
Abstract
Objective
We aimed to evaluate factors influencing survival after LDLT in Georgia and to identify underlying causes and strategies for improved outcomes.
Methods
A cross-sectional retrospective study including 103 living donor recipients transplanted
Results
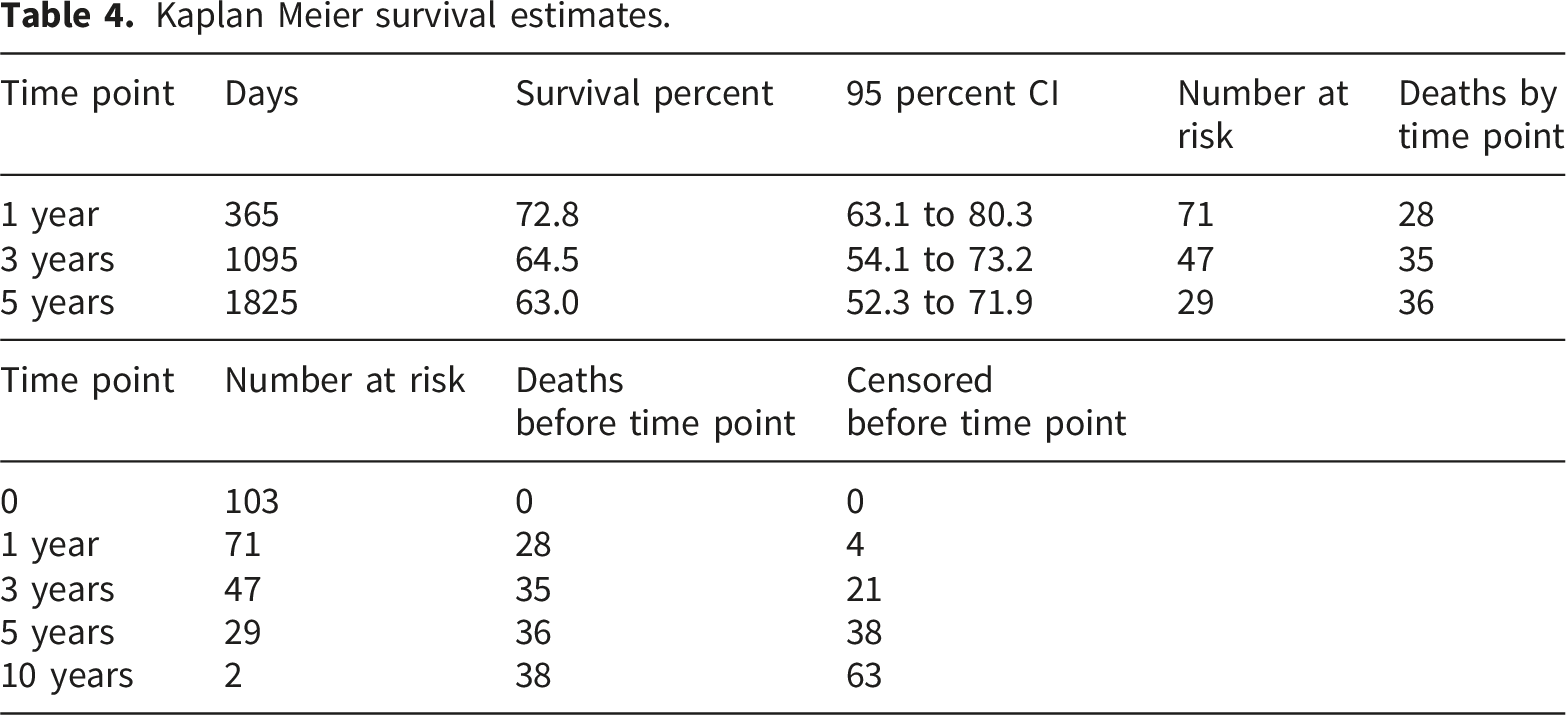
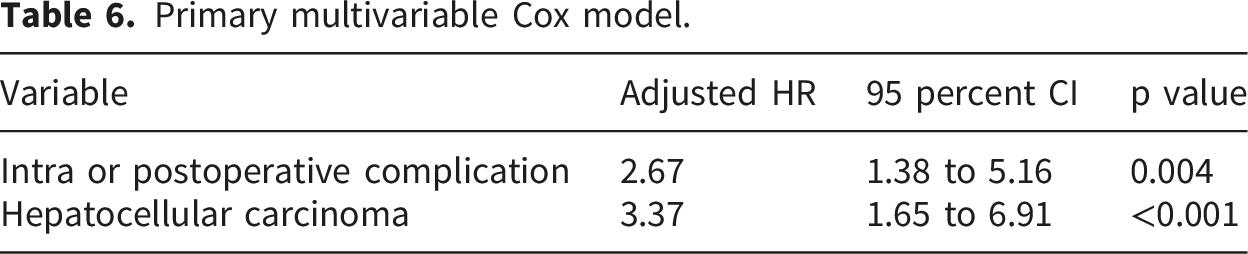
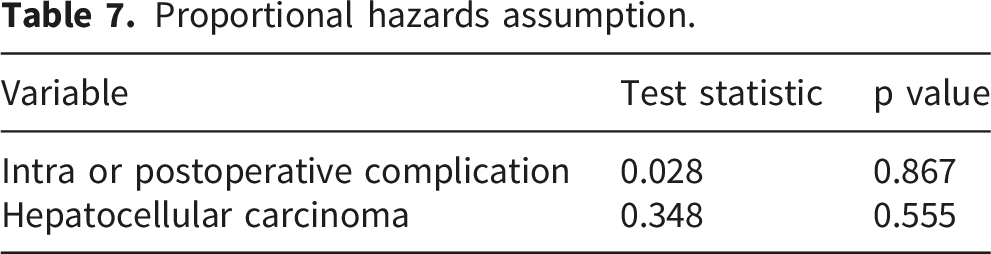
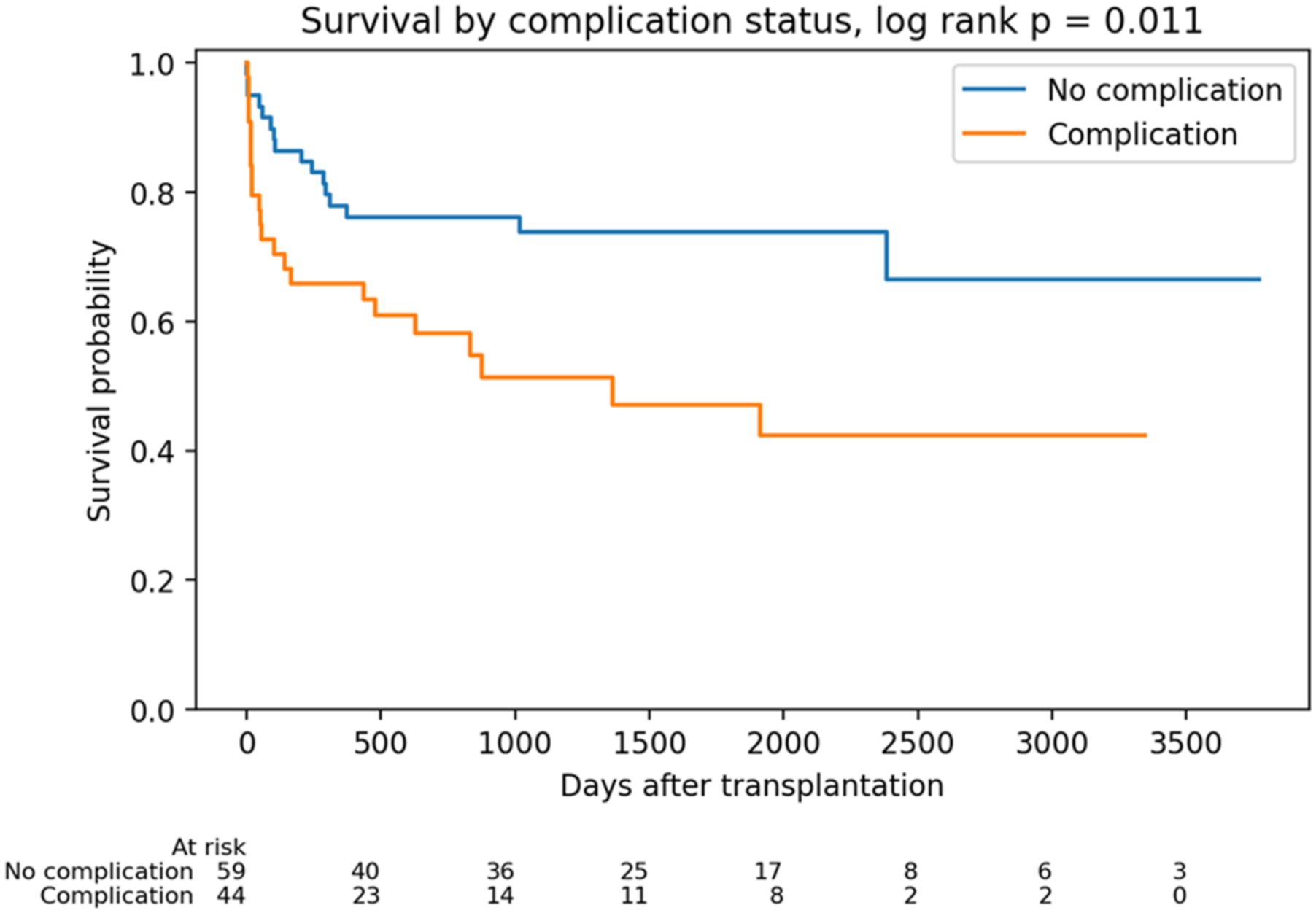
Overall survival (OS) declined significantly during the first post-transplant year. Kaplan Meier estimated patient survival was 72.8 percent at 1 year, 64.5 percent at 3 years and 63.0 percent at 5 years. The number at risk was 71 at 1 year, 47 at 3 years and 29 at 5 years. Among 103 LDLT recipients, 38 deaths occurred and 65 patients were censored alive during follow up. Median observed follow up was 878 days, IQR 286 to 1989. In the primary Cox proportional hazards model, intra or postoperative complications were associated with higher mortality, adjusted HR 2.67, 95 percent CI 1.38 to 5.16, p = 0.004. HCC was also associated with higher mortality, adjusted HR 3.37, 95 percent CI 1.65 to 6.91, p = <0.001. Schoenfeld residual based tests did not indicate violation of the proportional hazards assumption.
