
Abstract
Introduction
Mechanical ventilation is an essential lifesaving intervention for patients with severe illness. Mortality among patients receiving mechanical ventilation is high in low-resource settings, including Ethiopia. Evidence on predictors of time to death in such settings is limited. Therefore, this study aimed to assess time to death and its predictors among adult patients receiving mechanical ventilation in intensive care unit at Hiwot Fana comprehensive specialized Hospital, Eastern Ethiopia.
Method
An institution-based retrospective cohort study was conducted among 586 mechanically ventilated adult patients. Data were collected using structured checklist. Time to event analysis was performed using cox proportional hazards model to identify predictors of time to death. The proportional hazard assumption was assessed using schoenfeld residuals. Adjusted hazard ratios with 95% confidence interval were used to quantify associations.
Results
The incidence density of mortality was 6.74 per 100 person-days observations (95% CI: 5.92-7.68). Factors associated with a higher hazards of death included platelet count less than 150,000*106/L (Adjusted Hazard Ratio (AHR)=1.74, 95% CI: 1.26–2.40), cardiovascular failure during mechanical ventilation (AHR=1.62, 95% CI: 1.08–2.43), cardiopulmonary resuscitation (AHR=2.36, 95% CI: 1.71–3.31), vasopressor use (AHR=2.94, 95% CI: 2.02–4.27), and higher fraction of inspired oxygen at initiation of mechanical ventilation (AHR=1.01, 95% CI: 1.007-1.019) had higher risk of death. Gastrostomy was associated wit lower hazard of death (AHR=0.35, 95% CI: 0.18-0.68).
Conclusion
Several clinical and treatment related factors were associated with time to death among mechanically ventilated Intensive Care Unit (ICU) patients. Close monitoring and appropriate management of high risk patients are essential needed.
Introduction
Mechanical ventilation (MV) is critical lifesaving intervention widely used in Intensive Care Units (ICU) to support patients with severe and life threatening conditions. 1 Despite substantial advances in critical care medicine over recent decades, ICU mortality remains a major global public health concern. 2 A considerable proportion of critically ill patients depend on MV for survival, with studies indicating that up to 70% of ICU admissions require ventilatory support at some point during their stay.3–5 However, the use of MV is also associated with increased risk of complications and mortality, making outcomes among these patients a key indicator of ICU performance. 6
Globally, mortality among mechanically ventilated patients in ICUs varies widely, ranging from 20.3% to 77.2% depending on patient characteristics, healthcare settings, and resource availability.7,8 Although some improvements have been observed over time for instance, a decline in ICU mortality from 31% in 1998 to 28% in 2010 these gains are not uniformly distributed. 7 In low and middle-income countries (LMICs), including those in sub-Saharan Africa, mortality rates remain disproportionately high. 9 This disparity is often attributed to delayed healthcare-seeking behavior, limited access to advanced care, inadequate ICU infrastructure, and shortages of trained personnel and essential medical supplies.1,10
Evidence from sub-Saharan Africa shows substantial variability in ICU mortality among mechanically ventilated patients, ranging from 24.4% in South Africa to over 60% in countries such as Nigeria, Kenya, and Rwanda, with Ethiopia reporting rates between 29.6% and 62.2%.9,11–13 Such variation highlights the influence of contextual factors, including differences in ICU capacity, patient case-mix, and clinical management practices.3,14
Beyond overall mortality, understanding when deaths occur during ICU stay is equally important. Previous studies indicate that mechanically ventilated patients often experience short survival durations, with median time to death ranging from 13 to 16 days in Ethiopian settings.13,15 Moreover, patients on MV have been shown to have significantly higher hazards of death compared to non-ventilated patients.16,17 Several predictors of mortality have been identified, including advanced age, low body mass index, severity of illness (e.g., APACHE II score), presence of comorbidities, sepsis, low Glasgow Coma Scale (GCS), need for vasopressors, and ICU-related complications.18–20
However, most existing studies particularly in Ethiopia primarily report proportions of mortality without adequately accounting for the timing of death and censoring of observations. This limits the ability to fully understand patient survival patterns and may lead to incomplete or biased conclusions. Time-to-event (survival) analysis provides a more robust approach by incorporating both the occurrence and timing of death, allowing for better estimation of survival probabilities and identification of predictors influencing the hazard of death over time.
In Ethiopia, available studies on mechanically ventilated ICU patients are limited in scope, often restricted to specific populations, short follow-up periods, or single outcome measures such as mortality proportion.15,21 Furthermore, there is limited evidence focusing specifically on predictors of time to death among mechanically ventilated patients, particularly in eastern Ethiopia. This represents an important gap in the literature, as understanding survival dynamics is essential for improving clinical decision-making, resource allocation, and patient management in resource-limited settings.
Therefore, this study aims to assess the time to death and its predictors among adult ICU patients receiving mechanical ventilation at Hiwot Fana Comprehensive Specialized Hospital (HFCSH) in Harar, eastern Ethiopia. By applying survival analysis techniques, this study seeks to provide more comprehensive evidence that can inform targeted interventions, optimize patient care, and ultimately improve ICU outcomes in low-resource settings.
Methods and materials
Study setting and period
The study was carried out in HFCSH, located in Harar town, Eastern Ethiopia approxiamately 526 Km from Addis Ababa. Harari Regional State has an estimated population of 283,000 with an approximately equal male to female ratio. There are two public hospitals, two private hospitals, and one federal police hospitals in the region. The study was carried out from November 1 to November 30, 2024. The follow-up period for the cohort extended from January 1, 2019, to December 31, 2023.
