
Abstract
Background and aims
Coronary artery ectasia (CAE) can lead to adverse clinical outcomes, including coronary spasm, thrombosis, dissection and myocardial ischaemia. In patients with isolated CAE– in the absence of coronary artery stenosis, clinical symptoms such as angina pectoris may still occur. This study aimed to investigate the relationship between clinical features and circulating inflammatory marker levels in patients with isolated CAE.
Methods
Patients undergoing coronary angiography (CAG) who consented to participate underwent cardiovascular disease and risk assessment. The study enrolled 52 patients with isolated CAE and 25 control individuals with normal coronary angiograms. Coronary blood flow in the three groups was assessed using the Thrombolysis in Myocardial Infarction (TIMI) frame count. Levels of inflammatory markers-including C-reactive protein (CRP), interleukin-1β (IL-1β), interleukin-8 (IL-8), IL-10 and tumor necrosis factor-alpha (TNF-α) – were measured in the circulating blood of symptomatic and asymptomatic patients with isolated CAE and compared between the two groups.
Results
Symptomatic patients with isolated CAE showed significantly higher circulating levels of IL-1β and TNF-α than asymptomatic patients (p<0.05). In addition, coronary TIMI frame counts were lower (indicating slower blood flow) in symptomatic patients compared with asymptomatic individuals (p<0.05).
Conclusions
In patients with isolated CAE, the presence of symptoms is associated with elevated circulating levels of pro-inflammatory markers such as IL-1β and TNF-α, as well as reduced coronary blood flow.
Introduction
Coronary artery ectasia (CAE) generally refers to the diffuse or focal dilation of a coronary artery, with the lumen diameter of ectatic segment exceeding 1.5 times over the diameter of the adjacent normal reference segment. 1 CAE dilated coronary artery has decreased blood flow blood flow velocity, and the flow pattern shifts from laminar to turbulent flow leading to vascular injury that results in clinical symptoms such as chest pain. 1
Currently, it is believed that the common causes of CAE include hypertension, dyslipidemia, previous percutaneous transluminal coronary angioplasty, nodular polyarteritis, Kawasaki disease, and diabetes etc. 2 Atherosclerosis is considered as an additionally possible pathogenic mechanism. 3 Atherosclerosis is the main cause of coronary artery disease (CAD). For patients with concurrent CAD, it is generally believed to represent different stages or specific forms of atherosclerosis development, with inflammation being the essential characteristic of atherosclerosis. 4 Many epidemiological and clinical studies have shown that elevated levels of leukocytes, CRP, IL-1β, and other inflammatory markers are predictive factors for cardiovascular events in patients with CAD in later stages. 4
The clinical manifestations of CAE vary by subtype.1,5 The most widely used classification system is the Markis classification, which categorises CAE based on the extent and distribution of coronary involvement. Type I refers to diffuse ectasia involving two or three vessels. Type II describes diffuse ectasia in one vessel and focal ectasia in another. Type III denotes diffuse ectasia confined to a single vessel. Types I and II are more frequently associated with concomitant obstructive coronary artery disease. 5 Type IV, in contrast, describes focal or segmental ectasia involving a single vessel, with the remainder of the coronary tree being normal. This pattern represents the prototypical form of isolated CAE (ICAE), in which inflammation is considered the main pathogenic mechanism. Type IV ICAE is characterised by a lower atherosclerotic burden and no significant coronary artery stenosis on angiography.6,7
Coronary artery ectasia (CAE) is associated with congenital defects, atherosclerosis, endothelial dysfunction and inflammation. Frequently accompanied by coronary stenosis and abnormal blood flow, it can lead to adverse outcomes such as coronary spasm, thrombosis, distal embolisation, dissection and myocardial ischaemia. 5 Isolated CAE (ICAE) is defined by the absence of significant coronary stenosis,1,5 nevertheless, some patients still experience clinical symptoms, including angina and chest tightness. Although inflammation has been implicated in the pathogenesis of ICAE, few studies have examined the relationship between circulating inflammatory marker levels and clinical features. 6 Moreover, whether the clinical manifestation of ICAE is independently associated with the burden of systemic inflammation remains unclear. Therefore, the primary objective of this study was to test the hypothesis that, after adjusting for potential confounders, higher circulating levels of specific inflammatory markers are positively associated with the presence of typical cardiac symptoms in patients with ICAE.
Materials and methods
Clinical assessment and symptom definition
In this prospective cohort study, we investigated the association between clinical features and circulating levels of inflammatory markers in isolated CAE.
