
Abstract
Aim
To determine the prevalence and underlying causes of nonglaucomatous optic atrophy (NGOA) in a tertiary referral center in southeastern Iran and to identify predictors of current visual acuity in this population.
Methods
In this descriptive cross-sectional study, patients with a confirmed diagnosis of NGOA were included. All cases had a definitive etiologic diagnosis based on clinical evaluation, paraclinical investigations, and thorough review of medical records. Patients were classified into etiologic categories including hereditary or developmental disorders; secondary or consecutive optic atrophy; traumatic optic neuropathy (TON); compressive lesions; raised intracranial pressure–related involvement; inflammatory or demyelinating disease; infiltrative processes; toxic exposure; and ischemic causes.
Results
A total of 155 eyes from 155 patients with NGOA were analyzed, of whom 86 (55.5%) were male. Overall, 75 patients (48.4%) had a best-corrected visual acuity (BCVA) of ≥ 1.90 logMAR (logarithm of the minimum angle of resolution), corresponding to counting fingers vision or worse. Patients with toxic optic neuropathy demonstrated the poorest visual outcomes, with 5 of 6 cases (83.3%) having a BCVA of ≥ 1.90 logMAR. Ischemic causes were the most prevalent etiology, identified in 46 patients (29.7%), including 45 cases of non-arteritic anterior ischemic optic neuropathy (AION). TON was the second most common cause, observed in 37 patients (23.9%). In multivariate analysis, a longer duration from symptom onset was the sole independent predictor of poorer current visual acuity (β = 0.253, P = 0.010).
Conclusion
Previous non-arteritic AION was the most common cause of NGOA in this cohort, followed by TON. Toxic exposure was associated with the poorest visual acuities. Among all evaluated variables, the duration from symptom onset was the only independent predictor of current visual acuity.
Introduction
Optic nerve atrophy is a common long-term outcome of various disorders that result in damage to retinal ganglion cell axons. It represents a final clinical endpoint for a wide range of pathological processes affecting the optic nerve, optic tracts, brain, and, in some cases, the retina. With the exception of advanced glaucoma, which is a well-recognized cause of optic atrophy, other etiologies are classified as non-glaucomatous optic atrophy (NGOA). The underlying causes of NGOA are heterogeneous and include inflammatory, compressive, toxic, ischemic, and hereditary conditions that lead to optic neuropathy and subsequent axonal loss. Previous demographic and epidemiologic studies have demonstrated considerable variation in the prevalence of these etiologies across different populations and regions.1–6 Regardless of the underlying cause, once optic atrophy has developed, axonal damage is largely irreversible and no disease-specific therapies are currently effective in restoring visual function. 7 Therefore, determining the prevalence of etiologic factors is essential for identifying the most relevant acquired and genetic risk factors, as well as for guiding diagnostic and preventive strategies.
Several studies worldwide, including reports from Middle Eastern countries, have investigated the incidence and epidemiologic characteristics of NGOA.1–3 However, no large-scale study has evaluated the prevalence and etiologic spectrum of NGOA in Iran. Optic atrophy is a significant cause of visual impairment; in Iran, diseases of the optic nerve and optic tract account for approximately 10% of all cases of visual impairment and blindness.8,9 Given this relatively high burden and the lack of comprehensive national data, further investigation is warranted.
Accordingly, the present study was conducted to determine the prevalence and underlying causes of NGOA in patients evaluated at a tertiary referral center in southeastern Iran. In addition, we aimed to assess differences in current visual acuity among patients with NGOA based on etiologic factors, as well as to identify predictors of current visual acuity in this population.
Methods
Study design
This descriptive cross-sectional study was conducted between March 2024 and March 2025 at the Ophthalmology Department of Shafa Hospital, Kerman, Iran. The study protocol was approved by the Ethics Committee of Kerman University of Medical Sciences (approval code: IR.KMU.AH.REC.1402.211) and was performed in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants or their legal guardians.
