
Abstract
Background
The decision-to-delivery interval is the time between the decision to perform an emergency cesarean section and the delivery of the newborn. Prolonged decision-to-delivery interval increase the risk of adverse maternal and neonatal outcomes, including fetal hypoxia, neonatal morbidity, and maternal complications. World Health Organization recommend that delivery should occur within 30 minutes when there is an immediate threat to the life of the mother or fetus. According to the World Health Organization classification, emergency cesarean sections are categorized based on urgency, with Category 1 indicating an immediate threat to maternal or fetal life requiring rapid intervention. However, achieving the recommended decision-to-delivery interval remains challenging in low-resource settings. Therefore, this study aimed to assess delayed decision-to-delivery interval and identify factors among women undergoing emergency cesarean section in public hospitals, Northwest Ethiopia.
Methods
Institution-based cross-sectional study was conducted from January to March 2024 among 523 women who underwent emergency cesarean section in public hospitals. Participants were selected using systematic random sampling. Data were collected using a pretested interviewer-administered questionnaire, medical record review, and an observational checklist assessing operating room readiness and availability of surgical materials. Data were entered into Epi-Data and analyzed using SPSS. Binary logistic regression analysis was used to identify factors.
Result
The proportion of delayed decision-to-delivery interval (>30 minutes) was 79.9% (95% confidence interval: 76.2–83.3). Non-availability of operating room materials (adjusted odds ratio= 12.0; 95% confidence interval: 1.6–89.7), lack of a free operating room (adjusted odds ratio = 4.9; 95% confidence interval: 2.27–10.47), and cesarean section performed by integrated emergency obstetric surgeons (adjusted odds ratio = 2.98; 95% confidence interval: 1.03–8.62) were significantly associated with delayed.
Conclusion
Only one-fifth of emergency caesarean sections met the recommended 30-minute standard. Delays were mainly related to operating room availability, shortages of surgical materials, and surgery performed by integrated emergency obstetric surgeons rather than gynaecologists. Addressing these system-level and human resource constraints, and conducting further qualitative or quality improvement studies, is recommended.
Background
Cesarean section (CS) is a surgical procedure used to deliver a baby through incisions made in the abdominal wall and uterus when vaginal delivery is not safe for the mother or fetus.1,2 CS are generally classified as elective or emergency depending on the urgency of the clinical condition. 3 Elective CS is planned before the onset of labor, while emergency cesarean section (EmCS) is performed when complications arise during pregnancy or labor that threaten the life or health of the mother, fetus, or both. 1
Emergency cesarean section is a critical obstetric intervention aimed at preventing maternal and neonatal morbidity and mortality. In such situations, timely delivery is essential to reduce the risk of adverse outcomes such as fetal hypoxia, birth asphyxia, stillbirth, neonatal morbidity, and maternal complications.3,4 One of the key indicators used to evaluate the timeliness and quality of emergency obstetric care is the decision-to-delivery interval (DDI), which refers to the time between the decision to perform an EmCS and the delivery of the newborn.3,5 This interval includes patient preparation, transfer to the operating room, anesthesia administration, surgical preparation, and the time from skin incision to delivery.6,7 International obstetric guidelines recommend that the DDI for EmCS should ideally not exceed 30 minutes when there is an immediate threat to the life of the mother or fetus. This recommendation has been adopted by professional bodies such as the American College of Obstetricians and Gynecologists and the Royal College of Obstetricians and Gynecologists.8–10 However, achieving this standard is often difficult in low-resource settings due to limitations in infrastructure, shortages of skilled personnel, limited operating room availability, and delays in surgical preparation.
Globally, the use of CS has increased over the past decades. 11 According to the World Health Organization (WHO), the optimal population-level CS rate is between 10% and 15%, as higher rates do not necessarily improve maternal or neonatal outcomes. 12 In Ethiopia, the national CS rate remains relatively low compared with global estimates, although it has increased in recent years. 13 Despite this improvement, maternal and neonatal mortality remain major public health concerns in the country. 14 The Ethiopian Demographic and Health Survey reported a maternal mortality ratio of 412 per 100,000 live births and a neonatal mortality rate of 29 per 1,000 live births, highlighting the need to improve the quality and timeliness of emergency obstetric services. 15
Several studies conducted in low- and middle-income countries have reported that the majority of EmCS are performed beyond the recommended 30-minutes DDI. For example, studies in Tanzania and Ethiopia reported that only a small proportion of women receive EmCS within the recommended time frame. 16 Previous studies in Ethiopia, including those conducted in Gondar, 17 Bahir Dar, 18 and South Gondar Zone, 19 showed that between 79% and 85% of EmCS were performed after the recommended 30-minute interval.
Delayed decision-to-delivery interval has been associated with poor maternal and neonatal outcomes, including low Apgar score, neonatal intensive care unit admission, perinatal asphyxia, stillbirth, and increased maternal morbidity.19,20 Evidence suggests that newborns delivered after prolonged DDI are more likely to experience adverse neonatal outcomes compared with those delivered within the recommended time frame. 21
Although some studies in Ethiopia have examined the outcomes of CS, limited evidence exists regarding the magnitude of delayed DDI and the factors contributing to these delays, particularly in different health-care settings. Understanding these factors is important for improving the quality of emergency obstetric care and reducing preventable maternal and neonatal complications. Therefore, this study aimed to assess the magnitude of delayed DDI and identify associated factors among women undergoing EmCS in public hospitals of West and North Gojjam Zones, Northwest Ethiopia.
Methods
Study design, setting, and period
An institution-based cross-sectional study was conducted from January 20 to March 20, 2024 in public hospitals located in West Gojjam Zone and North Gojjam Zone, Amhara Regional State, Ethiopia. These two zones were previously part of the unified West Gojjam administrative zone before being divided into separate administrative zones.
