
Abstract
Introduction
Bowel obstruction is a major surgical emergency associated with considerable postoperative morbidity and mortality, particularly in low-resource settings. Evidence on surgical outcomes in Ethiopia remains inconsistent. This systematic review and meta-analysis aimed to estimate the pooled magnitude of poor surgical treatment outcomes of bowel obstruction and identify associated factors.
Methods
A comprehensive search of PubMed, Cochrane Library, HINARI, AJOL, and google scholar was conducted. Observational studies reporting surgical outcomes among Ethiopian patients with bowel obstruction were included. Poor surgical outcomes were identified as postoperative complications and/or death in the hospital. A random effect meta-analysis model was used to calculate pooled prevalence and pooled odds ratios with 95% confidence intervals. Heterogeneity and publication bias were assessed using standard statistical methods.
Result
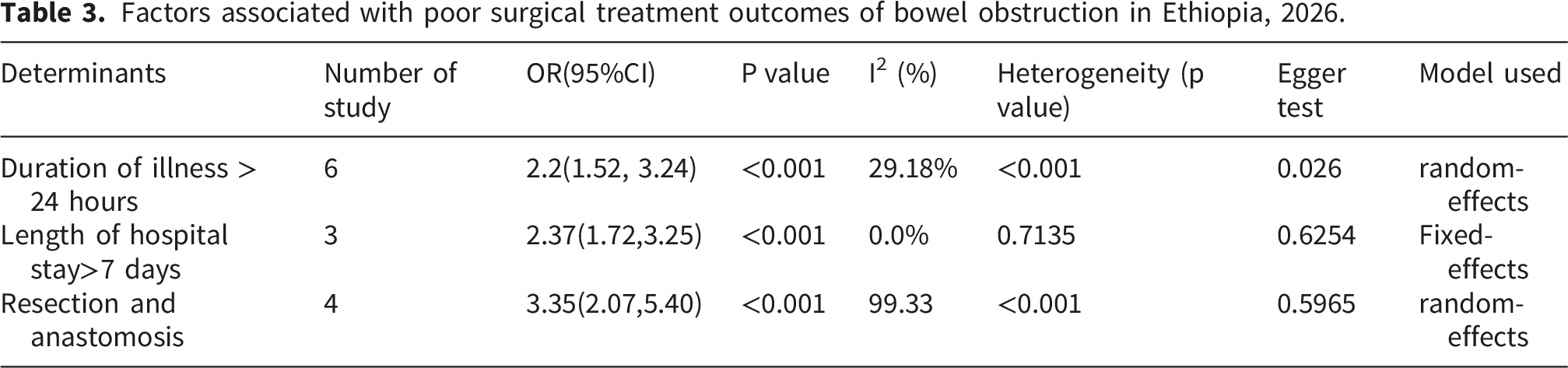
Twenty-one studies comprising 5,429 patients were included. The pooled prevalence of poor surgical treatment outcomes in Ethiopia was 24% (95% CI: 19%-28%), with substantial heterogeneity (I2=93.6%). Delayed hospital presentation (>=24hours) (OR=2.2; 95% CI: 1.52-3.24), hospital stay >7 days (OR=2.37; 95%CI 1.72-3.25), and undergoing resection and anastomosis (OR=3.35; 95% CI: 2.07-5.4) were significantly associated with poor outcomes.
Conclusion and recommendations
The prevalence of poor surgical treatment outcomes of bowel obstruction in Ethiopia was relatively high. Early presentation, timely intervention, and strengthening perioperative care are critical to improving surgical outcomes.
Introduction
Intestinal obstruction exists when blockage prevents the normal flow of intestinal contents through the intestinal tract. 1 There are two types of processes: mechanical and functional. Mechanical obstruction occurs when extrinsic or intrinsic lesions block intestinal lumen. Functional process is intestinal musculature cannot propel the contents along the bowel either due to interruption of innervation or vascular supply to the bowel2,3.
Most obstructions occur in the small intestine. Adhesions, hernia, and tumor account for 90% of obstructions in the small intestines 4 . The most common causes of large bowel obstruction are cancer (60%), diverticular disease (20%), and volvulus (5%). Other causes of large bowel obstruction include benign tumors, strictures, and obstipation or fecal impaction 5 .
Patients with large bowel obstruction experience weakness, weight loss, and anorexia. Eventually, the abdomen becomes markedly distended, loops of large bowel become visibly outlined through the abdominal wall, and the patient has crampy lower abdominal pain 5 . Approximately 25% of patients with obstruction will need surgical intervention 4 .
Although a previous systematic review and meta-analysis assessed surgical outcomes of bowel obstruction, several gaps remain. The earlier review included limited number of studies which may be insufficient given the larger volume of relevant research and newly published evidence in this area. Moreover, several recent primary studies have emerged that were not included in the previous meta-analysis, indicating the need for more up-to-date and comprehensive synthesis. Therefore, the primary aim of the proposed systematic review and meta-analysis is to comprehensively evaluate the prevalence of poor surgical treatment outcomes in patients with bowel obstruction and its associated factors. This approach will help address gaps in the current evidence base and better inform clinical decision-making and future research priorities 6 .
