
Abstract
The primary dental care team commonly encounters patients presenting with trismus as the result of various benign causes. Common among these causes are the range of temporomandibular disorder diagnoses. In a rare but significant number of cases the cause may be an underlying malignancy in which case urgent referral is mandatory. This article describes the implementation of the Trismus Checklist, a nine-item screening tool designed to improve patient safety by structuring the diagnostic process for trismus. Objective measurement techniques, including recording the intra-incisal distance, while emphasising the need to account for a pre-existing overbite or open bite are outlined. A passive stretch test is recommended to differentiate between myogenic limitations and mechanical obstructions. The routine use of the described Trismus Checklist helps safeguard clinicians against missing significant pathology. It is suggested that objective monitoring and follow-up are essential for all patients presenting with trismus, regardless of the initial suspected diagnosis.
Keywords
Learning Objectives
To outline the clinical significance of trismus and its role as a potential red flag for underlying malignancy
To explain how to objectively measure and monitor mouth opening using intra-incisal distance and bite gauges
To highlight the use of the Trismus Checklist to reduce diagnostic bias and guide urgent referral pathways
Introduction
“The most common things happen most commonly” is a useful rule to apply when faced with a patient presenting with a confusing array of signs and symptoms. This is particularly true in pain diagnosis, where the complex reality of nerve innervation and the emotional components inherent to the pain experience often leave clinicians uncertain about the underlying cause and the most appropriate management approach. However, there is a risk inherent in this mental shortcut, and that is that uncommon diagnoses may be missed. This diagnostic bias has the potential for significant consequences when the underlying pathology is malignant. 1
Diagnostic bias is a form of cognitive bias applied to the clinical judgement of healthcare professionals. It is a specific category of confirmation bias or “the seeking or interpreting of evidence in ways that are partial to existing beliefs, expectations, or a hypothesis in hand”. 2 In the healthcare setting it develops from a clinician’s training background, the environment they work in, their professional history and external pressures, such as appointment length and scarcity of resources.
