
Abstract
Objectives
The objective of this study was to provide the first multicenter evaluation of pediatric gastrointestinal endoscopy in Palestine, specifically characterizing clinical indications, sedation practices, diagnostic and histopathologic yield, and outcomes.
Methods
This study was conducted across multiple hospitals in the West Bank, Palestine, including patients ≤18 years who underwent gastrointestinal endoscopy between January 2019 and December 2023.
Results
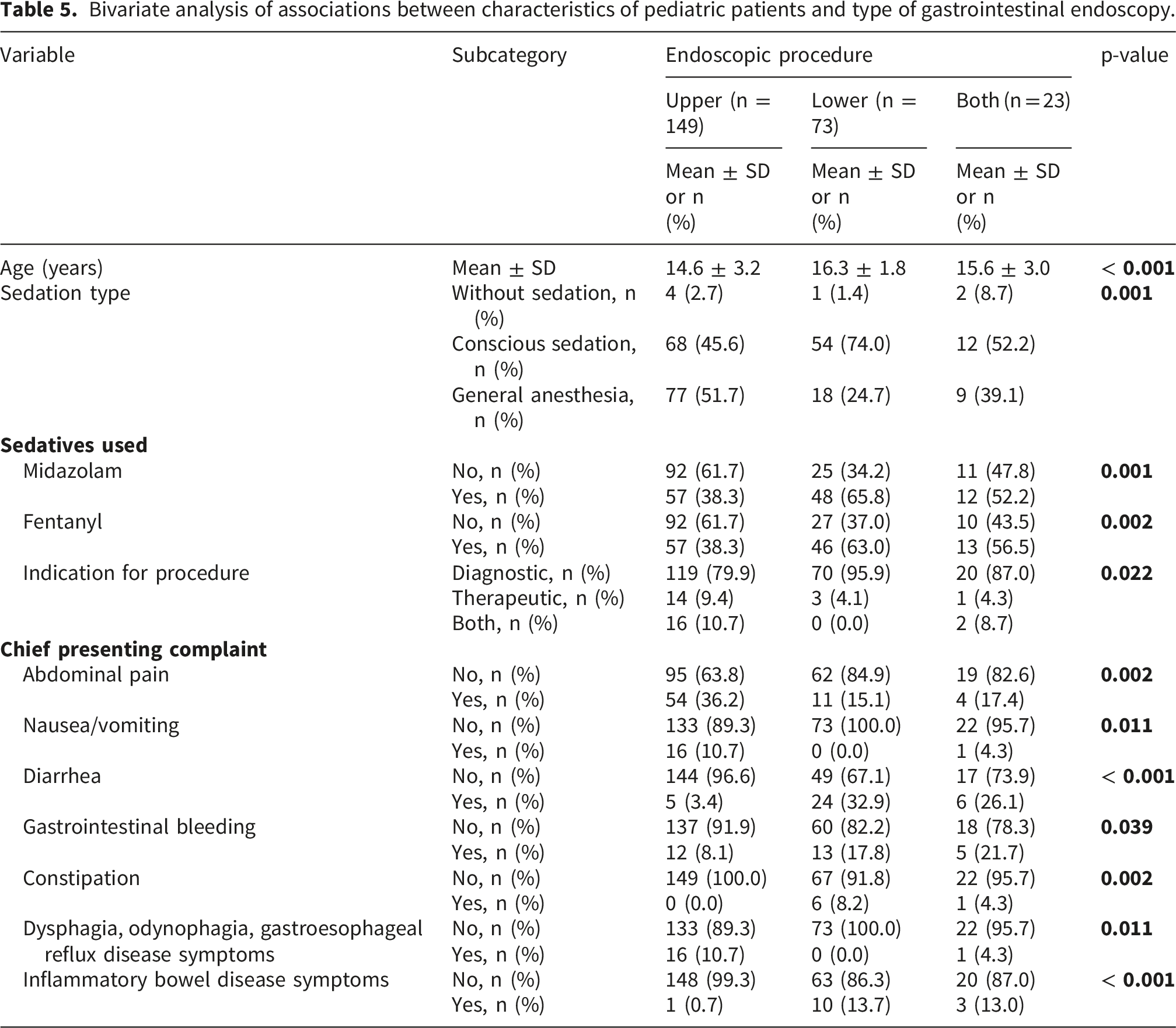
A total of 245 pediatric endoscopic procedures were performed across participating centers (mean age 15.2 ± 2.9 years; 51.0% female). Of these, 149 were upper endoscopies and 96 were lower endoscopies. Abnormal findings were documented in 113 upper endoscopies (75.8%), most commonly gastritis, esophagitis, and duodenitis, and in 72 lower endoscopies (75.0%), including colitis, polyps, and terminal ileitis. Biopsies were submitted in 186 procedures (75.9%), with histopathological abnormalities confirmed in 127 cases (68.3% of biopsied specimens). The most frequent final diagnosis was gastritis (n = 68; 27.8%), including Helicobacter pylori-associated and nodular gastropathy, followed by esophagitis (n = 17; 6.9%), Crohn’s disease (n = 10; 4.1%), and ulcerative colitis (n = 10; 4.1%). Patients who underwent lower endoscopy were significantly older (mean age 16.3 ± 1.8 years) compared with those undergoing upper endoscopy (14.6 ± 3.2 years) or combined procedures (15.6 ± 3.0 years; p < 0.001). The chief presenting complaint was diarrhea (n = 24; 9.8%) and inflammatory bowel disease symptoms (n = 10; 4.1%) when patients underwent lower endoscopy, whereas the chief presenting complaint was abdominal pain (n = 54; 22.0%) and nausea/vomiting (n = 16; 6.5%) when patients underwent upper endoscopy.
Conclusion
This multicenter study demonstrates that pediatric gastrointestinal endoscopy in Palestine yields a high diagnostic rate, with abnormal findings documented in approximately three-quarters of both upper and lower procedures. The findings primarily emphasize the importance of strengthening biopsy protocols and diagnostic pathways in resource-limited healthcare systems.
Keywords
Introduction
Pediatric gastrointestinal endoscopy has become an indispensable tool in modern pediatric medicine, with global utilization steadily increasing over the past decade.1–4 Recent estimates suggest that more than 70-80% of pediatric patients with suspected gastrointestinal pathology undergo endoscopic evaluation as part of their diagnostic workup,1,3,4 reflecting its central role in identifying and managing conditions such as inflammatory bowel disease, celiac disease, gastrointestinal bleeding, and structural abnormalities.5,6 The procedure is not only diagnostic but also therapeutic, enabling interventions such as polyp removal, dilation of strictures, and foreign body extraction.3–5,7 The demand for pediatric endoscopy continues to rise in parallel with the increasing prevalence of chronic gastrointestinal disorders in children, including inflammatory bowel disease and functional gastrointestinal disorders, which have shown a marked upward trend worldwide.5,8–10 In this context, pediatric GI endoscopy serves as a cornerstone for both early diagnosis and timely therapeutic intervention, directly impacting patient outcomes and long-term quality of life.
Safe and effective sedation is considered a cornerstone of pediatric gastrointestinal endoscopy, as it ensures patient comfort, minimizes anxiety, and facilitates procedural success.2,11–13 In resource-rich settings, pediatric endoscopy is now considered a standard of care, with studies reporting that over 90% of pediatric endoscopies are performed under sedation or anesthesia to ensure safety and patient comfort. 9 Conscious sedation with agents such as midazolam and fentanyl remains widely used, while propofol-based anesthesia has gained popularity due to its rapid onset and recovery profile.1,2,5,6,14 However, sedation practices vary considerably across regions, influenced by resource availability, institutional protocols, and the presence of trained anesthesiologists.5,10,11 Despite its benefits, sedation carries inherent risks, particularly in children with comorbidities or complex procedures. Reported adverse events include respiratory depression, apnea, hypotension, and paradoxical reactions.2,5,15 Recent studies emphasize the importance of tailoring sedation regimens to patient age, weight, and clinical condition, as well as adhering to standardized monitoring protocols to mitigate complications. 14 In resource-limited settings, where anesthesiologist support may be restricted, optimizing sedation strategies is especially critical to balance safety with feasibility.