Study design and reporting
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria were followed in the execution of this systematic review and meta-analysis. The protocol was developed and registered in the PROSPERO database under registration number CRD420261386499.
Eligibility criteria
Cross-sectional, case-control, and cohort observational studies that described the surgical results of intestinal blockage among Ethiopian patients were considered in this review. Studies that assessed poor surgical outcomes defined as peri-operative complications, morbidity, or mortality were eligible. Although only English-language articles were included, no articles published in other languages were found. Case reports, reviews, editorials, conference papers, and studies with insufficient outcome data were all removed. Studies that were carried out outside of Ethiopia or that exclusively addressed the non-surgical treatment of intestinal obstruction were excluded from consideration.
Searching strategy
A comprehensive search using PubMed, the Cochrane Library, HINARI, African Journals Online (AJOL), and Google Scholar, was carried out. “Bowel obstruction,' “intestinal obstruction,' “surgical outcome,' “postoperative complication,' “mortality,' and “Ethiopia' were among the keywords and Medical Subject Headings (MeSH). Terms were combined using boolean operators (AND, OR). To find other relevant studies, the reference lists of the included studies were further investigated.
Study selection
All identified articles were exported into reference management software, and duplicates were removed. Two independent reviewers screened titles and abstracts for relevance. Full texts of potentially eligible articles were retrieved and assessed against the exclusion and inclusion criteria. Disagreements between reviewers were resolved through discussion and, when necessary, by consultation with a third reviewer.
Data extraction
Data were extracted independently by two reviewers using a standardized and pretested data extraction form. The data were collected from February 2, 2025 to February 15, 2025. Information collected from included study comprised the first authors’ name, year of publication, study region, sample size, study design, and patient characteristics. In addition, details on the definition of poor surgical treatment outcome, the magnitude of poor treatment outcomes and reported associated factors along with their corresponding effect size (odds ratio) were extracted. Any discrepancies between reviewers during data extraction were resolved through discussion.
Outcome definition
The primary outcome of this review was poor surgical treatment outcome, defined as the occurrence of one or more adverse events, including postoperative complications and/or in-hospital or postoperative mortality among patients undergoing surgical treatment for bowel obstruction. Post-operative complications included surgical site infection, anastomotic leak, and sepsis. Given the variability in outcome definitions across the included studies, the original definitions reported by each study were retained and categorized under this composite outcome.
Quality assessment
The methodological quality of the included studies was assessed using Newcastle–Ottawa Scale (NOS) critical appraisal checklists appropriate for each study design, including cross-sectional studies 7 . Based on the appraisal results, each study was categorized as having low risk of bias(high quality), moderate risk of bias, or high risk of bias(low quality). Only studies judged to have acceptable methodological quality were included in the final meta-analysis. Any disagreements between reviewers during quality assessment were resolved through discussion.
Data analysis and statistical analysis
Meta-Analysis was performed using a random-effects model to account for between-study variability. The pooled magnitude of poor surgical treatment outcomes was calculated along with corresponding 95% confidence intervals. For associated factors, pooled odds ratios with 95% CI were computed for determinants reported in two or more studies. Statistical heterogeneity among studies was assessed using Cochran’s Q test and quantified using I2 statistic.
Publication bias was evaluated through visual inspection of funnel plots and formally tested using Egger’s regression test. In addition, trim-and-fill analysis was performed when appropriate to assess the potential impact of unpublished studies on the pooled estimates. Subgroup analysis was conducted to explore potential source of heterogeneity based on study region, year of publication and sample size. Sensitivity analysis was also performed to examine the robustness of the pooled estimates by assessing the influence of individual’s studies on the overall result.