The zones are located approximately 385 km northwest of Addis Ababa, the capital city of Ethiopia. Finote Selam is the administrative town of West Gojjam Zone, while Bahir Dar serves as the administrative center of North Gojjam Zone.
According to the zonal health departments, the two zones together have seven public hospitals, including six primary hospitals and one general hospital, all of which provide comprehensive emergency obstetric and surgical services. In these hospitals, obstetric services including EmCS are provided by obstetricians and gynecologists and integrated emergency obstetric surgeons (IEOS).
When a pregnant woman arrives with an obstetric emergency requiring CS, the attending clinician evaluates the patient and makes a clinical decision for EmCS. After the decision is made, the patient is prepared for surgery, informed consent is obtained, anesthesia is administered, and the patient is transferred to the operating room where the surgical team performs the procedure.
Based on reports from the zonal health offices, approximately 5,000 EmCS are performed annually in these hospitals. During the three months corresponding to the study period in the previous year, approximately 1,066 EmCS were conducted across these hospitals. The total population of the two zones is estimated at 2,474,254, of whom 1,253,777 are females. 22
Source and study population
All women who came for delivery service and undergone EmCS in West and North Gojjam zone public hospitals were the source population. All women in West and North Gojjam zone public hospitals who had undergone to EmCS during the study period were the study population.
Eligibility criteria
All women who had undergone to EmCS during the study period in West and North Gojjam zone public hospitals were included in the study.
Women with uterine rupture requiring immediate surgical intervention before standard surgical preparation, and those with incomplete or missing key clinical data required to determine the decision-to-delivery interval, were excluded from the study.
Sample size and sampling procedure
Sample size determination
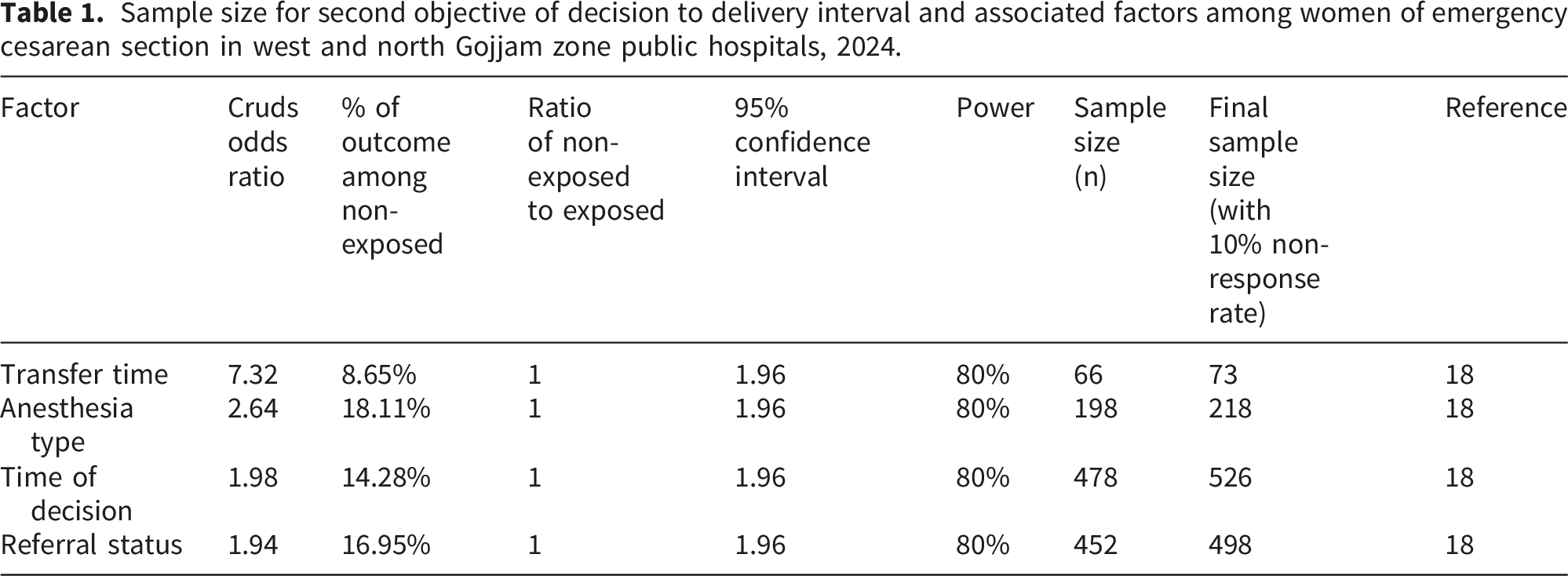
Sample size for second objective of decision to delivery interval and associated factors among women of emergency cesarean section in west and north Gojjam zone public hospitals, 2024.