Despite the widespread adoption of pediatric gastrointestinal endoscopy globally, there remains a striking lack of data from resource-limited healthcare systems, including Palestine. In such resource-limited healthcare systems, challenges such as restricted access to anesthesiologists, variability in sedation protocols, and limited infrastructure often shape clinical practice in ways that differ significantly from high-income settings.1,8 Recent global reviews emphasize that sedation practices are highly heterogeneous across regions, with outcomes strongly influenced by local resources and training capacity.1,2,5,6 For Palestinian hospitals, where pediatric endoscopy services are relatively new and expanding, understanding the patterns of sedation use, associated outcomes, and complication rates is critical to improving patient safety and procedural success.
Against this backdrop, the objective of this study was to provide the first multicenter evaluation of pediatric gastrointestinal endoscopy in Palestine, specifically characterizing clinical indications, sedation practices, diagnostic and histopathologic yield, and outcomes, in order to inform clinical practice and support the development of standardized protocols in resource-limited healthcare systems. By systematically reporting these practices and outcomes, this study provides the first evidence base on pediatric endoscopy in Palestine, highlighting both diagnostic yield and sedation patterns, and offering insights that may inform clinical practice, guide training, and support the development of standardized protocols across centers.
Methods
Study design and settings
This study employed a retrospective observational design and was conducted across the two main governmental and tertiary care hospitals in the West Bank, Palestine, which represent the principal centers where pediatric endoscopy services are mainly offered. These institutions encompass a diverse mix of tertiary referral centers and governmental hospitals, thereby providing a comprehensive and representative view of pediatric endoscopy practices in a resource-limited healthcare system. The study period spanned from January 2019 to December 2023, ensuring the inclusion of a large cohort of pediatric patients and capturing variations in sedation practices and outcomes over time. Data extraction was performed between March and November 2025.
By focusing on hospitals in the West Bank, the study design accounted for logistical challenges and restricted access to southern regions, ensuring feasibility while maintaining representativeness of the pediatric population in Palestine. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist, ensuring transparency, methodological rigor, and standardized reporting of observational research. Adherence to STROBE checklist is provided in Supplemental Table S1.
Study population, inclusion and exclusion criteria
The study population comprised pediatric patients aged 18 years or younger who underwent diagnostic or therapeutic gastrointestinal endoscopic procedures in participating hospitals across the West Bank between January 2019 and December 2023. Eligible patients were identified through hospital electronic health records and included those presenting with clinical indications such as gastrointestinal bleeding, abdominal pain, foreign body ingestion, suspected structural abnormalities, inflammatory bowel disease, celiac disease, or unexplained chronic vomiting. By encompassing a wide range of indications, the study sought to capture the diversity of pediatric endoscopy practice in Palestine.
To ensure methodological rigor, we applied clear inclusion and exclusion criteria. Patients were included if their medical records were complete and contained documentation of demographic details, sedation type, sedative dosage, endoscopic findings, and outcomes. Patients were excluded if their records were incomplete or lacked essential documentation of sedation or outcomes, if they had known allergies or contraindications to sedative agents, or if their procedures were performed outside the defined study period.
Sample size and sampling technique
The target population for this study comprised pediatric patients under the age of 18 years who required gastrointestinal endoscopy between January 2019 and December 2023 in the participating hospitals. Based on estimates from the Palestinian Central Bureau of Statistics, approximately 1.3 million children live in the West Bank. 16 To approximate the proportion requiring specialized endoscopic evaluation, we synthesized regional epidemiological data and clinical referral patterns. The cumulative prevalence of organic gastrointestinal disorders in children, including celiac disease, inflammatory bowel disease, and other organic conditions such as Helicobacter pylori-associated gastritis, eosinophilic esophagitis, and acute indications like foreign body ingestion or gastrointestinal bleeding, suggests that approximately 3% of the pediatric population may require endoscopic assessment.17–21 This translates into a target population of roughly 39,000 children.
Using the Raosoft sample size calculator (https://www.raosoft.com/) with a 95% confidence level, a 5% margin of error, and a response distribution of 20%, the minimum required sample size was calculated to be 245 patients. This figure was further validated by feedback from healthcare providers in the field, who reported case numbers consistent with these estimates.
Given the retrospective nature of the study and the reliance on hospital records, a convenience sampling technique was employed. All eligible pediatric patients with complete medical records during the study period were included, ensuring practicality while maximizing the representativeness of the cohort.
Definitions of variables and data collection
Data were extracted retrospectively from hospital electronic health records (EHRs) using a structured data collection form (Supplemental Table S2). The data collection form was developed to comprehensively capture the domains most relevant to pediatric endoscopy practice. Specifically, it was structured to document the types of sedation administered and the sedative agents used, together with their associations with patient age, comorbidities, and procedure type. In addition, the form was designed to record endoscopic findings, biopsy submission rates, and histopathological abnormalities, alongside the final diagnoses and therapeutic interventions performed. Each variable was defined a priori to minimize ambiguity and enhance reproducibility. The form was developed based on previous relevant studies and after consultation with gastroenterologists, pediatric gastroenterologists, anesthesiologists, pathologists, and clinical researchers to ensure that all relevant domains of patient care and sedation practice were captured.1,9,15,22–25 It was piloted on a small set of records to refine clarity and usability before full-scale application.
Demographic and baseline variables included age (years), sex, and the presence of comorbidities. Comorbidities were further categorized into gastrointestinal, cardiovascular, neurological, hematological, endocrine, immunological, and renal conditions. The physical status of patients was assessed using the American Society of Anesthesiologists (ASA) Physical Status Classification System, which stratifies patients according to pre-anesthesia comorbidities. 26
Clinical indications and presenting complaints were collected from physician notes and admission records. These included abdominal pain, diarrhea, gastrointestinal bleeding, nausea/vomiting, dysphagia/gastroesophageal symptoms, anemia-related symptoms, inflammatory bowel disease symptoms, weight loss, constipation, foreign body ingestion, celiac symptoms, dyspepsia, growth issues, and surveillance/screening indications. Each complaint was coded as present or absent.
Procedural characteristics encompassed the type of endoscopy performed (upper endoscopy, lower endoscopy, or combined procedures), the indication for procedure (diagnostic, therapeutic, or both), and the endpoint reached (duodenum, terminal ileum, or both).
Sedation-related variables were also collected. These included the type of sedation (none, conscious sedation, or general anesthesia), the sedatives administered (midazolam, fentanyl, propofol, atropine sulfate, pethidine, ketamine, atracurium), and their dosages (mg or mcg per weight category). These variables were collected from anesthesia and procedure notes.
Endoscopic findings were systematically recorded from procedure reports. Abnormal findings included signs of inflammation, ulceration/erosions, nodules, strictures/narrowing, polyps/masses, fissures, varices, hemorrhoids, fistula, bleeding, foreign body, and other nonspecific changes. Each finding was coded as present or absent.
Histopathology variables captured whether a biopsy was sent for histopathology and whether abnormal histopathological findings were present. Specific histopathological diagnoses included gastritis changes, colitis/inflammatory bowel disease patterns, infection/inflammatory changes, Helicobacter pylori-associated changes, lymphoid hyperplasia, celiac pattern/villous atrophy, polyps, metaplasia/dysplasia, eosinophilic esophagitis, ulcer changes, atypia, and other rare conditions. Biopsy sites were also documented (duodenum, terminal ileum, esophagus, colon segments, rectum). Therapeutic interventions were recorded when performed during endoscopy. Each intervention was coded as present or absent. These variables were collected from the histopathology reports. By systematically defining and coding these variables, the study ensured that all analyses were reproducible, transparent, and aligned with international reporting standards.