Regarding temporomandibular disorders (TMDs) some of the rare diagnoses that may not readily be considered by clinicians are neoplasms.3,4 Typically, these benign or malignant growths can occur in the temporomandibular joint (TMJ) itself, oral cavity, nasopharynx or salivary glands. Their space-occupying presence can lead to functional problems affecting the mechanics of the articulatory system as well as pain. The exact nature of these depends on the type and site of the neoplasm. The immediate challenge for the clinician is that the symptoms of pain and reduced function can easily be misdiagnosed as being a result of the more common myogenic or articular disc related pathologies. 5
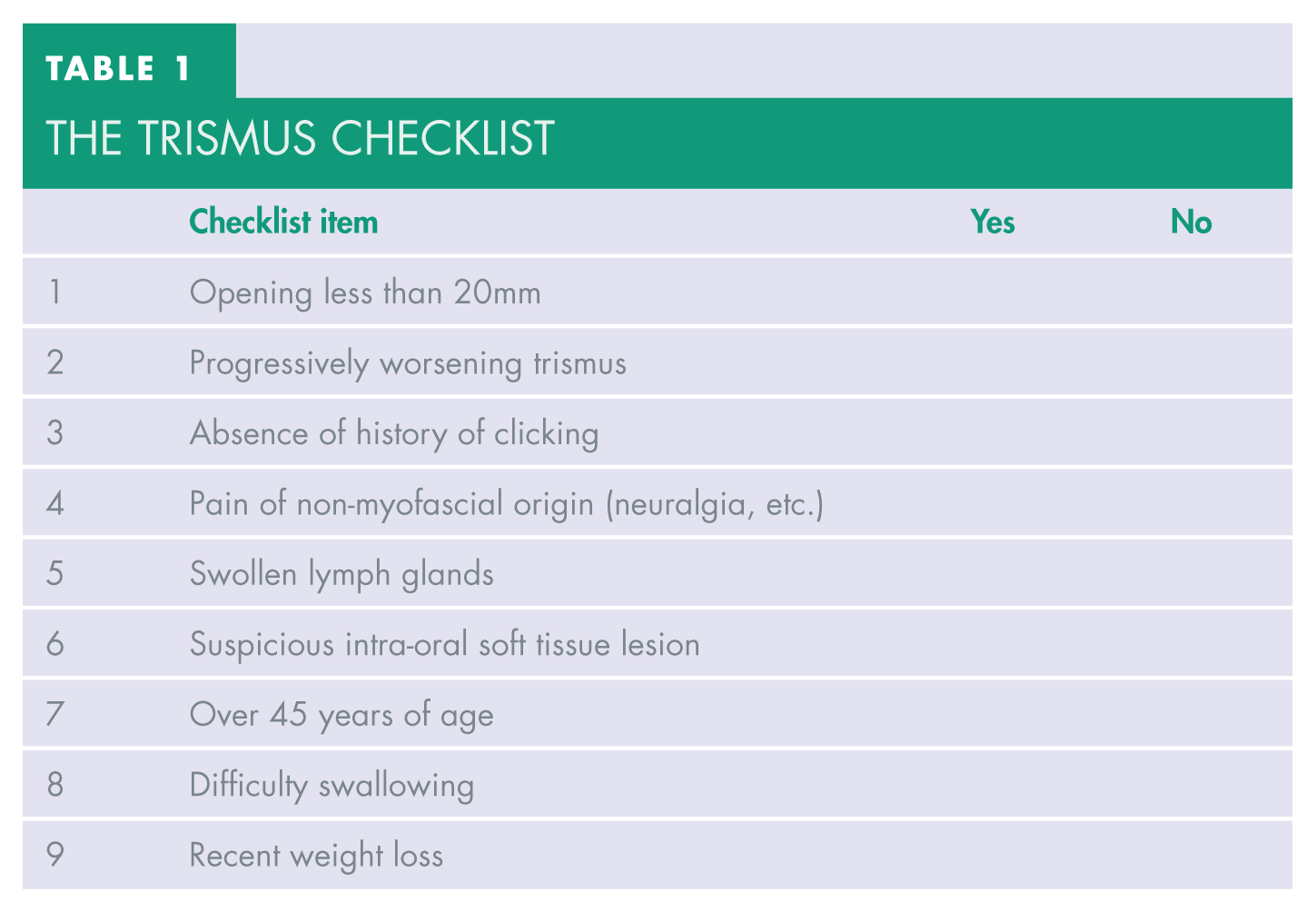
To help prevent misdiagnoses this article encourages greater awareness of the physical sign of trismus. Vigilance around this clinical sign, followed by appropriate investigations, is a helpful addition to any examination protocol. To facilitate this, the Trismus Checklist is a useful tool designed to structure this process. 6 It is a simple nine-item list to work through that can help guide clinical decision making (see Table 1).
The Trismus Checklist
What is trismus?
Most dental professionals will understand that trismus means reduced mouth opening. 7 As the mandible is the moveable bone it is this whose range of motion is for some reason impaired to give the effect of trismus. The question the clinician must then answer is why is this movement impeded? And at what value of mouth opening does trismus begin? The literature describes varying figures for the latter question.5,6
The most recent and extensive diagnostic criteria for TMD states that an inter-incisal distance of below 40mm should be considered to be reduced mouth opening in adult patients. 5 The ‘Brief Diagnostic Criteria’ 8 were developed out of that comprehensive document 5 and include a symptom questionnaire where patients self-report if they consider that their mouth opening is restricted. This has the advantage that the patient will know what their normal mouth opening feels like and will, therefore, be able to say intuitively if this feels restricted. The disadvantage is that it is not an objective measure and it cannot be monitored or compared over time.