Sampling procedure
All seven hospitals were included. The total sample size was proportionally allocated to each hospital based on the number of EmCS performed in the corresponding three-month period of the previous year. A systematic random sampling technique was used in each hospital. The sampling interval (K) was calculated by dividing the total number of EmCS in the hospital by the allocated sample size. The first participant was selected by simple random sampling from the first interval, and then every K-th eligible woman was included (Figure 1). Schematic diagram showed the sampling procedure of decision to delivery interval and associated factors among women of emergency cesarean section in west and north Gojjam zone public hospitals, 2024.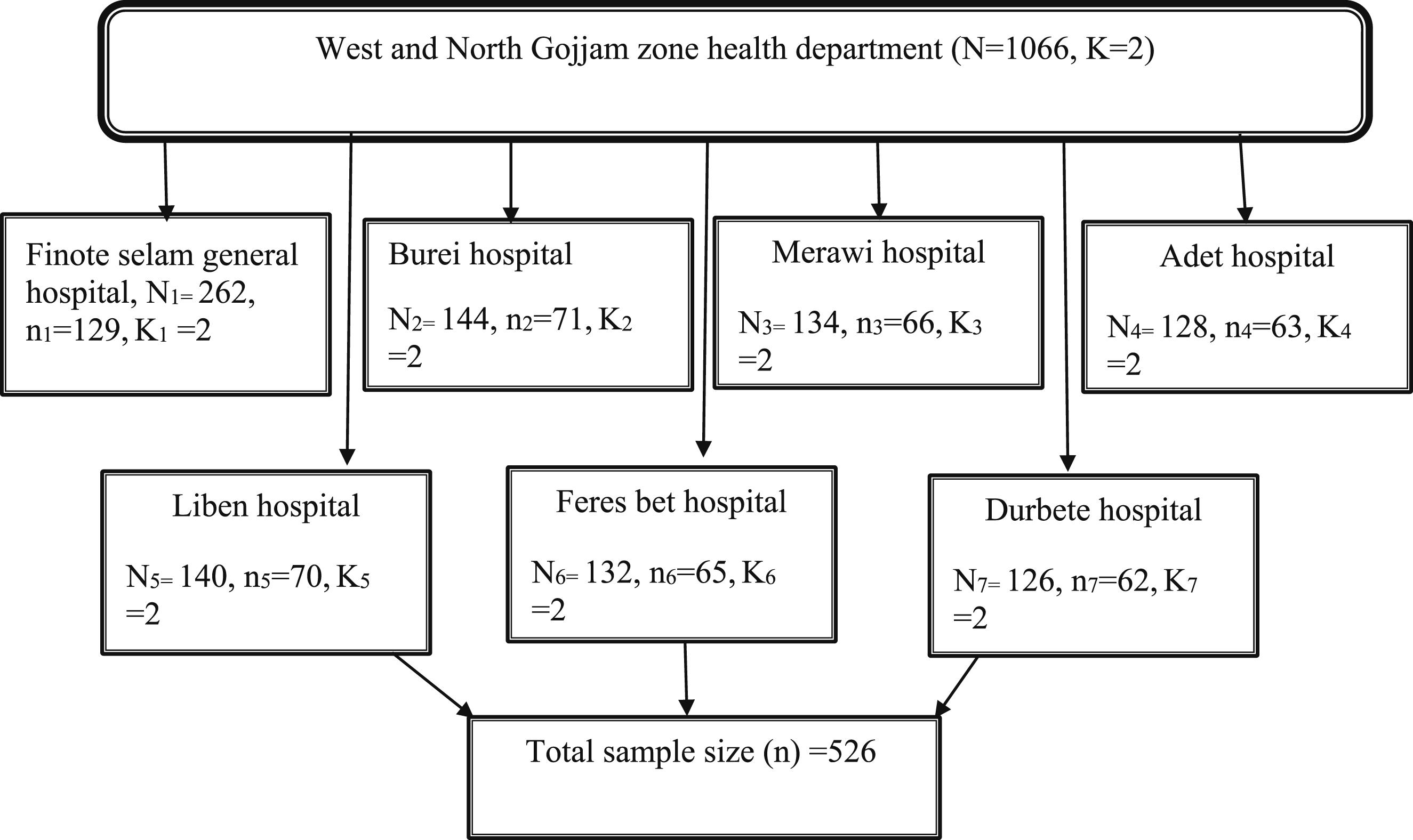
Variables of the study
Dependent variable
Decision-to-delivery interval (categorized as delayed >30 minutes vs. standard ≤30 minutes)
Independent variables
Operational definitions
Data collection tool and procedure
Data were collected using a structured questionnaire, observational checklist, and medical record review. The questionnaire was initially developed in English after reviewing relevant literature and was adapted to the local context.10,18 It was then translated into Amharic and back-translated into English to ensure consistency.
The questionnaire included sections on: • socio-demographic characteristics • obstetric history • resource availability • surgical team factors
A structured observation checklist was used prospectively at the time the decision for EmCS was made to document real-time availability of operating room, surgical materials, drugs, staff readiness, and transfer time. These operational variables could not be reliably retrieved retrospectively. Although we observed the time interval from decision to delivery for each participant, the data were collected at a single point in time (during the same surgical episode), which is consistent with a cross-sectional design. Each woman contributed only one observation, and we did not follow anyone beyond the surgery.
Data collectors were trained midwives, and supervision was conducted by public health professionals. A one-day training session was provided covering the study objectives, data collection procedures, ethical considerations, and proper completion of the questionnaire.
Data collection began when the decision for EmCS was made and ended at the time of fetal delivery.
Data quality assurance
To ensure data quality, the questionnaire was pretested on 5% of the sample size (27 women) at Debre Markos Comprehensive Specialized Hospital, which was not our study area. Necessary modifications were made based on the pretest findings. Daily supervision and cross-checking were performed to ensure completeness and consistency of the collected data
Data processing and analysis
Data were coded and entered into Epi-Data version 4.2 and exported to SPSS version 25 for analysis.
Binary logistic regression analysis was performed to identify factors associated with delayed decision-to-delivery interval. Variables with a p-value <0.20 in bivariable analysis were entered into multivariable logistic regression.
The Adjusted Odds Ratio (AOR) with 95% confidence interval was used to measure the strength of association. Statistical significance was declared at p < 0.05.
Model fitness was assessed using the Hosmer-Lemeshow goodness-of-fit test.
Result
Socio-demographic characteristics of the respondents
A total of 523 women who underwent EmCS participated in the study, yielding a response rate of 99.4%. The median age of the participants was 27 years (IQR: 24–31).
