
Abstract
Background
The effects of probiotics and synbiotics on bone health remain uncertain due to conflicting results across existing systematic reviews and meta-analyses (SRs/MAs).
Methods
PubMed/Medline, Cochrane, and Web of Science were searched through February 2025. SRs/MAs on probiotics or synbiotics for bone health were included. An umbrella review with meta-analysis of pooled effect sizes was conducted using random-effects models: Hedges’ g for bone mineral density (BMD) and muscle mass, and mean difference for muscle strength. Heterogeneity was assessed via I2, and AMSTAR2 rated confidence. PROSPERO ID: CRD42025636002.
Results
Our initial search identified 930 articles (488 from PubMed/MEDLINE, 260 from Web of Science, and 182 from Cochrane). After removing duplicates and screening titles, abstracts, and full texts, sixteen systematic reviews and meta-analyses were included (with 3,245 participants), and only human studies were considered for meta-analysis. Most studies investigated Lactobacillus and Bifidobacterium strains as probiotics. Probiotics and synbiotics supplementation significantly improved BMD (Weighted mean difference (WMD) = 0.39, 95% Confidence interval (CI): 0.14, 0.63, p = 0.002), muscle mass (WMD = 0.46, 95% CI: 0.23, 0.68, p < 0.001), and muscle strength (WMD = 1.99, 95% CI: 0.42, 3.57, p = 0.013). Subgroup analyses identified BMD measurement site, number of studies, sample size, and gender as sources of heterogeneity. According to AMSTAR2, 11 reviews were rated as high confidence, one as moderate confidence, and four as low confidences.
Conclusion
Probiotic/synbiotic supplementation showed modest, statistically significant BMD benefits, but with substantial heterogeneity. Findings for muscle mass and strength were based on a few meta-analyses, showed high heterogeneity, and sensitivity analyses nullified significance. Current evidence does not support clinical recommendations for probiotics/synbiotics in bone health prevention.
1. Introduction
Bone health is fundamental to overall physical function, as bones provide structural support, protect vital organs, and enable mobility. Maintaining strong and healthy bones depends critically on the balance between bone resorption and bone formation.1–3 Low bone mineral density (BMD) leads to significant disability, increased dependency, diminished quality of life, and higher economic burdens on healthcare systems.3–5 The World Health Organization (WHO) recognizes reduced bone density and mass as a major public health concern, particularly among older adults and postmenopausal women.1,3 Identified risk factors include age, female sex, family history, low body weight, sedentary lifestyle, smoking, and excessive alcohol consumption.3,4 Medications, bone diseases, and insufficient physical activity also adversely affect bone health. Previous studies have further indicated that hormone levels, immune cells, and gastrointestinal functions play roles in maintaining bone balance.6,7
The gastrointestinal tract absorbs bone-relevant minerals (calcium, magnesium, phosphorus) and produces endocrine factors (incretin, serotonin) that signal to bone cells, yet the precise mechanisms in humans remain unclear, with most evidence from animal or in vitro models.7–9 Gut microbiota (GM) is thought to influence bone health through nutrient absorption, vitamin synthesis, and modulation of inflammation.10–13 However, the direction of this relationship is uncertain: GM changes could drive bone loss, or conversely, osteoporosis-related shifts may alter GM composition.3,5,8 Dietary interventions are frequently promoted for osteoporosis, but high-quality evidence is limited by recall bias and few fracture endpoints; whether diet alone can reverse bone loss in established osteoporosis remains an open question.14,15
Recent systematic reviews and controlled trials indicate that probiotics and synbiotics play a crucial role in maintaining a healthy GM and enhancing overall well-being. Probiotics are described as live microorganisms that grant health benefits when administered in sufficient amounts.16,17 On the other hand, synbiotics refer to the synergistic combination of probiotics and prebiotics. Preclinical and small clinical trials suggest that probiotics can enhance the absorption of essential nutrients, such as magnesium and calcium, thereby fortifying the skeletal structure.16–18 By fostering a balanced GM, these beneficial microorganisms contribute to the reduction of inflammation linked to various chronic conditions that impact both gastrointestinal and bone health. This underscores the interrelationship between digestive health and skeletal integrity, implying that prioritizing the gut microbiome may yield substantial benefits for overall health.19–21
Studies on the relationship between bone health and probiotics have yielded conflicting results. Several SRs/MAs report modest benefits, while others find null effects, particularly when stratified by age, sex, or intervention duration. For example, Huang et al. (2022) reported that oral probiotic supplementation improved gut microbiota diversity and promoted bone growth and density. 8 However, the study by Sergeev et al. (2020) reported no significant effects. Their three-month study revealed that probiotic capsules did not affect bone mineral content in individuals with osteoporosis. 22
To date, at least 16 systematic reviews and meta-analyses have examined the effect of probiotics/synbiotics on bone health, with conflicting findings regarding population subgroups (age, sex, menopausal status), intervention duration, and bone sites. An umbrella review is therefore appropriate to synthesize this existing review-level evidence, assess the confidence in reported effects using AMSTAR2, and conduct a meta-analysis with overlap control and subgroup analyses. Considering the rising prevalence of aging-related issues, we aim to investigate skeletal changes in systematic reviews and meta-analyses in response to probiotics and synbiotic supplementation to gain a comprehensive understanding of their impact on bone health as the primary outcome, with muscle outcomes considered only as secondary outcomes.
2. Methods
2.1. Study design
We carried out this umbrella review with a meta-analysis following the Cochrane Handbook for Systematic Reviews of Interventions. The results were reported consistently with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (Supplemental Table 1). 23 This umbrella review identified all systematic reviews and meta-analyses regarding the effect of probiotics and synbiotics supplementation on bone and muscle health. The study protocol is registered in PROSPERO (CRD42025636002).
2.2. Literature search
Two investigators (NL and MM) independently searched the PubMed, Medline, Web of Science, and Cochrane databases from inception to 6 February 2025 to identify meta-analyses and systematic reviews of clinical trials and animal studies. The search strategy was designed accordingly to keywords including “Bone health”, “Osteoporosis”, “Osteopenia”, “Bone Disease”, “Low Bone Density”, “Bone Mineral Density”, bone loss”, “probiotic*”, “synbiotic*”, “Lactobacillus”, and “Bifidobacterium”. Supplemental Table 2 elucidates the search strategy.
All identified publications underwent a three-step parallel review of titles, abstracts, and full texts based on predefined both inclusion and exclusion criteria by two researchers (N.L. and M.M.), with discrepancies resolved by consensus (HS.E.).
2.3. Eligibility criteria
The umbrella review included meta-analyses and systematic reviews that performed quantitative analyses of the effect of probiotics and synbiotics on bone health.
Studies have been screened based on the following PICOS: 1. Population: subjects with or without previous osteoporosis disorders or animal models that had or had not undergone aging-inducing manipulations. 2. Intervention: any probiotics or synbiotics supplementation. 3. Comparators: subjects or animal models matching the population of interest who are given a placebo or a control group without intervention. 4. Outcome: Our primary outcomes were changes in bone parameters. Secondary outcomes included plasma biochemical profile, inflammatory markers, muscle mass, and muscle strength. 5. Type of study: systematic reviews and meta-analyses.
The exclusion criteria: 1. Original articles, letters, editorials, narrative reviews. 2. Studies reported a response to probiotics or synbiotics supplementation without investigating bone and muscle health.
2.4. Data extraction and data synthesis
We extracted baseline characteristics of the studies, including the first author, publication year, country, study design, study groups, and population characteristics, type and duration of intervention, and primary and secondary outcomes, including bone parammeters, plasma biochemical profile, inflammatory markers, muscle mass, and muscle strength. Additionally, we noted protocol registry, risk of bias assessment tools, source of heterogeneity assessment method, and publication bias assessment method.
The extracted studies included two categories of animal and human studies. Only meta-analyses on human studies were included in the meta-analysis, and the rest were examined in the systematic review. The overlap between primary studies across included meta-analyses has been checked. We combined the results of the included meta-analyses, because the percent of overlap was less than 15% among the included meta-analyses. The overlap among the included meta-analyses was assessed using the Corrected Covered Area (CCA) method. The calculated CCA was 3.57%, indicating a slight overlap among the included reviews. Thus, we combined the results of the included meta-analyses.
Regarding the existing heterogeneity among studies, the pooled ES and 95% CI were evaluated using random effects models with a restricted maximum likelihood approach. The effect sizes are weighted mean difference (WMD) in this study. Also, significant heterogeneity between studies was examined using the I2 statistic and Cochrane’s Q test, which is indicated by I2 values above 50% or Q test p values below 0.1. 24 In order to point out the sources of variation, we conducted a subgroup analysis based on the BMD measure point, number of studies, sample size, and the gender of the participants. Sensitivity analysis was also used to determine the impact of excluding a specific study on the overall effect size (WMD).