Conclusion
This study offers valuable insight into post-transplant LDLT outcomes in Georgia. Identification of key clinical risk factors highlights opportunities for targeted intervention. Given that Georgia’s short-term survival rates remain lower than those reported in high-income countries, optimizing modifiable risk factors may improve long-term outcomes.
Keywords
Introduction
Living Donor Liver Transplantation (LDLT) is a critical life-saving procedure, particularly in countries where cultural or logistical barriers limit the availability of deceased donors. It provides timely access to transplantation for patients presenting with acute and chronic liver failure and hepatocellular carcinoma.1–4 The success of LDLT is known to be influenced by a wide range of variables, which can be broadly categorized into three groups: recipient-related factors (e.g., Model for End-Stage Liver Disease (MELD) score5, age, comorbidities), donor-related factors (e.g., age, graft type), and procedural factors, which include the transplant centre’s experience, surgical complications, and postoperative management.6–9
The outcomes of LDLT have been extensively documented in high-resource settings, establishing international benchmarks for success. Most leading centres report 1-year patient survival rates between 86% and 93%, with 5-year survival typically ranging from 74% to 86%.10–12 These outcomes are achieved despite common challenges, including a high incidence of postoperative complications such as pulmonary, vascular, or biliary, haemorrhagic, and infectious complications.13,14 The management of all these complications, alongside long-term management of comorbidities suchas arterial hypertension and diabetes mellitus, is necessary to optimize the results.15–19
While these survival rates and their influencing factors are well-established from leading centres, there is a significant gap in the literature regarding outcomes in middle and upper-middle-income countries. Data from nations that are actively developing their transplant programmes to meet international standards are crucial for understanding regional challenges, addressing service disparities, and improving equitable access to this life-saving procedure. Examining local data can help identify unique risk profiles and opportunities for tailored quality improvement initiatives that may not be apparent from global reports.
Therefore, this study aimed to evaluate the factors influencing survival after LDLT in Georgia. Through examination of the causes of mortality and analyzing local risk factors, this research looks to identify potential strategies to improve patient care and outcomes at both the clinical and national levels.
Methods
In this retrospective cross-sectional study, we examined the medical records of all adult patients who underwent liver transplantation (N=103) at the Liver Transplant Centre of Batumi University Hospital between December 2014 and July 2024. No additional exclusion criteria were applied unless explicitly stated. Only two cases were performed as emergency procedures, while all others were elective. The study was conducted in full compliance with ethical principles of research. Ethical approval was obtained from the Local Ethics Committee of Batumi Referral Hospital (No. 01/23, dated 23.01.2023). In addition, approval was obtained from the Bioethics Committee of the University of Georgia (UGREC-34-23). This was a retrospective study, and written informed consent was waived. The use of anonymised data from medical records for scientific purposes was approved by the respective ethics committees. The primary endpoint of the study was patient overall survival (OS), measured by survival status (alive or deceased at the end of the follow-up period) and the total survival time calculated in days from the date of transplantation. The predictor variables collected for the analysis were grouped as follows: Sociodemographic and behavioural characteristics (recipient age, sex, nationality, body mass index (BMI), tobacco use, alcohol consumption, and history of intravenous drug use; donor age and sex; graft type; graft-to-recipient weight ratio (GRWR)); Pre-transplant clinical factors (aetiology of the underlying liver disease, MELD score at the time of transplant, hepatocellular carcinoma, and the presence of major liver-related complications (ascites, hepatic encephalopathy, oesophagogastric varices, hepatorenal syndrome); Peri and postoperative factors (length of surgery, hospital stay, and occurrence of intra- or postoperative complications). The complications included in this study refer to postoperative events occurring within ≤30 days and were observed in 44 patients (42.7%).
Statistical analysis
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Chicago, IL, USA). Continuous variables were assessed for normality and are presented as mean ± standard deviation (SD) when normally distributed, or as median and interquartile range (IQR) when non-normally distributed. Categorical variables are presented as frequencies and percentages. Overall survival (OS) was defined as the time from liver transplantation to death from any cause or censoring at the date of the last available follow-up. Survival probabilities at 1, 3, and 5 years were estimated using the Kaplan-Meier method. Cox proportional hazards regression analysis was performed to identify factors associated with mortality, and hazard ratios (HRs) with 95% confidence intervals (CIs) were reported. The proportional hazards assumption was evaluated using Schoenfeld residual-based tests. A two-sided p-value<0.05 was considered statistically significant.