Results
Study selection for included studies
Overall, 29,125 articles were retrieved from online data base. After being exported to Endnote 7 reference managers, 11,234 duplicates were removed. An additional 5,434 were removed by automated tools, and 1,234 articles were removed for other reasons. Then, 11,223 records were screened, of which 11,132 were excluded after title and abstract screening. A total of 91 full text articles were assessed for eligibility, but 64 could not be obtained. The remaining 27 full-texts articles were assessed for eligibility, of which 6 were excluded because they did not report surgical outcomes in adult patients. Finally 21 studies met the inclusion criteria and were included in this systematic review and meta-analysis (Figure 1). PRISMA flow diagram of study selection for Magnitude and Determinants of poor surgical Treatment outcomes of Bowel Obstruction in Ethiopia: A systematic review and Meta-Analysis.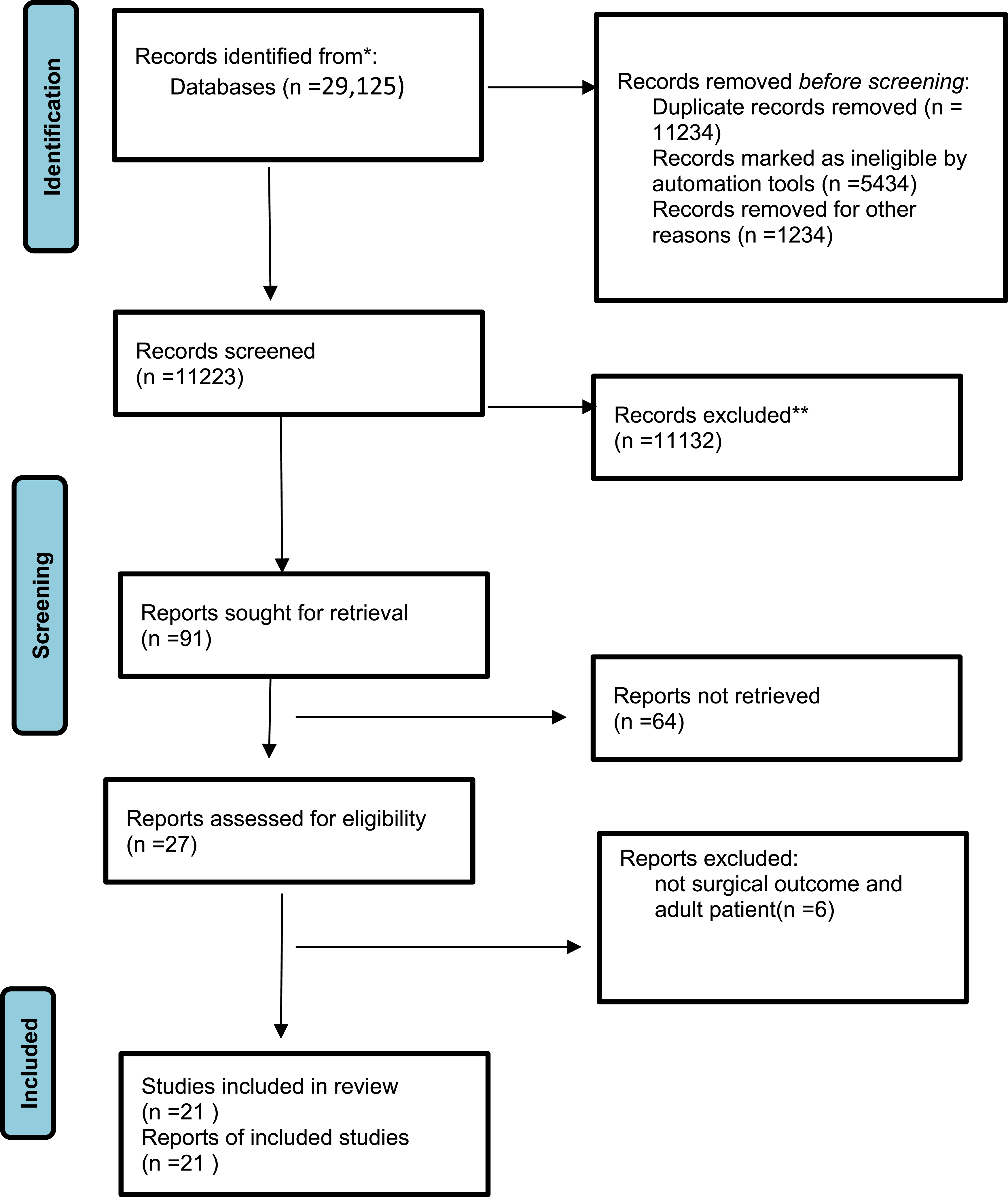
Characteristics of the included studies
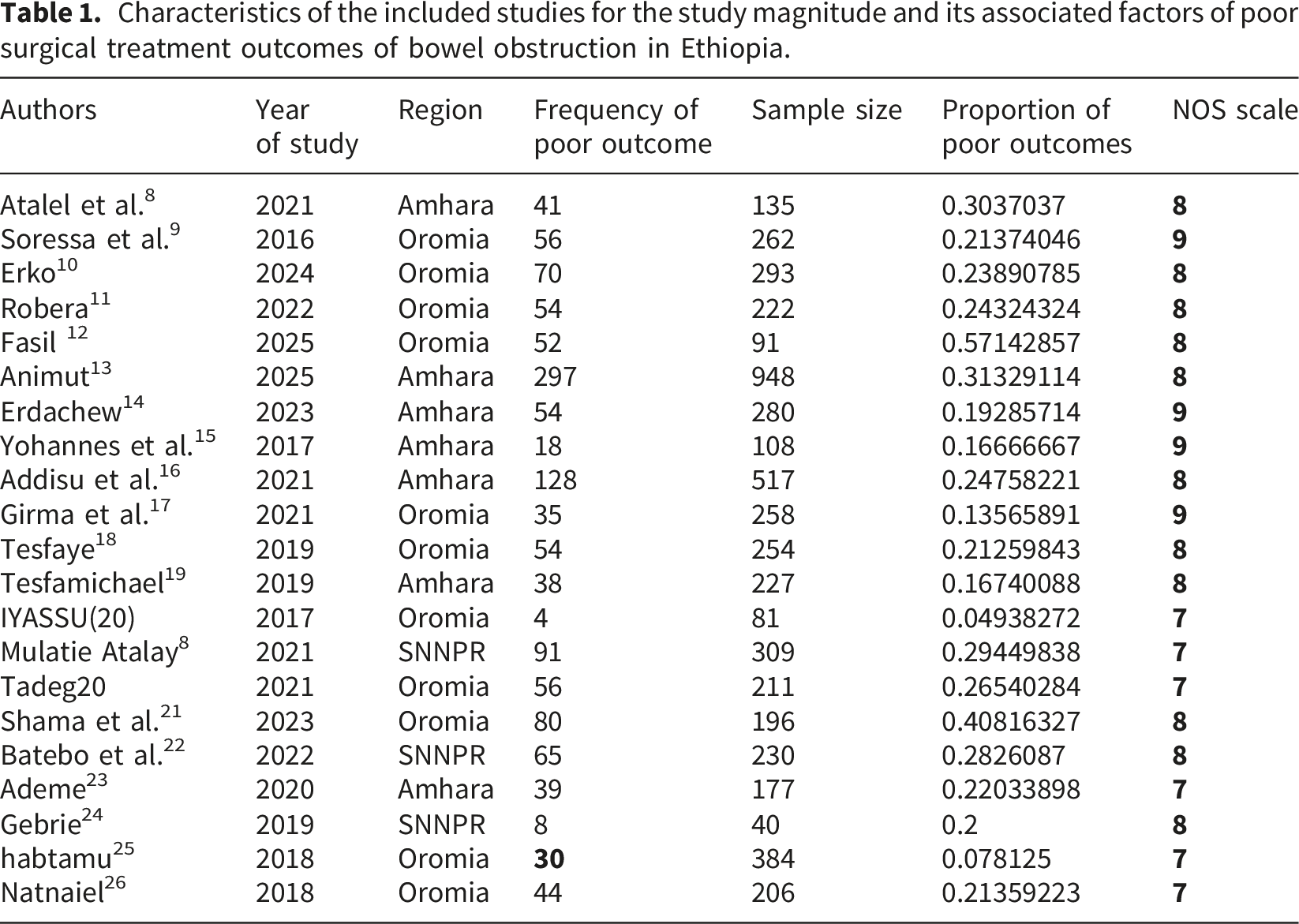
Characteristics of the included studies for the study magnitude and its associated factors of poor surgical treatment outcomes of bowel obstruction in Ethiopia.
Pooled poor surgical outcomes
A total of 21 studies were included in the meta-analysis to estimate the pooled magnitude of poor surgical treatment outcomes among patients with bowel obstruction in Ethiopia. Using random-effects