To evaluate publication bias, we visually inspected funnel plots. However, because fewer than 10 studies were included in each meta-analysis, formal regression-based tests (Begg’s tests) have low power. Instead, we assessed funnel plot asymmetry cautiously. When asymmetry suggestive of a small-study effect was observed, we applied the trim-and-fill method as a sensitivity analysis to estimate the potential impact of unpublished or missing studies on the pooled effect sizes.25–27P-values below 0.05 specified significance. All analyses were performed using STATA version 17.0 (Stata Inc., College Station, Texas, USA).
2.5. Quality assessment
We assessed the methodological quality of the included systematic reviews using AMSTAR2 (A MeaSurement Tool to Assess Systematic Reviews). 28 The AMSTAR2 criteria encompass items related to protocol registration before the commencement of the review (item 2), adequacy of the literature search (item 4), justification for excluding individual studies (item 7), risk of bias from individual studies being included in the review (item 9), appropriateness of meta-analytical methods (item 11), consideration of risk of bias when interpreting the results of the review (item 13), and assessment of the presence and likely impact of publication bias (item 15).
Following AMSTAR2 guidance, we did not calculate a numerical overall score. Instead, two authors (N.L. and M.M.) independently rated each review’s overall confidence as high, moderate, low, or critically low based on critical domain failures (items 2, 4, 7, 9, 11, 13, 15). A review was rated low confidence if it had one or more critical domain failures and critically low confidence if it had multiple critical domain failures. Any disagreement was resolved by the senior author (H.S.E.). Critical-domain failures identified in the included reviews are reported in Supplemental Table 3 (e.g., lack of a registered protocol [item 2], inadequate literature search [item 4], and/or failure to justify study exclusions [item 7]).
3. Results
Our initial search identified 930 articles (488 from PubMed/MEDLINE, 260 from Web of Science, and 182 from Cochrane). After removing duplicates and screening titles and abstracts, we narrowed the selection to 81 articles. We then assessed the full texts, resulting in the inclusion of sixteen systematic reviews and meta-analyses in our umbrella review (Figure 1). Of the 81 full-text articles assessed, 65 were excluded for the following reasons: 29 were primary studies (not systematic reviews/meta-analyses), 18 had no relevant bone or muscle outcomes, 12 were narrative reviews or editorials, 4 did not administer probiotics/synbiotics as the intervention, and 2 had insufficient data for extraction. Flow chart of study selection for inclusion studies in the umbrella review.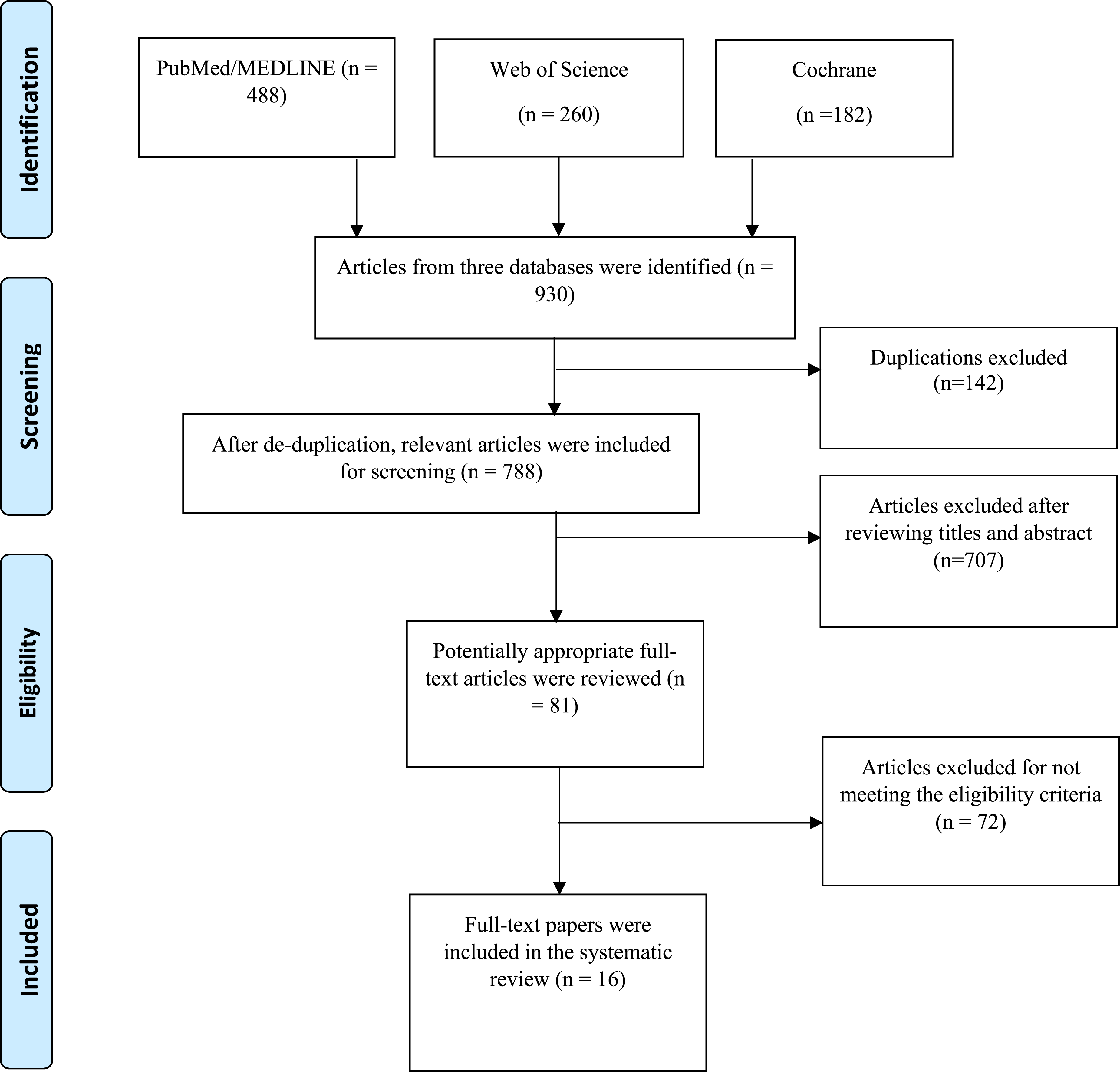
In this umbrella review, each “included study” is a systematic review or meta-analysis (SR/MA). The narrative synthesis of skeletal parameters, biochemical markers, and inflammatory outcomes (sections 3.3 and 3.4) reports the findings as stated by the included SRs/MAs; we did not re-analyse their primary data (section 3.5). For combining the results of the included meta-analyses, we used WMD when it was possible.
