
Abstract
Objectives
To determine the prevalence of electrocardiographic (ECG) abnormalities in diabetic ketoacidosis (DKA) patients, evaluate their associations with metabolic parameters, and identify independent predictors of clinical outcomes.
Methods
This retrospective study included 374 DKA patients (2012-2023). Baseline clinical characteristics, laboratory data, and initial ECG findings were analyzed. Multivariable logistic regression was performed to assess associations between metabolic parameters and corrected QT (QTc) prolongation, as well as clinical outcomes.
Results
Sinus tachycardia occurred in 54.8%, while QTc prolongation was found in 64.7% of patients using Bazett’s formula versus 27.5% using Fridericia’s correction. In multivariable analysis, lower serum bicarbonate levels were independently associated with QTc prolongation using both formulas (Bazett’s: adjusted OR 0.92, 95%CI 0.87–0.98, p=0.007; Fridericia’s: adjusted OR 0.91, 95%CI 0.85–0.97, p=0.002). These associations remained consistent across different QTc thresholds, including high-risk and very high-risk QTc prolongation. However, QTc prolongation was not independently associated with length of stay or in-hospital mortality.
Conclusions
QTc prolongation was frequently observed in patients with DKA and showed an association with the severity of metabolic acidosis, particularly reduced serum bicarbonate levels. Given its potential implication for arrhythmogenic risk, careful ECG assessment and monitoring should be considered during the initial evaluation and management of DKA.
Keywords
1. Introduction
Diabetic ketoacidosis (DKA) is an acute and potentially life-threatening complication of diabetes mellitus (DM), characterized by hyperglycemia and ketoacidosis, and requires prompt medical management.1,2 Electrolyte disturbances are frequently encountered in patients with uncontrolled DM and DKA, commonly involving sodium, potassium, bicarbonate, calcium, magnesium, and phosphorus. 3 These imbalances arise through diverse pathophysiological mechanisms. For example, metabolic acidosis arises from ketonemia and declining renal function; hypernatremia and hypomagnesemia are precipitated by osmotic diuresis; hyponatremia results from osmotically induced water shifts; and hypokalemia may occur following insulin therapy. 4
Potassium, calcium, and magnesium imbalances are well-recognized causes of significant electrocardiographic (ECG) abnormalities and life-threatening cardiac arrhythmias. 5 Hypokalemia, frequently observed in DKA, typically manifests as T-wave flattening or inversion and ST-segment depression; in severe cases, this may progress to prominent U waves, corrected QT (QTc) prolongation, torsades de pointes (TdP), ventricular tachycardia (VT), or ventricular fibrillation (VF). In contrast, hyperkalemia is characterized by peaked T waves, P-wave flattening, and PR-interval prolongation, which may progress to atrioventricular block or VF.5–7 Hypocalcemia characteristically results in QTc prolongation, whereas hypercalcemia is associated with QTc shortening.3,8 While hypomagnesemia often lacks pathognomonic ECG findings, it can potentiate QTc prolongation and life-threatening arrhythmias through synergistic interactions with concurrent potassium or calcium imbalances.5,9
Despite the high prevalence of electrolyte imbalances in DKA 3 and their potential to induce significant ECG manifestations, such as QTc prolongation associated with hypokalemia, clinical evidence regarding these relationships remains limited. 10 Existing literature is largely constrained by small sample sizes 11 and a predominant focus on pediatric cohort populations.12–15 To address this gap, we conducted a larger-scale retrospective cohort study to characterize the prevalence of ECG abnormalities in adults with DKA and to examine their associations with demographic factors, metabolic parameters, electrolyte disturbances, and clinically relevant outcomes.
2. Materials and methods
2.1 Participants
This retrospective cohort study included patients aged ≥ 15 years admitted to a single-center, university-based hospital between July 1, 2012, and December 31, 2023. Eligible participants were identified by a primary or secondary diagnosis of DKA using the International Classification of Diseases, 10th Revision (ICD-10) codes E10.1, E11.1, E12.1, E13.1, and E14.1. 16 Exclusion criteria comprised the absence of admission ECG data, incomplete biochemical profiles—specifically missing serum electrolytes or parameters required for DKA severity assessment (e.g., serum electrolyte, blood pH or serum beta-hydroxybutyrate); and documented use of QT interval–prolonging medications 17 at the time of presentation (Table S1). Clinical and biochemical data were extracted from the hospital’s electronic medical record database. This study received ethical approval from the institutional Human Research Ethics Committee and was performed in compliance with the Declaration of Helsinki.