Patients were classified into symptomatic, asymptomatic and control groups based on clinical records. 1
The symptomatic group was defined as the presence of any of the following typical or atypical cardiac chest discomfort potentially attributable to myocardial ischemia1,8: (1) Typical angina
Patients collection and study design
In this study, for patients with symptoms such as chest pain or tightness, abnormal electrocardiogram or cardiac enzyme findings, or other indications requiring definitive diagnosis. We prospectively enrolled 2,261 patients who were first diagnosed by coronary angiography at Ji’an Central People’s Hospital affiliated Jinggangshan University from January 2020 to December 2025. The inclusion criteria were as follows: 18<age <80years old; chronic coronary syndrome (CCS); acute coronary syndrome (ACS); receiving antiplatelet and statins therapy; informed consent form. Exclusion criteria included CAE after coronary artery bypass grafting, Vascular dilation after coronary interventional therapy, CAE associated with Kawasaki disease, Presence of coronary artery fistula or other vascular anomalies, Congestive heart failure, Untreated thyroid disease, Estrogen replacement therapy, Coexisting severe anemia, fever, or autoimmune diseases, CAD, hypertension, hyperlipidemia, diabetes, and family history of CAD were defined according to the previous studies.1,10 Among 2,261 patients who underwent coronary angiography, 189 were diagnosed with CAE, of whom 74 had isolated CAE. Of the excluded patients, there were 7 patients with congestive heart failure, 6 with abnormal hepatic or renal function, and 9 who met other exclusion criteria. Finally, 52 patients with isolated CAE were enrolled in this study. Based on the previous study definitions[1], they were divided into two groups: 23 symptomatic and 29 asymptomatic patients with CAE. Additionally, 25 individuals without CAE were included as a control group (NC) to establish a baseline reference, distinguish disease-related inflammatory changes from normal physiological variation, and ensure the robustness of the findings.
This study was reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)guidelines. A completed STROBE checklist is provided as Supplementary Material. And the study protocol was in accordance with the Declaration of Helsinki and approved by the local ethics committee of Jinggangshan University (serial number 2020-006). Written informed consent was obtained from each participant before any sample or data collection.
All patients underwent blood tests to assess the levels of inflammatory factors including CRP, IL-1β, IL-8, IL-10, and TNF-α in peripheral blood. The selection of inflammatory markers in this study was based on their established roles in vascular inflammation and pathological remodeling. Specifically, IL-1β, IL-8, IL-10 and TNF-α were measured because these are key mediators of the inflammatory response and have been implicated in promoting responses that further degrade vascular integrity and are related to an impaired coronary circulation as well.2,11 CRP was selected due to it involvements in promoting the secretion of matrix metalloproteinases (MMPs), which degrade extracellular matrix and lead to vessel wall weakening.12,13 This panel of markers provides a comprehensive evaluation of the inflammatory landscape in isolated CAE, as no single marker fully captures the complexity of the disease process. The number of segments with CAE was also evaluated, and coronary blood flow velocity was assessed using the Thrombolysis in Myocardial Infarction (TIMI) frame count (TFC).
Coronary angiography
Using a Philips Allura Xper FD10 system via the Judkins technique. 7 Standard angiographic views, including the hepatocranial view (caudal 30°+right 30°), right anterior oblique with cranial angulation (cranial 30°+right 30°), and left anterior oblique 45° view, were obtained to evaluate the left anterior descending artery (LAD), left circumflex artery (LCX), and right coronary artery (RCA), respectively.
Quantitative analysis of coronary artery dilation was conducted using angiography analysis software QCA-CMA 6.0. 14 Blood flow velocity was assessed using the thrombolysis in myocardial infarction (TIMI) frame count (TFC) method following established protocols. 2 Patients were classified into either isolated or complex coronary artery ectasia based on the presence or absence of luminal obstruction caused by the coronary dilation.
Blood sample collection
Venous blood samples were collected before operation, placed in an Eppendorf tube containing 5 ml EDTA anticoagulant, immediately inverted, left standing for 20 min, centrifuged at 2000 r.p.m for 10 min to separate the serum, and stored at -20°C for later use. As previously described, all measurements of inflammatory factors were standardized by concentration titration and appropriate purification, including: IL-1β<5 pg/ml, IL-8 <62 pg/ml, IL-10 <1.8 pg/ml, TNF-a <8.1 pg/ml.3,14
Laboratory analysis
Blood samples were tested using a fully automated analyser and a biochemical immunoprotein analyzer (Shanghai Biotechnology Pharmaceutical Company, Shanghai, China) for blood cell count, CRP, IL-1β, IL-8 and IL-10 measurement, respectively. Serum concentration of TNF-α were determined by enzymelinked immunosorbent assay (ELISA) kits (Cat no J20223, Wuhan, Hubei, China), following the manufacturers’ instructions.
