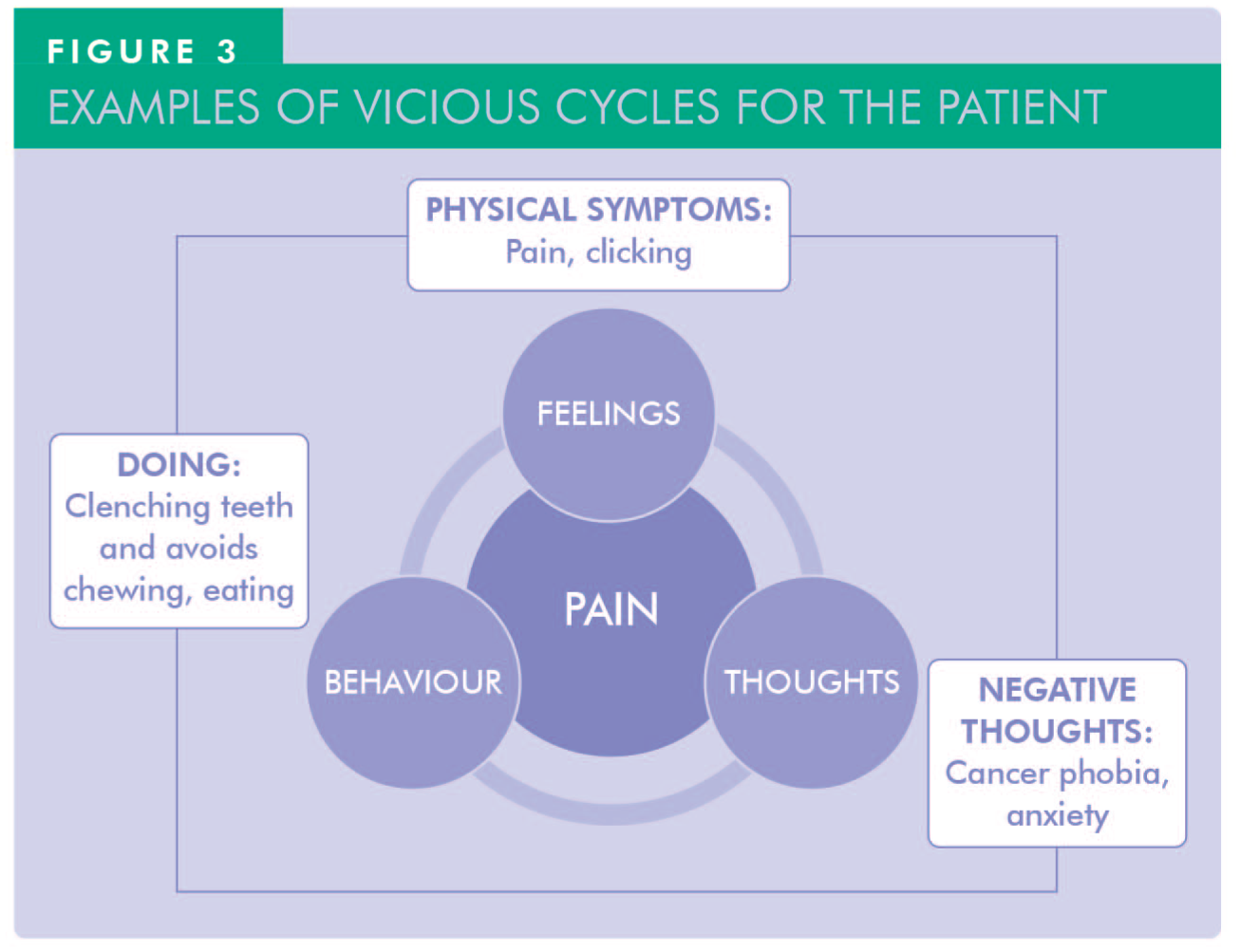
Having identified vicious cycles associated with her symptoms, both physical and psychological techniques were applied to break those cycles to improve her symptoms. Using this biopsychosocial approach, the management plan was as follows:
Factual reassurance
This involved providing explanations about the muscular origin of the symptoms and the reason for the clicking sounds. The illustration on page 19 of the guide is helpful to talk patients through palpating and feeling the tension in the masseter and temporalis as they clench their teeth. 3 We then use pain science education which includes the gate control theory and how to interrupt pain pathways by stimulating mechanoreceptors through massage and heat application. 27 It also includes explanation on how the limbic system via descending pathways also modulates the pain response. 27 The patient then understands how stress can lower pain thresholds and results in a vicious cycle that propagates pain symptoms.