To minimize bias, data were extracted independently by trained researchers who were final year medical students. Each record was reviewed systematically, and information was entered into a secure database with built-in validation checks to reduce transcription errors. Standardized definitions and coding rules were applied across all hospitals, ensuring consistency in how clinical complaints, sedation practices, endoscopic findings, and outcomes were recorded. This approach provided a reliable framework for capturing retrospective data while safeguarding against subjective interpretation, thereby strengthening the validity and reproducibility of the study’s findings.
Statistical analysis
All data were entered and analyzed using IBM SPSS for Windows, version 21.0. Descriptive statistics were first generated to provide an overview of the study sample. Age was treated as a continuous variable and summarized as means ± standard deviations (SD), while categorical variables, including sex, comorbidities, sedation type, sedatives used, clinical complaints, endoscopic findings, biopsy submission, histopathology results, and therapeutic interventions, were expressed as frequencies (n) and percentages (%).
For inferential analysis, bivariate comparisons were performed to explore associations between patient characteristics, sedation practices, procedural indications, and outcomes. Differences between age groups were assessed using the Student’s t-test or one-way analysis of variance (ANOVA), depending on the number of groups compared. Associations between categorical variables were examined using the Pearson chi-square test. Statistical significance was set at a p-value < 0.05.
Results
Demographic and baseline characteristics of the pediatric patients
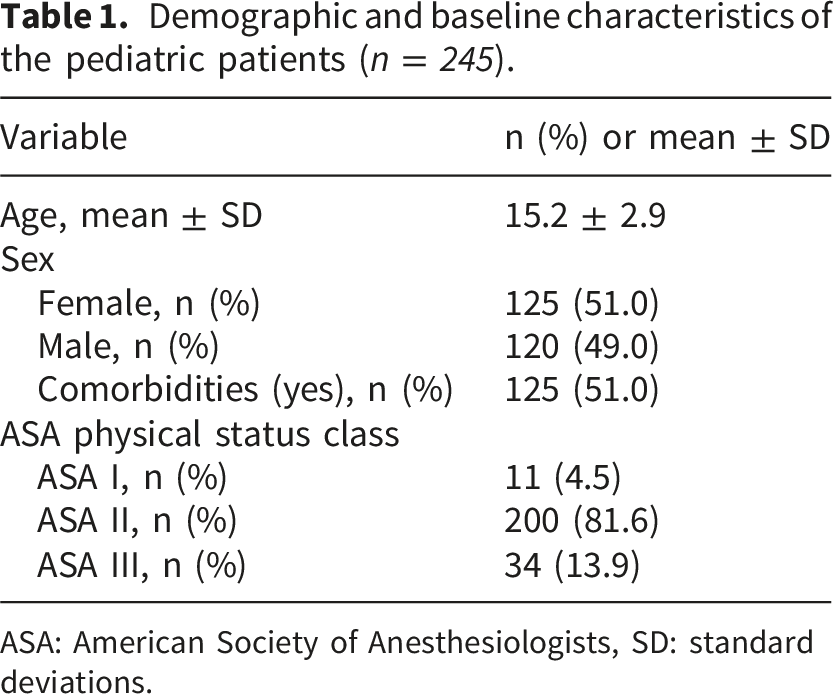
In this study, a total of 273 records were identified for pediatric patients who underwent gastrointestinal endoscopy (Figure 1). After excluding incomplete records, the study included 245 pediatric patients with a mean age of 15.2 ± 2.9 years (Table 1). The sex distribution was nearly equal, with 125 females (51.0%) and 120 males (49.0%). Notably, 125 patients (51.0%) had comorbidities, underscoring the complexity of this population. The majority of pediatric patients were classified as ASA II (n = 200; 81.6%), indicating mild systemic disease, while 34 (13.9%) were ASA III and only 11 (4.5%) were ASA I. Of the patients, 125 (51.0%) had comorbidities (Table 1). Details of these comorbidities are shown in Supplemental Figure S1. Flow chart of patient selection process. Demographic and baseline characteristics of the pediatric patients (n = 245). ASA: American Society of Anesthesiologists, SD: standard deviations.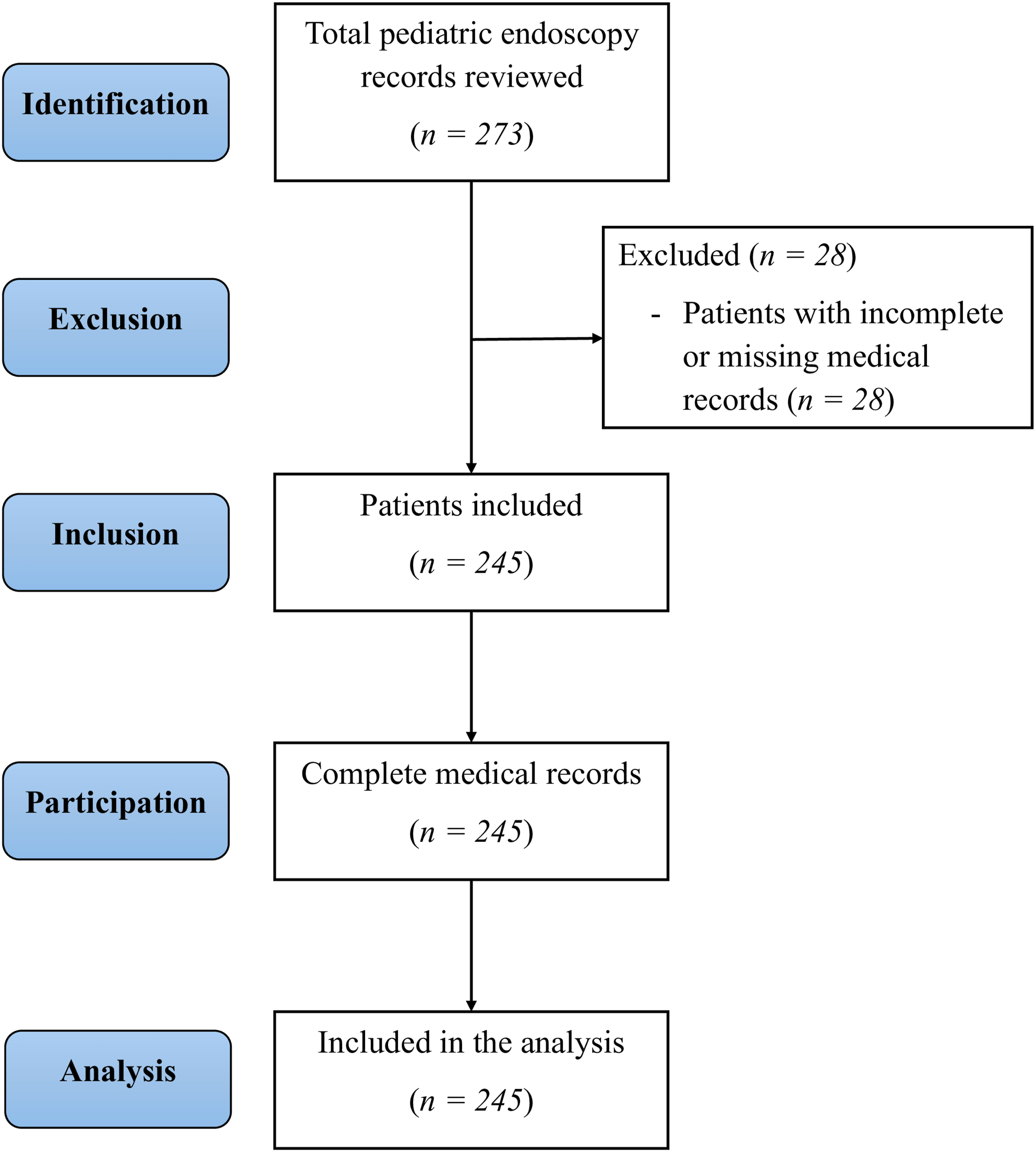
Endoscopies were performed using pediatric gastroscopes (outer diameter 5-7 mm, length 100-110 cm) and colonoscopes (outer diameter 9-11 mm, length 120-130 cm), with scope selection tailored to patient age and body size. In older adolescents, standard adult scopes were occasionally used when pediatric scopes were unavailable. All endoscopes were processed according to hospital infection-control protocols, including high-level disinfection in automated endoscope reprocessors with peracetic acid, followed by sterile rinsing, drying, and storage in ventilated cabinets.