For many clinicians the measurement of 40mm is perceived as too high. If trismus is to be used as an early identifier of potentially sinister pathology, then a number that provides sufficient sensitivity is required. For this reason, 25mm to 35mm have been suggested as cut off points that may be of clinical significance.6,9 First described in 2014, the Trismus Checklist has been repeatedly audited, and through that period of development 30mm has been settled on as a clinically robust number. 9
How to measure trismus?
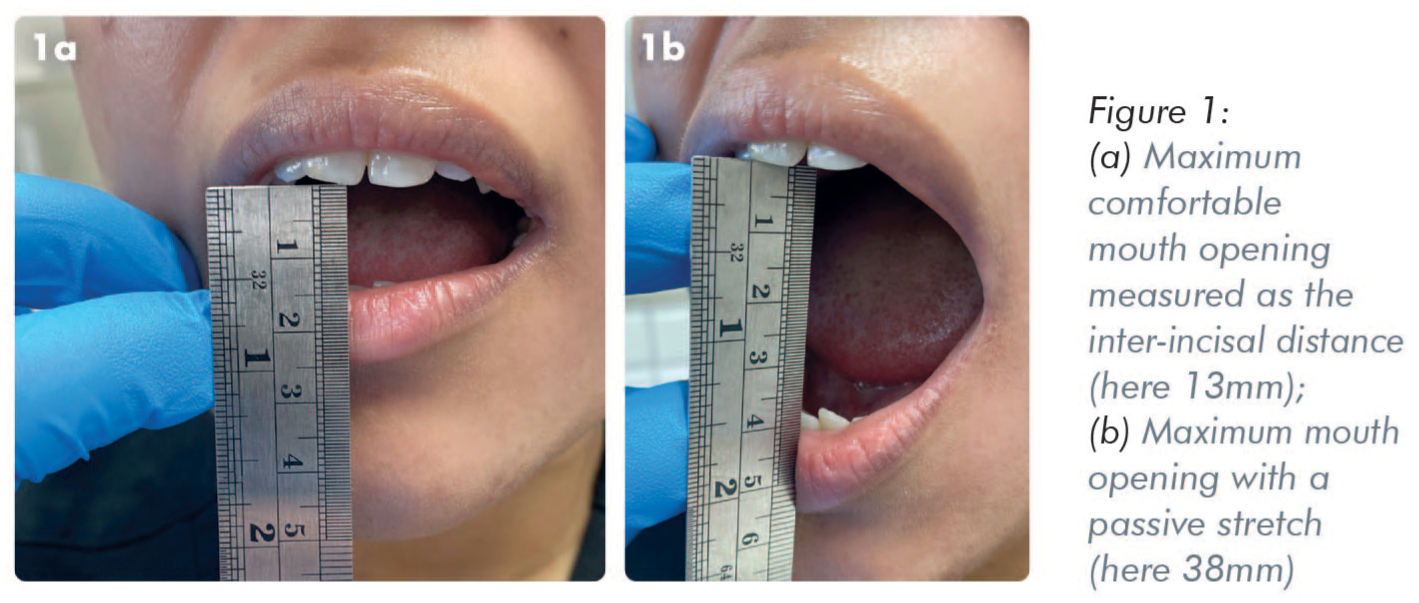
The simplest way of measuring mouth opening is to take the incisal edge of the maxillary incisors and measure the distance to the mandibular incisors using a ruler (see Figure 1a). The patient is asked to open to their maximum comfortable level, and this is recorded. Where this distance falls below a clinically critical value (recommended 30mm), a second reading of the measurement is indicated. Here the clinician places two digits against the upper and lower dentition aiming to gently stretch the mouth opening further, which can be measured with a ruler (see Figure 1b). This process is instructive. If further opening can be gained it indicates that the limitation is likely to be myogenic as it is the muscles of mastication that are no longer required to engage when the clinician takes over. If no further opening can be achieved, this indicates an obstruction that is not of muscular origin.