2.2 Data collection
Baseline demographic data included age, sex, body mass index (BMI), type of DM, comorbidities, and concomitant medications, with a specific focus on insulin therapy. Admission laboratory parameters included plasma glucose, glycated hemoglobin (HbA1c), serum beta-hydroxybutyrate, creatinine, and blood pH. A comprehensive electrolyte panel was also recorded, including sodium, potassium, chloride, bicarbonate, calcium, and magnesium. Analysis was strictly limited to the first laboratory values obtained upon hospital admission.
Standard 12-lead ECGs were obtained at the time of DKA diagnosis. ECG parameters assessed from the initial ECG included heart rate, rhythm, axis, P-wave morphology, PR interval, presence of Q waves, QRS duration, ST-segment changes, T-wave morphology, presence of U waves, and the QTc-interval. QT intervals were obtained from the automated ECG reporting system, and QTc values were subsequently calculated by the investigators using both Bazett’s 18 and Fridericia’s formulas. 19 Although Bazett’s formula is widely used in clinical practice, the Fridericia correction was applied due to its greater reliability in the setting of heart rate abnormalities. 20 Unlike Bazett’s formula, which overcorrects the QT interval at higher heart rates, Fridericia’s formula is less confounded by heart rate changes. QTc prolongation was defined as ≥ 450 ms in males and ≥ 460 ms in females. 21 For both sexes, high-risk and very high-risk QTc prolongation were defined as ≥ 480 ms and ≥ 500 ms, respectively.21,22 All ECGs were independently interpreted by an experienced cardiologist (V.P.) who was blinded to the patients’ demographic and biochemical data.
2.3 Outcomes
The primary outcome was the prevalence of ECG abnormalities in DKA and their association with metabolic parameters, with a particular focus on QTc prolongation. Secondary outcomes included assessing the impact of demographic factors, metabolic status, and ECG findings on clinical outcomes.
2.4 Data analyses
The sample size was based on a reported QTc prolongation prevalence of 60% among patients with DKA, as described by Talebi et al. 11 Using a single population proportion formula with a 5% margin of error, a 95% confidence level (α = 0.05), and a standard normal deviate (Z = 1.96), the minimum required sample size was of 368 participants.
All statistical analyses were performed using STATA statistical software version 18 (Stata Corp, LLC, College Station, TX). Descriptive statistics were used to summarize baseline demographic, clinical characteristics, ECG findings, and clinical outcomes. Categorical variables are presented as counts and percentages. Continuous variables are reported as mean ± SD for normally distributed data and as median (interquartile range [IQR]: 25th-75th percentiles) for non-normally distributed data. Normality was assessed using the Kolmogorov–Smirnov test.
Univariate analyses were conducted to assess associations between baseline characteristics and ECG findings, with particular emphasis on comparisons across QTc correction formulas and QTc prolongation thresholds. We further evaluated the relationships between these variables and clinical outcomes, including length of hospital stay (LOS) and all-cause mortality. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate, while continuous variables were analyzed using the independent t-test or Mann–Whitney U test, depending on data distribution.
Multivariable analyses were performed to identify independent predictors of ECG findings and clinical outcomes. Variables with p-value < 0.10 in univariate analyses, along with clinically relevant factors and potential confounders, were included in the models. Logistic regression was used for categorical outcomes, and linear regression was applied to continuous outcomes. Results from logistic regression are presented as odds ratios (ORs) with 95% confidence intervals (CIs), whereas results from linear regression are reported as regression coefficients (β) with 95% CIs. A two-sided p-value < 0.05 was considered statistically significant. Multicollinearity among the independent variables was assessed using variance inflation factors (VIFs). For logistic regression models, goodness-of-fit was evaluated using the Hosmer–Lemeshow test, and discrimination was assessed using the area under the receiver operating characteristic curve (AUC).