Clinical indications and procedural characteristics
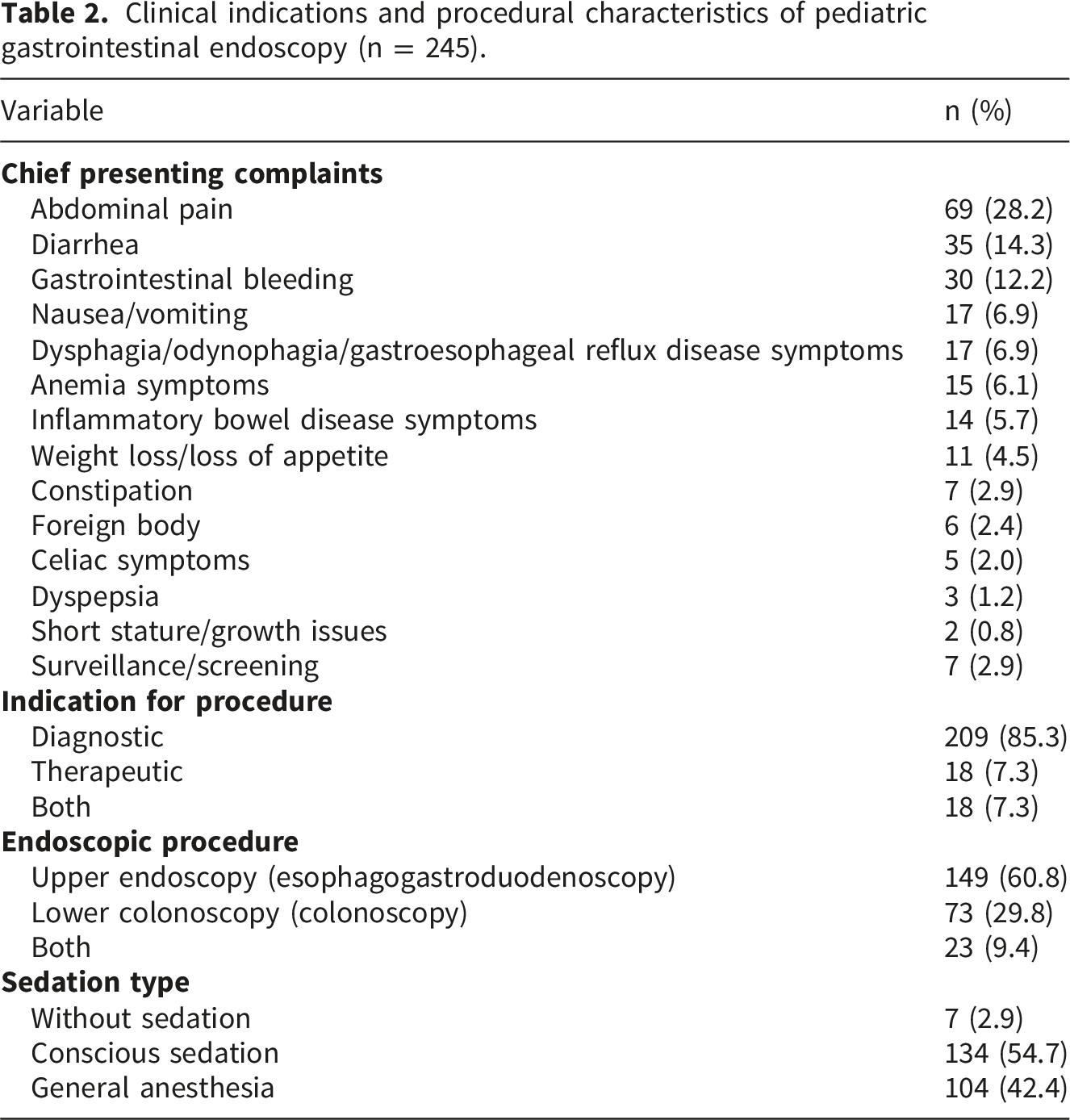
Clinical indications and procedural characteristics of pediatric gastrointestinal endoscopy (n = 245).
Endpoints reached and endoscopic outcomes
Endpoints reached and outcomes of pediatric gastrointestinal endoscopy (n = 245).
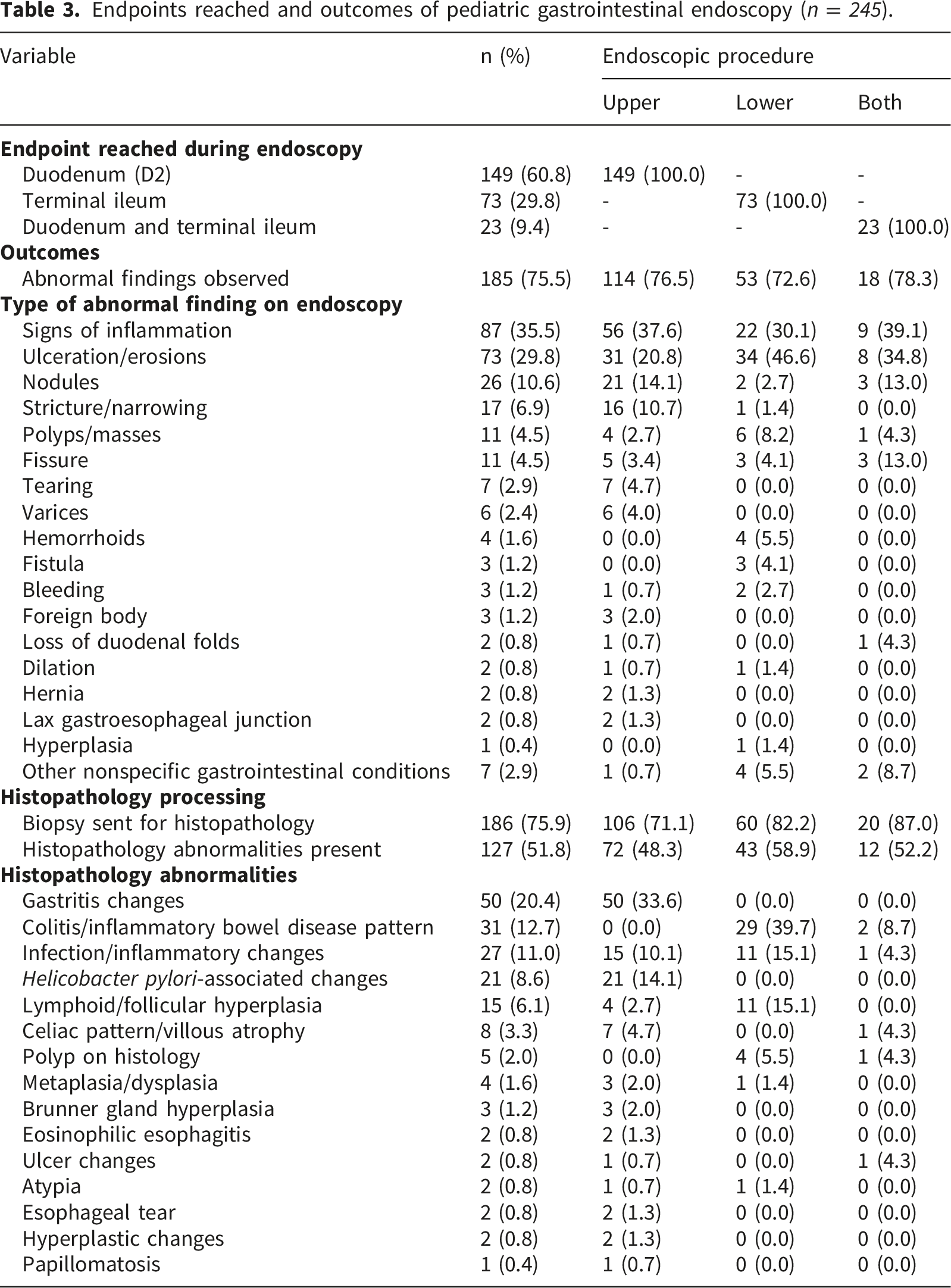
Biopsies were most frequently obtained from the duodenum (n = 83; 33.9%) and the terminal ileum (n = 50; 20.4%), followed by the esophagus (n = 17; 6.9%) and rectum (n = 13; 5.3%). Less common sites included the colon segments, ascending (n = 9; 3.7%), transverse (n = 14; 5.7%), descending (n = 14; 5.7%), sigmoid (n = 11; 4.5%), and the cecum (n = 6; 2.4%). Abnormal findings were most often localized to the stomach (n = 77; 31.4%), esophagus (n = 35; 14.3%), and duodenum (n = 35; 14.3%), with additional abnormalities noted in the terminal ileum (n = 33; 13.5%) and rectum (n = 23; 9.4%). Detailed of biopsy sites and abnormal findings in pediatric gastrointestinal endoscopy are presented in Supplemental Table S4.