Study design
A hospital-based retrospective cohort study design was employed to assess time to death and its predictors among mechanically ventilated adult ICU patients.
Source population
All adult patients admitted to the ICU and managed with mechanical ventilation at HFCSH between January 1, 2019, and December 31, 2023 were source popuation.
Study population
Selected adult ICU patients on mechanical ventilation whose medical records met inclusion criteria forms study population.
Inclusion criteria
Adult patients aged 18 years and above, patients who received mechanical ventilation in ICU were included.
Exclusion criteria
Charts with missing or unclear key dates (admission, ventilation initiation, or outcome) and incomplete records lacking critical variables were excluded from the study.
Sample size determination
The sample size was determined using Schoenfeld’s formula for survival analysis under the Cox proportional hazards model. A 95% confidence level (Zα/2 = 1.96) and 80% power (Zβ = 0.84) were assumed. The probability of event (death) was taken as 62.2% from a previous Ethiopian study conducted among mechanically ventilated patients 22 : Since previously reported hazard ratios in similar studies vary and are often large, a more conservative effect size (HR = 1.36) was assumed to ensure adequate power to detect modest associations. Equal allocation between exposure groups (ρ = 0.5) was assumed.
Using the Schoenfeld formula for Cox proportional hazards models:

Sampling technique
A sampling frame was constructed from ICU admission records of patients who received mechanical ventilation during the study period. Since the number of eligible patients exceeded logistical feasibility for full review, simple random sampling was applied using computer-generated random numbers to ensure representativeness and minimize selection bias.
Data collection methods
Structured and pretested data extraction format (that was developed from review of literatures18,22–26 was used for data collection (Appendix A). In this study, two BSc Holder data collectors and one Master degree holder supervisor was participated. One day training was given about the tool. Then, the data collectors were deployed to the data collection after we agreed on the tool. The primary investigator of the study and the supervisor was following the data collection process critically to minimize data errors.
Medical record numbers was collected from admission-discharge registration books of HFCSH ICU Wards and based on that those selected sampling unit, individual patient folders data was collected as per checklists.
Study variables
The Dependent variable for this study was time to death among mechanically ventilated patients. Independent variables included sociodemographic characteristics (age, body mass index), clinical-related predictors (cause of mechanical ventilation initiation such as ARDS, COPD, septic shock, diabetes mellitus (DM), pneumonia, sepsis, neurological failure, hepatic failure, renal failure, hypotension, and cardiovascular conditions; and diagnoses developed during mechanical ventilation such as ventilator-associated pneumonia (VAP), ARDS, COPD, septic shock, diabetes mellitus, sepsis, and cardiovascular failure), and management-related predictors (tracheostomy, vasopressor use, neuromuscular blocking agents, haemodialysis, cardiopulmonary resuscitation, and systemic corticosteroid use). To account for baseline illness severity, additional clinical indicators such as Glasgow Coma Scale 27 and vital sign were included as proxy measures of patient severity.
Operational definition
Data quality control
To control data quality the data retrieval form was pre-tested on 5 % of total sample in Jugal Hospital. This was conducted in another hospital to evaluate the clarity, completeness, and consistency of the data extraction tool, as well as the availability of required variables in routine medical records, while avoiding contamination of the actual study sample. Based on the findings of pre-test some modification was done for the tools. The review was conducted by trained data collectors. Two days intensive training was given to data collectors and supervisors about the purpose, study tool and an overall data collection procedure. The supervisor had checked the completeness and consistency of the filled data retrieval immediately before submission. Manual checks were done for completeness during data collection. Range and consistency was also been checked during entry of data. In addition, double data entry was done by two data clerk and checked for validation by the principal investigator of the research following data entry.
Data analysis
Data were collected using Kobo Toolbox, checked for completeness, and processed using Microsoft Excel and Stata version 17. Descriptive statistics, including means (±SD), medians, Inter Quartile Range (IQR), and proportions, were used to summarize continuous and categorical variables as appropriate. The primary outcome was time to death among mechanically ventilated patients, measured in days from initiation of mechanical ventilation to the occurrence of death or censoring (e.g., recovery, transfer, or end of follow-up). Survival experience was described using Kaplan–Meier survival curves, and differences between groups were compared using the log-rank test. The incidence density rate was calculated per 100 person-days of observation.
Both bivariable and multivariable Cox proportional hazards regression models were fitted to identify predictors of time to death. Variables were selected for multivariable analysis based on a combination of statistical criteria (p-value <0.25 in bivariable analysis) and clinical relevance informed by prior literature and subject-matter knowledge. A purposeful selection approach was employed to ensure inclusion of potential confounders regardless of their bivariable significance.
The proportional hazards assumption was assessed using Schoenfeld residuals and the global test (χ2 = 11.38, p = 0.9358), indicating no violation of the assumption. Additionally, graphical methods (e.g., log-minus-log survival plots) were used to support this assessment. Multicollinearity among independent variables was evaluated using the variance inflation factor (VIF), with a mean VIF <10 indicating no significant multicollinearity.