model, the pooled prevalence of poor surgical treatment outcomes was 24% (95% CI: 19%-28%). There was substantial heterogeneity among the included studies (I2=93.63%), indicating considerable variability in study estimates (Figure 2). Forest plot showing the pooled Magnitude of poor surgical Treatment outcomes of Bowel Obstruction in Ethiopia.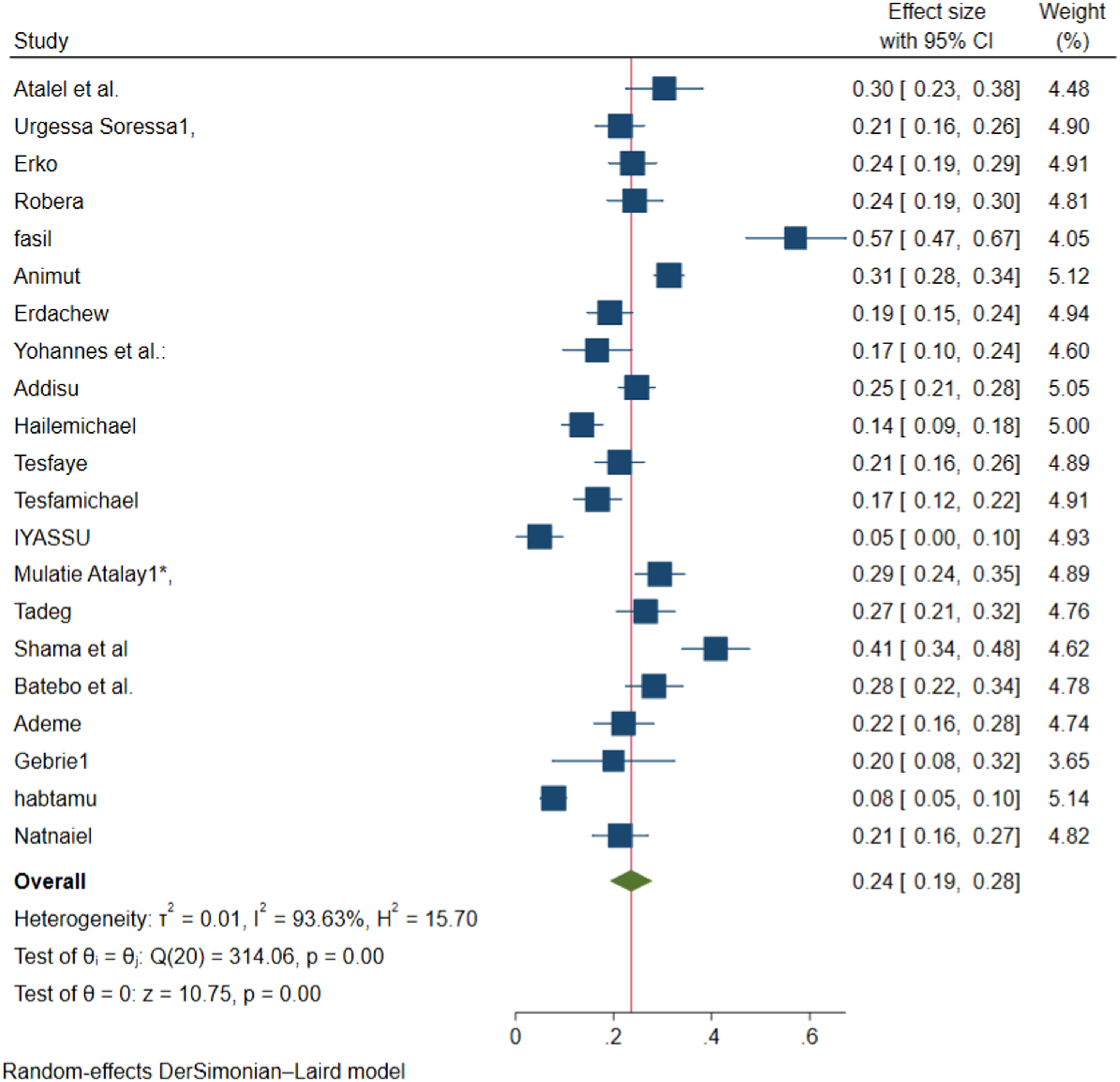
Publication bias
Visual inspection of the funnel plot suggested asymmetry, indicating possible publication bias. This was statistically supported by Egger’s regression test under a random-effects model, which demonstrated small-study effects (p=0.02). A nonparametric trim-and-fill analysis using a random-effects model was performed to assess