Results
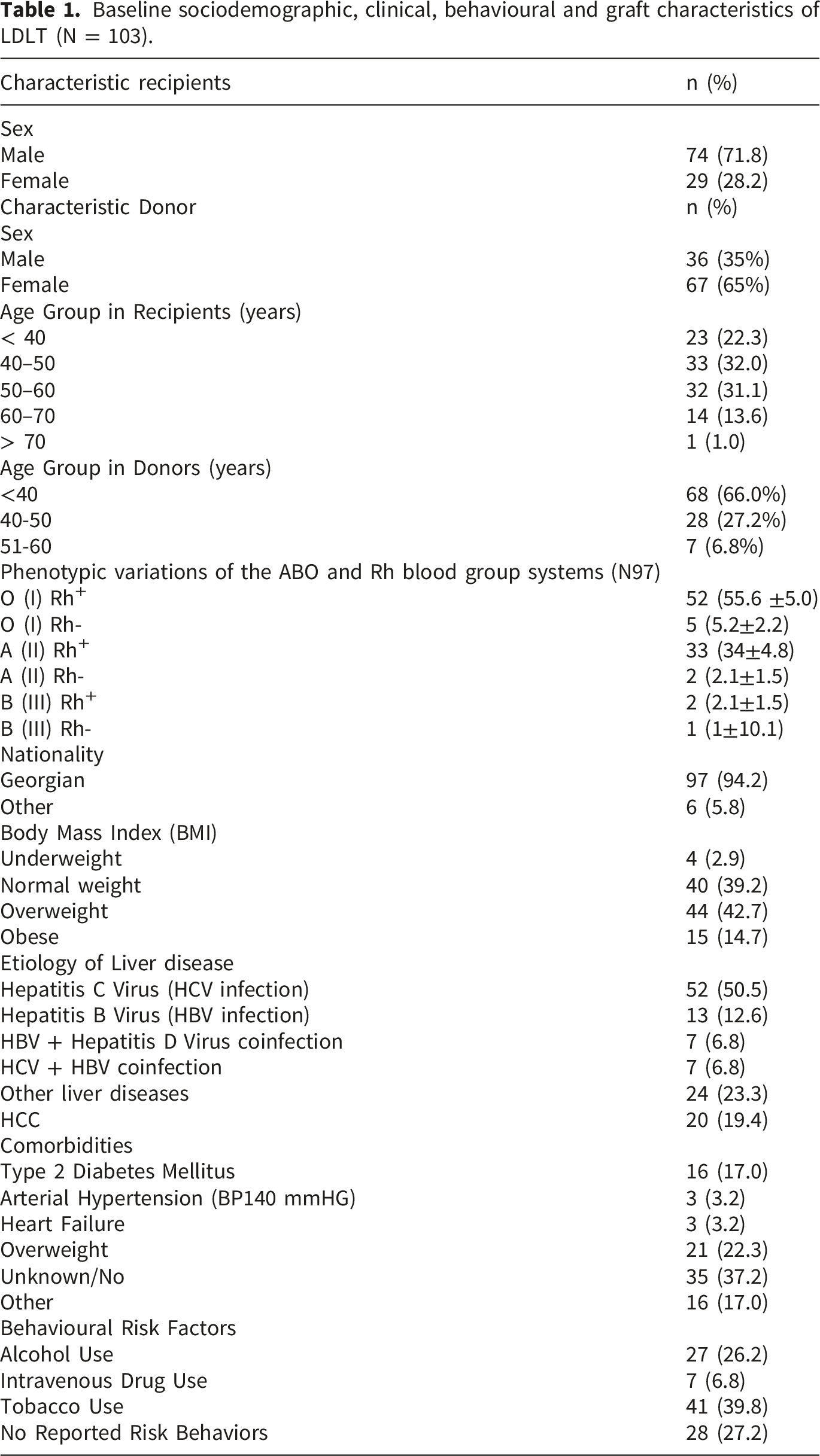
The study included 103 LDLT recipients, of whom 74 (71.8%) were male and 29 (28.2%) were female. The age distribution was as follows: <40 years (22.3%), 40–50 years (32.0%), 50–60 years (31.1%), 60–70 years (13.6%), and >70 years (1.0%). Most participants were Georgian nationals (94.2%).
Baseline sociodemographic, clinical, behavioural and graft characteristics of LDLT (N = 103).
Clinical severity, transplant details, and liver-related complications (N = 103).