Model adequacy was assessed using Cox–Snell residuals, and the model was found to fit the data well. Adjusted hazard ratios with 95% confidence intervals were reported to quantify the strength of associations, and statistical significance was declared at a p-value <0.05. The dataset was examined for missing values using frequency distributions and summary statistics. No missing values were identified for the key variables included in the final analysis.Therefore, no imputation or other missing data handling techniques were required.
Results
Socio-demographic characteristics
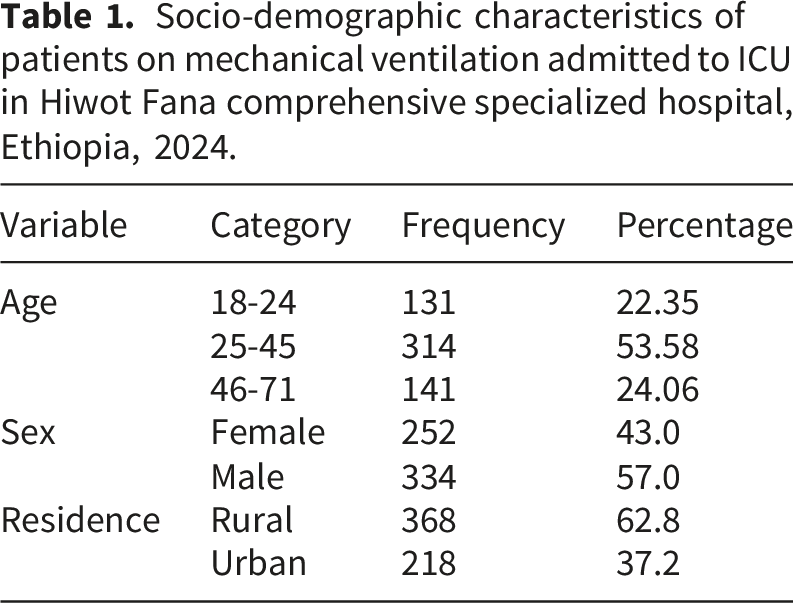
Socio-demographic characteristics of patients on mechanical ventilation admitted to ICU in Hiwot Fana comprehensive specialized hospital, Ethiopia, 2024.
Clinical characteristics
Nearly half of the patients (286, 48.8%) were admitted from the emergency department. Most patients were medical cases (334, 57.0%), while 303 (51.7%) underwent surgical interventions.
Clinical related characteristics of patients on mechanical ventilation admitted to ICU in Hiwot Fana comprehensive specialized hospital, Ethiopia, 2024.
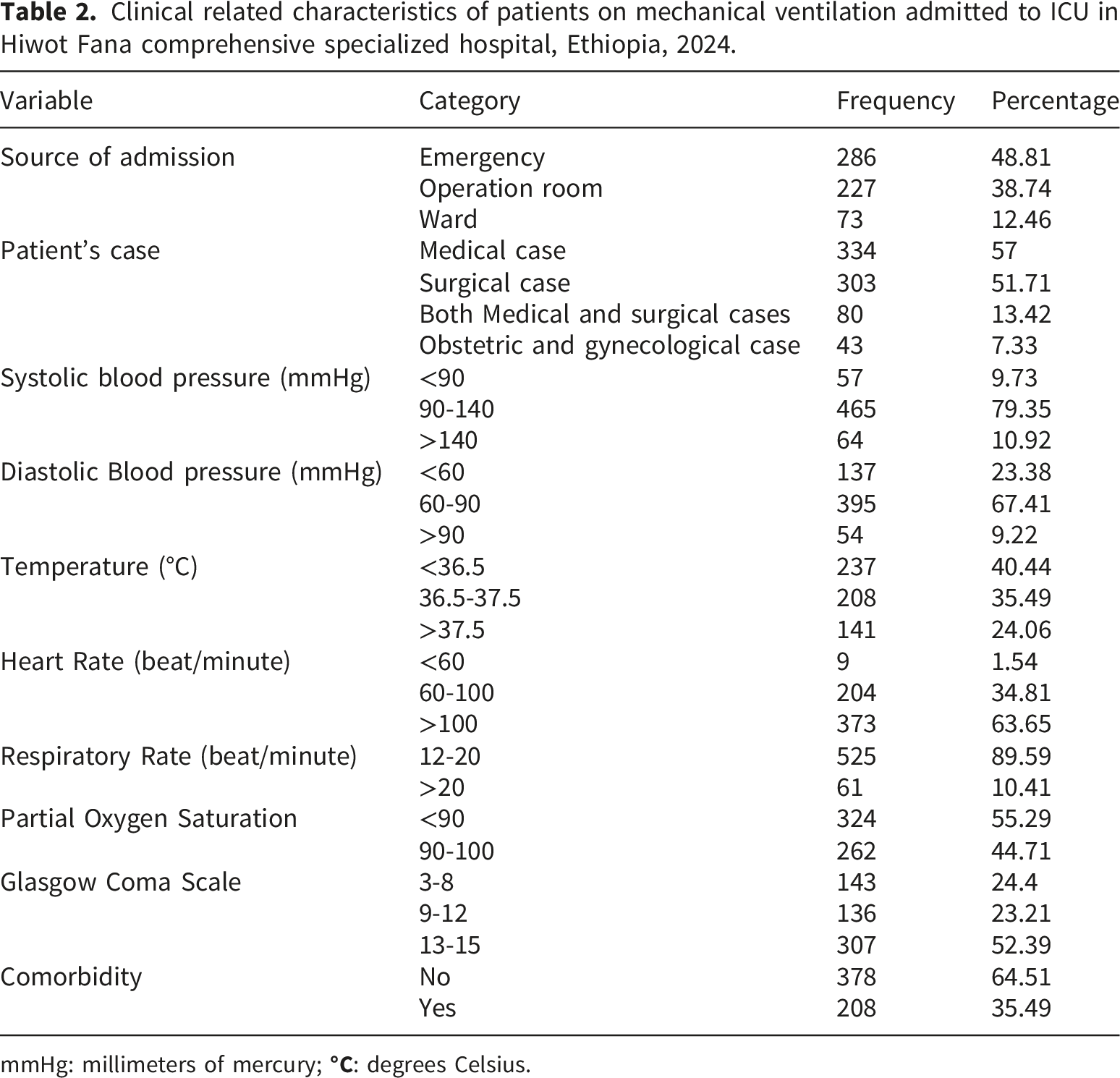
mmHg: millimeters of mercury;
Reasons for mechanical ventilation
Reason of patients on mechanical ventilation admitted to ICU in Hiwot Fana comprehensive specialized hospital, Ethiopia, 2024.