potential impact of publication bias. The analysis did not impute any missing studies on the left side of the funnel plot. This suggests, despite evidence of small study effects from Eggers test, publication bias is unlikely to have materially influenced the pooled estimate (Figure 3). Funnel plot for the study poor surgical treatment outcomes of bowel obstruction in Ethiopia, 2026.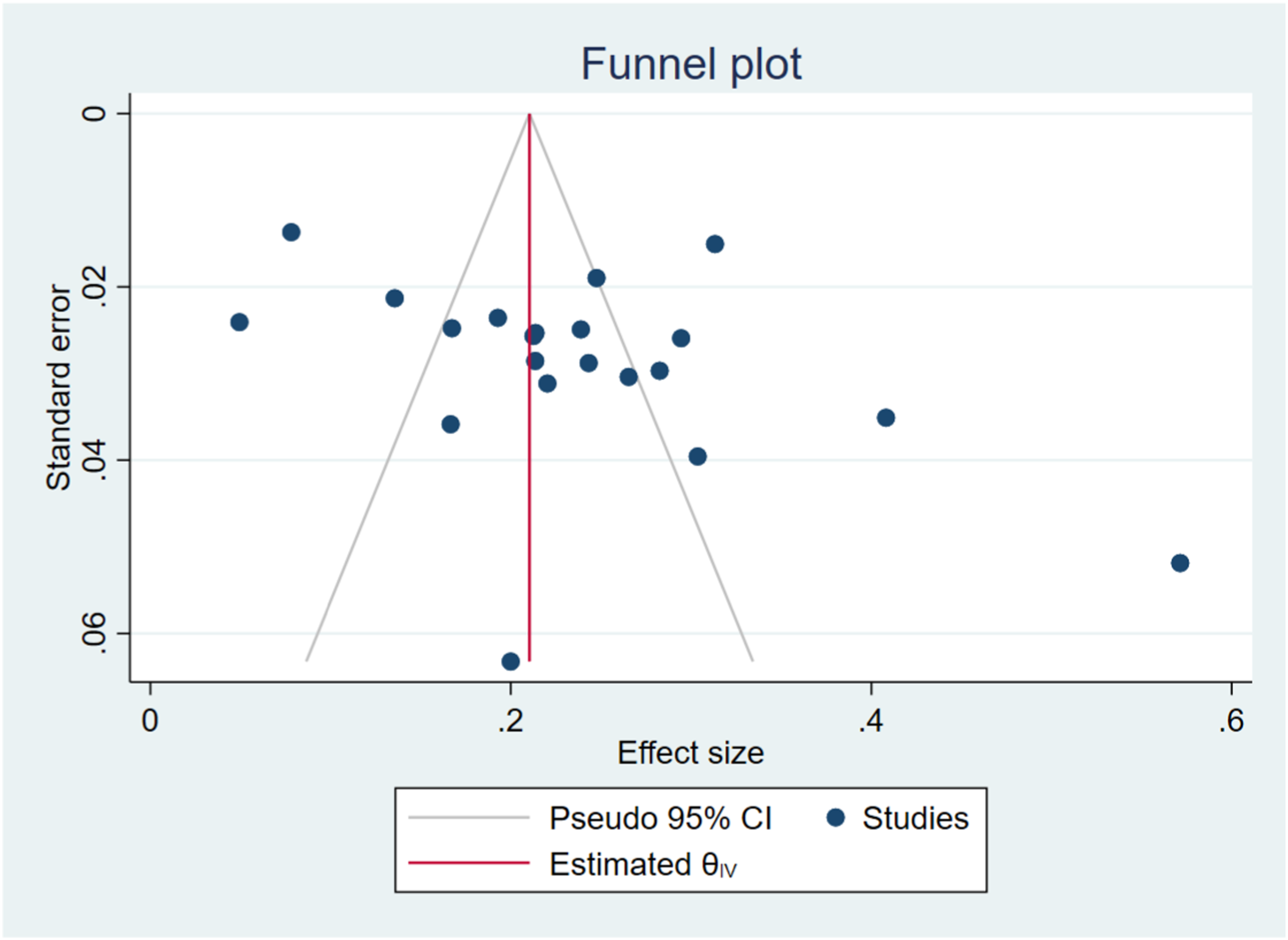
Sensitivity analysis
Leave-one-out sensitivity analysis showed that omitting any single study did not substantially change the pooled effect size of poor surgical outcomes of bowel obstruction in Ethiopia (Figure 4). Sensitivity analysis showing poor surgical treatment outcomes of bowel obstruction in Ethiopia.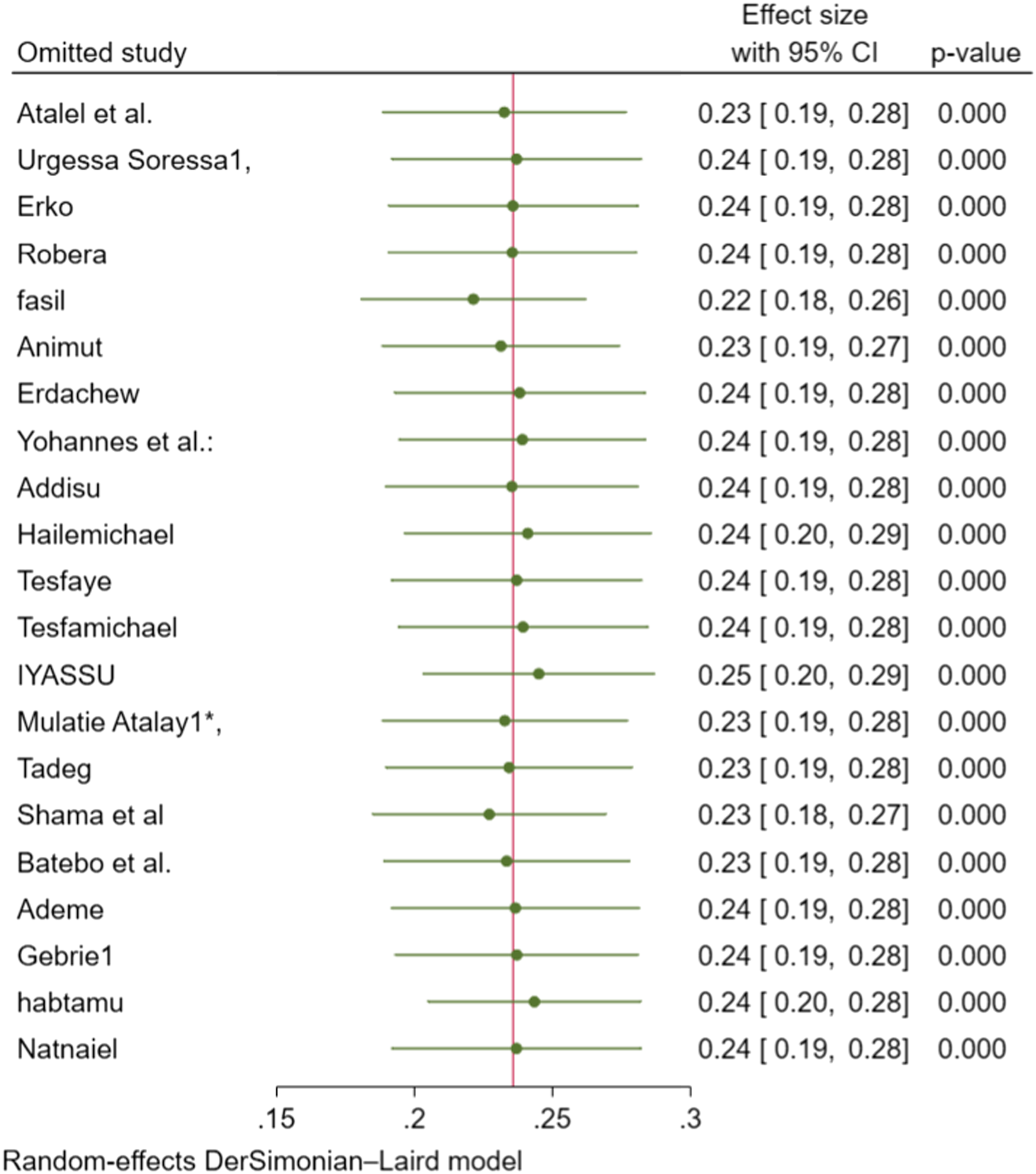