Socio-demographic characteristics of women who underwent emergency cesarean section in public hospitals of West and North Gojjam Zones, Northwest Ethiopia, 2024 (n = 523).
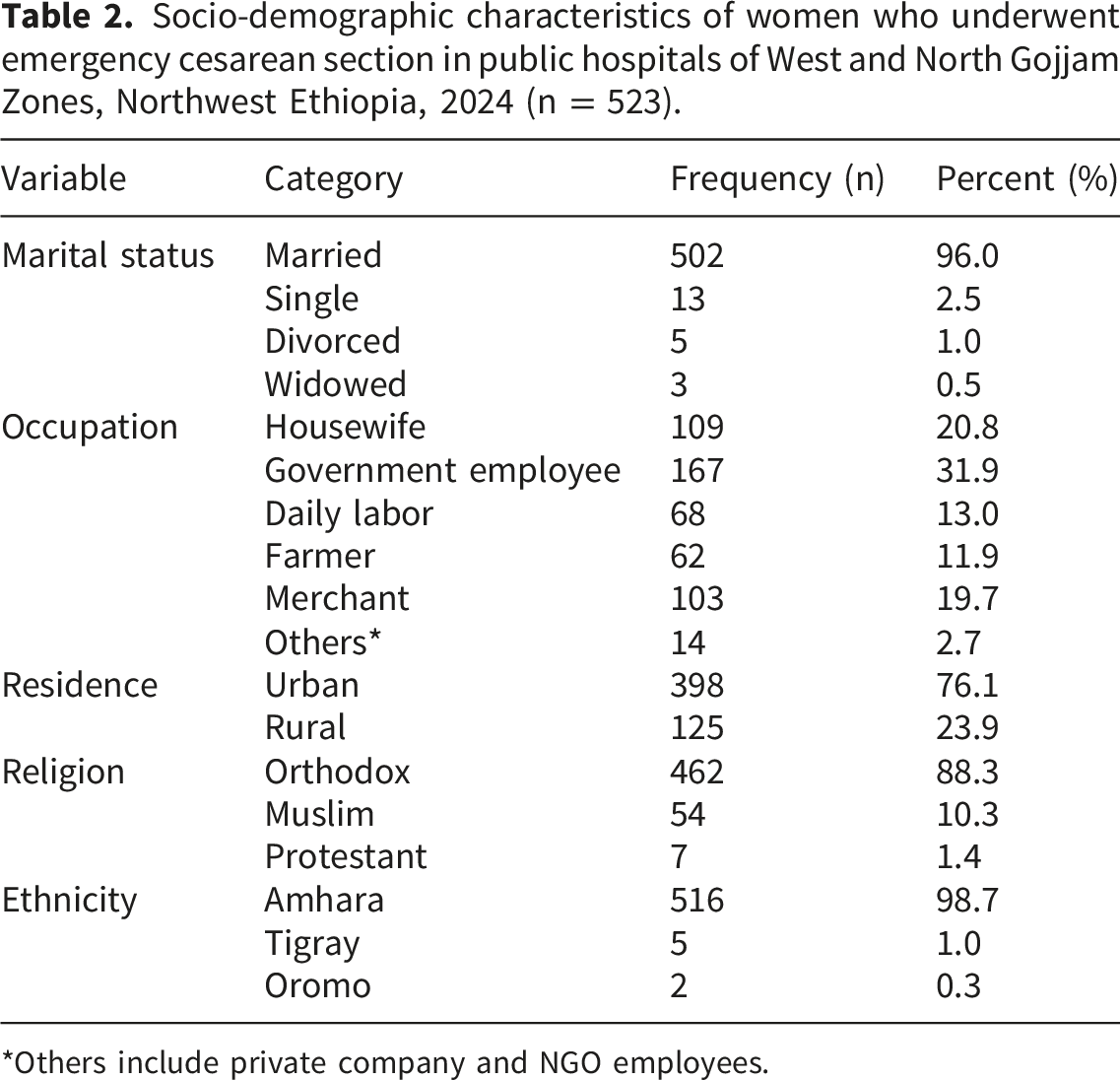
*Others include private company and NGO employees.
