
Abstract
Background
Tuberculosis remains a significant global public health challenge, with the African region accounting for one-quarter of global incident cases. In Ghana, TB prevalence reaches 356 cases per 100,000 population. Depression is prevalent among persons with tuberculosis, potentially worsening treatment outcomes and patient prognosis. This study aimed to investigate the prevalence and predictors of depression among persons with TB in Ghana.
Methods
A cross-sectional study was conducted across 20 randomly selected healthcare facilities providing TB care in eight administrative regions of Ghana. The study included 1,103 participants aged 18 years and older. Depression was assessed using the Patient Health Questionnaire (PHQ-9), with depression defined as a score ≥5. Data collection utilized systematic random sampling and a structured questionnaire implemented through the Research Electronic Data Capture (REDCap) platform. Modified Poisson regression with robust standard error was used for statistical analysis with STATA version 17.
Results
The study revealed a depression prevalence of 40.98% among PWTB. Among the predictors of depression, Females had a 28% higher likelihood of depression (Adjusted Relative Risk = 1.28 [1.06-1.56]). Participants with poor health had 2.19 times higher depression risk (Adjusted Relative Risk = 2.19[1.64-2.92]). Additionally, stigmatized participants showed 52% higher depression risk (Adjusted Relative Risk = 1.52 [1.22-1.89]).
Conclusions
The high prevalence of depression among TB patients in Ghana underscores the need for integrated mental health services in TB care. The study highlights the importance of addressing factors such as gender, health status, and stigma to improve mental health outcomes for persons with tuberculosis.
Introduction
Tuberculosis (TB) has been a major public health concern globally, and its co-occurrence with depression poses a significant challenge for healthcare systems. 1 The African region accounted for one-quarter of the global 131 incident cases per 100 000 population. 1 In Ghana, TB incidence reaches 126 cases per 100,000 population, positioning the country tenth among African nations surveyed. 1 The relationship between TB and depression is multifaceted and bidirectional, 2 revealing intricate immunological mechanisms underscoring both physiological and psychological connections. 3 There is evidence of comorbidity between depression and TB, with 10-52% of TB patients experiencing depressive symptoms.4–6 This relation between depression and TB worsens prognosis. Studies demonstrate depression among persons with TB (PWTB) leads to poorer adherence, higher likelihood of treatment failure, increased antimicrobial resistance, and elevated mortality risk.2,7,8
Despite the intersection and burden, the depression among PWTB in Ghana has not been extensively studied. Existing research has primarily focused on the prevalence of TB and its associated factors, with less attention given to assessing the prevalence and predictors of depression among PWTB in Ghana. 6 There is a noticeable gap in literature on the association between social and clinical factors and depression among TB patients in Ghana, which is essential for developing tailored interventions. The findings of this study will contribute to the existing body of knowledge on the intersection of depression and TB, which could advance the development of targeted interventions to improve the health and mental well-being of persons with TB in Ghana.
Methods
Study design and setting
This was a facility-based cross-sectional study conducted across randomly selected 20 healthcare facilities providing TB care in eight administrative regions of Ghana from 5th to 22nd February 2023. The study design was selected to provide insight on depression prevalence and associated factors among PWTB at a single point in time. The selected healthcare facilities represented a diverse geographical and healthcare system landscape, including primary, secondary, and tertiary level institutions across urban and rural settings.
Participants
The study population comprised PWTB accessing healthcare services at the selected facilities. Participants were carefully selected based on specific criteria designed to ensure meaningful and representative data collection. Individuals were eligible for inclusion if they were 18 years or older, had a confirmed tuberculosis diagnosis, were currently receiving TB treatment at the selected healthcare facilities, and were mentally competent to provide informed consent. To maintain data integrity and participant welfare, the study excluded individuals who were severely ill or hospitalized, as well as those unable to provide meaningful responses or consent to participate in the research.