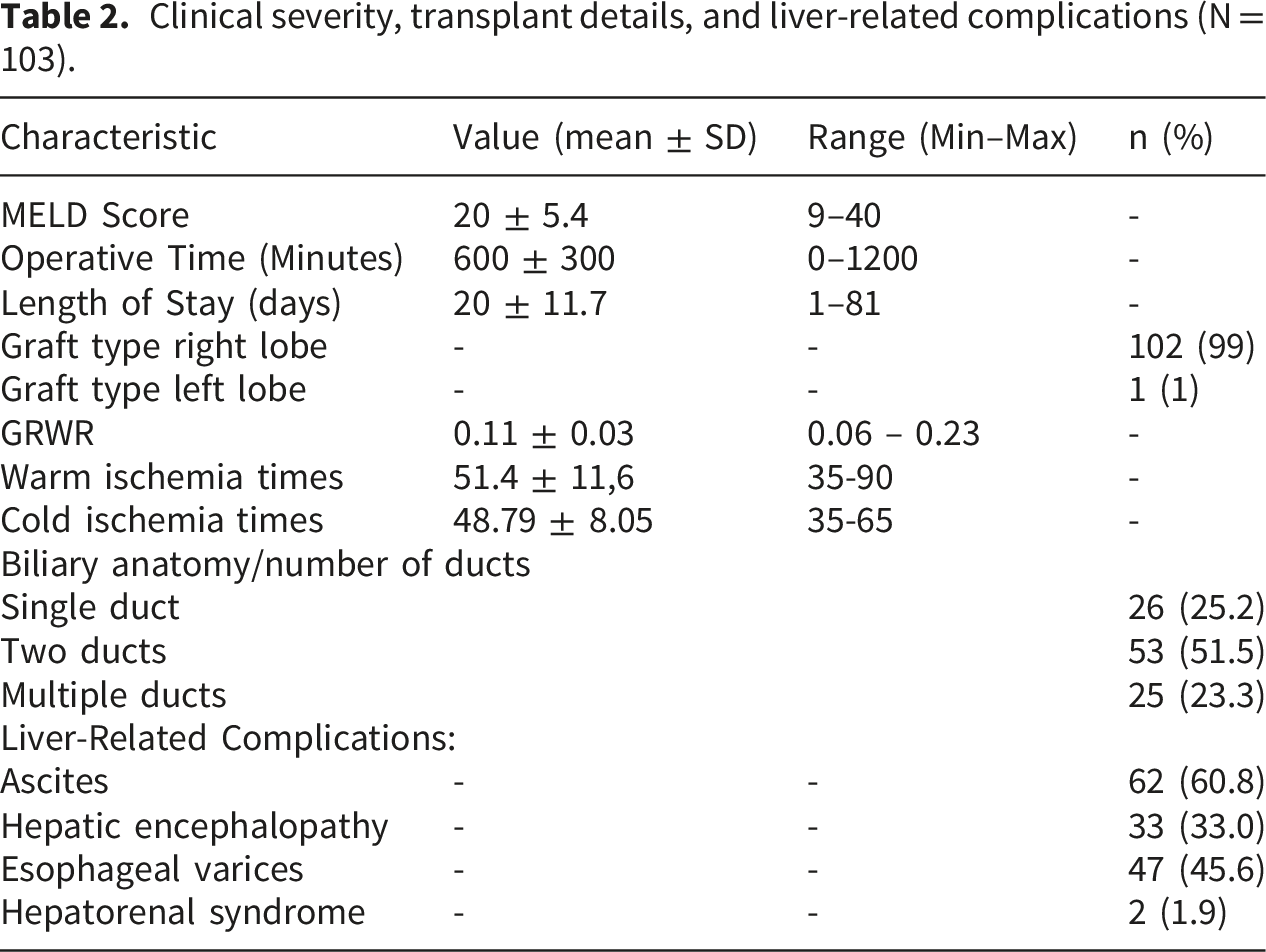
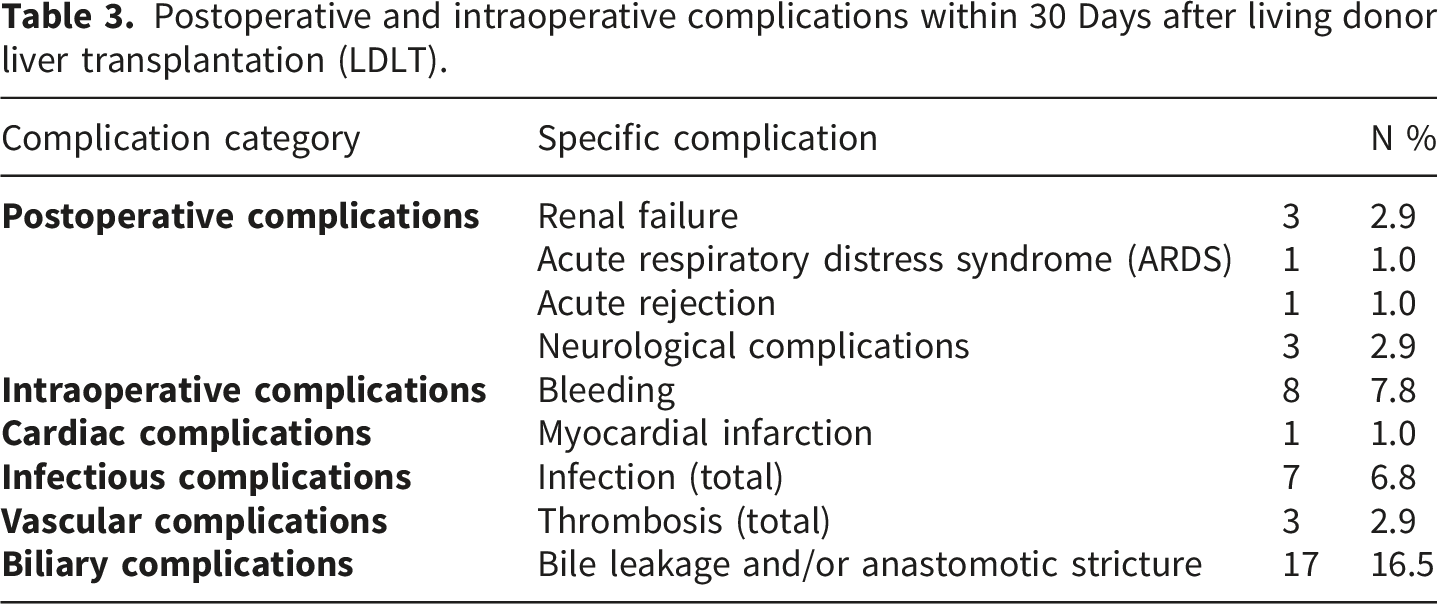
The complications included in this study refer to postoperative events occurring within ≤30 days and were observed in 44 patients (42.7%). Renal failure was identified in 3 patients (2.9%), acute respiratory distress syndrome (ARDS) in 1 patient (1.0%), acute rejection in 1 patient (1.0%), and neurological complications in 3 patients (2.9%). Among intraoperative complications, bleeding occurred in 8 patients (7.8%), including 2 cases of uncontrolled hemorrhage requiring temporary interruption of the procedure. Myocardial infarction was recorded in 1 patient (1.0%). Infectious complications were observed in 5 patients (4.9%), including 2 intraoperative cases (1.9%), in which hemodynamic instability persisted despite vasopressor support, requiring escalation to intensive antibiotic therapy. Vascular