3. Results
A total of 716 patients with DKA were initially screened. After applying the exclusion criteria, 374 patients were included in the final analysis, representing 52% of the initially screened patients. The main reasons for exclusion were potential drug-induced arrhythmias (21%), age <15 years (12%), and unavailable ECG data at diagnosis (9%) (Figure 1). Study flow diagram of patient selection. DKA = Diabetic Ketoacidosis. ECG = Electrocardiogram.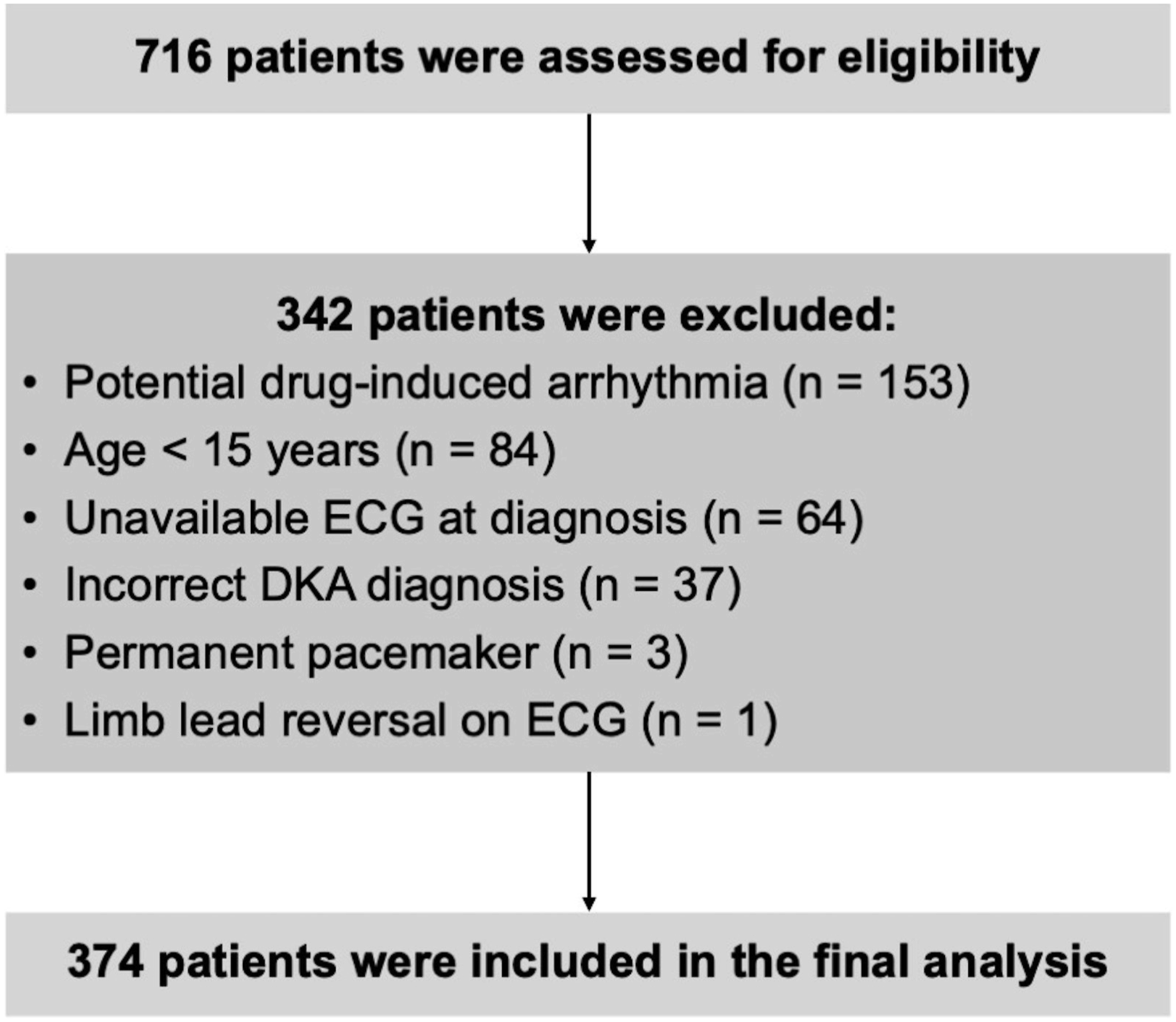
3.1 Baseline characteristics (Table 1)
Baseline characteristics.