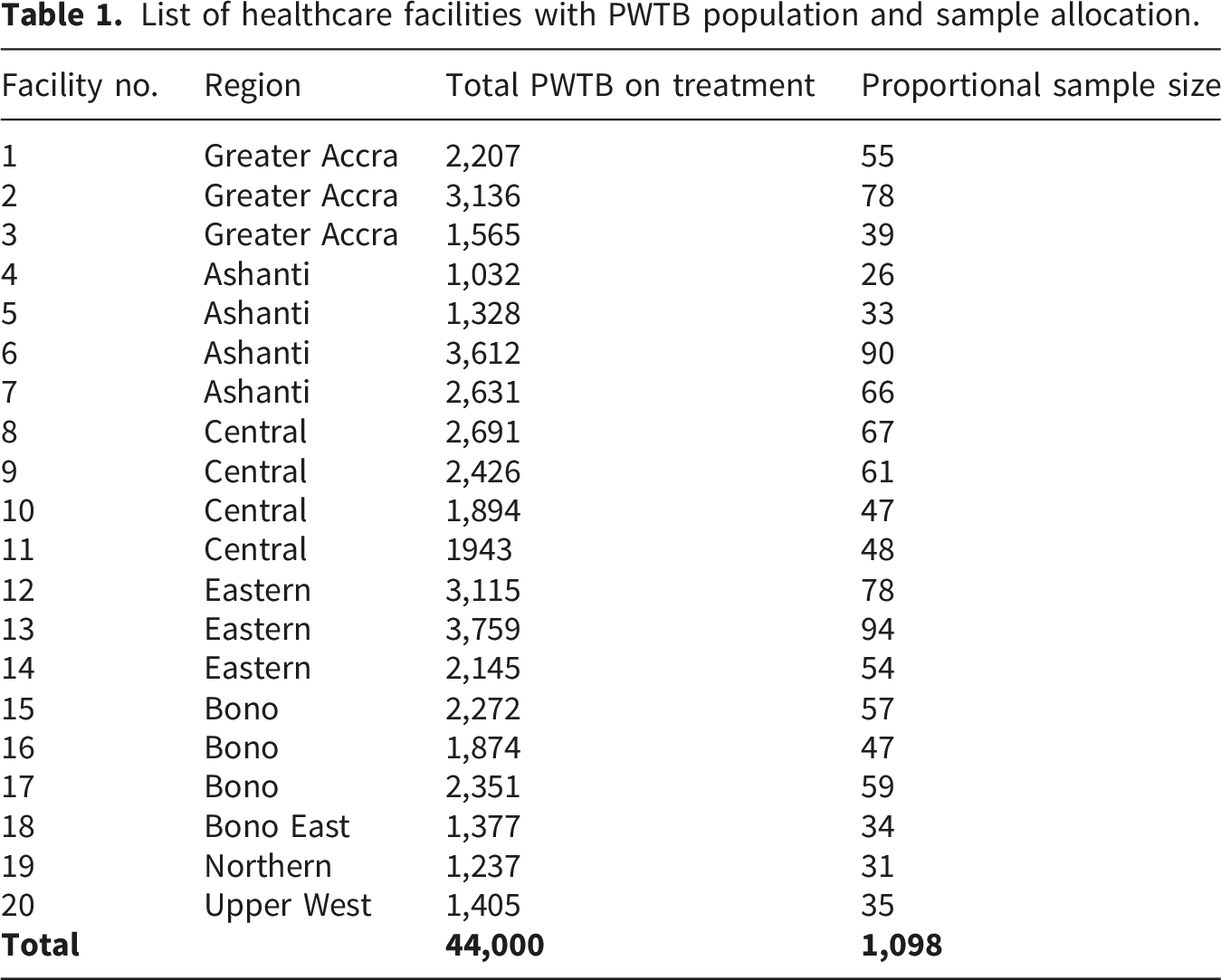
Sample size

List of healthcare facilities with PWTB population and sample allocation.
Sampling technique
The study utilized a systematic sampling technique designed to minimize selection bias and ensure randomized participant selection. Data collectors visited each of the 20 selected facilities from 5th to 22nd February 2023, calculating specific sampling intervals based on each facility’s TB patient volume on each visits. The initial participant in each facility was selected using a computer-generated random number, with subsequent participants chosen at predetermined intervals. In instances where a selected individual declined participation or did not meet inclusion criteria, they were replaced by the next eligible participant, maintaining the study’s sampling integrity and representativeness.