thrombosis occurred in 3 cases (2.9%), including 2 portal vein thromboses and 1 arterial thrombosis. In cases of portal vein thrombosis, relaparotomy was performed, whereas arterial thrombosis was managed conservatively. The most common postoperative complication was biliary tract complications (N = 17; 16.5%), manifested by bile leakage followed by anastomotic stricture formation. Despite the heterogeneity of complications, due to the limited cohort size, the analysis primarily focused on overall complication frequencies.
Postoperative and intraoperative complications within 30 Days after living donor liver transplantation (LDLT).
Kaplan Meier survival estimates.
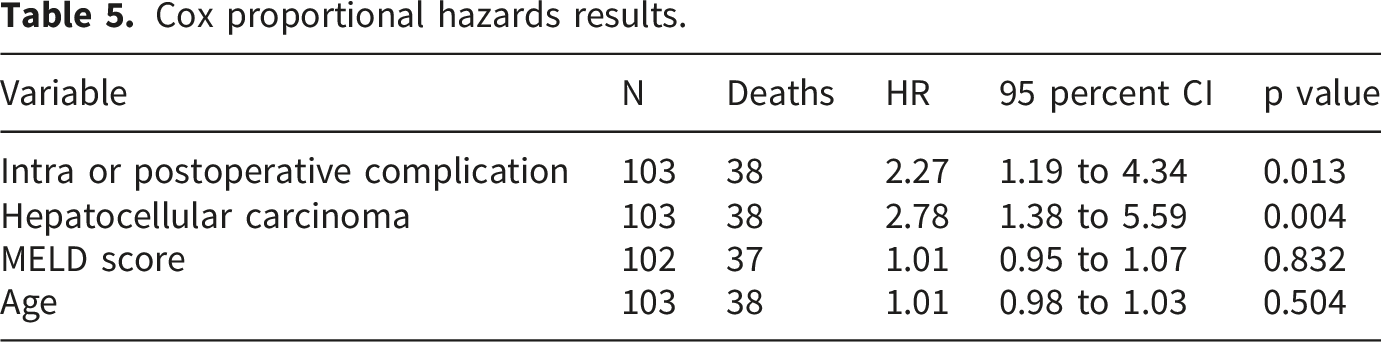
Cox proportional hazards results.
Primary multivariable Cox model.
Proportional hazards assumption.
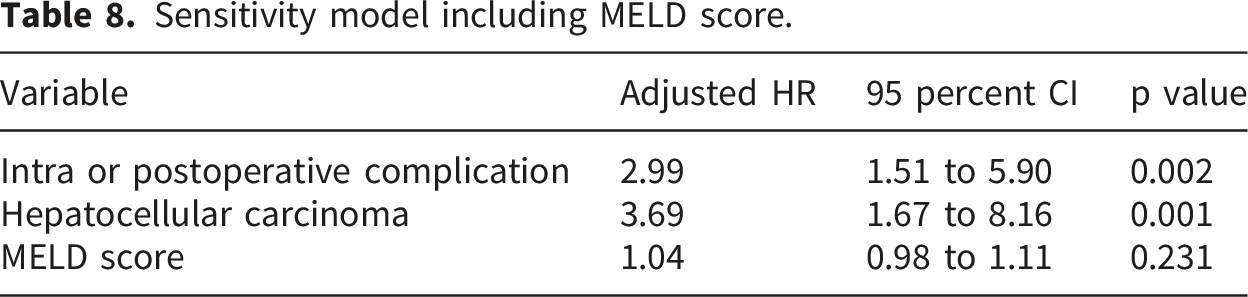
Sensitivity model including MELD score.