Final diagnoses and therapeutic interventions in pediatric gastrointestinal endoscopy
Final diagnoses in pediatric gastrointestinal endoscopy (n = 245).
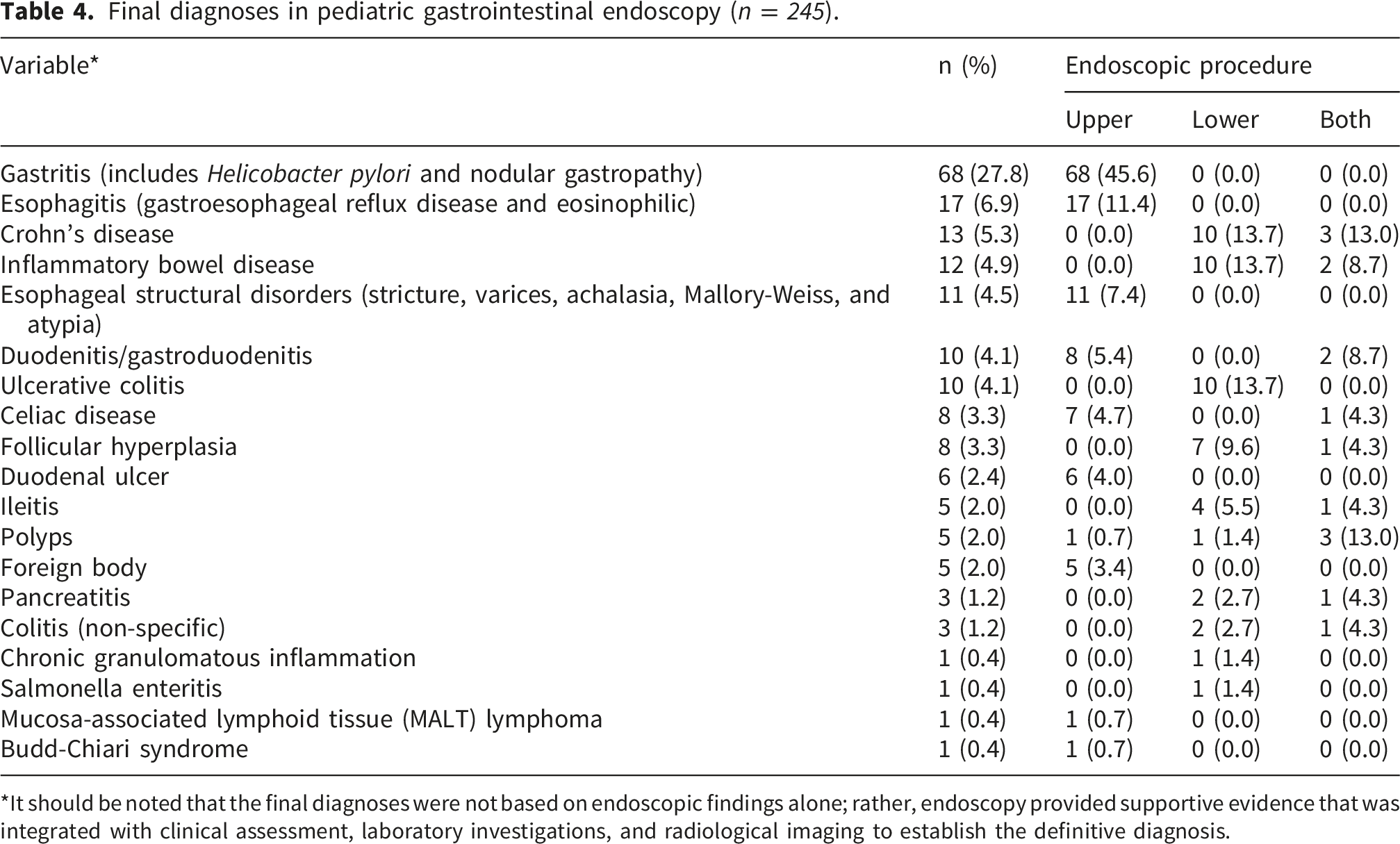
*It should be noted that the final diagnoses were not based on endoscopic findings alone; rather, endoscopy provided supportive evidence that was integrated with clinical assessment, laboratory investigations, and radiological imaging to establish the definitive diagnosis.
Therapeutic interventions were performed in 36 patients (14.7%), most commonly dilation (n = 15; 6.1%), stent placement (n = 5; 2.0%), and polyp removal (n = 5; 2.0%) (Supplemental Table S5). Less frequent interventions included foreign body removal (n = 4; 1.6%), hemostasis (n = 2; 0.8%), and percutaneous endoscopic gastrostomy tube insertion (n = 1; 0.4%).
Associations between characteristics of pediatric patients and type of gastrointestinal endoscopy
Bivariate analysis of associations between characteristics of pediatric patients and type of gastrointestinal endoscopy.
Associations between characteristics of pediatric patients and type of sedation
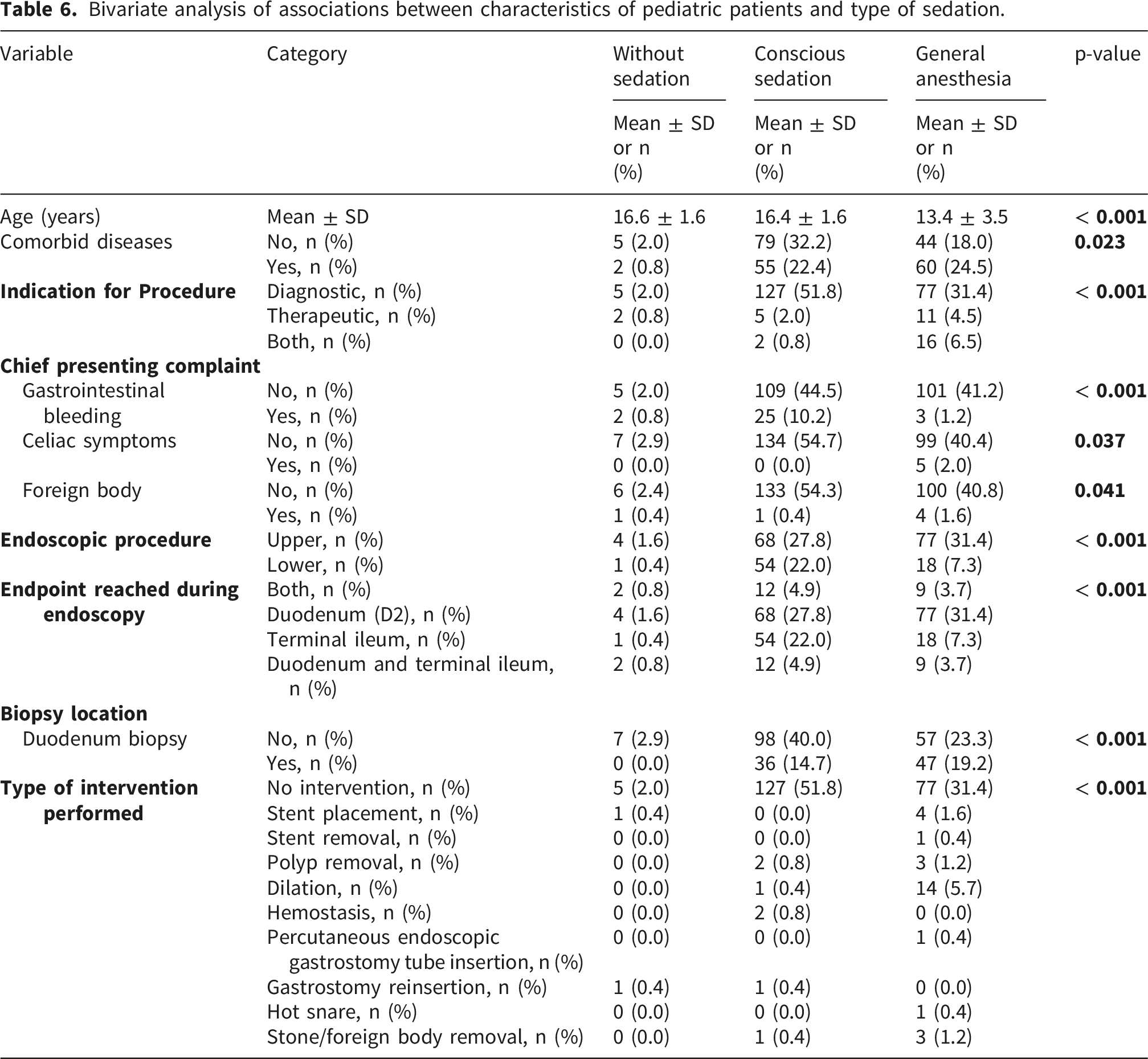
Bivariate analysis of associations between characteristics of pediatric patients and type of sedation.