Massage
Massage of masseter muscle from its origin to insertion. The patient is instructed to slide four fingers from the origin of masseter to its insertion into the mandible using the illustration on page 19 of the pain guide. 3 The patient then notices how this leads to the lower jaw dropping which causes separation of the teeth and prevents daytime clenching and at the same time eases tension in the muscle and controls pain by stimulating mechanoreceptors. This technique was tried and tested by a patient within our PPIE group and adopted into our intervention as a result. 3
The temporalis muscle is also massaged similarly by sliding fingers from the ear to the middle of the scalp. The patient in this case then became aware of why she was experiencing headaches due to tension in the temporalis because of teeth clenching. The patient was instructed to undertake this massaging on a regular basis and not when the pain was at its worst, thus starting to prevent the onset of pain. In this case study the patient used a roller to massage, as depicted in her online video. 26
Heat/cold therapy
Application of heat/cold to masseter and temporalis muscles on a regular basis and not when the pain is at its worst. This stimulates mechanoreceptors and eases tension in the muscles. Often patients prefer heat application using a wheat bag which they warm in the microwave. Again, regular application works towards preventing flare-ups.
Posture control
Sleeping on the back at night helped alleviate this patient’s night-time clenching and grinding. This technique is described on page 17 of the pain guide 3 and was developed by the patient who adjusted her pillow position to maintain her back-sleeping position throughout the night. This relieved her morning symptoms. This is not suitable for all patients (e.g. those with obstructive sleep apnoea and some who cannot adopt the position) as it can worsen their sleep.
Cognitive restructuring
Cognitive restructuring challenges negative thoughts using evidence tables and thought diaries; it is detailed on pages 31–34 of the pain guide. 3 In this case, the patient reports how her negative thoughts around her TMD symptoms were challenged by developing an understanding of the pain and the muscles involved. 26 She felt reassured that there was no serious underlying cause for her symptoms and that she was able to live well with them by stopping them interfering with her daily activities.
Behavioural activation
This involves balancing routine, necessary and pleasurable activities within a weekly activity diary (described on pages 23–30 of the pain guide 3 ), and helps to break the vicious cycle of avoiding activities of daily living. In her online video, the patient clearly describes how she used this to good effect to gain control over the pain. 26 The impact was immense for her as she was able to go back to the gym and walk her dog – activities she enjoyed that had been adversely impacted by the pain.
Relapse prevention and discharge
Once the patient had the necessary tools to continue to self-manage, the final session was focused on the discussion of how future flare-ups can be managed as her condition is chronic and episodic; the goal is to live well with the pain as it may not be completely cured. All sessions for this patient were delivered over the telephone, which were not only environmentally sustainable but also very convenient for the patient.
Discussion
TMDs present a significant clinical and public health challenge due to their high prevalence, complex aetiology, and frequent underdiagnosis or mismanagement in primary and secondary care.1,2,4,11 -14 This paper described the development and implementation of a biopsychosocial supported self-management intervention for chronic orofacial pain, particularly TMDs, co-produced with patients through extensive PPIE. 3 The findings underscore the value of co-production in creating a clinically relevant, patient-centred tool that not only addresses the biological aspects of TMD but also effectively integrates the psychosocial dimensions that are often overlooked.2,4,6,7
Patient narratives from the PPIE group illuminated a pervasive dissatisfaction with current care pathways, often characterised by repeated referrals, lack of coordinated care, and over-reliance on biomedical interventions with limited efficacy. These experiences reflect previous findings in the literature that highlight the gap between recommended biopsychosocial guidelines and the predominantly biomedical focus in both dental and general medical practice.2,4,6,7 Our intervention directly addresses this gap by providing a structured, accessible, and evidence-based tool designed to empower patients and facilitate more holistic management.