Obstetrics related characteristics of the respondents
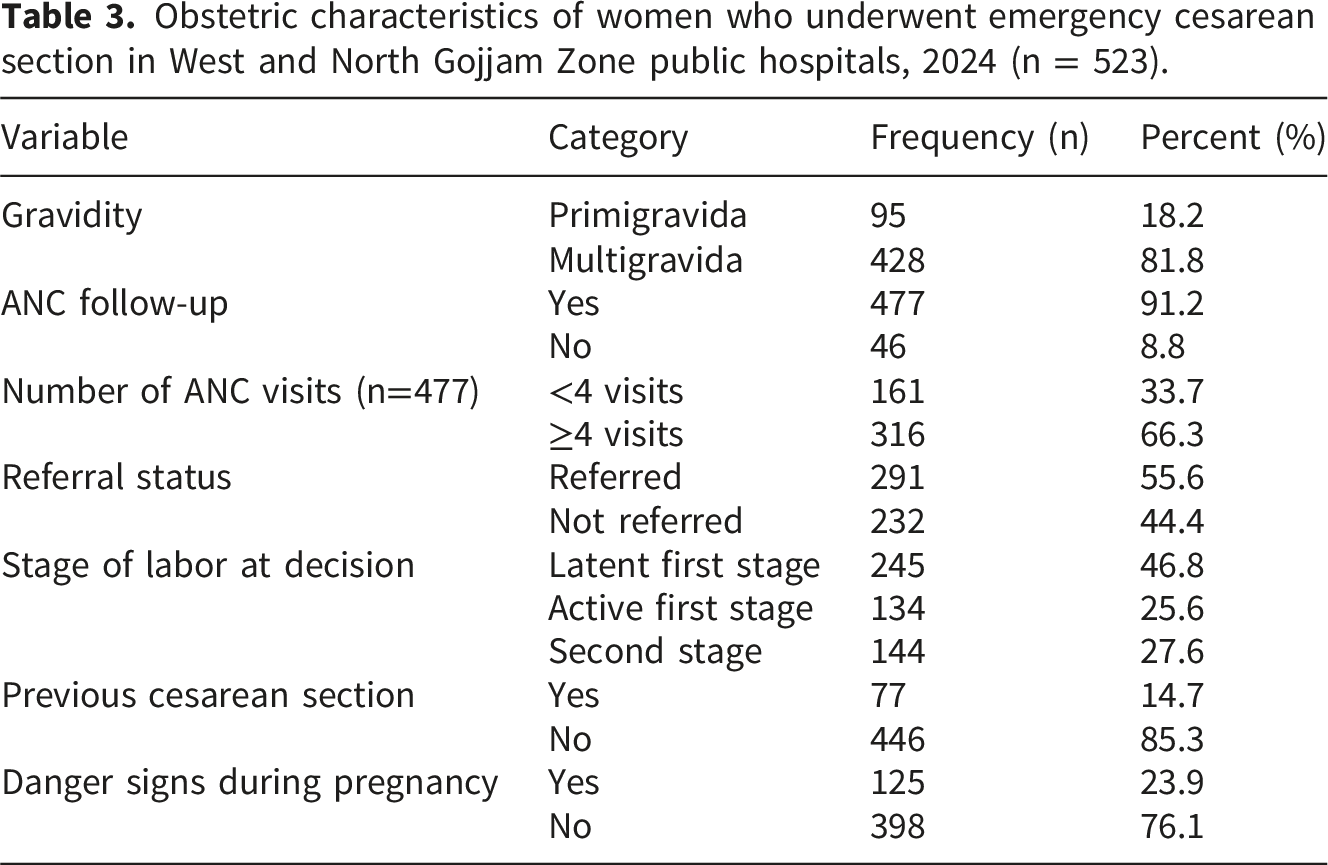
Among the participants, 428 (81.8%) were multigravida, and 477 (91.2%) had attended antenatal care during the index pregnancy. Among those who had ANC follow-up, 316 (66.3%) had four or more visits.
More than half of the participants 268 (51.2%) reported knowing their last normal menstrual period. Regarding referral status, 291 (55.6%) of the mothers were referred from other health facilities.
In relation to the stage of labor at the time of decision for EmCS, 245 (46.8%) were in the latent phase of the first stage of labor, 134 (25.6%) were in the active phase, and 144 (27.6%) were in the second stage of labor.
Obstetric characteristics of women who underwent emergency cesarean section in West and North Gojjam Zone public hospitals, 2024 (n = 523).