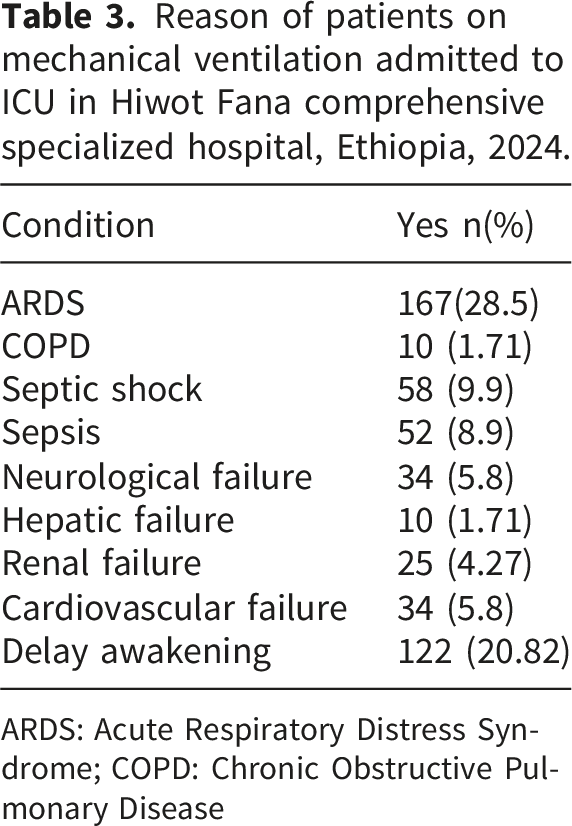
ARDS: Acute Respiratory Distress Syndrome; COPD: Chronic Obstructive Pulmonary Disease
Time to death among mechanically ventilated patients
A total of 586 mechanically ventilated patients were included in the analysis. The overall mortality rate was 38.6%. The median time to death was 9.81 days (95% CI: 8.91–12.86).
Patients were followed for a minimum of 0.27 days and a maximum of 72.98 days, contributing a total of 3,350.67 person-days of observation.
The overall incidence density of mortality was 6.74 per 100 person-days (95% CI: 5.92–7.68).
Kaplan–Meier analysis showed that cumulative mortality increased over time, with probabilities of 12.2% at day 1, 24.7% at day 3, 40.2% at day 6, and 50.6% at day 10 (Figure 1). Overall