The success of our intervention lies in its grounding within the current evidence base. 15 Systematic reviews have confirmed the long-term benefits of self-management for chronic pain, particularly when underpinned by cognitive-behavioural techniques such as behavioural activation and cognitive restructuring.15,28 By integrating these components alongside TMD-specific techniques (e.g. posture control, massage, habit reversal) the guide uniquely tailors established pain management strategies to the specific challenges of TMD management.2,3,7 This approach not only improves pain outcome but also supports patient agency, addressing the emotional toll and psychological co-morbidities such as anxiety and depression that frequently accompany chronic TMDs.4 -6
The case study illustrates how the intervention was adapted to an individual patient’s needs, aligning with a personalised care model. The structured approach based on understanding the pain from the patient’s perspective, using impact sheets and subsequently targeting goals to address the impact, allowed the patient to gain control over her own pain management. 26 This allowed for targeted strategies to be employed, including education on the gate control theory of pain and its relevance to self-regulation of symptoms. 27 Importantly, this patient-centred dialogue fostered reassurance and buy-in, which were crucial in engaging the patient and sustaining long-term behavioural change.4,26
A significant strength of this intervention is its delivery mode. Patient preference for remote consultations, popularised during the Covid-19 pandemic, aligns with trends toward digital and remote healthcare solutions. 29 Beyond convenience and accessibility, remote delivery also contributes to environmental sustainability – an increasingly important consideration in healthcare planning. 20 By reducing travel requirements for both clinicians and patients, the described model offers a more environmentally conscious alternative without compromising care quality or patient satisfaction. 20
Moreover, our proof-of-concept and case-series evaluations4,18,19 demonstrated measurable improvements not only in clinical outcomes (e.g. reduced pain intensity and interference with life), but also in health service utilisation and economic burden. 4 Given that a significant proportion of TMD-related healthcare costs stem from consultations and productivity losses, shifting toward supported self-management could yield substantial cost savings.4,12,13 These findings support the feasibility and scalability of the intervention, particularly in resource-constrained or rural settings where access to specialised care is limited and referral rates are disproportionately high. 29
The described intervention is suitable for delivery in the current shared care dental model focused on skill-mix and prevention which allows ease of access (including self-referrals) and aims to provide the most effective and least intrusive therapies first, in-line with a stepped-care model.30,31 The intervention is currently being considered for adoption in NHS primary dental care through flexible commissioning models where it can be delivered by Oral Health Champions closely supervised by dental practitioners and trained facilitators. This will ensure delivery at the point of diagnosis and may reduce the need for costly, invasive treatment and secondary care referrals. The guide has also been translated into commonly-spoken non-English languages making it usable across diverse populations, including those with lower health literacy or from non-English-speaking backgrounds. Those participating in PPIE recognised the benefits that supported self-management offers, especially as the programme employed has been co-produced with patients. Reported examples of feedback from members of the PPIE group include:
“CF had seen doctors and dentists interchangeably on a regular basis, but found the guide was the most effective information for her condition.”
“BF has distributed it to friends and employers who, having read it, have understood her pain issues and shown empathy.”
“Members of the group, who have used the guide would like to see it available to patients who are in pain now.”
Conclusion
This article presents a novel, co-produced biopsychosocial intervention that offers a patient-centred, evidence-informed response to the longstanding challenges in managing chronic TMD. The integration of clinical guidelines, real patient experiences, and self-management strategies tailored to TMD represents a shift toward more empathetic and effective care. The described guide contributes to the growing body of literature advocating for whole-person approaches in pain management and underscores the power of patient collaboration in healthcare innovation. 32
Footnotes
Acknowledgements
The authors would like to thank members of the PPIE group for their input in co-producing and refining the intervention. We would like to thank several collaborators with whom we developed the intervention including but not limited to the following: Dr Joanna Goldthorpe, Professor Sarah Peters, Professor Linda McGowan, Professor Elspeth Guthrie, Professor Alan Mighell.
Funding
The development of the intervention described in this paper was partly funded by a Clinician Scientist award held by Vishal Aggarwal and issued by the National Institute for Health Research and Care (NIHR) – grant number CS/2008/08/001. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. There are no conflicts of interest to declare.