3.1. Characteristics of the included studies
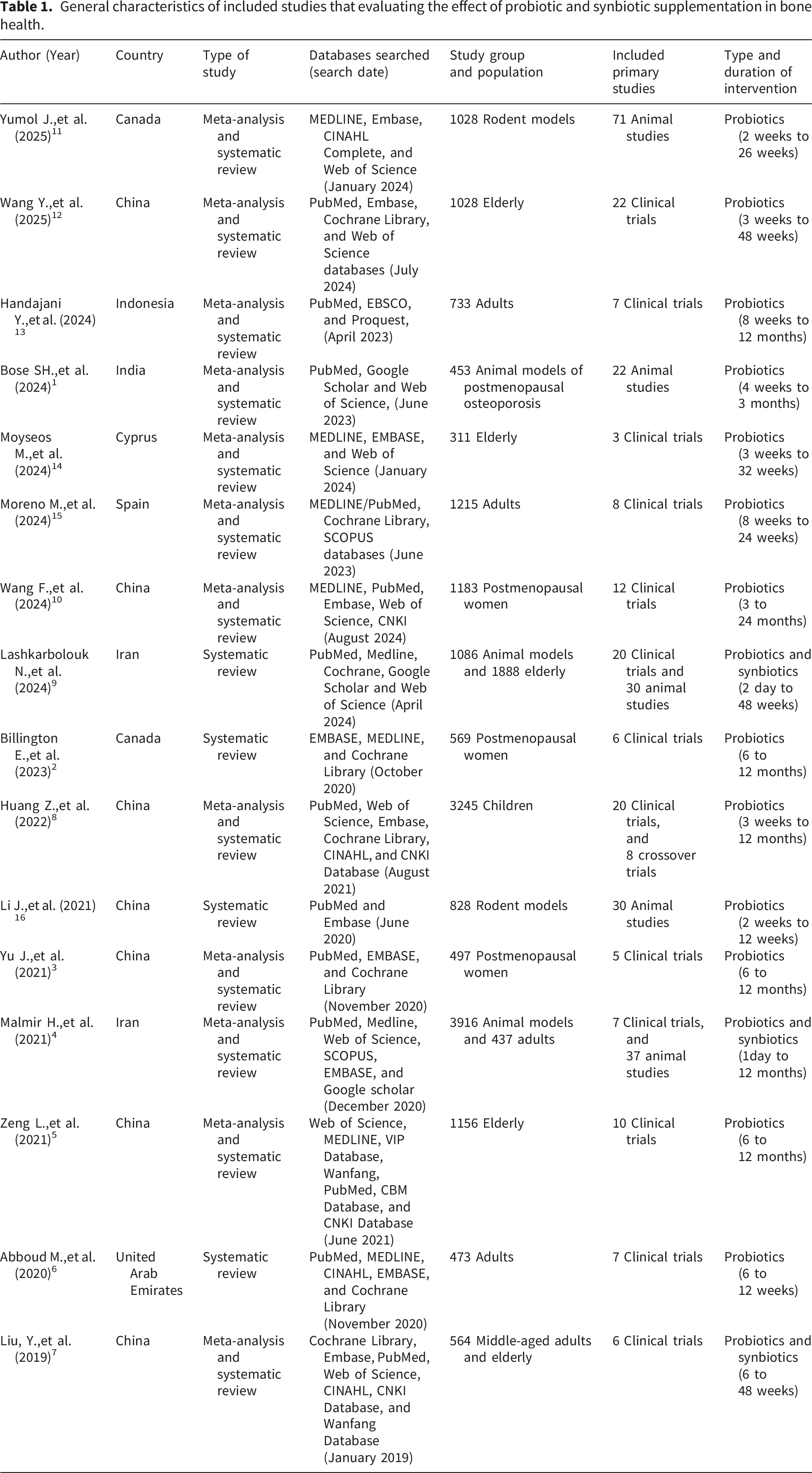
Our umbrella review included seven studies originating from China,3,5,7,8,10,12,16 two from Iran,4,9 two from Canada,2,11 and one each from India, 1 Indonesia, 13 Spain, 15 Cyprus, 14 and Dubai. 6 Three studies focused on probiotics and synbiotics,4,7,9 while thirteen exclusively examined probiotics.1–3,5,6,8,10–16
Among the 16 included studies, 12 were systematic reviews with meta-analyses (references 1, 3–5, 7, 8, 10–15) and 4 were systematic reviews without meta-analysis (references 2, 6, 9 and 16).
General characteristics of included studies that evaluating the effect of probiotic and synbiotic supplementation in bone health.
Main results and assessment method of included studies that evaluating the effect of probiotic and synbiotic supplementation in bone health.

Bone volume fractions: BV/TV, Bone marrow density: BMD, Irritable bowel syndrome: IBS, Parathyroid hormone: PTH, Tumour necrosis factor: TNF-α, Interleukin: IL, Interferon: IFN-γ, Collagen type 1 cross-linked C-telopeptide: CTX-1, Bone-specific alkaline phosphatase: BALP, Osteoprotegerin: OPG, Osteocalcin: OC, Calcium: Ca, Weighted mean difference: WMD, Standardized mean difference: SMD.
Supplemental Table 3 shows the overlap between primary studies across included meta-analyses in our umbrella review with a meta-analysis.
3.2. Type, dosage, and duration of probiotics and synbiotics
All studies in this umbrella review used an average probiotic dose of at least 108 CFU/g (colony-forming units per gram), which meets the current standard for effective probiotics necessary for measurable health benefits. They typically report a range of 108 to 1011 CFU, with a concentration of 108 CFU/g often cited as necessary for a clinical effect due to the challenges of surviving the stomach’s acidity.1,2,13
Probiotics administration methods varied in animal studies, including fermented products, dietary supplements, and oral gavage. All human studies tried oral supplements or consumed them in the diet as a component of fermented dairy products (e.g., cheese, yogurt, kefir).3–5 Animal studies in this systematic review tied oral gavage to their trials. The chosen method can significantly affect probiotics’ efficacy by influencing beneficial microbes’ viability and colonization potential.6–8,14
The synbiotics in these studies included bacterial strains along with cheese, yogurt, kefir, isoflavone, calcium, vitamin D3, fructose, galactooligosaccharides, soluble corn fibers, and vitamin K. These components were chosen for their synergistic effects to enhance gut microbiota diversity and overall health.4,9
Treatment durations in animal studies and clinical trials varied from 1 day to 48 weeks. However, most studies used 6 to 12 weeks for intervention duration and suggested that 6 to 12 weeks is often necessary to observe significant effects on bone health in various studies. Billington E’s study suggests that the variability in BMD results and bone turnover markers may stem from the necessity for all studies to last at least six months to capture maximal changes in these markers. 2
Most studies focused on Lactobacillus (L) and Bifidobacterium (B) strains as probiotics, with some also using Bacillus. The most common probiotics studied were L. reuteri, L. casei, L. paracasei, L. plantarum, L. acidophilus, L. helveticus, L. rhamnosus, B. bifidum, B. longum, B. breve, B. infantis, Bacillus subtilis, and Streptococcus thermophilus.1–16 These strains were often evaluated for their ability to survive the digestive tract, adhere to intestinal mucosa, and produce beneficial metabolites like short-chain fatty acids. Lactobacillus species, such as L. reuteri, L. paracasei, and L. plantarum, are well-studied for maintaining balanced gut microbiota, while Bifidobacterium strains like B. bifidum, B. lactis, and B. longum are linked to dietary fiber fermentation and beneficial short-chain fatty acid production.4,9,16 Additionally, Bacillus strains, such as Bacillus coagulans, have gained interest for their spore-forming ability, allowing them to survive harsh gastrointestinal conditions and reach the intestines intact. Together, these microorganisms enhance gut microbiome diversity and promote gut health.5–7,15
3.3. Skeletal parameters