Data collection
Data collection was conducted using a structured questionnaire (see supplementary file 1) implemented through the Research Electronic Data Capture (REDCap) platform, a secure and robust data management system. The primary outcome variable was depression status, assessed using the Patient Health Questionnaire (PHQ-9).9,10 The total score for the PHQ-9 is 27, with depression severity classified as 0-4 (None depression), 5-9 (Mild depression), 10-14 (Moderate depression), 15-19 (Moderately severe depression) and 20-27 (Severe depression). For this study, any depressive symptoms were defined as a PHQ-9 score ≥5, encompassing mild, moderate, moderately severe, and severe depression categories. This threshold was chosen to capture the full spectrum of depressive symptom burden relevant to TB care and treatment adherence, consistent with screening approaches in high-burden settings where early identification of psychological distress is critical. Independent variables included age, place of residence, gender, marital status, educational level, ethnicity, religion, accommodation, health status, treatment support, occupation, and stigmatized status.
Bias
To minimize potential sources of bias, the study implemented multiple methodological safeguards. Proportional sampling across facilities ensured representative participant selection, while systematic random selection techniques reduced selection bias. Standardized data collection protocols were developed and rigorously implemented, and all data collectors underwent comprehensive training to ensure consistency and reliability. The use of validated assessment tools like the PHQ-9 further enhanced the study’s methodological rigor, helping to minimize measurement bias and ensuring the comparability of results across different healthcare settings. 10
Statistical analysis
Statistical analysis was conducted using Stata version 17.0, 11 employing a comprehensive and sophisticated analytical approach. Descriptive statistics were used to characterize the study population, with frequencies and proportions calculated for categorical variables and means with standard deviations computed for continuous variables. Bivariate associations were assessed using Pearson’s chi-square test of independence (or Fisher’s exact test where expected cell counts were <5) to identify potential associations between depression and independent variables. All variables with a bivariate p-value <0.20 or of known clinical/epidemiological importance were entered into a multivariate modified Poisson regression model. Because the outcome prevalence exceeded 10%, violating the rare-disease assumption, modified Poisson regression with robust standard errors was used to obtain unbiased relative risks (RRs) and adjusted relative risks (ARRs), while accounting for within-facility clustering and potential heteroskedasticity.12,13 A two-sided p-value <0.05 was considered statistically significant.
Ethical consideration
The study was conducted in accordance with the Declaration of Helsinki. The study protocol received ethical approval from the Ghana Health Service Ethics Review Committee (Project ID: GHS-ERC 001/11/22). Written informed consent was obtained from all participants prior to data collection, ensuring voluntary participation and full understanding of the study’s purposes and procedures. For participants with no formal education, the consent form was read aloud in the participant’s preferred language by a trained research assistant. Consent was documented via a thumbprint or witnessed mark in the presence of an independent literate witness, as approved by the Ghana Health Service Ethics Review Committee. Participant confidentiality was maintained through secure data management protocols, with all personal identifiers protected and data anonymized during analysis.
Result
Socio-demographics
Socio-demographic characteristics of study participants.

*Mean (Standard Deviation).
Prevalence of depression
Chi-square test of independence between depression and independent variables.