Among 103 LDLT recipients, 38 deaths occurred and 65 patients were censored alive during follow up. Median observed follow up was 878 days, IQR 286 to 1989. Kaplan Meier estimated survival was 72.8 percent at 1 year, 64.5 percent at 3 years and 63.0 percent at 5 years. In the primary Cox proportional hazards model, intra or postoperative complications were associated with higher mortality, adjusted HR 2.67, 95 percent CI 1.38 to 5.16, p = 0.004. HCC was also associated with higher mortality, adjusted HR 3.37, 95 percent CI 1.65 to 6.91, p = <0.001. Schoenfeld residual based tests did not indicate violation of the proportional hazards assumption (Figures 1–3). Overall Kaplan Meier survival curve with number at risk. Kaplan Meier survival by HCC status with number at risk. Kaplan Meier survival by intra or postoperative complication status with number at risk.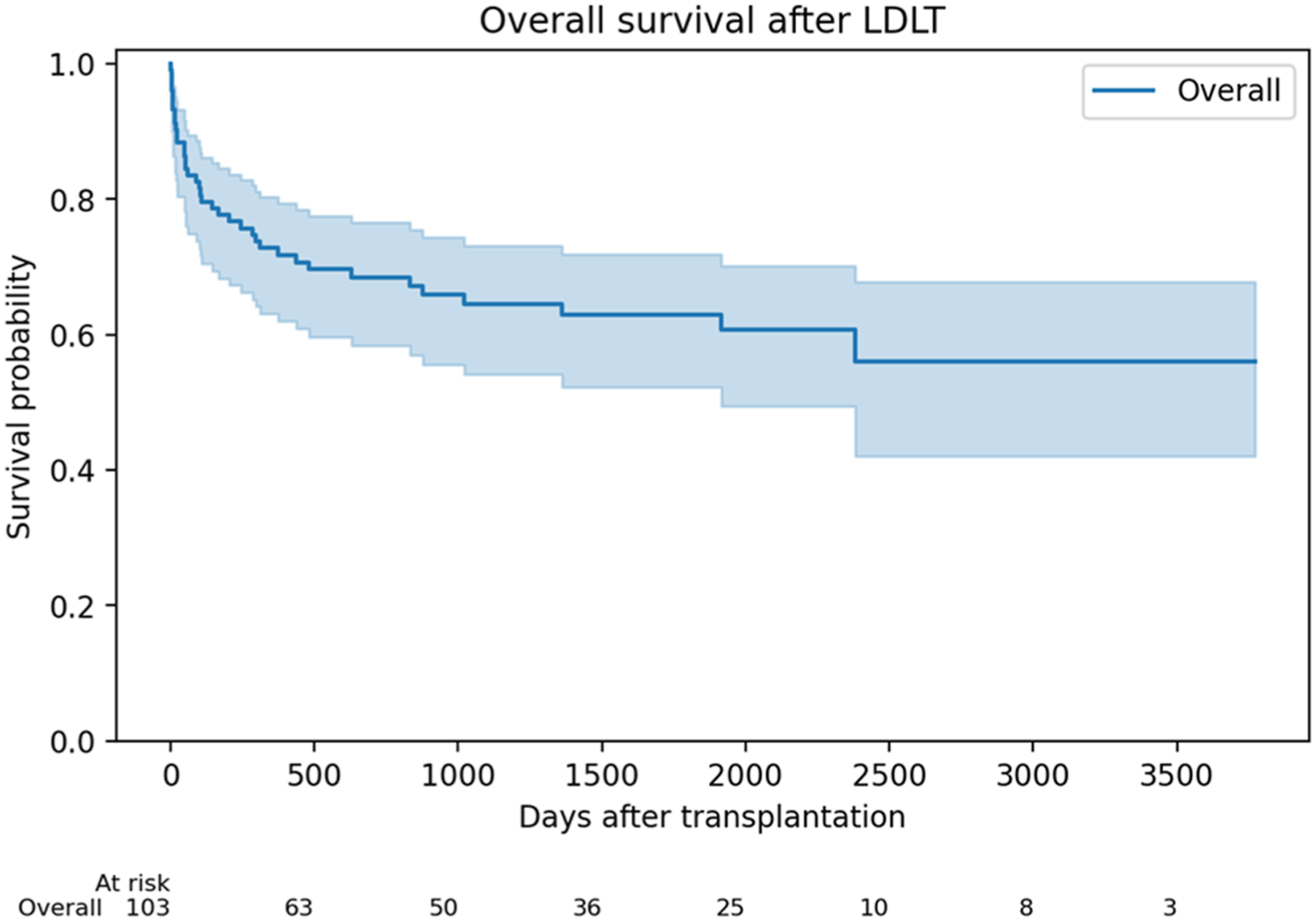

Discussion
The two principal findings of this study are the significant impact of intra- and postoperative complications and the pre-transplant diagnosis of hepatocellular carcinoma (HCC) on reduced post-transplant survival. These results suggest that perioperative surgical quality and oncological disease burden remain the most critical determinants of outcomes in this cohort. Postoperative complications likely reflect both technical complexity and perioperative management challenges, whereas HCC indicates a more advanced disease biology and an increased risk of recurrence or decompensation after transplantation. Notably, several established risk factors commonly reported in other populations such as MELD score and recipient age were not significantly associated with mortality in this study. This may reflect the relatively homogeneous clinical characteristics of the cohort or differences in case selection and programme maturity during the study period.