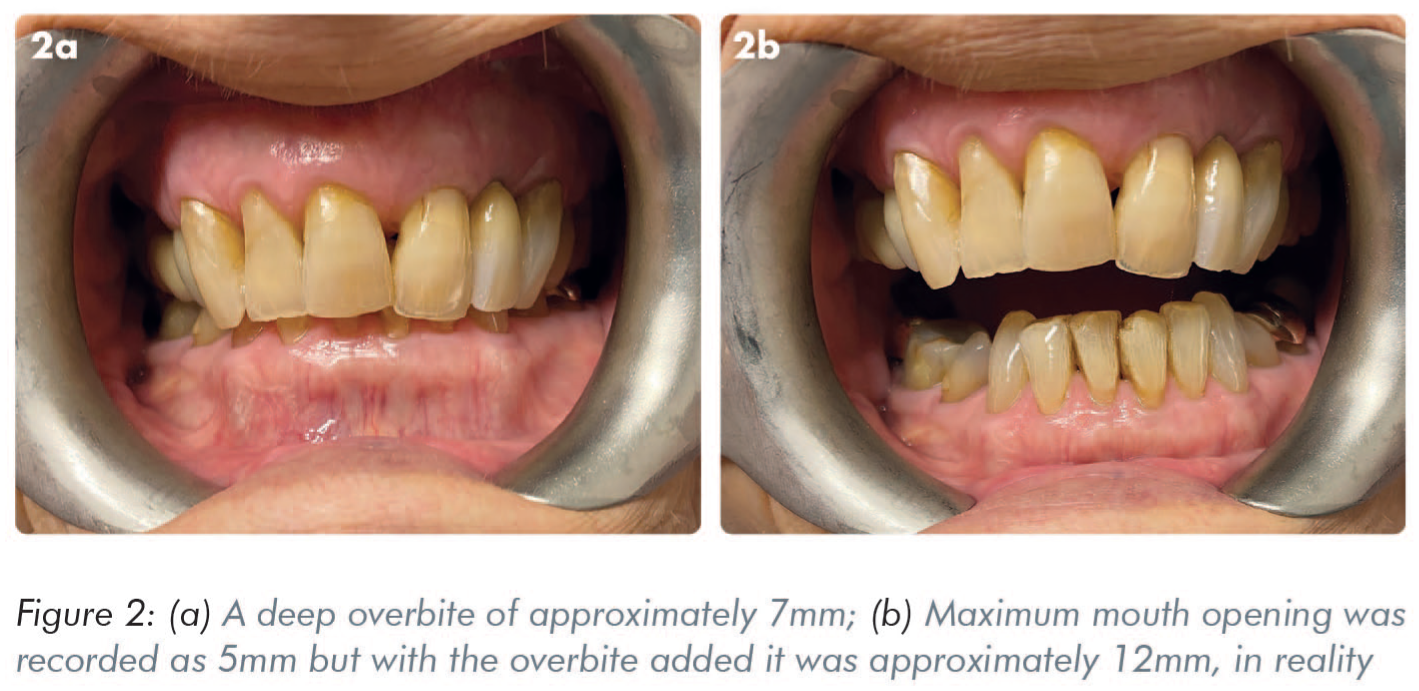
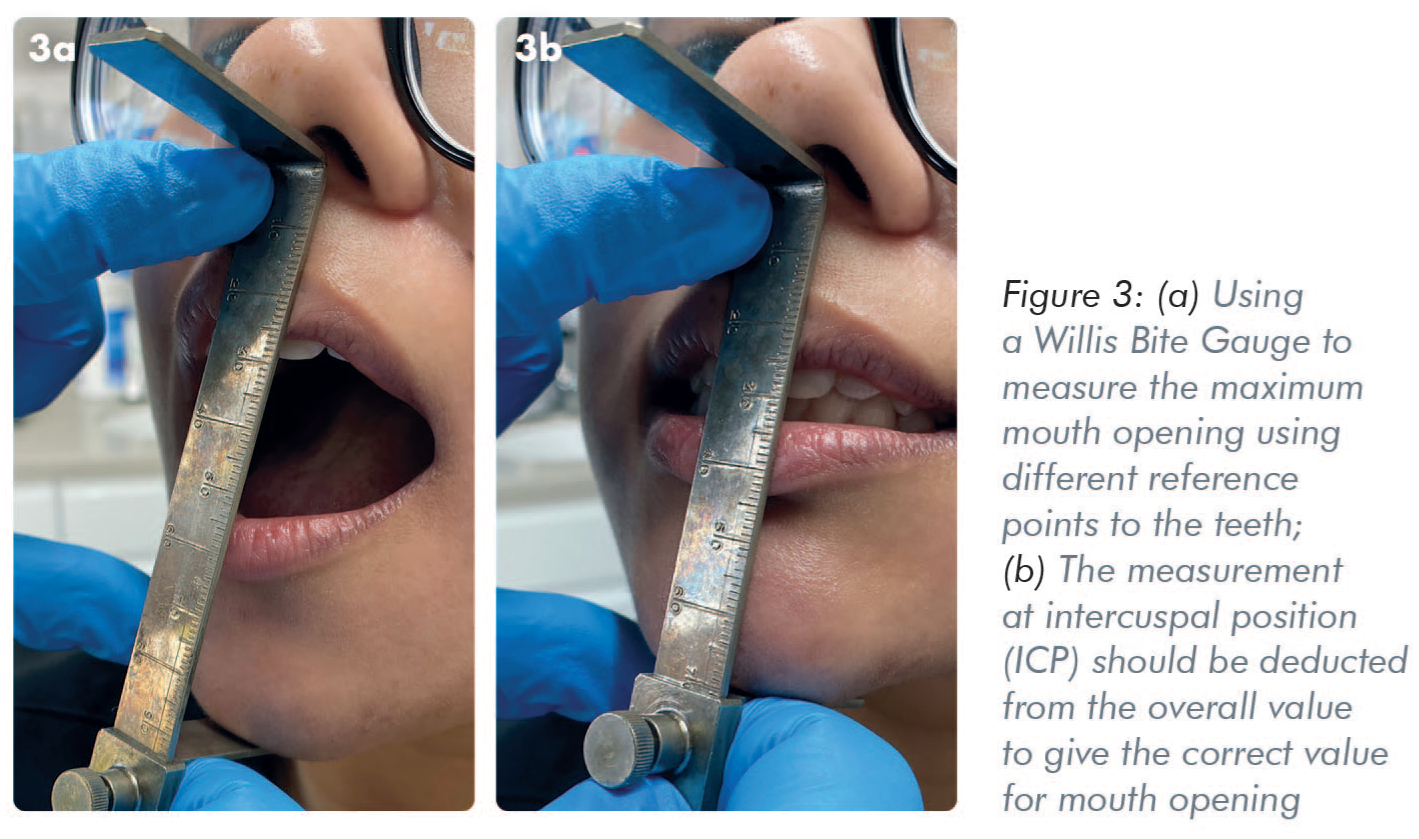
When the incisal distance is measured the clinician needs to be aware of the level of overbite or anterior open bite that pre-exists as these will influence the starting points of measurements between incisal edges (see Figure 2). This is particularly relevant when a case is considered borderline in its clinical significance. Where the clinician is unsure, a measurement of overbite can be added to the inter-incisal opening, or the measurement of open bite deducted from inter-incisal opening, to give a more accurate representation of the true value. Alternative methods, such as a Willis Bite Gauge, can be employed. In this instance the vertical height, either in intercuspal position (ICP) or in centric occlusion, is deducted from the measurement at maximum opening to give the value for mouth opening (see Figure 3).
What to do when trismus is identified?