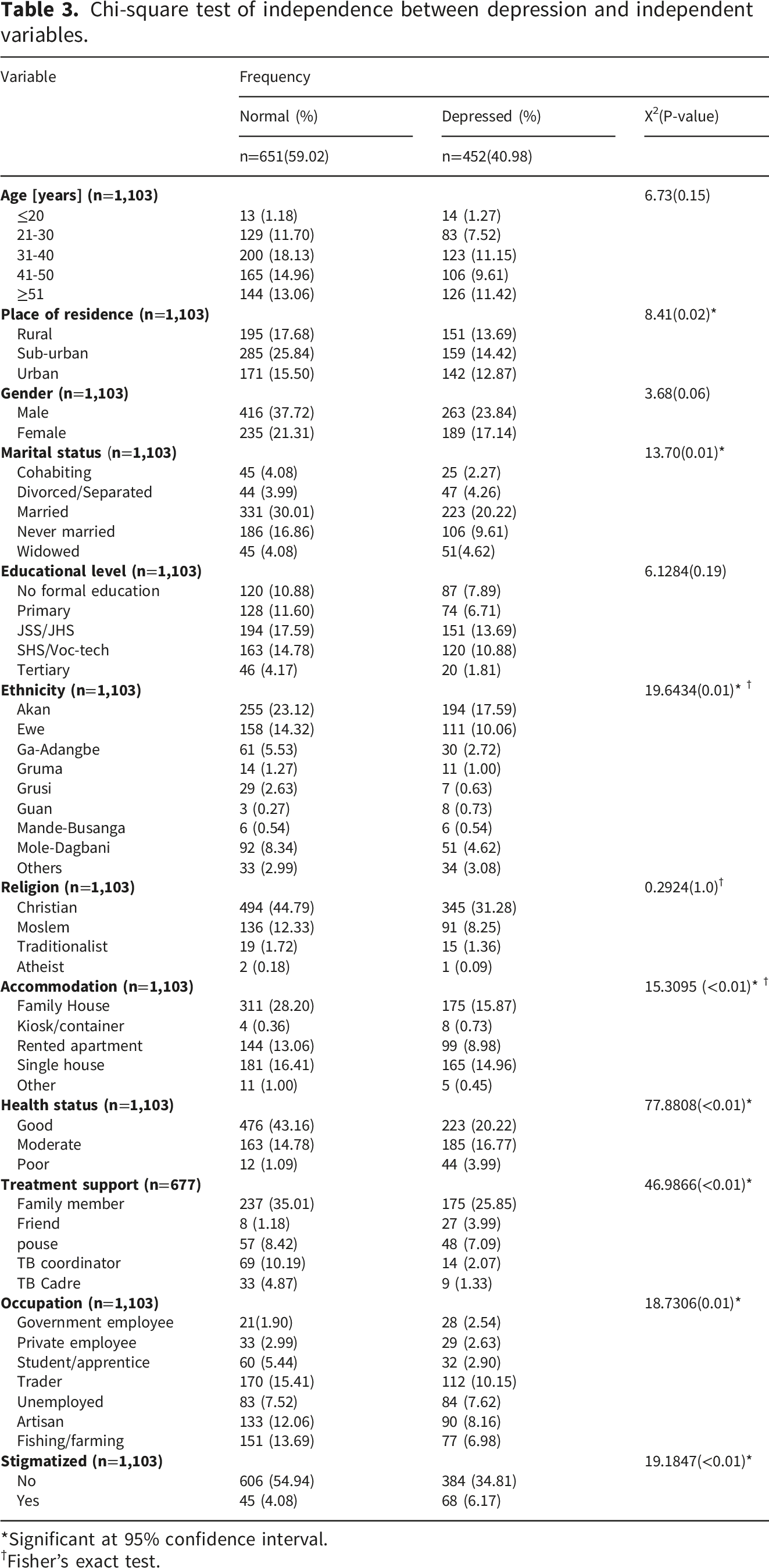
*Significant at 95% confidence interval.
†Fisher’s exact test.
Predictors of depression
Generalized modified poison regression models.