All included studies examined the effects of probiotics and synbiotics on BMD. BMD and bone mineral content (BMC) were assessed by dual-energy X-ray absorptiometry or single-photon absorptiometry. Three systematic reviews found that probiotics and synbiotics significantly increased BMD along with enhanced bone mineral content (BMC) at various sites, including the femur, tibia, hip, and vertebra.6,9,16 In contrast, one systematic review investigated BMD changes, reporting no differences between probiotic and control groups. 2
Eight meta-analyses studies focused on hip and lumbar spine BMD, with four showing a significant impact of probiotics and synbiotics on hip BMD,1,8,10,11 while four did not.3–5,7 In contrast, five studies indicated a significant effect on lumbar BMD,1,3,5,8,10 with three showing no significant impact.4,7 Malmir’s study revealed that probiotics consumption had no effect on spinal BMD or total hip BMD. 4 In Bose’s study, probiotics treatment was found to significantly increase BMD across all sites (total femur, trabecular femur, trabecular tibia, cortical tibia, and vertebra), with the greatest effect noted in total femoral BMD (SMD = 5·24, 95 % CI (3·04, 7·43); P < 0·001). 1 A meta-analysis of rodent studies indicated that probiotics significantly improved femoral and hip BMD (SMD = 0.43, 95% CI [0.13, 0.74], I2 = 3%, p = 0.006), which correlated with increased BV/TV (SMD = 0.63, 95% CI [0.25, 1.02], I2 = 57%, p = 0.001). No significant effects were observed on BV/TV and BMD at the spine (SMD = 0.68, 95% CI [−0.31, 1.67], I2 = 83%, p = 0.18), (SMD = 0.42, 95% CI [−0.01, 0.84], I2 = 61%, p = 0.05). 11
Two meta-analyses indicate that probiotics supplementation significantly improves muscle mass, muscle strength, and handgrip strength in older adults compared to controls.13,15 For instance, Handajani Y et al., (2024), reported significant improvements in muscle mass (SMD = 0.684, 95% CI: 0.002-1.366, p = 0.049), muscle strength (SMD = 1.037, 95% CI: 0.077-1.996, p = 0.03), gait speed (MD [95% CI], 0.10 m/s [0.03-0.16], P = .003; I 2 = 0%) and handgrip strength (MD = 2.50 kg, 95% CI: 1.33-3.66, p < .001, I2 = 0%) with probiotics use. 13 A meta-analysis in sarcopenic patients found no significant difference between probiotics and placebo in muscle mass, handgrip strength, or lean body mass, but did show a significant improvement in global muscle strength with probiotics (MD: 2.99, 95%CI: 2.14–3.85; Z = 6.86, P < 0.001). 12 Similarly, a meta-analysis in osteoarthritis (OA) patients reported that probiotics had no effect on WOMAC scores, including pain, stiffness, or physical function. 14
Additionally, one meta-analysis mentioned that probiotics treatment enhanced bone volume compared to controls, showing notable improvements in bone volume fractions (BV/TV) in ovariectomized animals, particularly in the tibia and vertebra (SMD=2·26, 95 % CI of (0·75, 3·77), P-value=0·003). Also, reported a reduction in bone formation rate (BFR) upon probiotics treatment; however, the effect was not statistically significant (SMD = −0·66, CI (–1·34, 0·02); P = 0·056). On osteoclast surface/bone surface (Oc.S/B.S) data, it was reported that although probiotics treatment tended to reduce Oc. S/B.S, the effect was not statistically significant. 1
Three systematic reviews on human and animal models declared that probiotics feeding also affected an increase in trabecular thickness, bone volume, tibia length, and femur weight, and a significant reduction in trabecular separation. However, no meta-analysis was done on these bone parameters.4,6,9
3.4. Plasma biochemical profile and inflammatory markers
Nine studies reported osteocalcin (OC) levels in intervention and control groups. Results indicated that probiotics and synbiotics treatments tended to increase this bone formation marker significantly. However, six of these articles conducted meta-analyses that found this change was not statistically significant. For example, Zeng’s study found no statistically significant improvement in OC between the experimental and control groups (SMD −0.12 (−0.85, 0.61), P=0.75, random effects model). 5