Study setting and population
All participants underwent a comprehensive ophthalmologic examination, including measurement of best-corrected visual acuity (BCVA), assessment of pupillary light reflex for detection of a relative afferent pupillary defect (RAPD), slit-lamp biomicroscopy, Goldmann applanation tonometry, and dilated fundus examination. BCVA was measured using a Snellen E-chart and converted to logarithm of the minimum angle of resolution (logMAR) units for statistical analysis. Visual acuity categories were assigned the following logMAR equivalents: no light perception (3.0), light perception (2.7), hand motion (2.3), and counting fingers (1.9). 10 In patients with bilateral optic atrophy, the eye with worse visual acuity was selected for analysis to ensure inclusion of only one eye per patient.
A detailed history of symptom onset was obtained, including decreased visual acuity (blurred or reduced vision), visual field defects, color vision disturbances (e.g., washed-out colors), reduced contrast sensitivity (difficulty seeing in dim light or lack of visual sharpness), and altered brightness perception (objects appearing dimmer in the affected eye). The time of symptom onset was recorded. In young children, indirect indicators such as nystagmus, strabismus, incidental detection during routine ophthalmologic examination, or referral by a neurologist or pediatrician leading to the diagnosis of optic atrophy were considered.
Diagnostic criteria and etiologic classification
Diagnostic criteria for etiologic classification of non-glaucomatous optic atrophy (NGOA) 11 .

LHON: Leber hereditary optic neuropathy, ADOA: Autosomal dominant optic atrophy, OPA1: Optic atrophy 1 gene, m.11778G>A/m.14484T>C: Mitochondrial DNA point mutations associated with LHON, RPE: Retinal pigment epithelium, ERG: Electroretinography, OCT: Optical coherence tomography, RAPD: Relative afferent pupillary defect, CT: Computed tomography, MRI: Magnetic resonance imaging, CSF: Cerebrospinal fluid, LP: Lumbar puncture, AION: Anterior ischemic optic neuropathy, MS: Multiple sclerosis.
Patients in whom a definite etiology for optic atrophy could not be established were excluded from the study.
Systemic risk factors for ischemic or vascular events, including diabetes mellitus and hypertension, were evaluated based on documented medical history, current medication use, or contemporaneous laboratory results.
Patients were excluded if they had incomplete medical records, optic nerve or central nervous system pathologies that had not progressed to optic atrophy (such as acute optic neuritis without atrophic changes), or glaucomatous optic nerve atrophy. Glaucomatous optic atrophy was differentiated from NGOA based on characteristic features, including relatively preserved neuroretinal rim coloration, less prominent pallor, deeper and more focal optic disc cupping, and the presence of peripapillary atrophy, which supported a glaucomatous etiology. 2
Data analysis
Statistical analyses were performed using SPSS software version 24 (IBM Corp., Chicago, IL, USA). Continuous variables were summarized using mean, standard deviation, and range, while categorical variables were presented as frequencies and percentages. Multiple linear regression analysis was performed to identify predictors of current BCVA. Variables with a variance inflation factor greater than 5 were considered to exhibit excessive multicollinearity and were excluded from the model. Independence of residuals was assessed using the Durbin–Watson statistic, with values between 1.5 and 2.5 indicating acceptable independence. A two-tailed p-value less than 0.05 was considered statistically significant.
Results
Demographic characteristics, clinical features, and etiologies of nonglaucomatous optic atrophy.