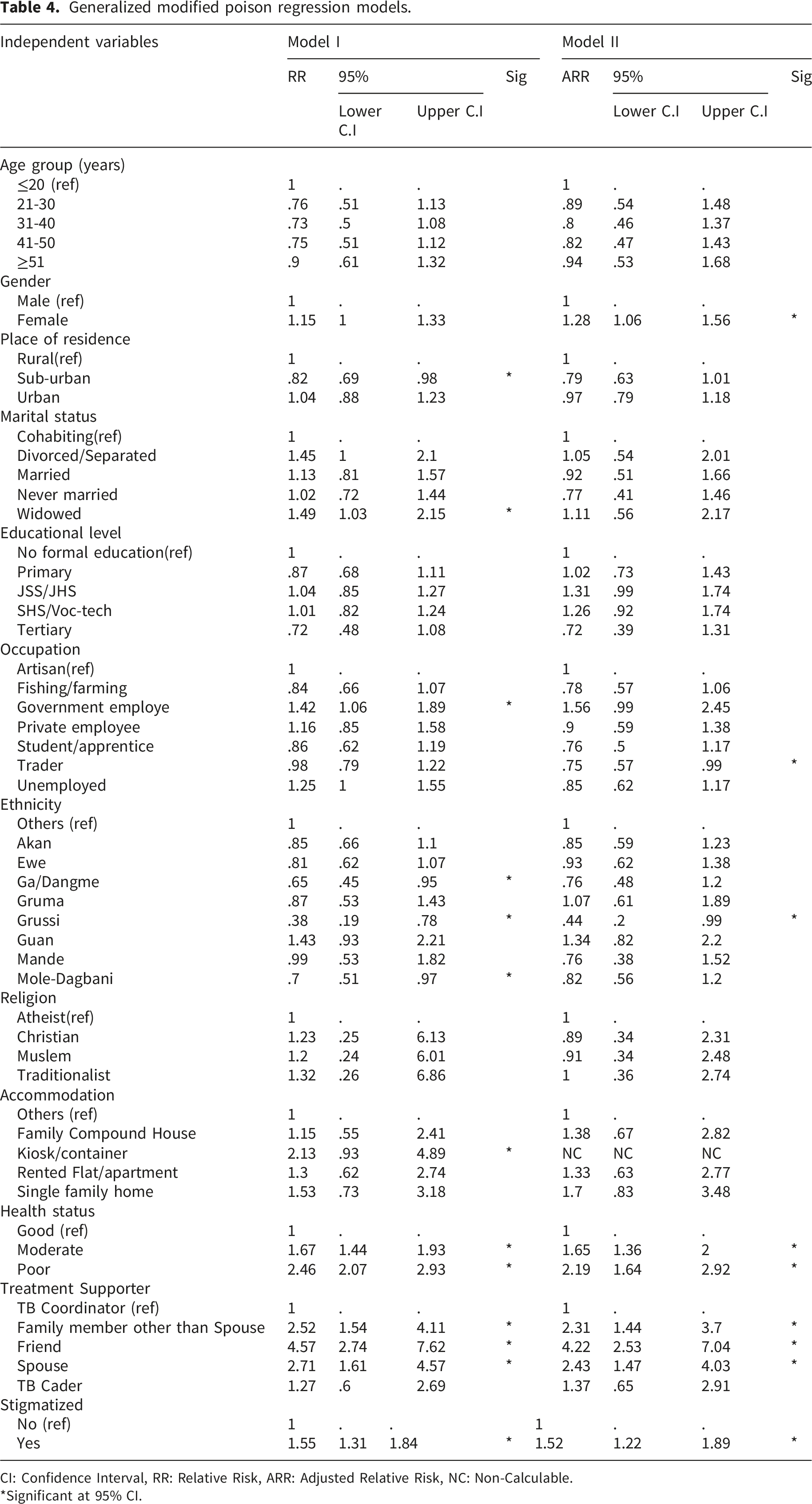
CI: Confidence Interval, RR: Relative Risk, ARR: Adjusted Relative Risk, NC: Non-Calculable.
*Significant at 95% CI.
Discussion
The study aimed to investigate the prevalence and predictors of depression among PWTB in Ghana, revealing a significant depression prevalence of 41% using the PHQ-9 ≥5 threshold. This prevalence falls within the upper range of pooled estimate reported in systematic review of depression among PWTB in Ghana. 6 The study’s outcome captures any depressive symptoms (mild through severe) rather than clinical depression alone, which is appropriate for screening in TB care settings where early identification of psychological distress can inform integrated mental health interventions and prevent progression to severe disease.