Statistical analysis
Statistical analyses were performed using SPSS20.0 software (SPSS Inc., Chicago, IL, USA). Normality of the distribution of continuous variables was assessed using the Shapiro-Wilk test. Homogeneity of variances among groups was evaluated using Levene’s test. If the assumptions of normality and homogeneity of variances were met, one-way ANOVA followed by post hoc tests was used for comparisons among the three groups. If the assumptions were violated, the non-parametric test was applied, followed by pairwise comparisons using the Mann–Whitney U test with Bonferroni correction. Additionally, the continuous variables are presented as means±standard deviations for normally distributed data, while non-normally distributed data are resented as medians. Independent samples Student t-test was used for inter-group analysis. Chi-square test or Fisher’s exact test was used for categorical variable analysis. Pearson or Spearman correlation analysis was used for correlation analysis. In addition, to identify independent factors associated with inflammatory marker levels and to adjust for potential confounders, we also performed subgroup analyse. A p-value<0.05 was considered statistically significant.
Power analysis
Based on previous research 15 and the characteristics of the data in this study, we calculated the statistical power to be 0.52. We further conducted a sensitivity power analysis using G*Power 3.1.9.7 software to determine the minimum effect size that could be reliably detected given our current sample size.
Results
Age and gender difference of the patients with isolated CAE and the clinical features
A total of 52 patients with isolated CAE were enrolled in the study (44 men and 8 women, with ages ranging from 41 to 87 years; median, 66 years), of whom 23 were symptomatic and 29 were asymptomatic, The patient screening flowchart is shown in Figure 1. Coronary angiography findings and circulating inflammatory factor levels were analyzed in detail. The demographic and clinical characteristics of the study population are presented in Table 1. The patient screening flow chart. LAB data. Data are presented as mean±SD for normal distribution continuous and % (numbers, n) for categorical characteristics. ICAE: Isolated Coronary Artery Ectasia; BMI: body mass index; LVEF: left ventricular ejection fraction; ACEI: angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; B-blocker, beta blocker; CCB, calcium channel blocker; TFC: TIMI frame count; LAD: left anterior descending coronary artery; RCA: right coronary artery; ICAE: Isolated Coronary artery ectasia.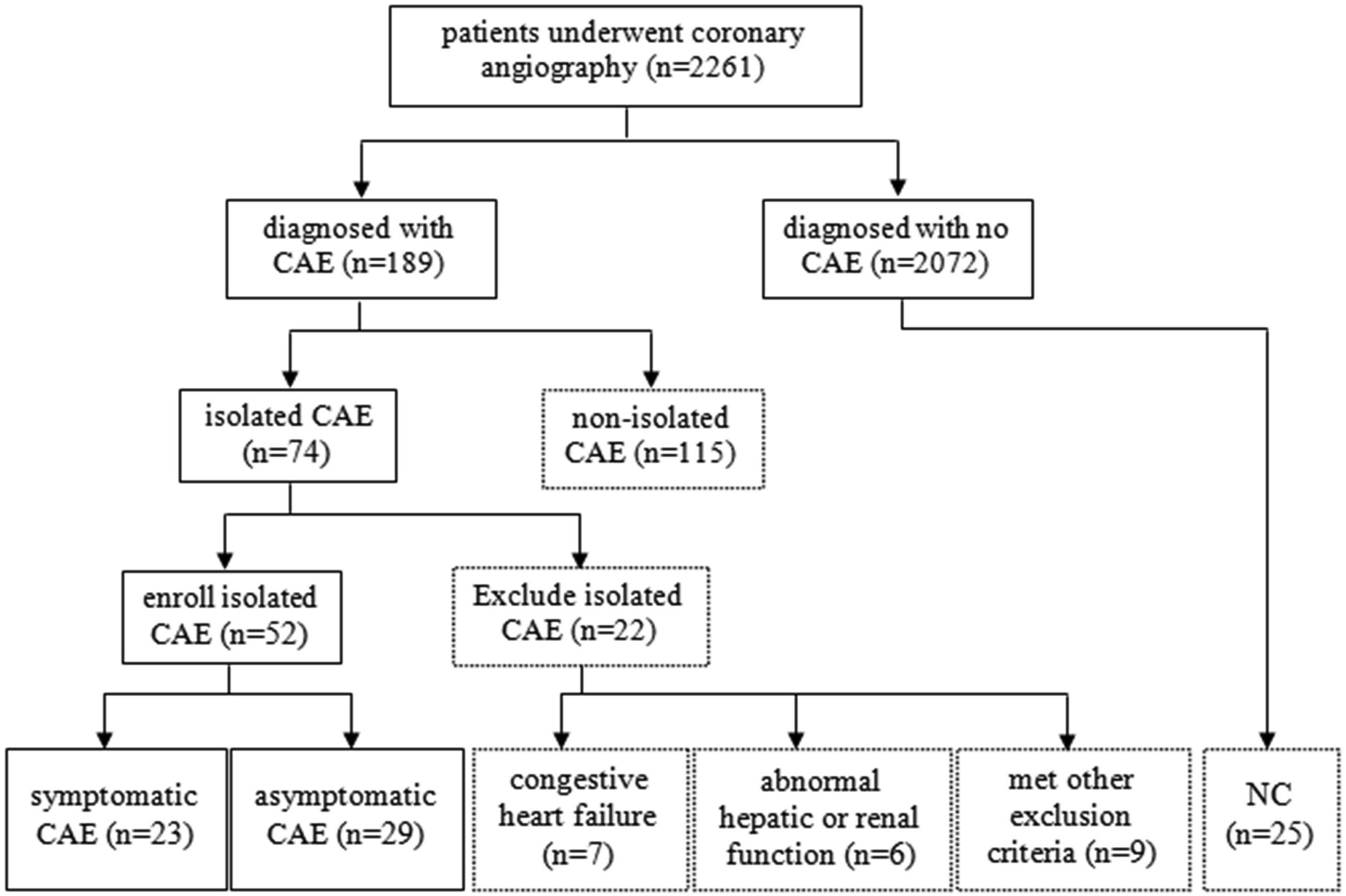

In both symptomatic and asymptomatic isolated CAE, the incidence was higher in men than in women (86.96% vs. 82.76%, p= 0.024). Symptomatic isolated CAE patients had a higher proportion of coexisting hypertension (82.61% vs. 75.86%, p = 0.033). In addition, the proportion of smokers (39.13% vs. 34.48%, p= 0.041) and of those with dyslipidemia (65.22% vs. 58.62%, p< 0.01) was significantly higher in the symptomatic group compared with the control group (Figure 2). Dilated coronary artery Angiogram. A: Isolated CAE of LAD; B: Cae of LAD complicated with CAD; C: Isolated CAE of RCA; D: Cae of RCA complicated with CAD.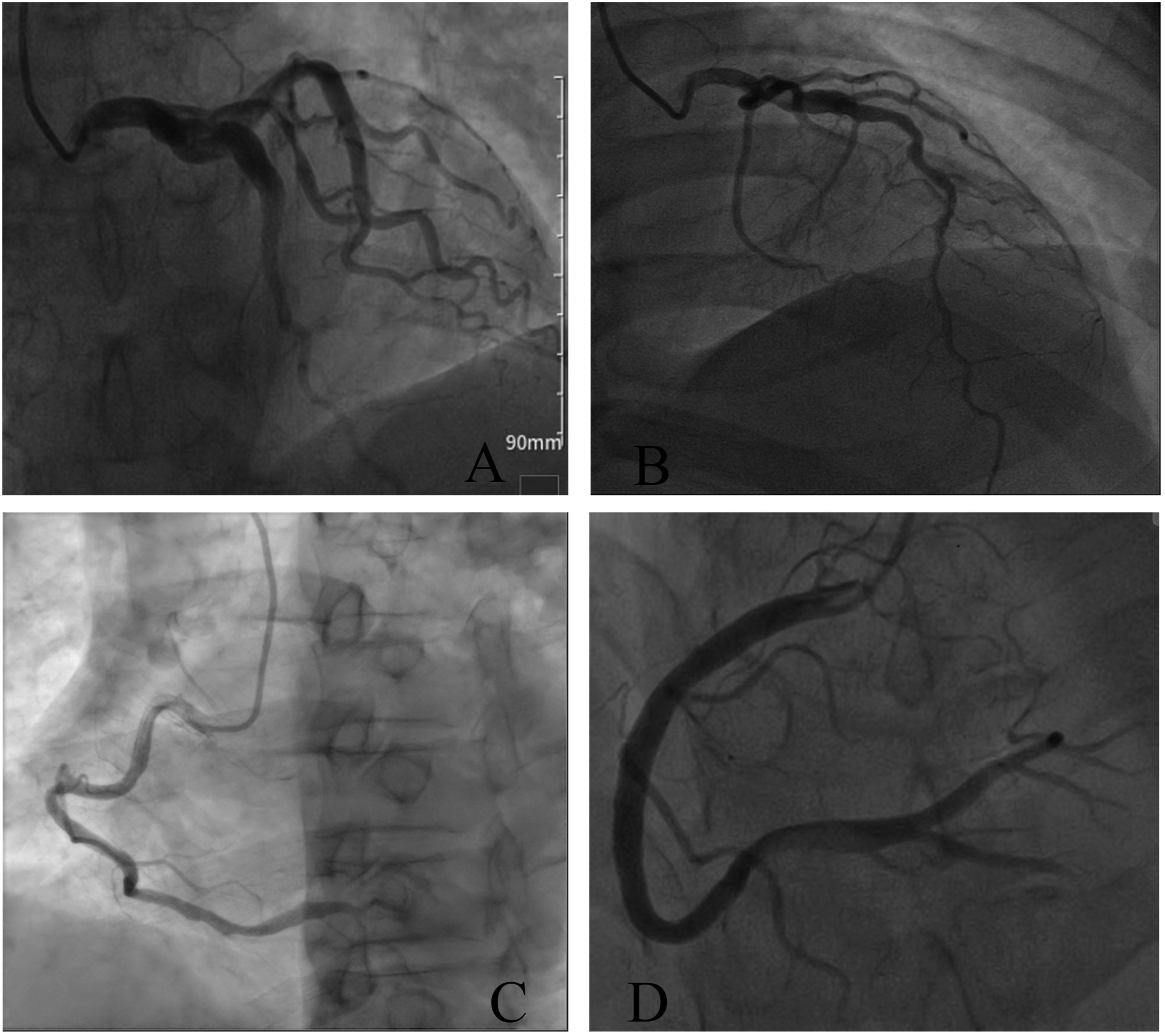
Clinical features of patients with isolated CAE correlate with the involved vessels and the number of affected segments
The angiographic images of patients with isolated and complicated CAE are shown in Figure 1. The clinical data of the three subject groups are shown in Table 1.
To investigate the relationship between clinical features and the involved vessels as well as the number of affected segments in patients with isolated CAE, we performed a detailed analysis of differences in lesion location and segment involvement across three patient groups. We found that coronary artery dilation was more common in the right coronary artery (RCA) in the symptomatic group than in the asymptomatic group (82.61% vs. 51.72%, p<0.01). In contrast, the asymptomatic group more often presented with involvement of the left coronary artery (LAD) (48.28% vs. 34.78% p=0.038). Additionally, the average number of affected coronary artery segments in the symptomatic group was significantly higher than the asymptomatic group (2.89±0.53 vs. 1.96±0.41, p=0.033).
Circulating inflammatory marker levels are elevated in patients with isolated CAE
Laboratory test data.
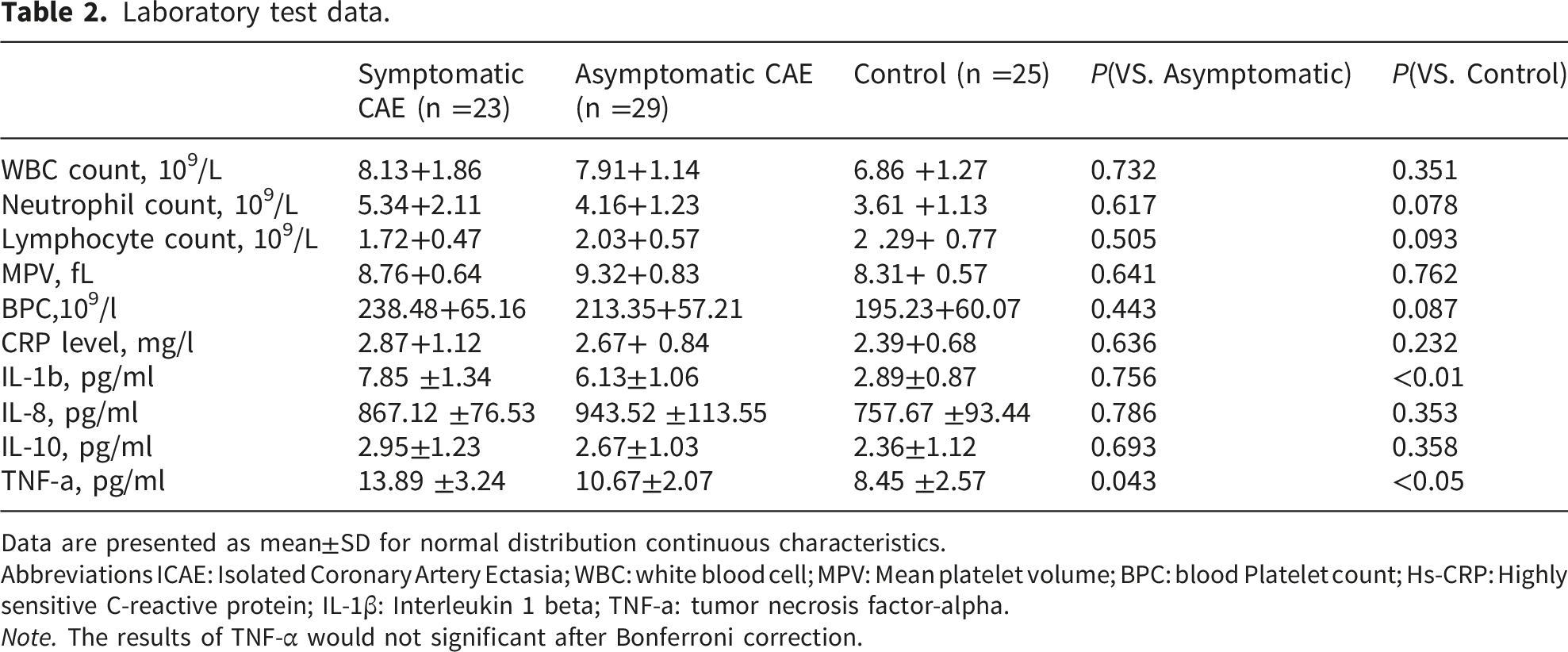