Associations between characteristics of pediatric patients and submission of biopsy for histopathology
Bivariate analysis of associations between characteristics of pediatric patients and submitting biopsy for histopathology.
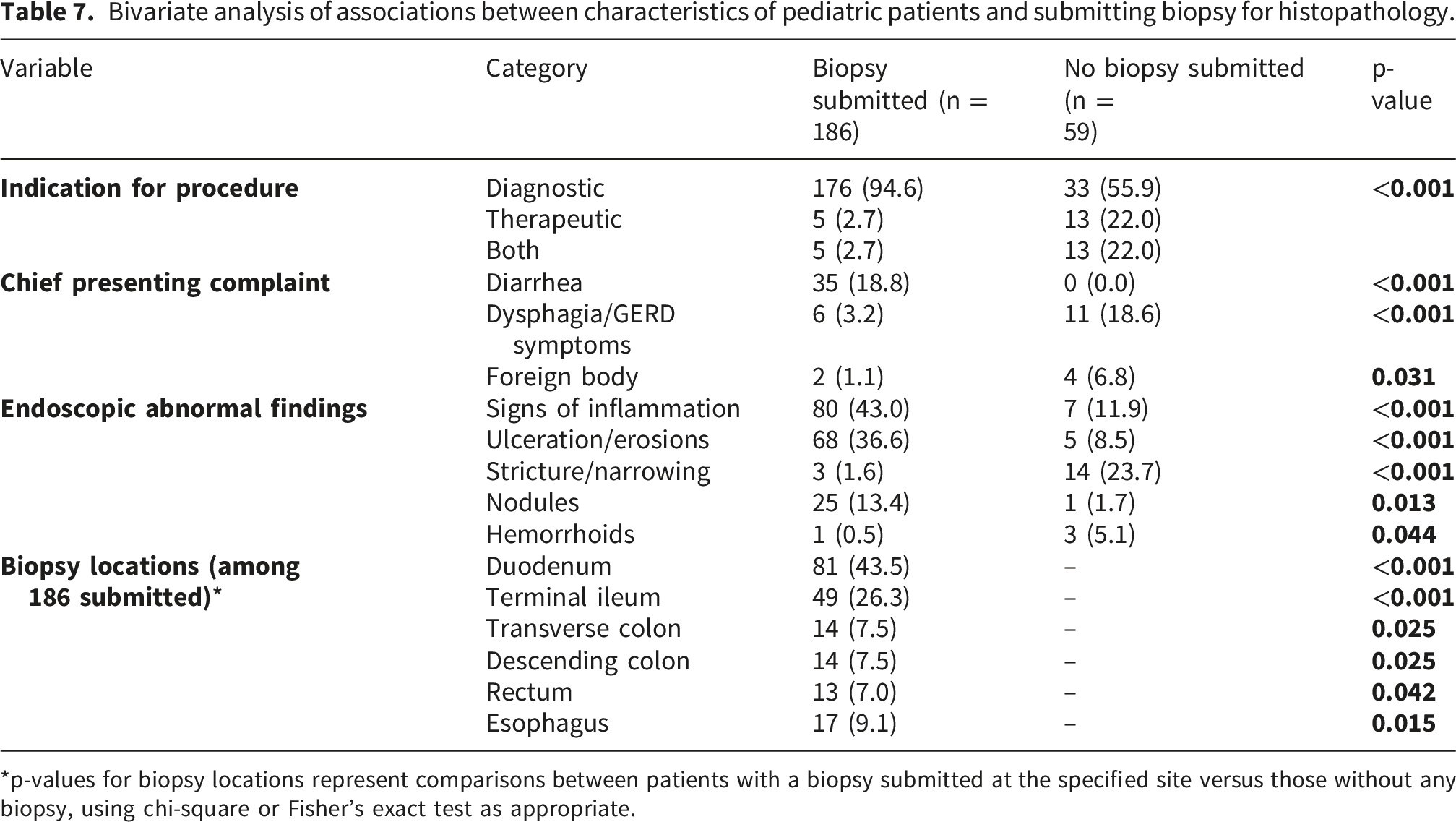
*p-values for biopsy locations represent comparisons between patients with a biopsy submitted at the specified site versus those without any biopsy, using chi-square or Fisher’s exact test as appropriate.