Kaplan-Meir survival of patients on mechanical ventilation admitted to ICU in Hiwot Fana comprehensive specialized hospital, Ethiopia, 2024.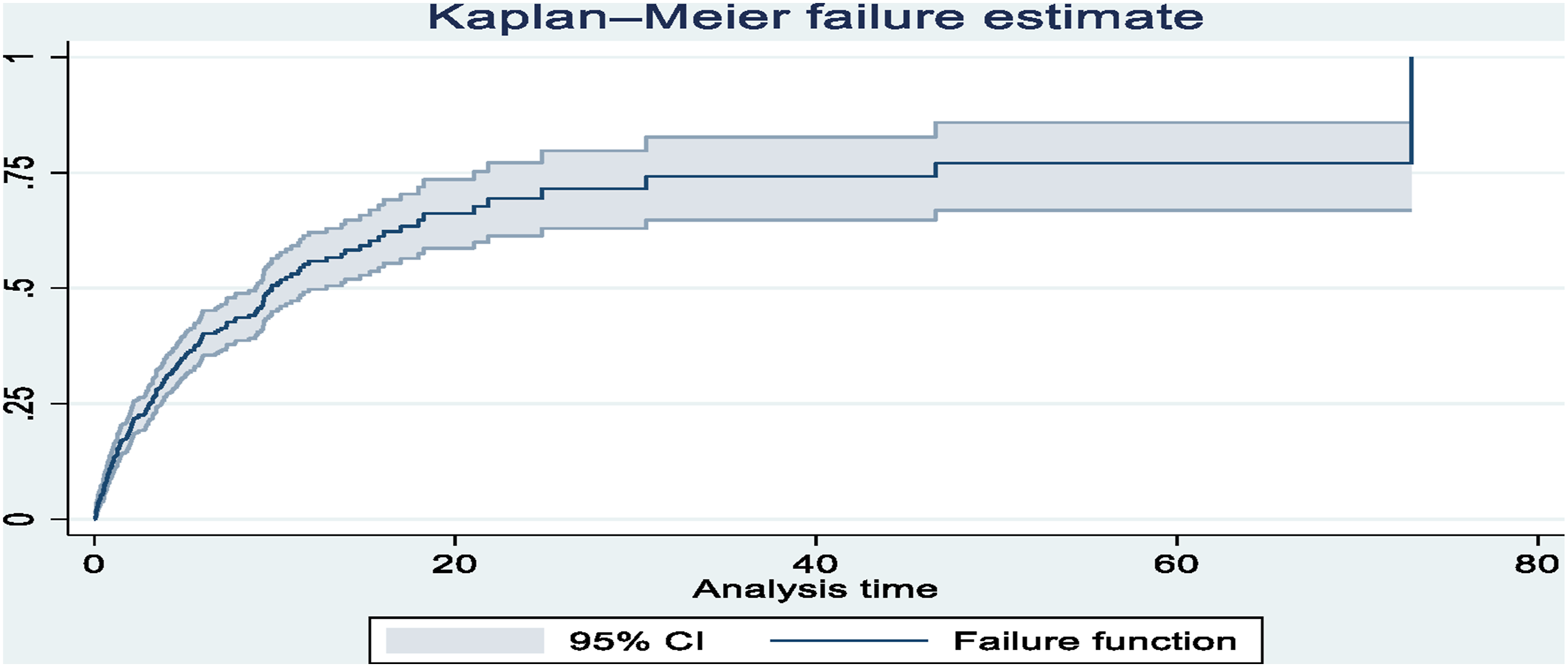
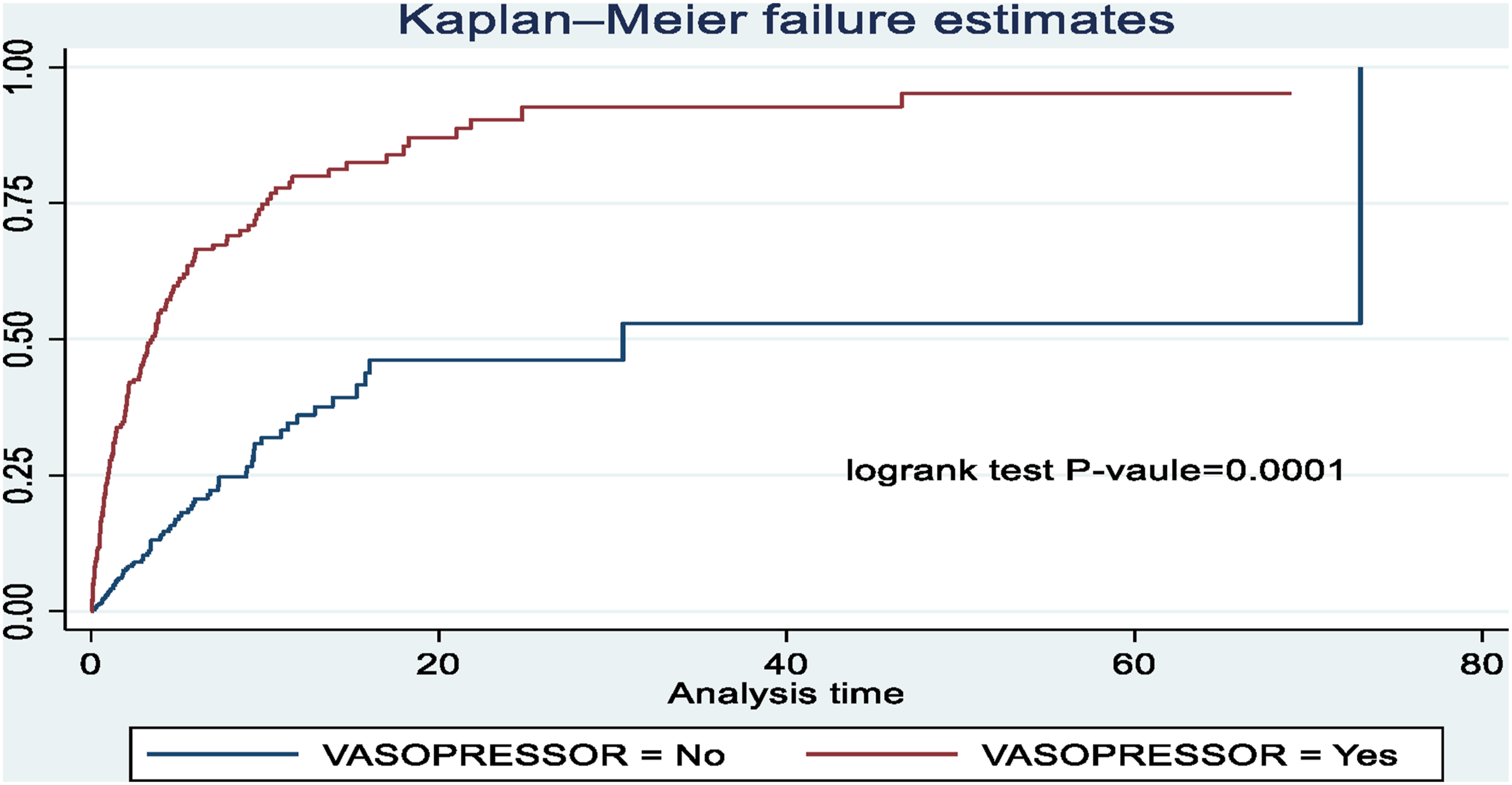
Patients receiving vasopressors and those who did not undergo gastrostomy had lower survival probabilities compared to their counterparts (Figures 2 and 3). Kaplan-Meir survival curve compares survival time of patients who received gastrostomy procedure during mechanical ventilation admitted to ICU in Hiwot Fana comprehensive specialized hospital, Ethiopia, 2024. Kaplan-Meir survival curve compares survival time of patients who received vasopressor and on mechanical ventilation admitted to ICU in Hiwot Fana comprehensive specialized hospital, Ethiopia, 2024.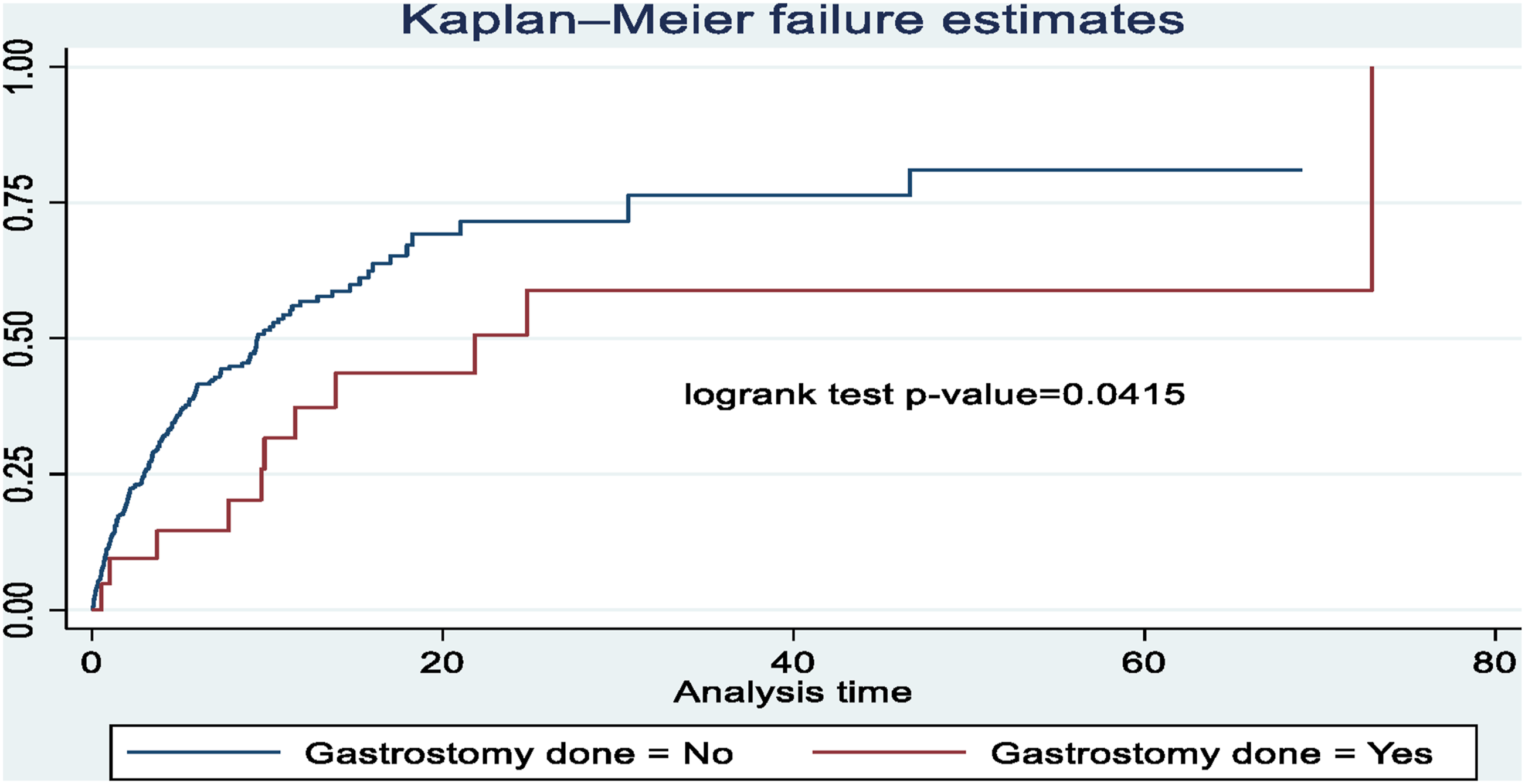
Predictor of time to death among mechanically ventilated patients
In bivariable Cox regression, variables with p < 0.25 and clinically relevant covariates were included in the multivariable model. After adjustment, platelet count <150,000/mm3, cardiovascular failure during mechanical ventilation, cardiopulmonary resuscitation (CPR), vasopressor use, gastrostomy procedure, and fraction of inspired oxygen (FiO2) were independent predictors of time to death.
Patients with platelet count <150,000/mm3 had a 74% higher hazard of death compared to those within the normal range (AHR = 1.74; 95% CI: 1.26–2.40).
Cardiovascular failure during mechanical ventilation increased hazard of death by 62% (AHR = 1.62; 95% CI: 1.08–2.43).