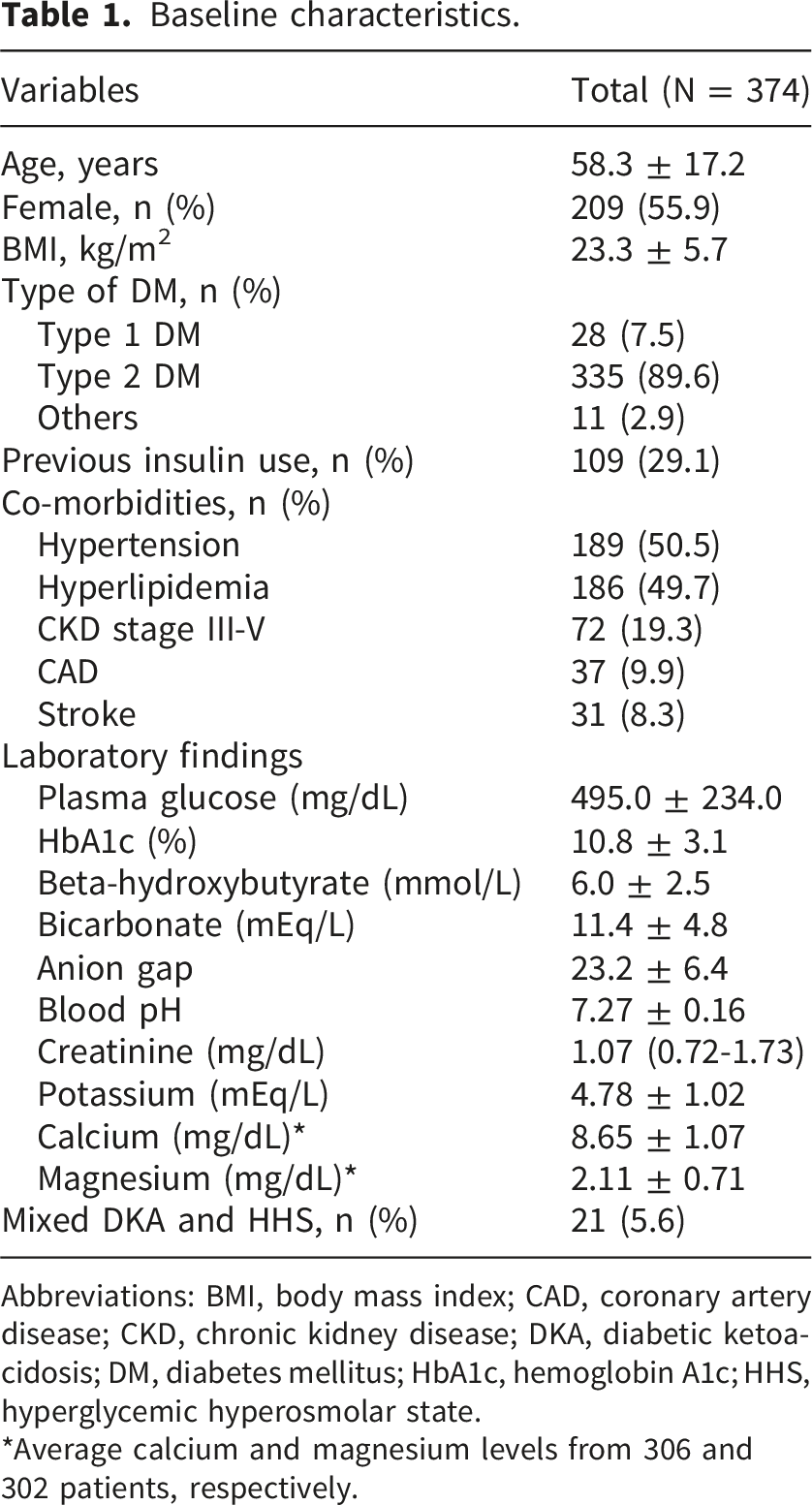
Abbreviations: BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; DKA, diabetic ketoacidosis; DM, diabetes mellitus; HbA1c, hemoglobin A1c; HHS, hyperglycemic hyperosmolar state.
*Average calcium and magnesium levels from 306 and 302 patients, respectively.
The mean plasma glucose level was 495.0 ± 234.0 mg/dL, and the mean recent HbA1c was 10.8 ± 3.1%. The mean serum beta-hydroxybutyrate was 6.0 ± 2.5 mmol/L, serum bicarbonate was 11.4 ± 4.8 mEq/L, the anion gap was 23.2 ± 6.4, and pH was 7.27 ± 0.16. Mixed DKA and hyperglycemic hyperosmolar state (HHS) were observed in 5.6% of patients. Other laboratory findings included a mean serum potassium level of 4.78 ± 1.02 mEq/L and a median creatinine level of 1.07 (0.72–1.73) mg/dL. The mean calcium and magnesium levels were 8.65 ± 1.07 mg/dL and 2.11 ± 0.71 mg/dL, with data available for 306 and 302 patients, respectively, out of the 374 total patients.
3.2 ECG findings (Table 2)
ECG findings and QTc measurements according to different correction formulas.