Nine studies examined serum Collagen cross-linked C-telopeptide (CTX) levels in intervention and control groups, indicating that probiotics and synbiotic treatments may reduce bone resorption by lowering CTX levels. Four meta-analyses were performed; three found a significant decrease in CTX, while Bose’s meta-analysis noted that probiotics treatment modestly lowered serum CTX-1, though the effect was not significant. Yu’s study indicated that probiotics supplements lowered CTX levels compared to the placebo group (SMD = −0.34, 95% CI −0.60 to −0.09), with substantial heterogeneity. 1
Nine studies reported a decrease in serum bone-specific alkaline phosphatase (BALP), but a meta-analysis revealed no significant relationship in three of these studies. Liu’s research indicated no significant differences in BALP levels among participants receiving probiotics, prebiotics, or synbiotics compared to the control group (-−10.64 U/L, 95% CI [−43.67, 22.38], heterogeneity: p = .0010, I2 = 86%). In sensitivity analyses, excluding individual articles showed no significant difference between experimental and control groups (6.94 U/L, 95% CI [−3.97, 17.85], p = .63), (−24.52 U/L, 95% CI [−86.96, 37.92], p = .0004; 22.22 U/L, 95% CI [−90.91, 46.48], p = .0006). 7 The study by Wang mentioned that probiotics supplementation was associated with reduced levels of BALP (SMD = -1.80, 95%CI -2.78 to -0.81). 10
Three studies on the Receptor activator of nuclear factor-kB ligand (RANKL) produced mixed results: one reported significant improvement, 9 while the others found no statistically significant changes.5,10
One systematic review assessed additional resorption markers such as urinary type I collagen cross-linked N-telopeptide (NTX) and type 1 procollagen N-terminal propeptide (P1NP); one study in this systematic review observed a reduction in NTX and an increase in P1NP with probiotics, while the other two found no difference. 2 Also, one meta-analysis of P1NP reported that probiotics did not show any significant alteration. 10
Four studies examined osteoprotegerin (OPG). One systematic review found a significant improvement in this marker, while three meta-analyses reported no association between probiotics and OPG. The study by Zeng indicated that the improvement in OPG in the experimental group was not statistically significant compared to the control group (WMD −0.10 (−1.00, 0.79), P = 0.82, random effects model). 5
Six studies examined serum and urinary calcium levels, revealing that both probiotics and synbiotics increased serum calcium compared to controls, though one meta-analysis found non-significant results. 1 Three other meta-analyses reported increased serum calcium levels and absorption. Malmir’s study indicated that probiotics consumption significantly raised serum calcium levels (weighted mean difference: 3.82 mmol/l; 95% CI: 1.05, 6.59 mmol/l; I-square = 98.0%, P < 0.001) and notably affected urinary calcium levels (WMD: 4.85 mmol/l; 95% CI: 1.16, 8.53 mmol/l; I-square = 97.6%, P < 0.001). 4
Five studies reported parathyroid hormone (PTH) levels with no change (two studies) or a decrease in levels (three studies). Three studies meta-analysed PTH levels; one showed significant decreases, 4 while two reported insignificant changes.7,8 Liu’s analysis found no significant difference in PTH levels between participants receiving probiotics, prebiotics, or synbiotics and the control group (0.71 pg/ml, 95% CI [−7.46, 8.88], heterogeneity: p = .09, I2 = 59%). Conversely, the Malmir study indicated that probiotics consumption significantly reduced PTH levels (WMD: −5.53 ng/l; 95% CI: −9.83, −0.86 ng/l, I2 = 98.2%, P < 0.001). 4
Four studies declared the positive effects of probiotics on tumor necrosis factor-α (TNF-α). One meta-analysis reported no evidence that probiotics supplements were associated with decreased levels of TNF-α. 3
Four studies investigated vitamin D status, while three focused on phosphorus and magnesium. All reported that probiotics and synbiotics elevated these markers, but none performed a meta-analysis on these levels.
Two systematic reviews highlighted significant changes in plasma biochemical profiles, including zonulin, claudin-3, branched-chain amino acids, creatine kinase, butyrylcarnitine, N-terminal telopeptide, tartrate-resistant acid phosphatase, and short-chain fatty acids. It noted a reduction in inflammatory markers such as CRP, IL-1, IL-6, IL-8, and interferon-γ. 9 Additionally, another systematic review reported a significant decrease in specific inflammatory markers like IL-1 and antioxidative parameters. 6