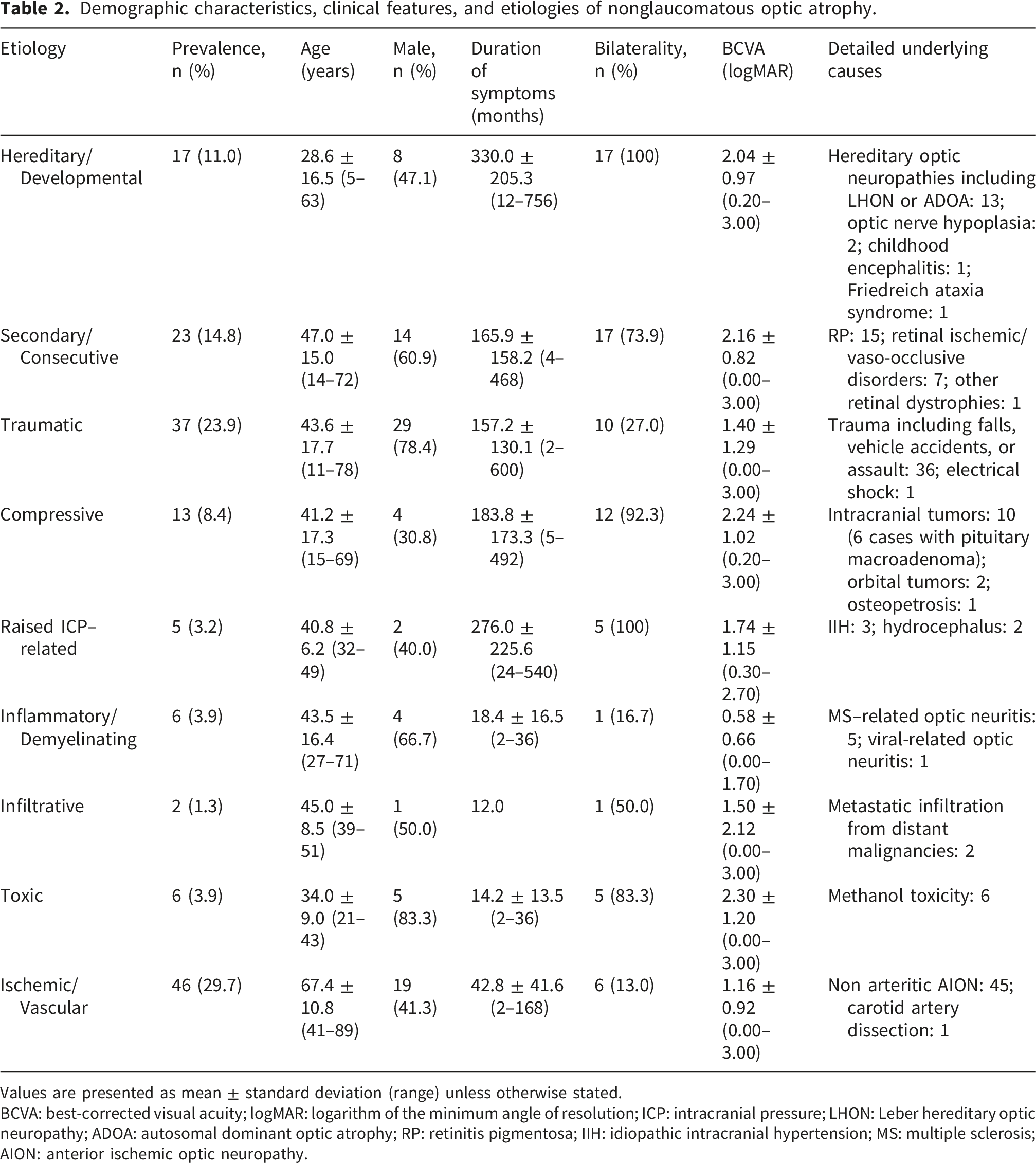
Values are presented as mean ± standard deviation (range) unless otherwise stated.
BCVA: best-corrected visual acuity; logMAR: logarithm of the minimum angle of resolution; ICP: intracranial pressure; LHON: Leber hereditary optic neuropathy; ADOA: autosomal dominant optic atrophy; RP: retinitis pigmentosa; IIH: idiopathic intracranial hypertension; MS: multiple sclerosis; AION: anterior ischemic optic neuropathy.
Distribution of best-corrected visual acuity (BCVA) in logMAR ranges across etiologies of nonglaucomatous optic atrophy (NGOA).

Values are presented as number (percentage within each etiologic group).
BCVA: best-corrected visual acuity; logMAR: logarithm of the minimum angle of resolution; ICP: intracranial pressure.
Eleven patients (7.1%) were aged 18 years or younger and were classified as the pediatric subgroup. In this subgroup, the most common etiologies were hereditary causes (4 cases, 36.4%), traumatic optic neuropathy (3 cases, 27.3%), secondary/consecutive causes (2 cases, 18.2%), and compressive optic neuropathy (2 cases, 18.2%).