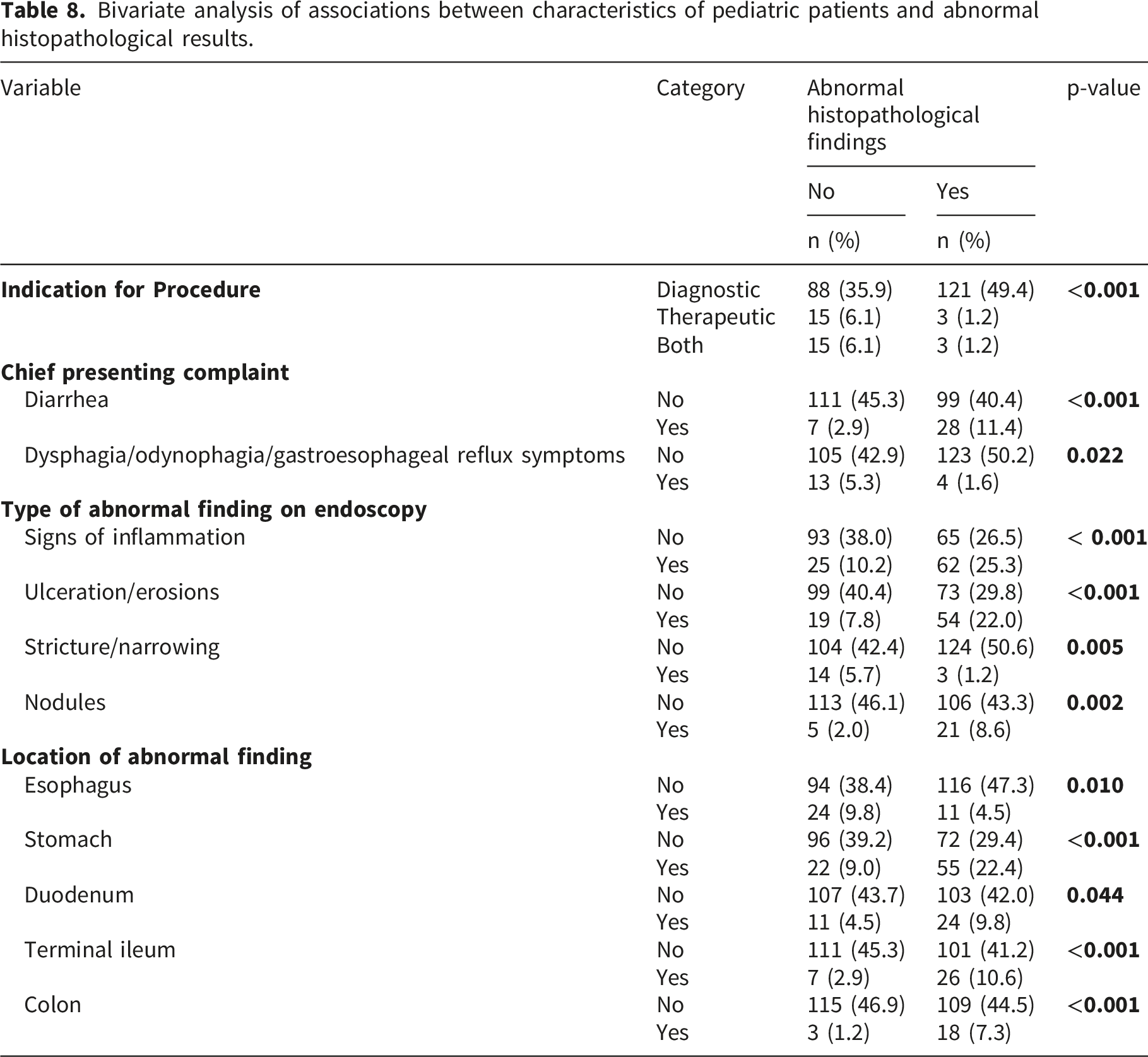
Associations between characteristics of pediatric patients and abnormal histopathological results
Bivariate analysis of associations between characteristics of pediatric patients and abnormal histopathological results.
Discussion
Pediatric gastrointestinal endoscopy is central to timely diagnosis and targeted therapy in children, especially where clinical uncertainty and limited resources intersect.1,3–5,9 This multicenter retrospective study set out to characterize indications, sedation practices, and outcomes across Palestinian hospitals, providing the first multicenter evidence base from Palestine on real-world pediatric endoscopy. Among 245 pediatric patients, diagnostic upper endoscopy predominated (60.8%), abdominal pain was the leading indication (28.2%), and abnormal endoscopic findings were common (75.5%), with gastritis the most frequent final diagnosis (27.8%). Sedation patterns reflected pragmatic adaptation to capacity as conscious sedation was used in 54.7% and general anesthesia in 42.4%, while histopathology was pursued in 75.9% with abnormalities in 51.8%. These findings are directly informative for pediatric gastroenterologists, anesthesiologists, endoscopy nurses, and hospital administrators, and they offer actionable signals for policymakers and training programs seeking to standardize protocols, optimize sedation safety, and improve diagnostic yield in resource-limited settings.
Biopsy decisions in our cohort were primarily guided by diagnostic intent and the presence of abnormal mucosal findings such as inflammation, ulceration, or nodules. In contrast, procedures performed for therapeutic purposes (e.g., foreign body removal) and those with macroscopically normal mucosa were less frequently biopsied. This selective approach reflects both clinical judgment and resource considerations, and is consistent with international pediatric endoscopy practice, where biopsies are prioritized when histopathology is expected to add diagnostic value. When compared with international experiences, our findings show both similarities and context-specific differences. The overall diagnostic yield of abnormal findings in our cohort (75.5%) is consistent with reports from Europe and North America.1,3–5,9 However, our data were slightly higher than those reported in Egypt. 23 Sedation practices in our study differ from high-income countries, where anesthesiologist-administered propofol sedation predominates. 27 Biopsy submission rates in our cohort were lower than those reported in Western centers, reflecting opportunities to strengthen biopsy protocols.1,28 Finally, while pediatric endoscopies in high-income countries are typically performed by pediatric gastroenterologists, in Palestine and other resource-limited settings adult gastroenterologists often contribute to pediatric procedures, highlighting workforce challenges and the importance of pediatric-specific training.9,29
The predominance of conscious sedation and general anesthesia in this cohort reflects pragmatic adaptation to resource availability. International surveys, such as the European Society of Gastrointestinal Endoscopy (ESGE) report, show wide heterogeneity in sedation practices across Europe, with propofol increasingly favored where anesthesiologist support is available.2,14 In contrast, resource-limited healthcare settings often rely more heavily on benzodiazepine-opioid combinations due to cost and staffing constraints.2,14,24,25 Midazolam and fentanyl were the predominant agents, with midazolam most often administered at 5 mg and fentanyl at 100 mcg. These regimens are broadly consistent with international practice, where midazolam and fentanyl are commonly used, but they highlight the need for standardized pediatric-specific dosing guidelines in Palestine.1,23,28 Clear documentation of dosing is essential for developing safe, reproducible sedation protocols and for training programs in resource-limited healthcare systems. The Palestinian experience underscores this global disparity. While midazolam and fentanyl were frequently used, propofol remained rare. This suggests that expanding anesthesiology support and training could improve access to propofol-based protocols, which have been associated with shorter recovery times and fewer adverse events in children.8,14,24,30,31 A recommendation here is to develop standardized sedation pathways tailored to resource-limited settings, ensuring safety while gradually integrating newer agents as capacity allows.
The high proportion of abnormal endoscopic and histopathological findings in this study highlights the appropriateness of referrals and the diagnostic value of pediatric endoscopy in Palestine. Comparable studies in Europe report diagnostic yields of 40-60% depending on indication,22,23,32–35 while this cohort demonstrated even higher yields, particularly for gastritis and inflammatory bowel disease-related changes. This may reflect selective referral patterns in resource-limited systems, where only children with severe or persistent symptoms are prioritized for endoscopy.36–38 The implication is that endoscopy services are being used judiciously, but the high burden of pathology also signals unmet needs in early detection. Strengthening referral guidelines and expanding access could allow earlier diagnosis of conditions like celiac disease and Crohn’s disease, reducing long-term morbidity.
Although therapeutic interventions were less frequent, their presence demonstrates the expanding role of pediatric endoscopy beyond diagnosis. International reports emphasize that therapeutic procedures, such as dilation, polypectomy, and foreign body removal, are increasingly integral to pediatric practice.3,4,6,8,24 The relatively modest rates in Palestine likely reflect both the early stage of service development and limited availability of specialized equipment.5,9 However, the successful performance of dilation and stent placement indicates growing technical capacity. Recommendations include investment in advanced pediatric endoscopic tools and training, which would reduce reliance on surgical interventions and improve outcomes for children with structural or obstructive lesions.
The predominance of abdominal pain and diarrhea as leading indications aligns with global pediatric practice, where nonspecific complaints often drive referrals.22,23 However, the relatively high rates of gastrointestinal bleeding and anemia symptoms in this cohort suggest that children are often referred at later stages of disease progression. This contrasts with data from high-income countries, where surveillance and early referral for subtle symptoms are more common. 23 The implication is that strengthening primary care recognition of gastrointestinal disorders and lowering thresholds for referral could improve early diagnosis. Educational interventions for pediatricians and family physicians may help standardize referral practices and reduce delays.
Taken together, these findings emphasize the need for capacity building in pediatric endoscopy services in Palestine. International reviews stress that sedation safety, diagnostic yield, and therapeutic capability are closely linked to workforce training and institutional protocols.5,23 This study provides baseline evidence that can inform national guidelines, support training curricula for anesthesiologists and gastroenterologists, and guide investment in equipment. Policymakers should prioritize the integration of standardized sedation protocols, expansion of histopathology services, and development of therapeutic endoscopy capacity. These steps would align Palestinian practice with international standards while respecting local resource constraints.