3.5. Results of meta–analysis
3.5.1. The effect of probiotics supplementation on BMD
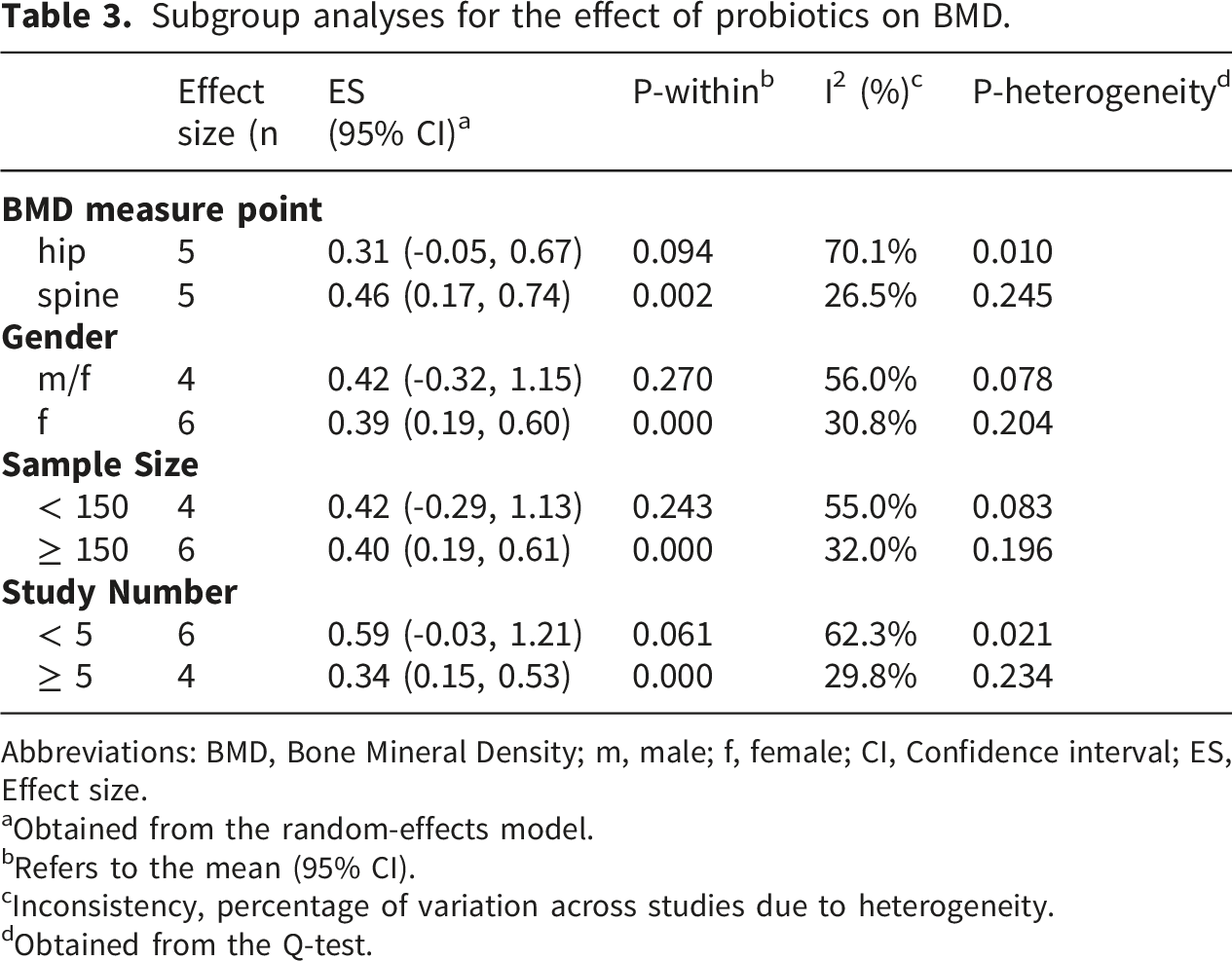
Combining the results of five meta-analyses comprising 10 effect sizes (WMD) indicated that probiotic supplementation significantly increased the BMD levels (WMD= 0.39 (95% CI: 0.14, 0.63), p = 0.002) (Figure 2). There was a high amount of heterogeneity (I2=71.5%, p <0.001) among the studies. After excluding each study using sensitivity analysis, no significant difference in the pooled results was found (Sup Figure 1). Begg’s tests (p = 0.788) indicated there was no minor study effect. Visual inspection of the funnel plot, however, revealed an asymmetry to the right of the funnel plot. Therefore, the trim-and-fill method was applied by 10 meta-analyses (five imputed by test), and the effects of probiotics on BMD levels became statistically non-significant after a minor decrease in ES magnitude (WMD: 0.232 (95% CI: -0.018, 0.481)). The subgroup analysis results indicated that probiotic supplementation had a positive effect on spine BMD (p 0.002). Also, a greater positive effect on BMD was observed in studies that included only females (p <0.001). Similarly, a greater positive effect on BMD was seen in studies with a sample size of ≥ 150 and a number of studies of ≥ 5 (Table 3). These exploratory findings should be interpreted with caution and require confirmation in future studies designed a priori to test subgroup effects. (a) Forest plot detailing effect sizes and 95% confidence intervals (CIs) and (b) funnel plot of the effect of probiotics supplementation on BMD. Subgroup analyses for the effect of probiotics on BMD. Abbreviations: BMD, Bone Mineral Density; m, male; f, female; CI, Confidence interval; ES, Effect size. aObtained from the random-effects model. bRefers to the mean (95% CI). cInconsistency, percentage of variation across studies due to heterogeneity. dObtained from the Q-test.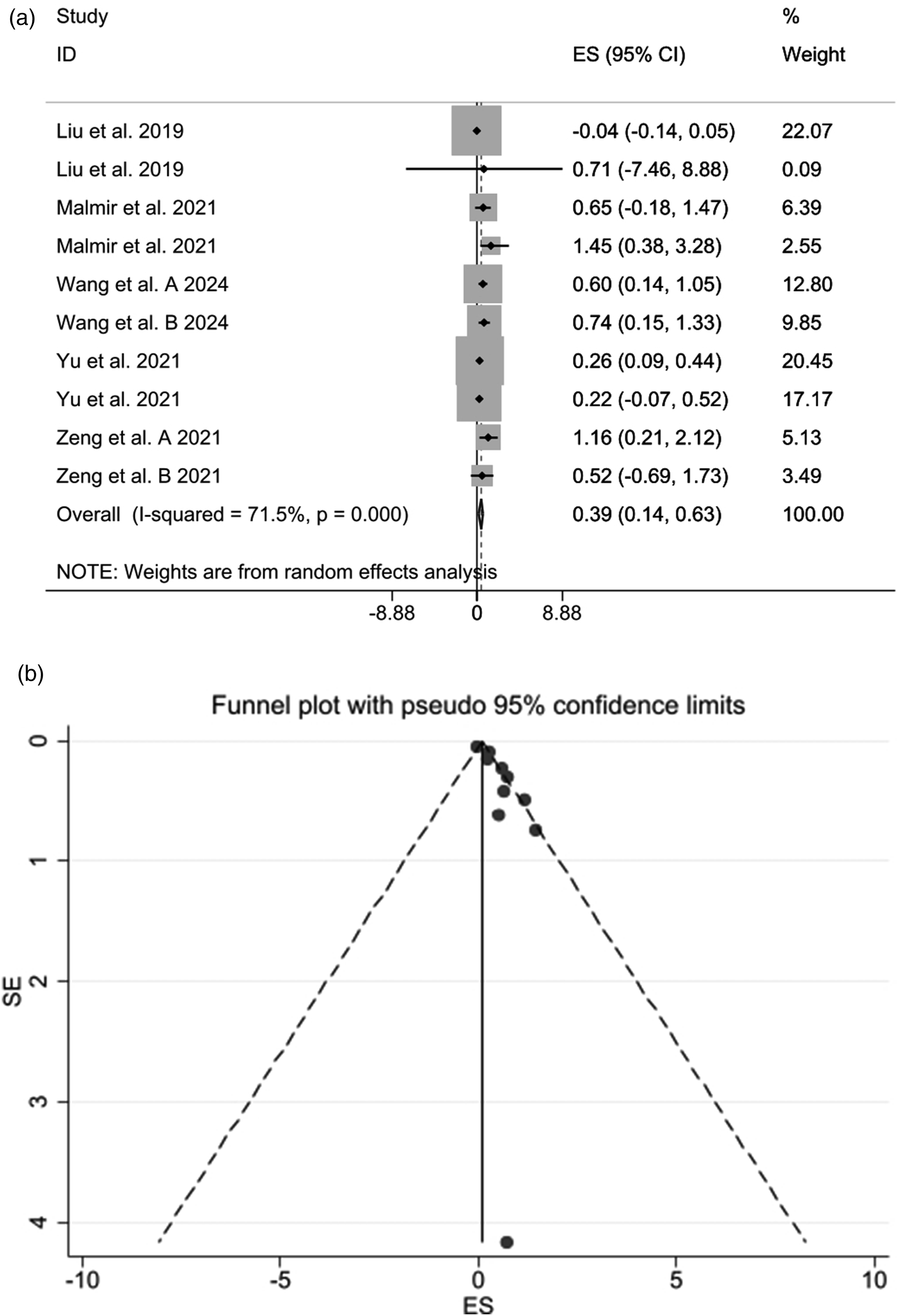
3.5.2. The effect of probiotic supplementation on muscle strength
The pooled estimate of three meta-analyses of clinical trials reported a significant effect of probiotic supplementation on improving MS of participants (WMD = 1.99 (95% CI: 0.42, 3.57), p = 0.013) (Figure 3). The heterogeneity test results (I2 = 87.0%, p = <0.001) revealed that there was high heterogeneity among meta-analyses. The overall effects of probiotic intervention on MS became nonsignificant following the removal of wang et al. (WMD = 1.466, 95%CI: -.502, 3.435) and Besora-Menore et al. (WMD = 1.749, 95%CI: -.700, 4.199) using sensitivity analysis (Sup Figure 2). Based on the Begg test results (p = 0.602), no significant publication bias was observed. (a) Forest plot detailing effect sizes and 95% confidence intervals (CIs) and (b) funnel plot of the effect of probiotics supplementation on MS.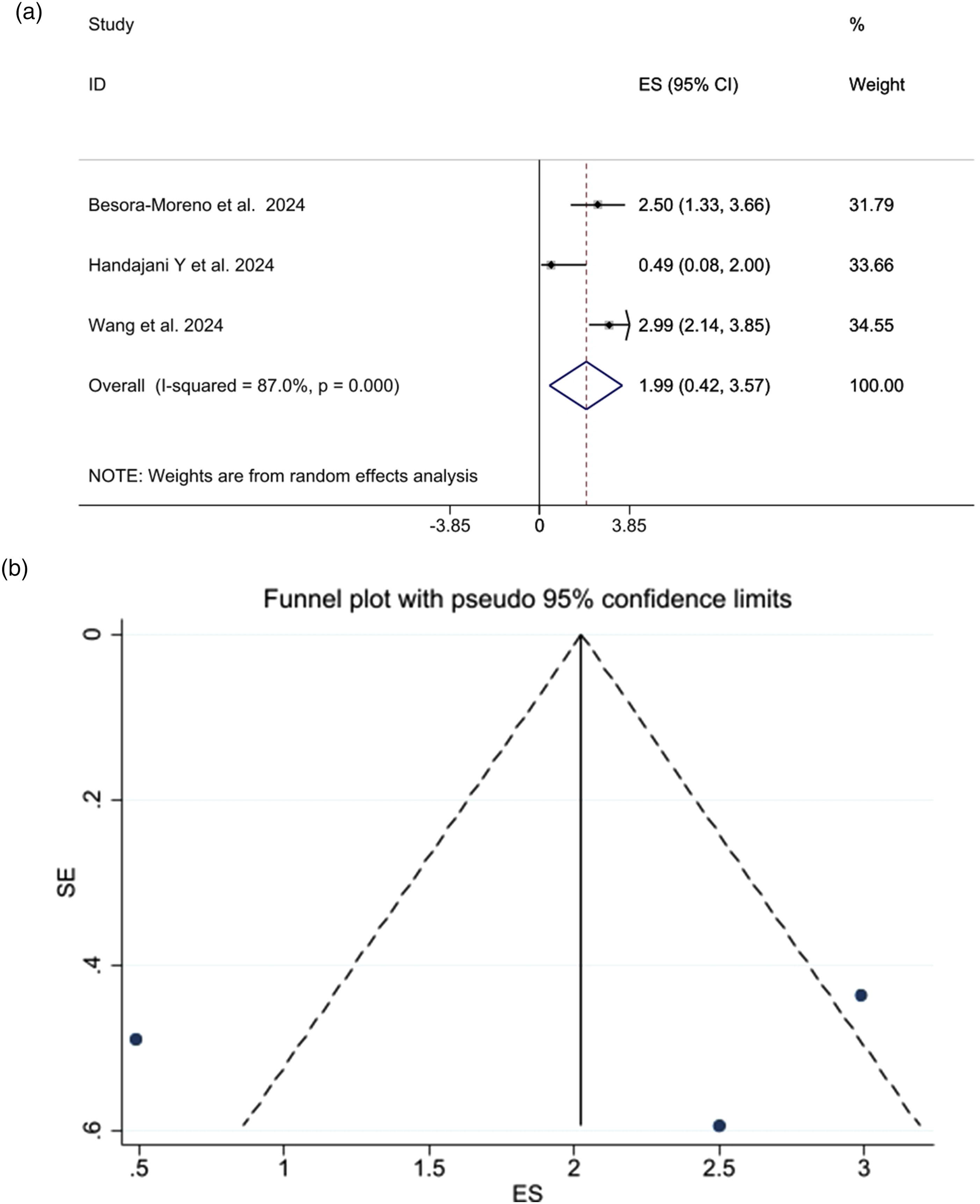
3.5.3. The effect of probiotic supplementation on muscle mass
Two meta-analyses evaluated the effects of probiotic supplementation on MM. The pooled results from these studies indicated that MM was significantly enhanced after probiotic supplementation (WMD = 0.46, 95% CI 0.23, 0.68), p = <0.001 (Figure 4). The heterogeneity test results (I2= 0.0%, p = 0.740) revealed that there was probably low heterogeneity among studies. Forest plot detailing effect sizes and 95% confidence intervals (CIs) of the effect of probiotics supplementation on MM.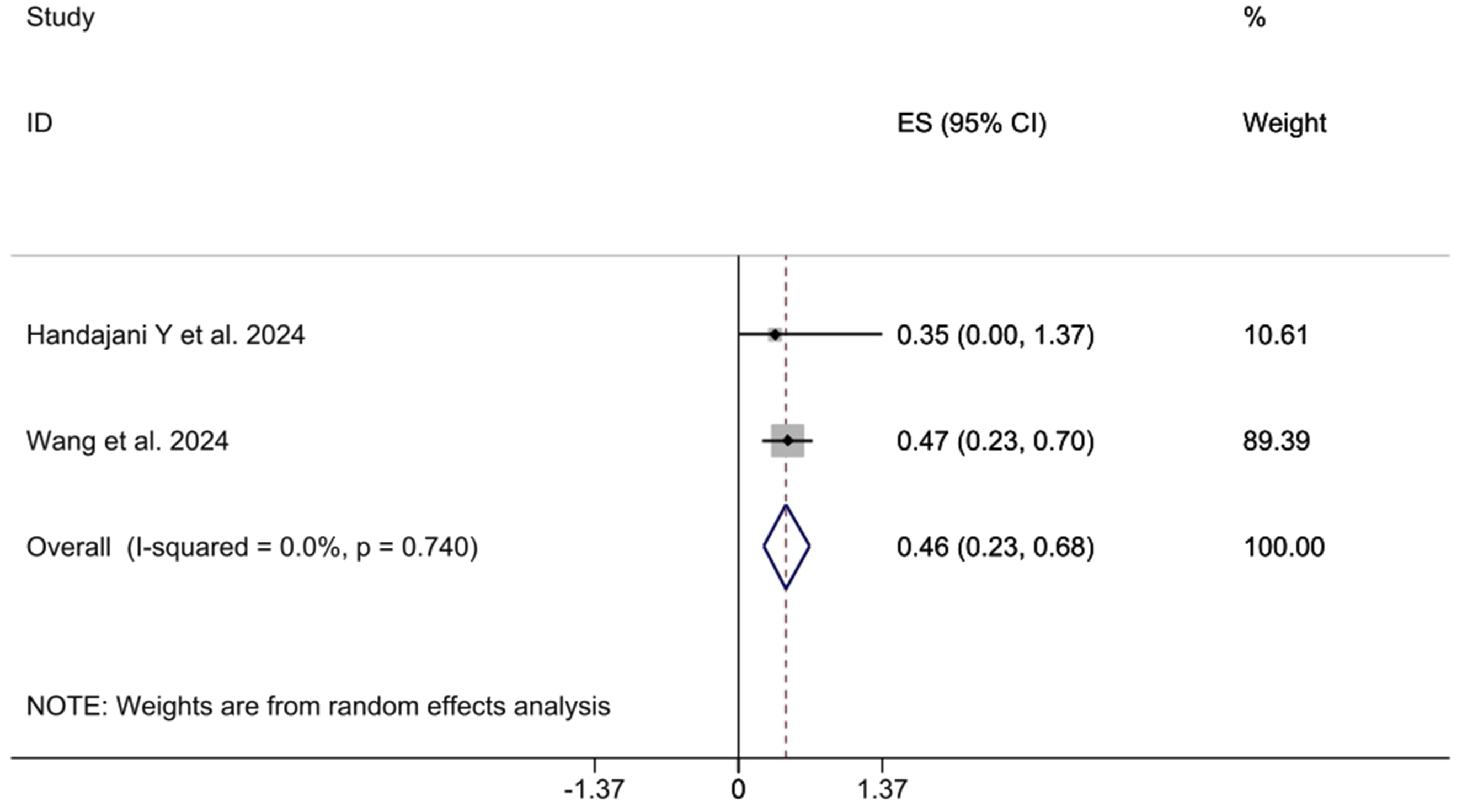
3.6. Quality assessment of the included studies
The methodological quality of the 16 included systematic reviews was assessed using the AMSTAR2 tool. Following official guidance, we did not calculate a numerical overall score. Instead, two reviewers independently assigned each review an overall confidence rating of high, moderate, low, or critically low based on failures in seven critical domains (items 2, 4, 7, 9, 11, 13, and 15).
Overall confidence ratings: High confidence – 11 reviews,1,3,4,7,8,10–15 Moderate confidence – 1 review, 5 Low confidence – 4 reviews,2,6,9,16 Critically low confidence – 0 reviews.
Results of assessment of the methodological quality of included meta-analysis.