Data are presented as mean±SD for normal distribution continuous characteristics.
Abbreviations ICAE: Isolated Coronary Artery Ectasia; WBC: white blood cell; MPV: Mean platelet volume; BPC: blood Platelet count; Hs-CRP: Highly sensitive C-reactive protein; IL-1β: Interleukin 1 beta; TNF-a: tumor necrosis factor-alpha.
Note. The results of TNF-α would not significant after Bonferroni correction.
Subgroup analyses of inflammatory marker levels by symptomatic status stratified by potential confounders.

Data are presented as mean±SD or mean (95 confidence interval, CI) for continuous characteristics.
The p for interaction tests whether the association between symptomatic status and CRP levels differs across strata of each confounder. A p>0.05 suggests no significant effect modification, indicating that the observed association is robust across subgroups.
Abbreviations: isolated coronary artery ectasia; CRP: C-reactive protein; IL-1β: Interleukin-1 beta; TNF-a:Tumor Necrosis Factor-alpha.
Sensitivity analysis using E-value to assess robustness to unmeasured confounding.

Sensitivity analyses revealed that symptomatic status in patients with ICAE was associated with increased circulating levels of IL-1β and TNF-α.
Abbreviations: isolated coronary artery ectasia; CRP: C-reactive protein; IL-1β: Interleukin-1 beta; TNF-a
Clinical features of patients with isolated CAE are associated with reduced coronary blood flow