Patients who underwent Cardio Pulmonary Resuscitation (CPR) had more than twice the hazard of death (AHR = 2.36; 95% CI: 1.71–3.31), while vasopressor use was associated with nearly threefold increased hazard (AHR = 2.94; 95% CI: 2.02–4.27).
Each 1% increase in FiO2 at initiation of mechanical ventilation was associated with a 1% increase in hazard of death (AHR = 1.01; 95% CI: 1.007–1.019).
Bivariable and multivariable analysis using cox regression model for predictors of time to death of patients on mechanical ventilation admitted to ICU in Hiwot Fana comprehensive specialized hospital, Ethiopia, 2024.
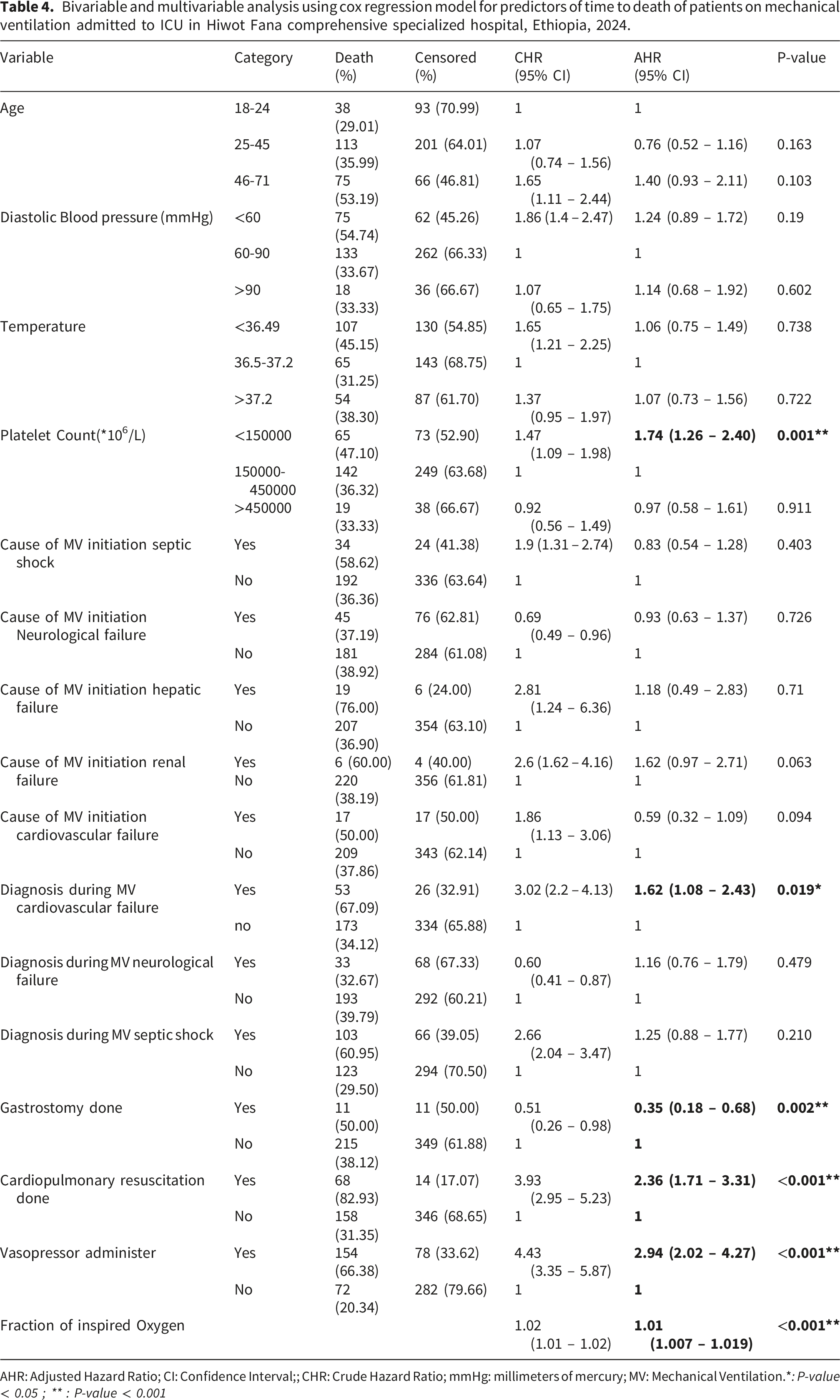
AHR: Adjusted Hazard Ratio; CI: Confidence Interval;; CHR: Crude Hazard Ratio; mmHg: millimeters of mercury; MV: Mechanical Ventilation.*: P-value < 0.05 ; ** : P-value < 0.001
Discussion
The present study assessed time to death and its predictors among adult patients receiving mechanical ventilation in the ICU of Hiwot Fana Comprehensive Specialized Hospital. The median time to death was 9.81 days (95 CI: 8.91-12.86). This finding is comparable with studies conducted in Addis Ababa, Ethiopia (13 days:95% CI: 8.0, 18.0) 26 and Korea (9 days: IQR 7 – 10 days). 18 The relatively short survival time observed in this study suggests that a substantial proportion of mortality occurs early during ICU admission among mechanically ventilated patients. However, this should be interpreted cautiously, as survival time is influenced by case mix, admission severity, and ICU resource availability rather than reflecting a uniform disease progression pattern.