Taken together, the findings of this study provide a unique and timely contribution to pediatric gastroenterology in Palestine, where endoscopy services are still developing within a resource-limited healthcare system. The high diagnostic yield, frequent histopathological abnormalities, and pragmatic sedation practices observed here underscore both the clinical value of pediatric endoscopy and the systemic challenges that shape its use. Compared with international cohorts, Palestinian children appear to undergo endoscopy later in the disease course, which explains the high burden of gastritis, inflammatory bowel disease-related changes, and ulcerative lesions. This highlights the need for earlier referral pathways and stronger primary care awareness of gastrointestinal disorders. The reliance on benzodiazepine-opioid sedation, with limited use of propofol, reflects global disparities in resource allocation and anesthesiology support. While safe and effective within current constraints, these practices call for capacity building in sedation training and infrastructure, aligning with international recommendations for pediatric endoscopy safety. Similarly, the relatively modest rates of therapeutic interventions demonstrate growing technical capacity but also emphasize the need for investment in advanced pediatric endoscopic tools. Ultimately, this study provides the first systematic evidence base for pediatric endoscopy in Palestine, offering actionable insights for clinicians, hospital administrators, and policymakers. The results can inform the development of national guidelines, support training curricula for pediatric gastroenterologists and anesthesiologists, and guide resource allocation to strengthen diagnostic and therapeutic endoscopy services. By situating Palestinian practice within the broader international context, this work lays the foundation for standardization, safety optimization, and improved outcomes for children across the region.
This study was deliberately restricted to pediatric patients, as the objective was to characterize clinical indications, sedation practices, and outcomes of gastrointestinal endoscopy in children. Adult patients were not included, and therefore no comparative data are available in this cohort. It is noteworthy, however, that in many resource-limited healthcare systems, including Palestine, pediatric endoscopies are often performed not only by pediatric gastroenterologists but also by adult gastroenterologists due to workforce constraints and limited subspecialty training programs. This overlap in practice underscores the importance of developing standardized pediatric-specific protocols and training pathways to ensure optimal safety and diagnostic yield in children.
Strengths and limitations
A major strength of this study lies in its multicenter design, which captured pediatric endoscopy practices across multiple hospitals in the West Bank. This provided a broad and representative view of clinical indications, sedation strategies, and outcomes in a resource-limited healthcare system. The use of a structured data extraction form, piloted and refined before full implementation, enhanced consistency and reproducibility. Adherence to the STROBE checklist further strengthened methodological transparency and reporting quality. A key strength of this study is that final diagnoses were established through a multidisciplinary approach rather than relying solely on endoscopic findings. Endoscopy served as an essential diagnostic tool, but its results were consistently corroborated with clinical assessment, laboratory investigations, and radiological imaging. This integrated approach minimized misclassification, enhanced diagnostic accuracy, and ensured that rare conditions such as Budd-Chiari syndrome or MALT lymphoma were confirmed through appropriate complementary modalities. By combining endoscopic evidence with broader clinical and investigative data, the study provides a more reliable and comprehensive characterization of pediatric gastrointestinal disorders in a resource-limited healthcare system. Importantly, this is the first systematic study of pediatric endoscopy in Palestine, offering baseline evidence that can inform clinical guidelines, training programs, and policy development.
Nevertheless, some limitations should be acknowledged. First, the retrospective design inherently relies on the accuracy and completeness of medical records, which may introduce information bias. Although patients with incomplete records were excluded, this may have led to selection bias by disproportionately omitting certain cases. It is important to note that no major sedation-related or procedure-related complications were documented in this cohort. Minor adverse events such as transient hypoxia or post-procedure abdominal discomfort were not systematically recorded in the hospital records and therefore could not be analyzed. While the absence of documented major complications in our cohort can be reassuring and consistent with international reports that pediatric endoscopy is generally safe when performed under appropriate sedation and monitoring. However, the retrospective design may have underestimated minor adverse events, as these are often under-reported in routine records. Future prospective studies with standardized complication reporting are warranted to provide a more comprehensive safety profile. Second, the study was limited to hospitals in the West Bank, and findings may not fully generalize to other regions of Palestine or neighboring countries with different healthcare infrastructures. Third, the reliance on convenience sampling means that the cohort may not perfectly reflect the broader pediatric population, particularly those who did not access tertiary care. Finally, while bivariate analyses provided valuable associations, the absence of multivariate modeling limited the ability to control for potential confounders such as socioeconomic status, nutritional factors, or referral pathways.
Despite these limitations, the study provides robust and novel insights into pediatric endoscopy in a resource-limited setting, establishing a foundation for future prospective studies, multicenter collaborations, and capacity-building initiatives.
Conclusion
This multicenter study provides the first systematic evidence on pediatric gastrointestinal endoscopy in Palestine, revealing that the majority of procedures were diagnostic, most children presented with abdominal pain or diarrhea, and abnormal findings were highly prevalent, particularly gastritis and inflammatory bowel disease-related changes. Sedation practices were dominated by conscious sedation and general anesthesia, reflecting pragmatic adaptation to limited resources, while therapeutic interventions, though less frequent, demonstrated growing technical capacity. Together, these findings underscore both the clinical value of pediatric endoscopy and the urgent need to strengthen infrastructure, standardize sedation protocols, and expand training to optimize safety and diagnostic yield. By situating Palestinian practice within the global context, this study offers actionable insights for clinicians, hospital administrators, and policymakers committed to improving pediatric gastroenterology services in resource-limited settings.
Supplemental material
Supplemental Material - Clinical indications and outcomes of pediatric gastrointestinal endoscopy in a resource-limited healthcare system: Findings from the first multicenter study
Supplemental Material for Clinical indications and outcomes of pediatric gastrointestinal endoscopy in a resource-limited healthcare system: Findings from the first multicenter study by Shahd Abu Halima, Khadija Salhab, Bayan Al-Thuluth, Ayah Nassar, Iyad Maqboul, Mohammad Jaber, Ramzi Shawahna in Sage Open Medicine
Footnotes
Acknowledgments
An-Najah National University (https://www.najah.edu/) and An-Najah National University Hospital (![]() ) are acknowledged for making this study possible. The authors would like to thank the participating hospitals.
) are acknowledged for making this study possible. The authors would like to thank the participating hospitals.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and adhered to internationally recognized standards for research involving human participants. The study received ethical approval from the Institutional Review Board (IRB) of An-Najah National University and the participating hospitals (approval #: NNU-IRB: Pharm/12-24/53). Given the retrospective design, data were extracted from hospital electronic health records without direct patient contact, the IRB formally waived the requirement to obtain written informed consent from the legally authorized representatives of pediatric patients as well as assent from the pediatric patients. Similarly, the IRB formally waived the requirement to obtain written informed consent from the 18 years old patients. Throughout the study, strict measures were taken to ensure privacy and confidentiality. All data were anonymized prior to analysis, and no identifying information such as names, medical record numbers, or personal details were included in the dataset or reported in the manuscript. Access to patient records was restricted to authorized members of the research team, and data were stored securely in compliance with institutional policies. These safeguards ensured that the rights and welfare of the pediatric patients were fully respected while enabling the generation of valuable evidence to inform clinical practice in resource-limited healthcare settings.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Data Availability Statement
All data analyzed in this study were included in the manuscript. The datasets used in the analysis or entered into statistical software can be obtained from the corresponding author upon making a reasonable request.
Declaration of generative AI and AI-assisted technologies in the writing process
In line with the journal’s policy on transparency, the authors wish to declare that during the preparation of the manuscript, the authors used Grammarly (Superhuman Platform Inc., San Francisco, California), Copilot (Microsoft Inc., Redmond, Washington), and ChatGPT (OpenAI, San Francisco, California) solely to edit the language and improve grammar, spelling, punctuation, readability, and style of the manuscript. After using these tools/services, the authors reviewed and edited the content as needed and take full responsibility for the scientific content, accuracy, and integrity of the manuscript. Artificial intelligence tools/services were not used for generative editorial work, autonomous content creation, data analysis, statistical interpretation, or the generation of scientific content.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.