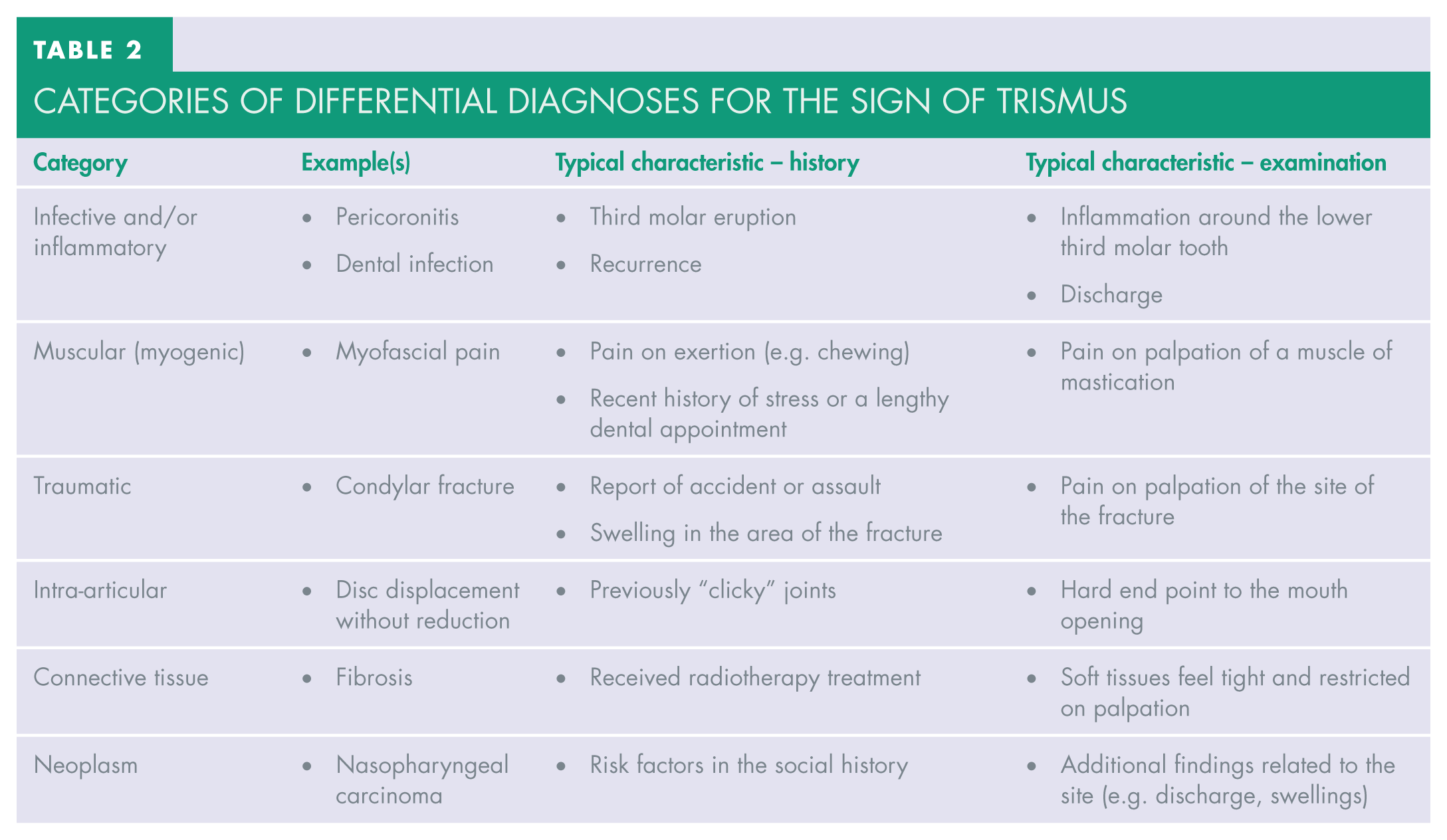
Once it has been established that a patient presents with trismus, the clinician must work through a list of differential diagnoses to determine the underlying cause. In broad terms, these diagnoses may be infective and/or inflammatory, muscular, traumatic, intra-articular (within the TMJ capsule), connective tissue related, or the result of a neoplasm. Examples from each of these categories together with some typical characteristics that may emerge from the history and examination are shown in Table 2.