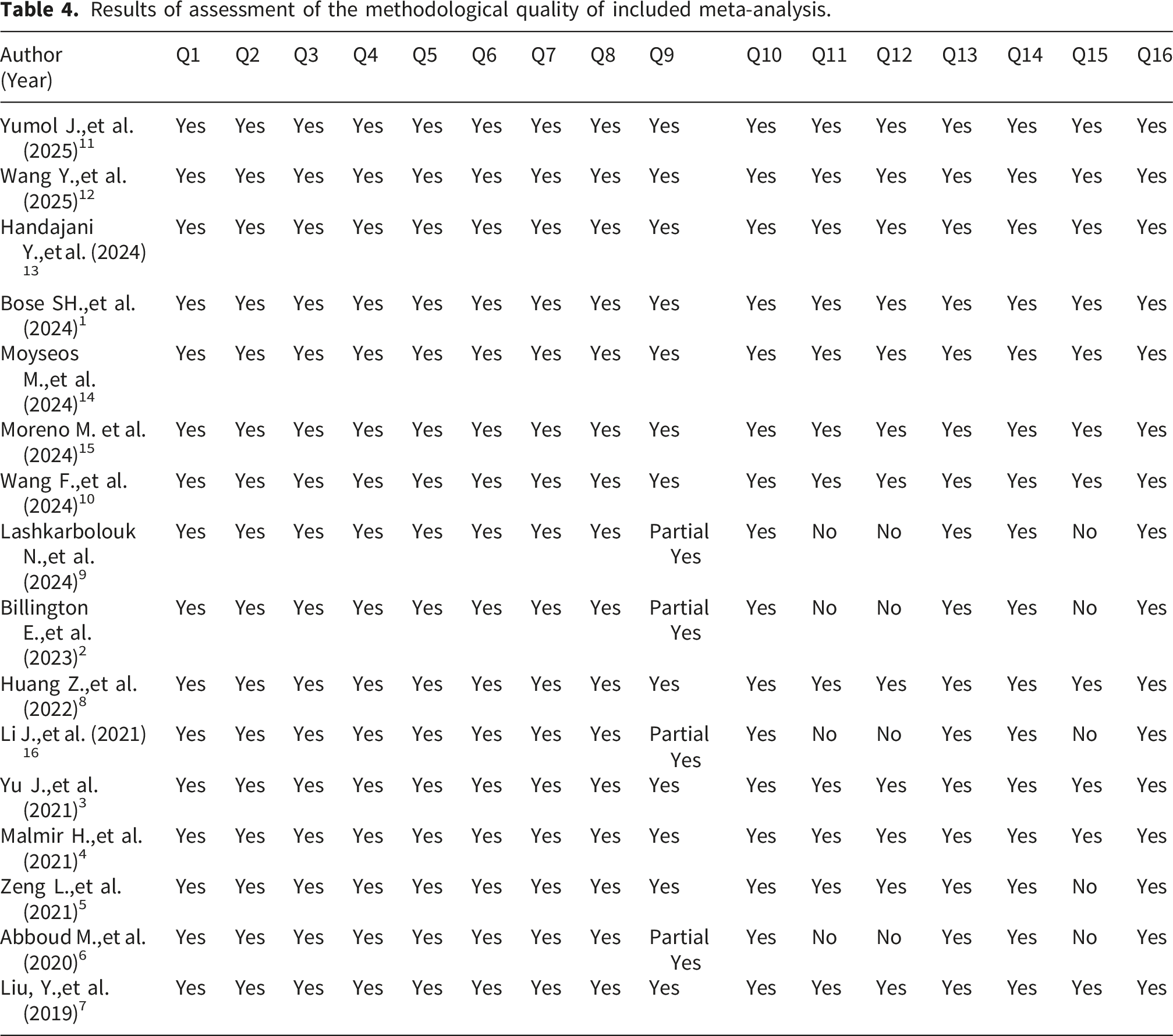
Most common critical-domain failures among moderate- and low-confidence reviews: 1. Item 11 (appropriateness of meta-analytic methods) – rated “No” in 4 reviews,2,6,9,16 all of which were systematic reviews without a quantitative synthesis or with inappropriate pooling. 2. Item 15 (assessment of publication bias) – rated “No” in 5 reviews.2,5,6,9,16 3. Item 9 (adequacy of risk-of-bias assessment) – rated “Partial Yes” in 4 reviews,2,6,9,16 indicating that a risk-of-bias tool was used but applied incompletely or not reported in sufficient detail.
No review failed the other critical domains (items 2, 4, 7, 13), meaning that all 16 reviews had a registered protocol (or justified its absence), performed an adequate literature search, justified study exclusions, and considered risk of bias when interpreting results.
4. Discussion
Osteoporosis and osteopenia primarily affect older adults, reducing their resilience to physical stress. As the global population ages, the rising prevalence of osteoporosis presents significant challenges. Bone density loss increases fracture risk, leads to prolonged disability, increases the health costs, and diminishes quality of life.3,5,8 Probiotics and synbiotics have been proposed as potential adjunctive interventions, but the strength and consistency of the supporting evidence require careful scrutiny. Dysbiosis may increase intestinal permeability, promoting the translocation of pro-inflammatory cytokines that can harm bone tissue. GM is involved in vitamin synthesis, lipid metabolism, and immune regulation.11–13 Animal studies show that metabolites such as short-chain fatty acids (SCFAs), particularly butyrate, can influence osteoblast and osteoclast activity.29–31 However, these mechanistic data come mainly from rodent models or in vitro experiments. Their translation into clinical benefits in humans remains incompletely established.
In this umbrella meta-analysis of human studies, probiotic supplementation significantly increased BMD in the pooled analysis (ES = 0.39 [0.14–0.63], p = 0.002). Nevertheless, this finding must be interpreted with substantial caution for several reasons. First, visual inspection of the funnel plot showed asymmetry, and after trim-and-fill correction (imputing five missing studies), the effect size became non-significant (ES = 0.23 [0.018–0.481]). Second, there is high heterogeneity: I2 = 71.5% (p < 0.001), indicating that the true effect varies considerably across studies and settings; heterogeneity was only partially explained by BMD measurement site, sample size, and participant sex. Third, positive effects were more consistently observed at the lumbar spine (five meta-analyses showing significant effects) than at the hip (four meta-analyses positive, four null), suggesting that probiotics, if effective, may preferentially influence trabecular-rich sites. Fourth, the pooled effect on muscle strength (ES = 1.99 [0.42–3.57], p = 0.013) became non-significant after its removal in sensitivity analyses (Supplemental Figure 2), indicating that the result is not robust to the exclusion of a single study. Thus, the overall human evidence for probiotics improving BMD or muscle strength is suggestive but not robust. It does not support strong clinical recommendations or claims of causality (Figure 5). Graphical abstracts of the study.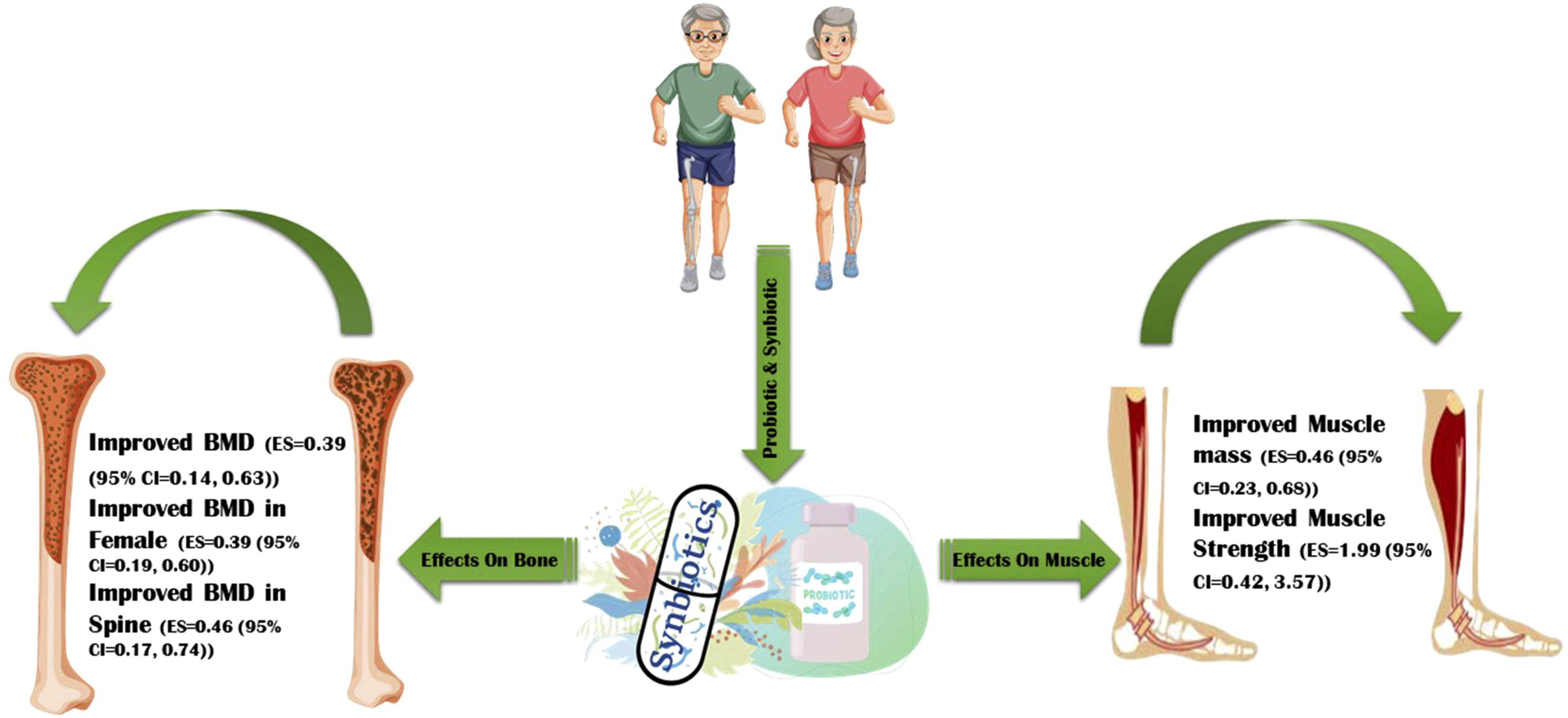
4.1 Type, dosage, and duration of supplementation (human studies)
Most included studies used Lactobacillus and Bifidobacterium strains at doses of 108–1011 CFU/g. The minimum dose of 108 CFU/g is commonly cited as necessary to survive gastric transit, but direct dose-response evidence for bone outcomes is lacking.15,16,32 Intervention durations varied from 6 to 48 weeks. While some systematic reviews suggested that longer durations (≥6 months) are associated with more positive BMD changes,2,3,9 this observation is based on cross-study comparisons, not within-trial randomization.