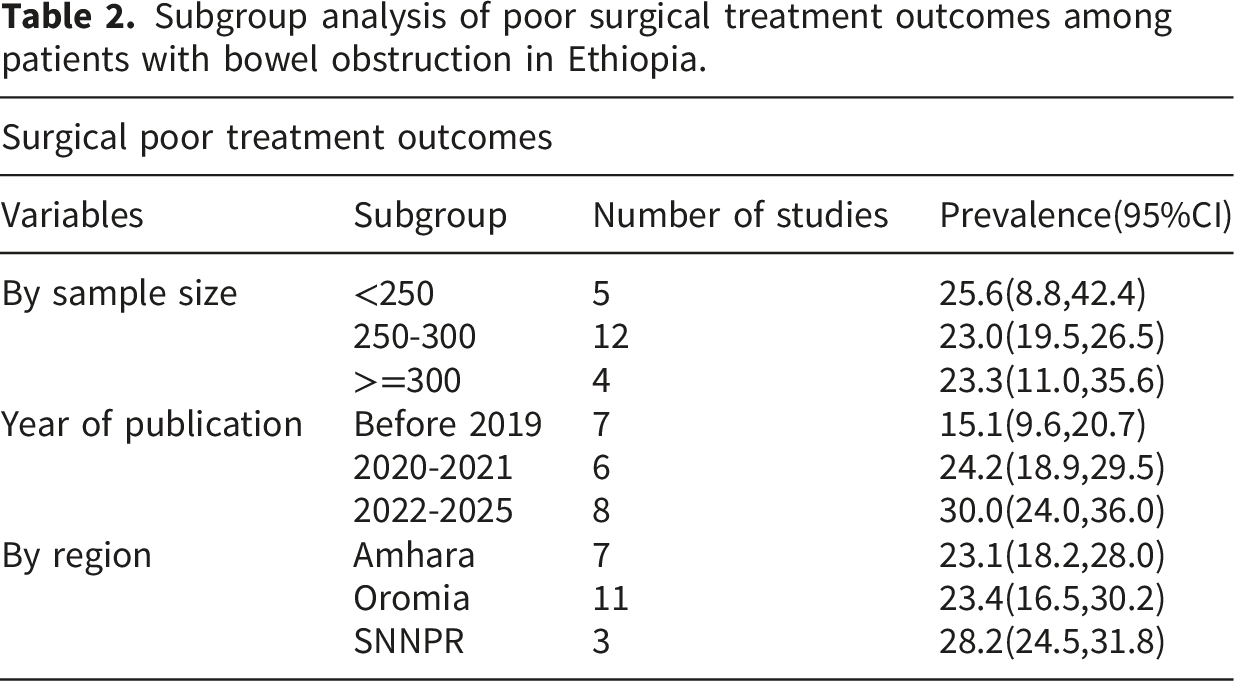
Subgroup analysis
Subgroup analysis of poor surgical treatment outcomes among patients with bowel obstruction in Ethiopia.
Meta regression
Random-effects meta-regression demonstrates that year of publication was a significant predictor of poor surgical treatment outcomes. Each increase in publication year category was associated with a higher prevalence of poor outcomes (p<0.001), suggesting that the year of publication may contribute to the observed heterogeneity across studies.
Factors associated with poor surgical treatment outcomes
Factors associated with poor surgical treatment outcomes of bowel obstruction in Ethiopia, 2026.