To elucidate the relationship between clinical features and coronary blood flow in patients with isolated CAE, we analyzed coronary flow velocity across different groups. The findings showed that, in terms of coronary blood flow, symptomatic patients with dilation of the RCA had a significantly higher TFC (i.e., reduced blood flow) than those with involvement of the LAD (20.31±3.42 vs. 14.47±2.62, p<0.05), Figure 3(a). Furthermore, the TFC on RCA in the symptomatic group was higher than that in the asymptomatic group (20.31±3.42 vs. 16.72±3.55, p=0.027) and also significantly higher than in the control group (20.31±3.42 vs. 12.50±2.63, p<0.01), Figure 3(b) and (c). Statistical analysis of coronary blood flow among the three groups of subjects. A: Comparison of coronary flow between LAD and RCA in symptomatic patients with ICAE; B: Comparison of TFC on LAD; C: Comparison of TFC on RCA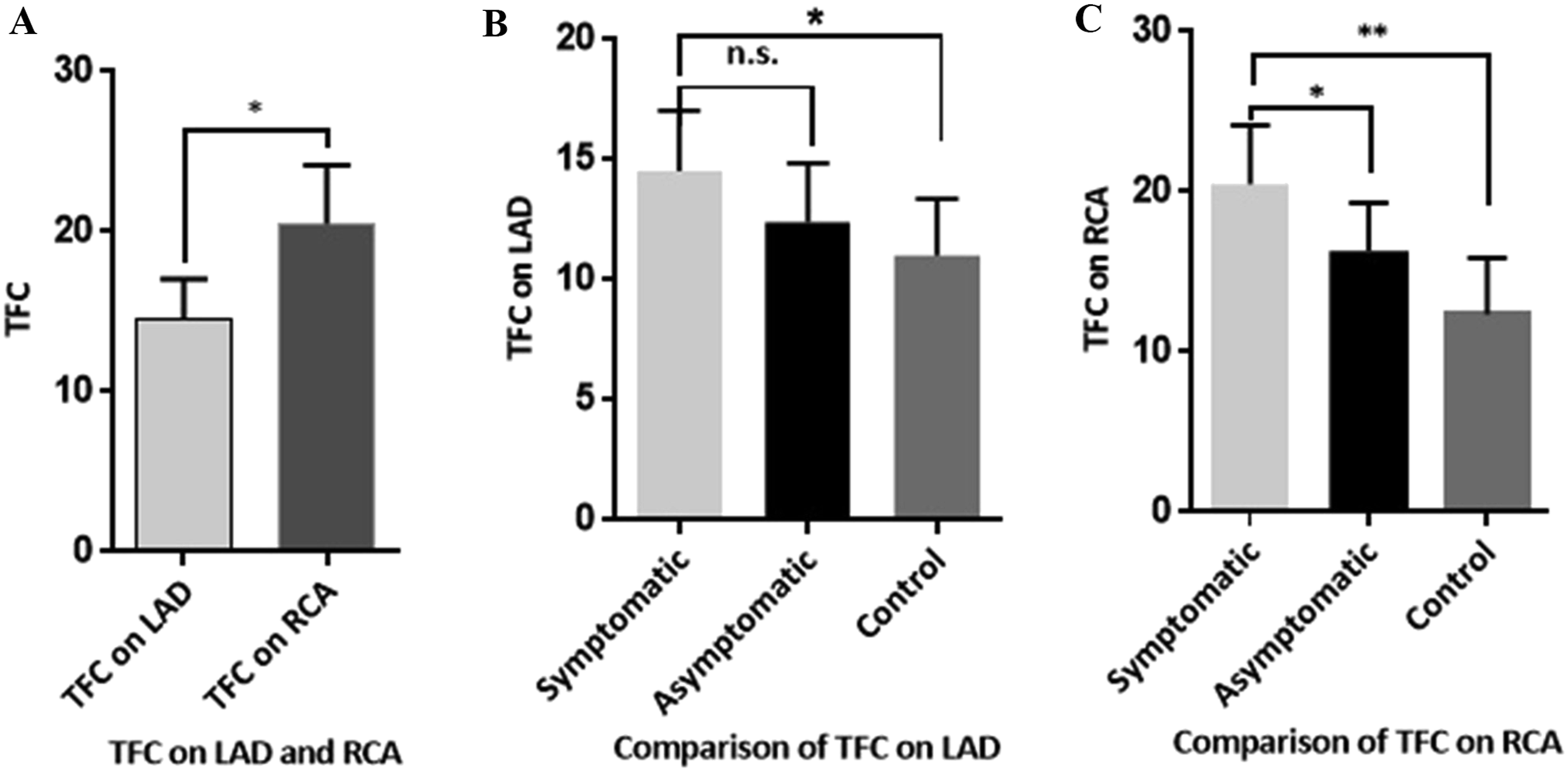
Discussion
The main findings of this study are as follows: 1) The incidence of isolate CAE was significantly higher in males than in females. 2)In symptomatic patients with isolated CAE, lesions are more frequently localized to the RCA, whereas asymptomatic patients more often exhibited involvement of the LAD. 3)Symptomatic patients with isolated CAE have involvement of a greater number of coronary segments than asymptomatic patients. 4)Symptomatic patients with isolated CAE show elevated levels of circulating inflammatory markers. 5)Symptomatic patients with isolated CAE exhibit lower coronary blood flow velocity.