Patients diagnosed with cardiovascular failure during mechanical ventilation had higher hazard of death compared those without this condition. Similar findings have been reported from Brazil. 23 This association is likely explained by underlying disease severity, including hemodynamic instability, impaired tissue perfusion, and progression to multiorgan dysfunction. However, cardiovascular failure in this context should be interpreted as a marker of critical illness severity rather than an independent causal determinant of mortality, and residual confounding by unmeasured severity indices (e.g., APACHE II scores) is likely.
Patients who underwent CPR had a higher hazard of death compared to those who did not, consistent with findings from Ethiopia. 22 This association should not be interpreted as CPR increasing mortality risk. Rather, CPR is typically performed in patients who are already in extremis, indicating reverse causality and confounding by severity of illness. Therefore, CPR reflects a terminal clinical state rather than a modifiable predictor of outcome.
Vasopressor administration was associated with increased hazard of death, consistent with findings from Korea and Colombia.23,25 This relationship likely reflects the presence of shock and severe hemodynamic instability. Therefore, vasopressor use should be considered a proxy indicator of disease severity rather than an independent causal factor of mortality. The observed association is likely confounded by baseline physiological instability and organ failure severity.
Increasing FiO2 at initiation of mechanical ventilation was associated with a slightly increased hazard of death. Similar findings have been reported in multicenter studies.29,30 This may indicate that patients requiring higher oxygen concentrations at initiation of ventilation are more likely to have severe hypoxemic respiratory failure. 31 However, the magnitude of effect was small, and this association should be interpreted in a clinical context rather than as a strong independent predictor of mortality.
Thrombocytopenia was associated with increased hazard of death, consistent with studies from Turkey and Denmark.32,33 This finding may reflect underlying coagulopathy, sepsis-related platelet consumption, or organ dysfunction. However, platelet count may also act as a surrogate marker of systemic illness severity rather than a direct causal factor of mortality.
Patients who received gastrostomy had a lower hazard of death compared to those who did not.
This finding should be interpreted cautiously due to potential survivor bias (immortal time bias), as patients must survive long enough to receive the procedure. Therefore, the observed protective association may reflect selection of less severely ill or more stable patients rather than a true causal protective effect. Additionally, unmeasured confounding related to nutritional status and overall prognosis may have influenced this association. 34
Despite providing important evidence on time to death and its predictors among mechanically ventilated adult patients, this study has several limitations that should be considered when interpreting the findings. First, the study employed a retrospective cohort design based on medical record review, which is inherently subject to limitations such as incomplete documentation, missing variables, and potential recording errors. Second, important clinical variables such as body mass index (BMI), APACHE II score and other standardized severity of illness indicators were not available in the medical records. The absence of these variables limits the ability to fully adjust for baseline disease severity and increases the likelihood of residual confounding.
Third, although multivariable Cox regression was applied, the study may still be affected by unmeasured confounding, particularly due to the lack of comprehensive physiological and laboratory severity indicators. Fourth, the findings are based on a single-center study, which may limit the generalizability of the results to other ICU settings with different patient profiles, staffing levels, and resource availability. Finally, selection bias cannot be excluded, as only patients with complete and retrievable medical records were included in the analysis.
Conclusions
In summary, the median time to death among mechanically ventilated patients in this study was comparable to findings from similar settings. Several factors, including low platelet count (<150,000/mm3), cardiovascular failure during mechanical ventilation, cardiopulmonary resuscitation, vasopressor use, and higher fraction of inspired oxygen at initiation, were associated with an increased hazard of death, while receipt of gastrostomy was associated with a lower hazard of death.
However, these associations should be interpreted cautiously, as many of these variables likely reflect underlying severity of illness rather than direct causal effects. In particular, interventions such as vasopressor use and cardiopulmonary resuscitation may represent markers of critical clinical status.
From a clinical perspective, the findings highlight the importance of close monitoring and timely management of critically ill patients, especially those presenting with indicators of severe illness. Nevertheless, causal inferences cannot be established due to the observational nature of the study.
Future research using prospective study designs and incorporating standardized severity scoring systems, such as APACHE II is recommended to better clarify these relationships.
Footnotes
We would like to express our sincere gratitude to Haramaya University, College of Health and Medical Sciences, School of Public Health, and the Postgraduate Program Directorate for providing the opportunity to conduct this research. We also extend our appreciation to the staff and administration of Hiwot Fana Comprehensive Specialized Hospital for their cooperation during data collection.
Ethical considerations
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University, College of Health and Medical Sciences (Ref. No: IHRERC/305/2024). As the study used secondary/anonymized data and involved no direct contact with participants, the requirement for written informed consent was waived by the Ethics Review Committee. Permission to access patient records was obtained from the hospital administration. All data were collected using a structured data extraction tool, and no personal identifiers (such as names, medical record numbers, or contact information) were recorded. To ensure confidentiality, data were anonymized and stored securely with access limited to the research team. The study was conducted in accordance with relevant ethical guidelines and regulations for research involving human subjects.
Authors’ contributions
Conception and design of the work, acquisition of data, analysis, and interpretation of data were done by Rahma Esmael. Data curation, drafting the article, revising it critically for intellectual content, validation, and final approval of the version to be published were done by Adisu Birhanu Weldesenbet, Behailu Hawulte Ayele and Rahma Esmael. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All necessary information’s were included with the manuscript.