Discussion
This systematic review and meta-analysis provides an updated and comprehensive synthesis of the magnitude and associated factors of poor surgical treatment outcomes in patients treated for intestinal obstruction in Ethiopia. The study adheres to reporting standards recommended by the PRISMA 2020 Statements, which emphasizes transparent and complete synthesis of systematic reviews evidence across introduction, methods, results and discussion section 19 . The pooled prevalence of poor surgical treatment outcomes was 24% ( 95%CI: 19%-28%), indicating that nearly one in four patients experienced postoperative complications and/or death. A high degree of heterogeneity was observed among the included studies, indicating substantial variability in reported outcomes. This may be due to differences in hospital levels, case severity, surgical techniques, perioperative care, and study periods across settings. These variations likely contributed to the observed differences in effect estimates. Given this high heterogeneity, the pooled estimates should be interpreted as an overall summary rather than a precise effect size applicable to all settings, and should therefore be interpreted with caution 27 .
The observed pooled prevalence of poor surgical outcomes in this review is higher than previously reported in a systematic review and meta-analysis of poor management outcomes in Ethiopia, which found a pooled prevalence of about 20.22% for similar patient populations, albeit with fewer included studies 6 . The review includes more recent studies and a larger sample, suggesting an updated and potentially more robust estimate.
However, the pooled prevalence in this study is lower than reports from Nigeria, where poor outcomes were 31% and mortality 11% 28 . The difference may reflect variations in the underlying causes of bowel obstruction and case profiles across settings. For example, studies from Nigeria have reported a higher proportion of postoperative adhesions, while in Ethiopia volvulus, hernias, and tumors are commonly reported issues. These differences in case mix and clinical context partly explain the variation in reported outcomes.
The pooled prevalence in this study is also comparable with a study from Iraq, which reported 23.8% poor outcomes and 6.6% mortality. This similarity may reflect comparable healthcare system limitations and clinical care challenges in both settings, such as delays in presentation and resource constraints 29 . Patients in both settings often require complex procedures such as resection and anastomosis, which is associated with postoperative complications.
Delayed presentation to hospital, duration of illness >=7 days and resection and anastomosis were significantly associated with poor treatment outcomes of bowel obstruction 6 . This association may reflect more advanced disease severity and complicated clinical presentation at the time of surgery, as well as the complexity of cases requiring more extensive surgical procedures.
For example, patients undergoing resection and anastomosis often have more advanced disease or complicated obstruction, requiring extensive surgery, which may carry a high risk of postoperative complications such as anastomotic leak, infection or prolonged recovery.
Subgroup analysis suggests a trend toward higher prevalence of poor surgical outcomes in more recently published studies compared with earlier studies, and somewhat higher prevalence in the SNNPR of Ethiopia region compared with Amhara and Oromia regions. These patterns may reflect temporal and regional differences in study settings, including variations in healthcare access and clinical practices across regions. Nigerian studies include patients from tertiary hospitals with higher case severity and referral delays, increasing the risk of complications and death.
Implication of the study
This study highlights a high rate of poor surgical outcomes in bowel obstruction in Ethiopia and emphasizes the need for early presentation, timely surgery, and improved perioperative care to reduce complications and mortality.
Strength and limitations
This study provides the most up-to-date and comprehensive synthesis of surgical outcomes for bowel obstruction in Ethiopia, including 21 studies with a large combined sample size. The use of standardized meta-analysis methods, subgroup and sensitivity analysis, and quality assessment of included studies enhances the reliability and robustness of the findings. High heterogeneity among studies and potential differences outcome definitions may affect comparability. Additionally, most studies were hospital-based, limiting the generalizability of findings to the broader population.
Conclusion
This meta-analysis found that poor surgical treatment outcomes of bowel obstruction in Ethiopia were relatively high, affecting approximately 24% of patients, with a mortality rate of 6%. Delayed hospital presentation, prolonged duration of illness, and undergoing resection and anastomosis were significant associated factors of poor surgical outcomes. These findings highlight the need for early intervention, improved perioperative care, and strengthening surgical services to reduce complications and mortality.
Recommendation
Early diagnosis and prompt referral bowel obstruction cases should be strengthened to reduce delays in treatment. Surgical teams should implement standardized perioperative care and closely monitor high-risk patients, particularly those undergoing resection and anastomosis. Policymakers should prioritize improving emergency surgical services and capacity across regions to reduce complications and mortality.
Footnotes
Acknowledgements
We would like to thank all the authors of the studies included in this systematic review and meta-analysis.
Consent for publication
Since this is systematic review and meta-analysis consent for publication is not applicable.
Authors contributions
Conceptualization: ASA.
Data curation: ASA, DMK.
Formal analysis: ASA. Investigation: ASA, TKD.
Methodology: ASA, DSN.
Project administration: TB, TKD.
Software: ASA.
Supervision: TB and TL.
Validation: ASA, DMN.
Visualization: ASA, Writing original draft: ASA, JMK, DMK, TKD, Writing review & editing: ASA, TL and JMK.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is provided within the manuscript or supplementary information files.
Artificial intelligence disclosure statement
Artificial intelligence (AI) tools were used solely to assist with language editing and improvement of grammar and readability. No AI tools were used for study design, data collection, data analysis, or interpretation of results. The authors take full responsibility for the content of the manuscript and have reviewed and approved the final version in accordance with the journals policy on artificial intelligence use.