4.2 Musculoskeletal parameters: Inconsistent across skeletal sites
Our synthesis shows that probiotics and synbiotics may have a modest positive effect on lumbar spine BMD in some meta-analyses1,3,5,8,10 but not in other sites.4,7 Hip BMD effects are even less consistent, with as many null as positive meta-analyses. This discrepancy may reflect differences in bone composition (trabecular vs. cortical), turnover rates, or mechanical loading. At present, the evidence does not support a claim that probiotics improve BMD at all skeletal sites. Pooled estimates showed significant improvements in muscle mass (ES = 0.46 [0.23–0.68], I2 = 0%) and strength (ES = 1.99 [0.42–3.57], I2 = 87%). However, the high heterogeneity for strength and its sensitivity to single-study exclusion limit confidence. Moreover, a meta-analysis in sarcopenic patients found no significant difference in muscle mass or handgrip strength, although global muscle strength improved. 12 In osteoarthritis patients, probiotics had no effect on physical function. 14 Collectively, the evidence for muscle outcomes is mixed and not robust.
4.3. Plasma biochemical profile and inflammatory markers
Despite plausible mechanisms, most bone turnover markers did not show statistically significant meta-analytic changes (osteocalcin, BALP, OPG and RANKL). Two meta-analyses showed no significant change in PTH level7,8; one showed a significant reduction, but with very high heterogeneity (I2 = 98.2%). 4 Three out of four meta-analyses showed a significant decrease in CTX, but heterogeneity was substantial.1,3,10 Calcium levels were increased in most meta-analyses, but this may be confounded by the calcium content of fermented dairy products used as delivery vehicles.5–9 Inflammatory markers (TNF-α, CRP, IL-6) showed some reductions, but not uniformly across studies. The lack of consistent effects on bone turnover markers, despite occasional BMD changes, raises questions about the clinical meaningfulness of the BMD findings. It is possible that the small BMD effect size (ES = 0.39) is below the detection threshold of these markers, or that the markers were measured at inappropriate time points.
Why effects may be absent or inconsistent: slow bone remodeling is one factor, as most trials lasted only 6–12 weeks whereas measurable BMD changes typically require at least six months, 2 meaning short-term studies are unlikely to capture true effects. Regarding the target population, probiotics may only benefit individuals with low baseline BMD, inadequate calcium or vitamin D intake, or known gut dysbiosis, while studies enrolling healthy, replete populations may show ceiling effects. Concomitant medications are also relevant because many older adults take calcium, vitamin D, bisphosphonates, or other drugs that could obscure or interact with probiotic effects. Biomarker variability plays a role: bone turnover markers have high biological variability (diurnal, dietary, assay-dependent), and single time-point measurements in small samples may fail to detect true but small changes.33–37 Strain specificity matters because not all probiotic strains are equally effective; most studies used Lactobacillus and Bifidobacterium, but within these genera effects may differ, yet no head-to-head strain comparisons exist for bone outcomes. High heterogeneity (I2 often >70%) was present for BMD and muscle strength, and this heterogeneity is not merely a statistical nuisance – it reflects genuine variation in study populations, interventions, comparator groups, outcome measurements, and follow-up durations. Consequently, any pooled estimate must be viewed as an average that may not apply to any specific clinical setting. Subgroup analyses (e.g., by BMD site, sample size, gender) were exploratory and not pre-specified in most original meta-analyses; they should be interpreted as hypothesis-generating, not confirmatory.32,38–41 For example, the observation that Asian studies showed a larger effect than European studies 12 was based on post-hoc comparisons with high subgroup heterogeneity (I2 = 76%). This could reflect differences in diet, baseline calcium intake, or probiotic strains, but it may also be a spurious finding, and we refrain from interpreting it as a true geographical effect. In addition to the limitations noted above (heterogeneity, publication bias, fragility of results), the following limitations warrant emphasis: although low (Supplemental Table 3), some degree of overlap across included meta-analyses cannot be ruled out, which may introduce bias through double-counting of original trials. We did not apply GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) to individual outcomes; doing so would likely rate the evidence as low or very low for most outcomes due to high heterogeneity, imprecision, and publication bias. There is an inability to adjust for multiple comparisons, as subgroup analyses and multiple outcome testing increase the risk of type I errors, so our conclusions should be viewed as exploratory. Finally, the lack of individual patient data meant we could not assess effect modification by age, sex, baseline BMD, or probiotic strain at the individual level. In summary, the available human evidence suggests modest, inconsistent, and fragile benefits of probiotics and synbiotics on bone mineral density (primarily lumbar spine) and muscle strength, but these effects are not robust to correction for publication bias or sensitivity analyses. Bone turnover markers and hip BMD show no consistent improvements. Mechanistic plausibility is supported by animal studies, but translation to clinical efficacy remains unproven.42–47 Current evidence does not support routine prescription of probiotics or synbiotics for the prevention or treatment of osteoporosis or sarcopenia.48–50 They may be considered as part of a broader dietary approach (e.g., fermented dairy intake), but should not replace established therapies (calcium, vitamin D, bisphosphonates, exercise). Large, well-designed, long-duration (≥12 months) randomized controlled trials are needed, with pre-specified subgroup analyses, standardized probiotic strains and doses, and fracture as a primary endpoint. Mechanistic studies should measure gut microbiota composition and turnover markers longitudinally.
It should be noted that, because the number of contributing meta-analyses/effect sizes was limited, formal assessments of funnel plot asymmetry and small-study effects were considered exploratory and interpreted cautiously. Begg’s test has limited statistical power in analyses with few studies, and funnel plot asymmetry should not be interpreted as definitive evidence of publication bias. In addition, the trim-and-fill procedure was used only as a sensitivity analysis to evaluate the potential influence of potentially missing studies on pooled estimates.
Also,we have avoided strong or definitive conclusions regarding muscle outcomes, and instead state that these findings should be interpreted with great caution and require confirmation in future larger meta-analyses.
5. Conclusion
This umbrella review found that probiotic and synbiotic supplementation was associated with modest, statistically significant benefits for BMD in human studies, although substantial heterogeneity and a trim-and-fill sensitivity analysis that rendered the pooled effect non-significant indicate low to moderate certainty in this estimate. Muscle mass and strength outcomes were derived from very few meta-analyses, with high heterogeneity and sensitivity analyses that eliminated statistical significance; these findings should therefore be considered exploratory and preliminary. Animal studies provide mechanistic plausibility (e.g., modulation of gut microbiota, inflammation, and mineral absorption) but cannot be generalized to human clinical efficacy. The evidence is further limited by overlap among primary studies across the included systematic reviews, variation in methodological quality (AMSTAR2 confidence ratings: 11 high, 5 moderate/low), and the absence of long-term fracture outcomes. Future research should prioritize large, long-term randomized controlled trials with fracture endpoints, standardized probiotic strains and doses, and clear separation of probiotic-only from synbiotic interventions (the latter of which may contain calcium, vitamin D, or prebiotics that independently affect bone). Until such evidence emerges, clinical recommendations remain unsupported.
Supplemental material
Supplemental material - The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis
Supplemental material for The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis by Mahdi Mazandarani, Narges Lashkarbolouk, Hanieh-Sadat Ejtahed, Azadeh Dehghani, Roghayeh Molani-Gol, Shirin Hasani-Ranjbar and Bagher Larijani in Sage Open Medicine.
Supplemental material
Supplemental material - The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis
Supplemental material for The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis by Mahdi Mazandarani, Narges Lashkarbolouk, Hanieh-Sadat Ejtahed, Azadeh Dehghani, Roghayeh Molani-Gol, Shirin Hasani-Ranjbar and Bagher Larijani in Sage Open Medicine.
Supplemental material
Supplemental material - The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis
Supplemental material for The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis by Mahdi Mazandarani, Narges Lashkarbolouk, Hanieh-Sadat Ejtahed, Azadeh Dehghani, Roghayeh Molani-Gol, Shirin Hasani-Ranjbar and Bagher Larijani in Sage Open Medicine.
Supplemental material
Supplemental material - The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis
Supplemental material for The impact of probiotics and synbiotics supplementation on bone health; an umbrella review of systematic reviews and meta-analysis by Mahdi Mazandarani, Narges Lashkarbolouk, Hanieh-Sadat Ejtahed, Azadeh Dehghani, Roghayeh Molani-Gol, Shirin Hasani-Ranjbar and Bagher Larijani in Sage Open Medicine.
Footnotes
Ethical considerations
This article does not contain any studies with human participants or animals performed by any of the authors.
Author Contributions
M.M, N.L and H-SE came up with the idea for this article and did the final proofreading. MM, NL, and H-SE undertook the study search and evaluated the articles. NL and MM wrote the manuscript and the tables. A.D, RM did the meta-analysis. SHR and BL supervised the process. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in supplementary information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.