Univariate and multivariate regression analyses evaluating the effect of demographic and clinical variables on current BCVA (LogMAR).

BCVA: best-corrected visual acuity, CI: confidence interval.
Discussion
Although previous studies have reported etiologic distributions of NGOA in various populations, including some Middle Eastern countries, large cohort data from Iran remain limited.2–6,8 Furthermore, previous studies have not evaluated independent predictors of current visual acuity using multivariate models incorporating etiology, disease duration, and demographic variables. Therefore, this study provides novel insights into both the etiologic spectrum and determinants of visual acuity in NGOA in southeastern Iran.
The most common cause of optic atrophy in the present study was ischemic/vascular optic neuropathy (29.7%), with non arteritic AION accounting for nearly all cases (45 of 46). Similarly, Kılıçarslan et al. reported that 29.2% of NGOA cases in Turkey were attributable to AION, including both arteritic and non-arteritic forms. 2 In our cohort, this etiologic group had the highest mean age (67.4 ± 10.8 years), which is consistent with existing literature indicating that AION is the most common optic neuropathy in individuals over 50 years of age.13,14 Thus, our results align well with prior epidemiologic studies.
TON was the second most common cause of optic atrophy in our study, accounting for 23.9% of cases. The frequency and etiologic distribution of TON vary widely across regions and countries.2,4,15–17 In Nepal, Shrestha et al. reported trauma as the leading cause of optic atrophy (25.8%), 4 which is comparable to our findings. The relatively high frequency of TON in our study may be explained by the high burden of road traffic accidents in Iran, which remains a major cause of trauma-related injuries and mortality. 18 Since most TON cases in our cohort were associated with traffic-related accidents, TON constituted one of the leading etiologies of NGOA in our region and was the second most common cause in our study population. Therefore, compared with studies from other countries, the higher prevalence of TON in our cohort may reflect the greater incidence of traffic-related trauma in Iran. 18 The mean age of patients with traumatic optic atrophy in our study (43.6 ± 17.7 years) was slightly higher than that reported in several previous studies, in which the majority of patients were younger than 40 years.2,4,15–17 The higher mean age of patients in our study compared with previous reports may be related to the broader age distribution of individuals involved in road traffic accidents in our population. 18 In contrast, studies from other countries may include fewer trauma cases and may involve predominantly younger age groups. Male predominance was evident (78.4%), consistent with earlier reports, likely reflecting higher exposure of males to high-risk activities. Road traffic accidents were the most common cause of trauma in our cohort, in agreement with previous studies.2,4,15–17
Hereditary and developmental disorders constituted the most common etiologic category among pediatric patients. Previous studies have similarly reported hereditary optic neuropathies (such as LHON and ADOA) and developmental brain or optic nerve disorders as leading causes of NGOA in children.19,20 This explains the relatively younger mean age observed in this etiologic group in our study.
Several studies have reported intracranial tumors as a leading cause of optic atrophy. For instance, Kılıçarslan et al. found that central nervous system–related causes, particularly intracranial tumors, accounted for 27.2% of NGOA cases, 2 while Mbekeani et al. reported tumors as the predominant etiology (55.4%) in a Saudi Arabian cohort. 3 Our findings are in agreement with Kılıçarslan et al., as pituitary adenoma was the most frequent intracranial tumor associated with NGOA in both studies. However, in our cohort, compressive optic neuropathy accounted for only 8.4% of cases. This discrepancy may be attributed to referral patterns, selection bias, differences in study populations, and variability in access to specialized neurosurgical services across centers.
Consecutive optic atrophy related to chorioretinal diseases constituted a substantial proportion of NGOA cases in our cohort. Studies from India and underdeveloped African countries have similarly reported a high prevalence of consecutive optic atrophy, with RP being the most common underlying cause.5,6 Consistent with these findings, RP was the leading cause within this category in our study.
Toxic optic neuropathy accounted for 3.9% of cases, with all affected patients having methanol toxicity and a strong male predominance. This finding closely parallels results from Turkey, where toxic causes accounted for 3.5% of optic atrophy cases, with methanol ingestion responsible for approximately half. 2 The high prevalence of severe visual loss in this group underscores the devastating visual consequences of methanol poisoning.