When compared with international benchmarks, the 1-year survival rate in this cohort is lower than the 85-90% reported by high-volume LDLT centres worldwide. This discrepancy underscores the challenges faced by an evolving transplant programme and highlights the importance of continuously analyzing clinical outcomes to identify areas for improvement.
Development of liver transplantation services in Georgia has been shaped by two major systemic changes. First, a 2016 legislative amendment broadened donor eligibility by allowing emotionally related individuals-rather than only genetically related donors—to serve as potential living donors. Second, since 2018, full state funding for liver transplantation has significantly improved access to care. Parallel to these policy changes, refinements in surgical technique were gradually introduced. In the early phase of the programme, interrupted biliary anastomoses were standard practice and were associated with a higher rate of biliary complications. Transitioning to continuous anastomotic techniques subsequently reduced both the incidence and severity of bile leakage.
With increasing experience, operative times decreased significantly. Procedures that initially lasted more than 15 hours have now stabilized at approximately 9-11 hours, with the anhepatic phase typically lasting 60-90 minutes. These improvements reflect not only technical progress but also optimization of perioperative workflows and team coordination. The study’s findings highlight opportunities for improvement in perioperative care protocols, intensive care infrastructure, and the management of complex surgical cases. The strong association between HCC and poorer outcomes aligns with global literature and emphasizes the need for robust pre-transplant screening and tailored management strategies for high-risk oncology patients. Hepatitis C virus infection remained the leading indication for transplantation. Despite the significant success of Georgia’s national HCV elimination programme, a subgroup of patients continues to progress to end-stage liver disease due to long-standing infection. This observation underscores the ongoing necessity of ensuring timely referral of patients with advanced fibrosis to specialized liver centres. As the largest single-centre experience in Georgia, this retrospective analysis provides valuable insight into factors influencing patient outcomes after LDLT and establishes a foundation for future research and evidence-based policy development. Peri- and post-transplant protocols including psychosocial evaluation and support must continue to be refined to advance outcomes in this complex field of medicine. The broader implications of these findings extend to national healthcare planning. With the prevalence of viral hepatitis declining, emerging liver disease etiologies-such as alcohol-associated liver disease, non-alcoholic fatty liver disease, and primary liver cancer are expected to become increasingly important. Proactive establishment of screening and referral pathways will be essential for timely identification of transplantation candidates. Continued progress will require a multidisciplinary strategy aimed at improving surgical techniques, optimizing pre- and postoperative management, strengthening long-term follow-up, and integrating transplant care into primary healthcare services. Future prospective, multicentre studies will be necessary to validate these findings and refine risk prediction in the Georgian LDLT population.
This study has several limitations. Its retrospective single-centre design introduces inherent risks of selection and information bias. The analysis lacked detailed grading of intra- and postoperative complications and comprehensive staging of hepatocellular carcinoma. Temporal changes in surgical technique and perioperative management were also not formally analyzed, which may have influenced outcomes over the 10-year study period. Finally, the relatively small sample size limits statistical power for subgroup analyses and restricts generalizability to other transplant programmes.
Conclusion
This single-centre study provides valuable insight into LDLT outcomes in Georgia and identifies key clinical predictors associated with post-transplant survival. The findings highlight the significant impact of intra- and postoperative complications, as well as pre-transplant HCC, on patient prognosis. These results underscore the importance of optimizing perioperative management and strengthening selection and monitoring strategies for recipients. Continued refinement of surgical techniques, postoperative care pathways, and institutional protocols may contribute to improve outcomes in the future. Further prospective and multicentre studies are warranted to validate these observations and support the development of evidence-based practices within the national transplant programme.
Footnotes
Acknowledgments
We gratefully acknowledge the Transplantation Center team and the donors for their heroic contribution. We would like to express our special gratitude to Shota Rustaveli National Science Foundation of Georgia for financial support during doctoral research. (Competition for funding doctoral educational programs - PHDF-22-2975). Also, we wish to acknowledge support from the University of California, San Francisco’s International Traineeships in AIDS Prevention Studies (ITAPS), U.S. NIMH, R25MH123256. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author contributions
Marika Mortuladze: Data collection; manuscript drafting; review and final approval of the manuscript. Sophio Beridze: Data collection and investigation; provision of study materials (Batumi University Hospital). George Kamkamidze: Study design; implementation of the research; data analysis and interpretation. Kakhaber Kashibadze: Provision of study materials and resources (Batumi University Hospital); clarification and verification of all necessary clinical details from medical records. Lela Shengelia: Study conception; supervision of the project; critical revision of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by Shota Rustaveli National Science Foundation (PHDF-22-2975).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.