Regarding the indications for EmCS, non-reassuring fetal heart rate was the leading indication, accounting for 121 (22.4%) of cases. This was followed by cephalopelvic disproportion, which accounted for 113 (21.0%) of the cases. The distribution of indications for EmCS is presented in (Figure 2). Bar chart showing the indications for emergency cesarean section among women who underwent the procedure in public hospitals of West and North Gojjam Zones, Northwest Ethiopia, 2024 (n = 523). Other = Previous cesarean section history and failed instruments.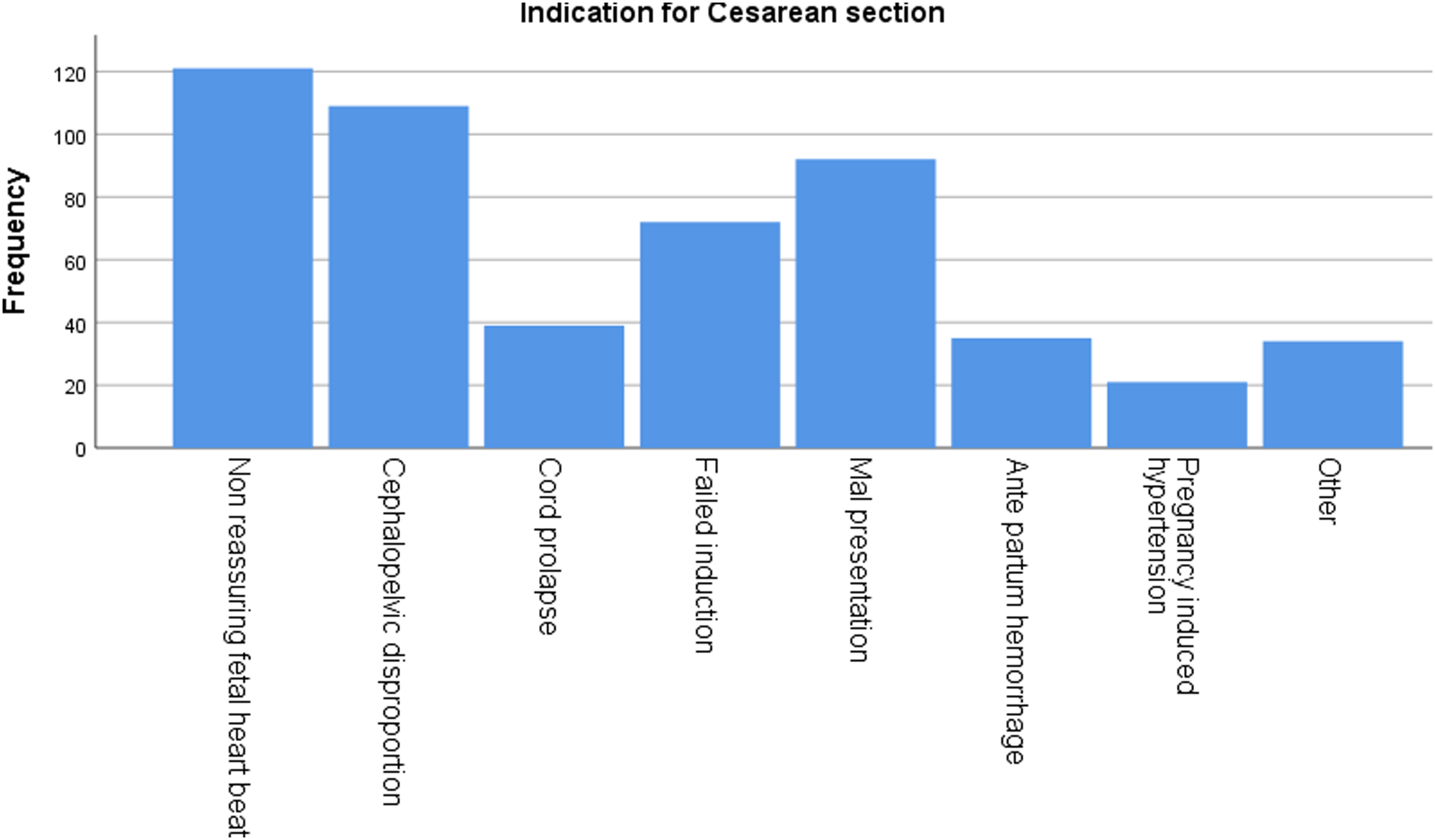
Anesthesia and operation room related factors
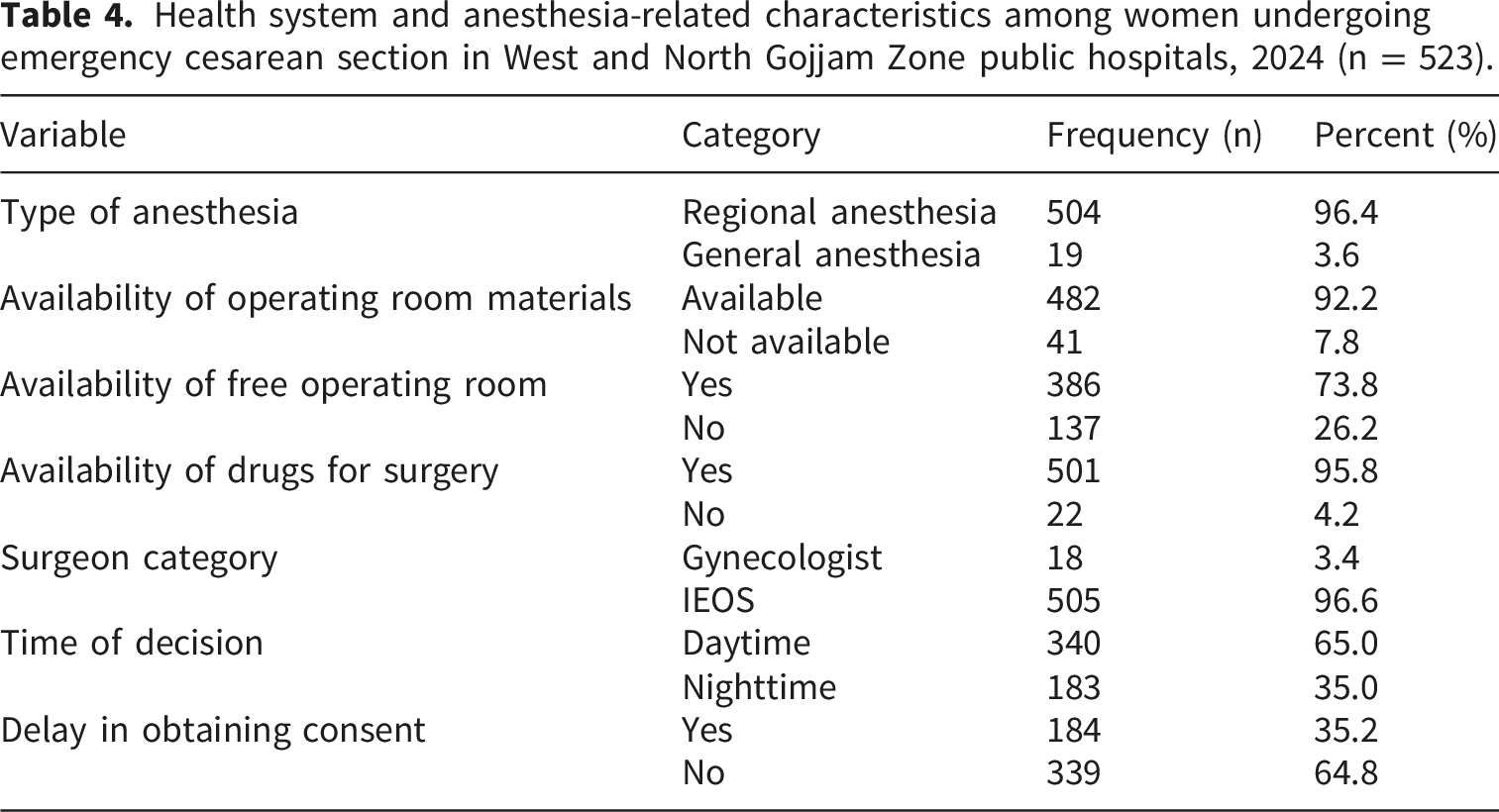
Most EmCS 504 (96.4%) were performed under regional anesthesia, while the remaining procedures were conducted under general anesthesia.