Inflammatory or demyelinating optic neuropathy accounted for 5.6% of NGOA cases in our study, with MS being the most common underlying cause. This is consistent with previous reports. 2 Although MS-related optic neuritis is more prevalent among females, male patients may experience greater retinal nerve fiber layer thinning and more pronounced neuroaxonal loss following inflammation, 21 which may explain the male predominance observed in our cohort.
We excluded cases with unknown or idiopathic optic atrophy, which accounted for 10 patients. Other studies have reported varying proportions of idiopathic optic atrophy, often attributed to limited diagnostic resources or incomplete investigations. 1 Differences in environmental exposure, genetic background, access to advanced diagnostic tools (such as genetic testing), and heterogeneity in etiologic classification systems likely contribute to the wide variation in reported NGOA etiologies across regions.
Optic atrophy is a major cause of visual impairment and blindness worldwide.22,23 In our study, toxic optic neuropathy was associated with the poorest visual acuity outcomes, with 83.3% of cases having BCVA ≥ 1.90 logMAR, consistent with previous reports. 2 However, in multivariate analysis, the etiology of NGOA was not independently associated with current visual acuity. Instead, the duration from symptom onset was the only significant predictor of worse current visual acuity. This finding suggests that optic atrophy represents a progressive process of axonal degeneration, in which prolonged disease duration leads to cumulative neuroaxonal loss and worsening visual acuity, even when the optic disc appearance remains relatively stable over time. 24
Although reduced visual acuity is the most common presenting symptom of optic atrophy, some patients may primarily exhibit deficits in other visual functions, such as visual field, contrast sensitivity, or color vision. In our study, 9.7% of patients had normal or near-normal BCVA (0.00–0.10 logMAR), which is consistent with previous reports.2,3,20 Visual acuity reflects foveal function, whereas optic atrophy reflects axonal loss that may spare the papillomacular bundle, preserving central vision. Additionally, in cases of post-inflammatory or post-edematous optic atrophy following resolved optic neuritis or chronic papilledema, visual acuity may recover fully despite residual optic disc pallor. 25 Therefore, clinicians should not rely solely on visual acuity when evaluating suspected optic atrophy; comprehensive assessment of visual fields, contrast sensitivity, and color vision, along with fundus examination, OCT, and neuroimaging when indicated, is essential.
This study has some strengths, including a relatively large sample size and access to neuroimaging and laboratory investigations, which enhanced diagnostic accuracy. However, several limitations should be acknowledged. The single-center design and the absence of a formal sample size calculation may limit the generalizability of the findings. The relatively small pediatric sample limits age-stratified analyses. Additionally, not all visual functions or structural parameters, including retinal nerve fiber layer and ganglion cell layer thickness on OCT, were assessed in every patient, as advanced testing was primarily performed in cases with near-normal visual acuity or atypical clinical presentations. Future multicenter, population-based studies with comprehensive functional and structural assessments are needed to better characterize NGOA in Iran and clarify regional differences.
Conclusion
In this cohort, the most common cause of NGOA was previous AION, followed by TON. The poorest visual acuity was observed in patients with toxic optic neuropathy secondary to methanol poisoning. Among all evaluated variables, the duration from symptom onset was the only independent predictor of current visual acuity, underscoring the importance of early recognition and evaluation of optic nerve disorders.
Footnotes
Ethical considerations
The study was approved by the ethics committee of Kerman University of Medical Sciences, Kerman, Iran (ethics code: IR.KMU.AH.REC.1402.211). The study was explained to eligible participants and written informed consents were obtained. The study was in accordance with Declaration of Helsinki and the national guidelines and regulations.
Consent to participate
Written informed consent was obtained from all participants or their legal guardians, regarding any research use of medical information without disclosing their identity.
Author contributions
Me.Sharifi and A.Sharifi designed the study. Mo.Sharifi and A.Sharifi collected data. A.Zand and Me.Sharifi analyzed and reported the data. Mo.Sharifi and Me.Sharifi wrote the first draft of the paper. A.Sharifi and A.Zand contributed to the writing and revision of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.