Categories of differential diagnoses for the sign of trismus
To reduce diagnostic bias, and to discern whether the patient would benefit from further investigations to rule out malignant causes, it is recommended here that the Trismus Checklist (Table 1) be used routinely in every case of limited mouth opening. Following its initial inception the checklist has been developed and modified through a process of regular audit and scrutiny, an evolution that has been recorded and published. 9
The nine items are phrased in such a way that if any of them can be answered affirmatively then further investigation should be initiated either by the clinician themselves or via onward referral. In these circumstances it is reasonable for such a referral to be made, initially under a Faster Diagnosis pathway (formerly known as a Two-Week Wait referral). The checklist is simple to apply and requires no specialist equipment.
Follow up
Local protocols will vary, and in the primary care setting the opportunity for actions may be limited to sending an urgent referral into secondary care once an affirmative response to the Trismus Checklist has been made. Depending on the specific features of the history and examination, follow-up investigations may include one or more of the following imaging techniques:
panoramic radiography to determine any pathology related to bone, teeth or sinuses
where a dental cause is suspected, intra-oral radiography may be preferable, but it is not always physically possible to carry out in cases of severe trismus
a magnetic resonance imaging (MRI) scan to assess for hard and soft tissue pathology of the TMJ, salivary glands and superior aspects of the neck
an ultrasound examination to assess any superficial swellings that are palpable
The latter two imaging techniques require specialist reporting by an appropriately trained radiologist or sonographer.
In the primary care setting it is important to ensure that the patient is not “lost in the system”. Where there is an opportunity to track a referral using existing software this should be done weekly. If not, then it is prudent to book fortnightly reviews with the patient to continue to assess the level of trismus and the progress of their referral.
Even if Trismus Checklist responses are all negative and the decision has been made not to refer the patient initially (e.g. when a diagnosis has been confidently made of a non-suspicious pathology such as pericoronitis), patients should still be followed up to ensure that the mouth opening is improving and the management is proving effective.
Case example
A 40-year-old female presented to her general dental practitioner (GDP) complaining of pain and reduced mouth opening. On examination, her GDP noted that her mouth opening was indeed reduced as the intra-incisal measurement was 24mm with 2mm of overbite.
The GDP also noticed that her mandible had a lasting deviation to the right. On further examination there was tenderness in the right temporalis muscle on palpation. The pain was not controlled by conservative measures. The patient reported no history of previous episodes of TMD. The pain could be shooting in nature and without an obvious stimulus. She also complained of a feeling of nausea.
The Trismus Checklist was implemented and gave affirmative responses to:
absence of history of clicking
pain of non-myofascial origin (e.g. neuralgia)
The patient had a myogenic TMD diagnosis because there was pain on palpation of one of the muscles of mastication. However, she still presented an affirmative response to the Trismus Checklist and so an urgent referral was made to secondary care.
The local Dental Hospital initiated an MRI scan of the TMJs and head. This scan revealed multiple lesions of metastatic malignant melanoma, and the patient was referred on to Oncology.
This case demonstrates that:
the Trismus Checklist acts as a prompt for further action
multiple pathologies can co-exist
even though one correct diagnosis has been made, clinicians should still be open to further issues.
Conclusion
This article highlighted that trismus may be a sign of significant underlying pathology. Vigilance for clinical findings can help safeguard clinicians from missing or misdiagnosing pathology in their patients. There are different ways of measuring mouth opening that can be easily and quickly implemented. These offer an objective measurement that can be recorded and monitored over time. The Trismus Checklist is a simple screening tool to help guide clinicians in their management decisions around trismus. Patients with trismus should be kept under review, regardless of whether they have been referred onwards or not.