Regarding operating room readiness, 482 (92.2%) of the procedures were performed when the required surgical materials were available, and 386 (73.8%) of the procedures were conducted when a free operating room was available at the time of decision.
Health system and anesthesia-related characteristics among women undergoing emergency cesarean section in West and North Gojjam Zone public hospitals, 2024 (n = 523).
Magnitude of delayed decision-to-delivery interval
This study found that 79.9% (95% CI: 76.2–83.3) of EmCS had a delayed decision-to-delivery interval (>30 minutes).
The median decision-to-delivery interval was 40 minutes (IQR: 32–50 minutes). The minimum and maximum recorded intervals were 15 minutes and 120 minutes, respectively. Half of the EmCS were performed after 40 minutes from the time of decision, and 75% were completed within 50 minutes
Factors associated with delay in decision to delivery interval
In the bivariable logistic regression analysis, several variables were associated with delayed DDI interval at a p-value <0.20, including: • delay in obtaining consent • stage of labor at decision • non-availability of operating room materials • lack of a free operating room • surgeon category • presence of danger signs during pregnancy • need for patient stabilization before surgery • non-availability of drugs required for surgery
Factors associated with delayed decision-to-delivery interval among women undergoing emergency cesarean section in West and North Gojjam Zone public hospitals, 2024 (n = 523).
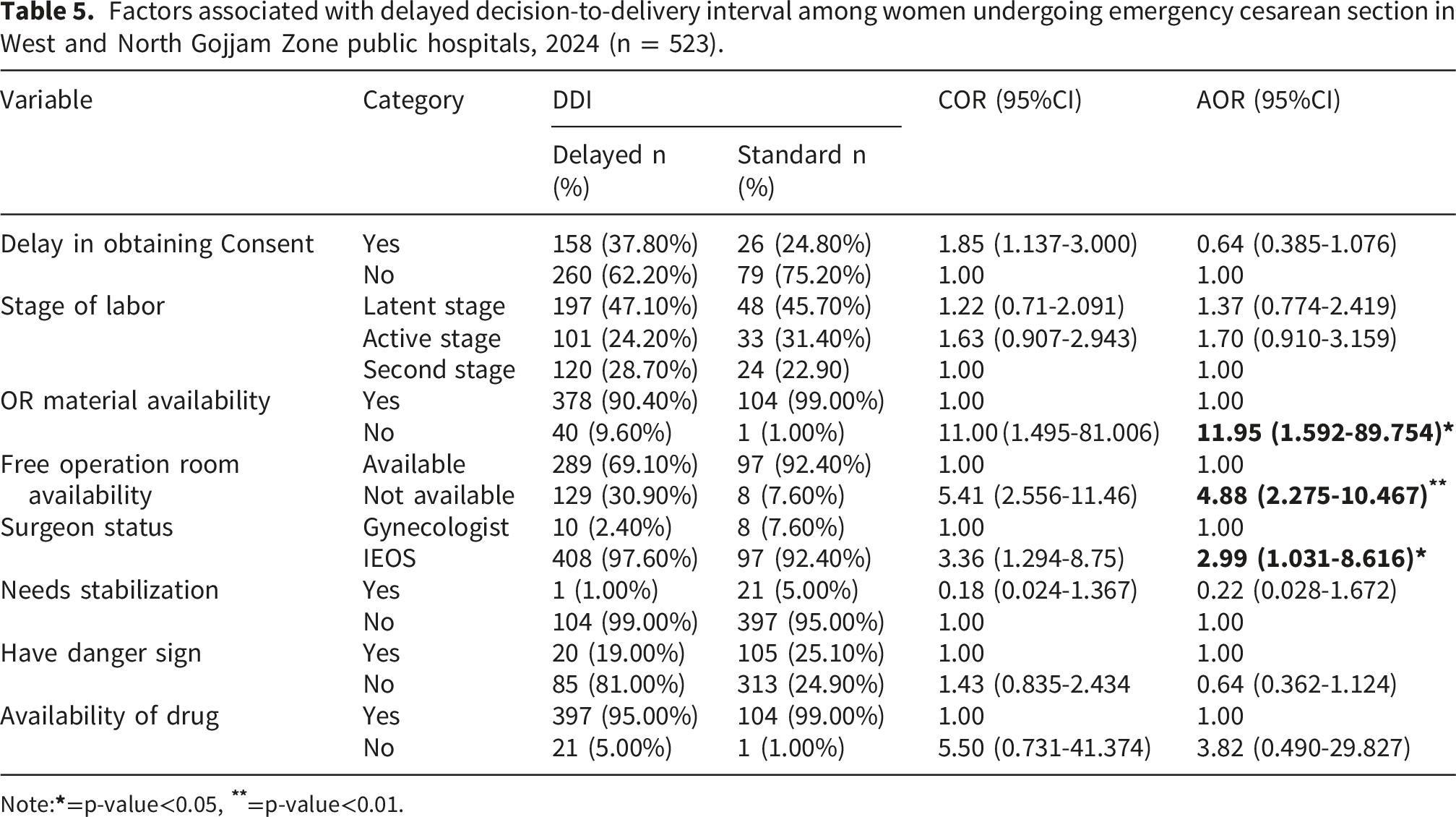
Note:
Discussions
This study found that 79.9% (95% CI: 76.2–83.3) of EmCS experienced a delayed DDI exceeding the recommended 30 minutes. This finding indicates that only a small proportion of EmCS deliveries met the internationally recommended time standard, highlighting challenges in providing timely emergency obstetric care in the study setting.