Coronary artery ectasia (CAE) is defined as localised or diffuse dilation of a coronary artery exceeding 1.5 times the diameter of adjacent normal segments.1 Its underlying pathophysiology involves coronary atherosclerosis, chronic inflammation, endothelial dysfunction and vascular smooth muscle cell (VSMC) apoptosis, among other factors.1,16,17 Patients with CAE exhibit a pronounced systemic inflammatory state, characterised by elevated levels of markers such as CRP and IL-6. These factors not only directly damage the endothelium but also activate matrix metalloproteinases (MMPs), particularly MMP-2 and MMP-9, leading to degradation of elastic fibres and smooth muscle structures within the tunica media. 18 Endothelial dysfunction constitutes another critical component: impaired endothelial cells fail to adequately secrete vasodilatory mediators such as nitric oxide (NO), while concurrently promoting a prothrombotic and proinflammatory milieu, thereby increasing vascular fragility. 19 Against this background, excessive VSMC apoptosis deprives the vessel wall of essential structural support, culminating in irreversible dilation under haemodynamic stress. Such pathological changes can lead to adverse clinical consequences, including coronary spasm, thrombosis, dissection and myocardial ischaemia. Notably, even in patients with isolated CAE— who have no concomitant coronary artery stenosis— clinical symptoms such as angina pectoris and chest tightness may still occur.20,21
The clinical manifestations of CAE are diverse yet non-specific, often overlapping with those of concomitant coronary atherosclerosis. Some patients remain asymptomatic, with the condition discovered incidentally during coronary angiography or other imaging examinations. 5 In symptomatic individuals, angina pectoris is the most common presentation, resulting from distal myocardial hypoperfusion caused by turbulent flow, vortex formation, and microthrombus generation within the ectatic segments. 22 Other patients may present with acute coronary syndromes, including unstable angina or even myocardial infarction, typically due to distal embolization following thrombus formation and detachment within the aneurysm. Additionally, the risk of coronary artery spasm may also be elevated in patients with CAE.23,24 Notably, although CAE frequently coexists with atherosclerosis, it can also occur independently as a sequela of vasculitis such as Kawasaki disease, the core pathophysiology of which similarly involves inflammation-driven destruction of the vascular wall. 2 Therefore, a thorough understanding of the complex pathophysiological mechanisms underlying CAE—centered on the inflammation–endothelium–smooth muscle cell axis—is essential for guiding comprehensive therapeutic strategies aimed at anti-inflammation, improvement of endothelial function, and thrombosis prevention. 25
In this study, symptomatic patients with ICAE exhibited involvement of a greater number of coronary segments, significantly elevated levels of circulating inflammatory cytokines such as IL-1β and TNF-α, and markedly reduced coronary blood flow (TFC: 20.31±3.42 vs. 16.72±3.55, p=0.027). The underlying mechanism may involve inflammation-induced impairment of coronary circulation, reflected as slower coronary blood flow, which in turn leads to symptoms of myocardial ischemia such as angina and chest tightness. These findings suggest that activation of the inflammatory response in patients with CAE may represent a potential target for statin therapy. However, whether the anti-inflammatory effects of statins can alleviate clinical symptoms and delay disease progression in patients with CAE remains to be determined by further clinical studies.
Limitations of the study
There were several limitations in the present study. First, owing to the relatively low clinical incidence of isolated CAE and the constraints of a single-centre design, only a limited number of cases were enrolled, and no a priori sample size calculation was performed. The small sample size may have limited our ability to detect weaker but clinically meaningful associations between circulating inflammatory marker levels and clinical symptoms. Consequently, the observed correlation coefficients or risk estimates may lack stability. Future multicentre studies with larger sample sizes and sample size calculations based on expected effect sizes are needed to validate our findings. Second, this study did not present adjusted p-values. The findings of this trial warrant further investigation in larger, multi-center cohorts.
Conclusion
Symptomatic ICAE patients have elevated circulating levels of inflammatory markers such as IL-1β and TNF-α, as well as reduced coronary blood flow. These findings suggest a role for inflammation in the pathophysiology of symptomatic CAE. Although speculative at this stage, the potential anti-inflammatory properties of statins may warrant further investigation as a therapeutic strategy in this condition.
Supplemental material
Supplemental material - Association between clinical features of isolated coronary artery ectasia and circulating levels of inflammatory markers
Supplemental material for Association between clinical features of isolated coronary artery ectasia and circulating levels of inflammatory markers by Junping Ou, Zhijia Zhuo, Zhongwen Liu, Yuping Wang, Jie Zeng, Xiaolin Li and Lingjuan Liu in Sage Open Medicine.
Footnotes
Acknowledgements
We thanks for the participation of all patients in the present study.
Author contributions
Xiaolin Li made the conception and study design, Junping Ou collected and organized the research data, Zhijia Zhuo and Zhongwen Liu conducted the coronary angiography, Yuping Wang and Lingjuan Liu performed blood vessel diameter measurements, Jie Zeng analyzed the data. All authors took part in drafting, revising or critically reviewing the article. Junping Ou, Zhijia Zhuo and Zhongwen Liu contributed equally to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the funds from the National Natural Science Foundation of China ( 82460085), the Natural Science Foundation of Jiangxi Province (20224BAB206014).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.