The gender dimension of depression emerged as a critical finding, with females demonstrating a 28% higher likelihood of experiencing depression compared to males. This disparity aligns with existing literature that suggests complex interactions between biological, psychological, and social factors contribute to female vulnerability to depression. 14 The relationship between gender and mental health underscores the need for more gender-sensitive approaches in TB and mental health care. 1 Additionally, health status proved to be a crucial predictor of depression risk. Patients with poor health were 2.19 times more likely to experience depression, while those with moderate health status showed a 1.65 times higher depression risk compared to patients with good health. This bidirectional relationship highlights the intricate connection between physical and mental well-being.2,3 Poor health can significantly impact mental health by limiting daily activities, reducing quality of life, and creating additional psychological stressors for PWTB. 15
Stigma emerged as a particularly significant factor, with stigmatized patients experiencing a 52% higher risk of depression. This finding underscores the profound psychological impact of social marginalization and discrimination. TB-related stigma can induce feelings of shame, isolation, hopelessness, and worthlessness, creating additional mental health challenges for patients already dealing with a complex medical condition. 16 Contrary to the study findingd of Gariépy and Co, 17 receiving support from friends, spouses, and family members was associated with higher depression risks. This unexpected finding challenges existing assumptions about social support and suggests a more complex dynamic in how support is perceived and experienced by PWTB.
Lastly, cultural and occupational factors also played a significant role in depression risk. The Grussi ethnic group showed a 66% reduced depression risk, while traders exhibited a 25% lower depression risk compared to artisans. These variations suggest that cultural context, economic opportunities, and occupational characteristics can significantly influence psychological resilience and mental health outcomes. 18
Study limitations and strengths
The study’s cross-sectional design presents limitations in establishing causal relationships between depression and identified predictors. Self-reported data may introduce recall and social desirability biases. However, the research’s strengths include a large sample size, systematic random sampling, and robust statistical analysis using modified Poisson regression, providing valuable insights into the complex landscape of depression among PWTB.
Implication for research and practice
The findings of this study carry significant implications for healthcare providers and policymakers. They highlight the urgent need to improve the integration of mental health screening into TB care services, develop targeted interventions to reduce TB-related stigma, provide comprehensive support addressing both physical and mental health needs, and create socioeconomic support programs to improve PWTBs’ overall well-being.
Conclusion and recommendation
This study highlights the high prevalence of depression among PWTB in Ghana and the need to improve gender and culturally sensitive approaches with targeted interventions to reduce TB-related stigma. Screening for depression should be a routine part of TB care, and patients with depression should be provided with appropriate counselling and support.
Supplemental material
Supplemental material - Prevalence and associated factors of depression among persons with tuberculosis in Ghana: A cross-sectional study
Supplemental material for Prevalence and associated factors of depression among persons with tuberculosis in Ghana: A cross-sectional study by Jacob Solomon Idan, Enock Ko-mati-oo Yentariba, Benjamin Spears Ngmekpele Cheabu, Jerry Amoah-Larbi, Francis Adjei Osei, Georgina Benyah, and Aliyu Mohammed in Sage Open Medicine.
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki. The study protocol received ethical approval from the Ghana Health Service Ethics Review Committee (Project ID: GHS-ERC 001/11/22).
Consent to participate
Written informed consent was obtained from all participants prior to data collection, ensuring voluntary participation and full understanding of the study’s purposes and procedures. For participants with no formal education, the consent form was read aloud in the participant’s preferred language by a trained research assistant. Consent was documented via a thumbprint or witnessed mark in the presence of an independent literate witness, as approved by the Ghana Health Service Ethics Review Committee. Participant confidentiality was maintained through secure data management protocols, with all personal identifiers protected and data anonymized during analysis.
Author contributions
J.S.I and E.K.Y wrote the draft manuscript. J.S.I., E.K.Y., and B.S.N.C. played a role in the conceptualization and data analysis. J.A.-L. and F.A.O. contributed to the literature review. A.M, G.B. and J.S.I provided critical insights and contributed to manuscript revisions. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.