The proportion of delayed DDI in this study is higher than findings from a hospital-based cross-sectional study conducted in tertiary hospitals in India, where 57.6% of EmCS were delayed. 24 The difference may be explained by variations in health system capacity and study settings. The Indian study was conducted in tertiary referral hospitals with multiple operating theatres, better availability of surgical materials, and a higher number of senior obstetric specialists, which may facilitate faster surgical preparation and decision implementation.
Conversely, the proportion of delayed DDI in the present study is slightly lower than that reported in a hospital-based cross-sectional study conducted in northern Tanzania, where 87.7% of EmCS exceeded the recommended DDI. 25 Differences in institutional workflow, resource availability, and patient load across facilities may explain this variation.
The finding of this study is comparable with previous institution-based cross-sectional studies conducted in Ethiopia, including studies from Bahir Dar public hospitals (79.7%), the University of Gondar Comprehensive Specialized Hospital (80.4%), and South Gondar Zone public hospitals (82.5%).17–19 The similarity may be attributed to comparable health system structures, clinical management protocols, and resource constraints within public hospitals in Ethiopia.
In contrast, another cross-sectional study conducted in Bahir Dar city public hospitals reported a slightly higher proportion of delayed DDI (85.5%). 10 In that study, the use of general anesthesia was identified as a significant contributor to delayed DDI, whereas in the present study most cesarean sections (96.4%) were performed under spinal anesthesia, which may have reduced preparation time for anesthesia and contributed to a relatively lower proportion of delay.
The availability of operating room materials was significantly associated with delayed DDI in this study. Women for whom surgical materials were not readily available at the time of decision were more likely to experience delays. This finding is consistent with studies conducted at the University of Gondar Comprehensive Specialized Hospital and South Gondar Zone public hospitals,17,19 which reported that delays in collecting surgical instruments and supplies contributed to prolonged DDI. In low-resource settings, shortages of surgical supplies or delays in retrieving them from central stores may prolong the preparation process. In addition, limited birth preparedness and logistical arrangements may delay the procurement of necessary surgical materials, further extending the time between decision and delivery.
Similarly, the absence of a free operating room was significantly associated with delayed DDI. Women who required EmCS when no operating room was available were nearly five times more likely to experience delayed delivery compared with those who had immediate access to an operating theatre. This finding is consistent with a hospital-based study conducted in Nigeria, 26 which reported that limited operating theatre availability contributed to delays in emergency surgical procedures. Competition for operating theatre space, particularly in facilities with only one operating room serving multiple surgical departments, may result in prolonged waiting time before surgery can begin.
The category of the surgical provider was also significantly associated with delayed DDI. Emergency cesarean sections performed by IEOS were more likely to experience delayed DDI compared with those performed by obstetricians/gynecologists. A similar finding was reported in a cross-sectional study conducted in Bahir Dar city public hospitals, 18 where procedures performed by obstetricians were more likely to achieve the recommended DDI. This difference may be related to variation in clinical experience, decision-making speed, and exposure to complex obstetric emergencies.
Limitation of the study
Several limitations should be considered. The observational component may have introduced a Hawthorne effect, artificially shortening recorded decision-to-delivery intervals. Incomplete medical records led to exclusion of some cases, potentially introducing selection bias. The cross-sectional design allows only associations, not causation.
Conclusion and recommendation
This study found that 79.9% of emergency caesarean sections in public hospitals of West and North Gojjam Zones, Northwest Ethiopia, exceeded the recommended 30-minute decision-to-delivery interval, meaning that only one-fifth of women received timely emergency obstetric care.
The non-availability of operating room materials, lack of a free operating room, and surgery performed by integrated emergency obstetric surgeons (IEOS) rather than gynaecologists were significantly associated with delayed DDI. These findings highlight that system-level factors (operating room readiness and resource availability) and human resource factors (surgeon category) are key determinants of timely EmCS. Strengthening operating room preparedness, ensuring consistent availability of surgical supplies, and addressing provider-related delays could help reduce the proportion of prolonged DDI.
Supplemental material
Supplemental material - Decision-to-delivery interval and associated factors among women undergoing emergency caesarean section in public hospitals of West and North Gojjam Zones, Northwest Ethiopia: A cross-sectional study, 2024
Supplemental material for Decision-to-delivery interval and associated factors among women undergoing emergency caesarean section in public hospitals of West and North Gojjam Zones, Northwest Ethiopia: A cross-sectional study, 2024 by Nurlign Zelalem, Mulunesh Alemayehu, Mulatu Kassahun, Bekalu Endalew, Daniel Mulat Eshetu, Alehegn Chalie, Andinet Bewketu and Gedefaw Diress in Sage Open Medicine
Footnotes
Acknowledgments
First, we would like to acknowledge the study participants for their involvement; without them, this research would not have been possible. We also express our heartfelt gratitude to the Department of Public Health at Debre Markos University College of Medicine and Health Sciences. Our thanks go to the administration of west and north Gojjam zone public hospitals administrations for providing the necessary data for this study. Furthermore, we extend our sincere appreciation to the data collectors for their valuable contributions.
Ethical considerations
Ethical clearance was obtained from the Institutional Review Board of Debre Markos University, College of Medicine and Health Sciences (Approval No: MHSC/R/C/TT/D/123//11/15). Permission letters were obtained from the respective zonal health departments and participating hospitals.
Consent to participate
Written informed consent was obtained from all participants. For participants who were unable to read and write, the consent form was read and explained in the local language, and informed consent was obtained using a thumbprint in the presence of an independent witness. Data collectors ensured privacy by interviewing participants after stabilization and recovery from procedures, and interviews were conducted in a private setting. Participants who declined to participate continued to receive routine clinical care without any interference.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used for this study are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.