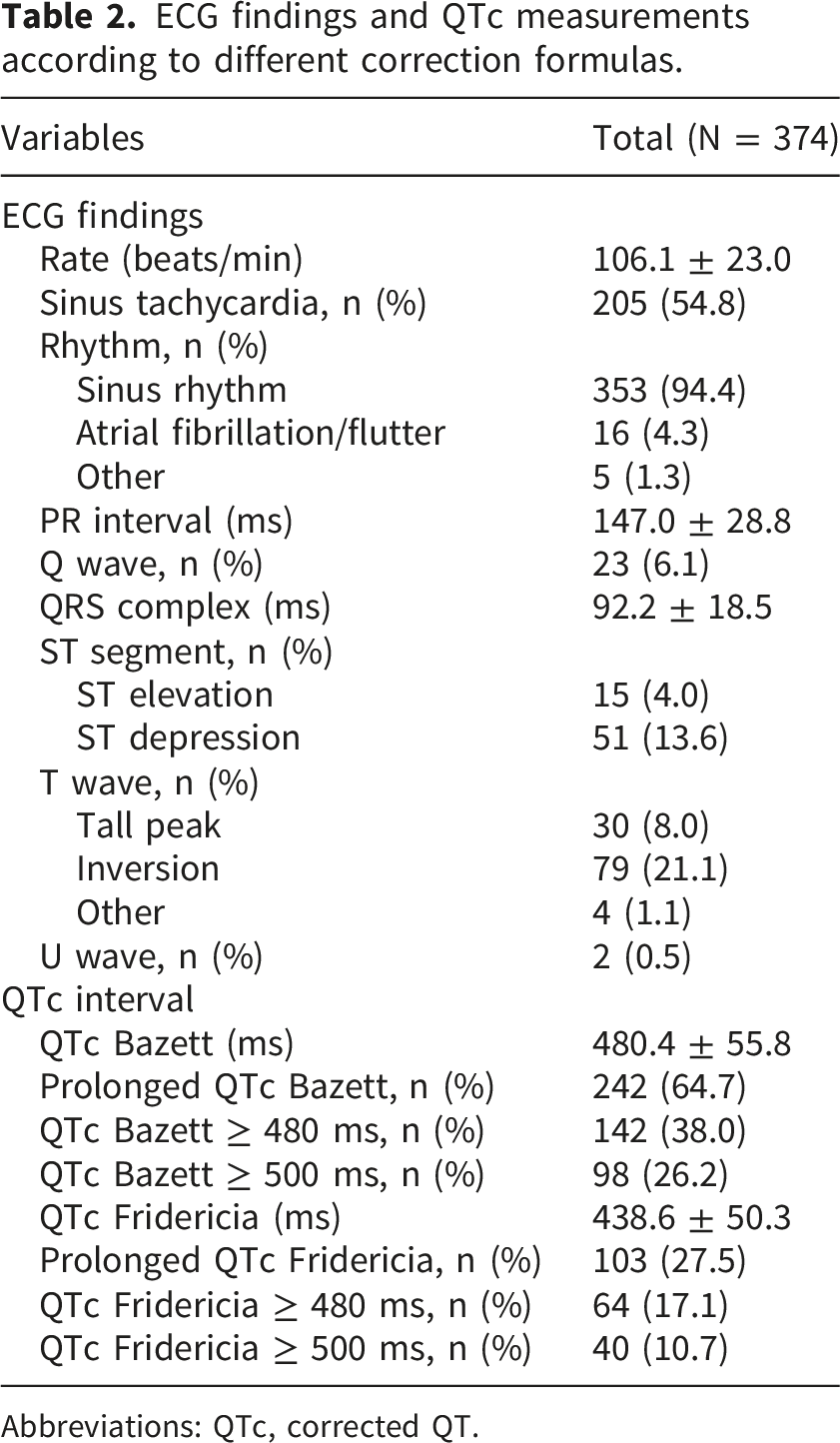
Abbreviations: QTc, corrected QT.
The mean QTc interval was 480.4 ± 55.8 ms using the Bazett’s formula and 438.6 ± 50.3 ms using Fridericia’s formula. QTc prolongation was observed in 64.7% of patients using Bazett’s correction and 27.5% using Fridericia’s correction. The prevalence of high-risk QTc prolongation was 38.0% with Bazett’s formula and 17.1% with Fridericia’s formula. The prevalence of very high-risk QTc prolongation was 26.2% and 10.7%, respectively. Additional ECG findings are presented in Table 2.
Based on the Bland-Altman analysis, Bazett’s formula yielded higher QTc values than the Fridericia’s formula, with a mean difference of approximately 42 ms. The Kappa coefficient for agreement between the two methods was 0.334.
3.3 Clinical outcomes
The median LOS was 9 (6-17) days, and the all-cause in-hospital mortality rate was 9.6%. The primary cause of death was infection (75.0%), followed by advanced malignancy (8.3%) and other causes (16.7%), which included bowel ischemia, stroke, and massive hemoptysis. No deaths were attributed to primary cardiac causes, including cardiac arrhythmia. In addition, no patients experienced life-threatening arrhythmias, such as TdP, VT, or VF.
3.4 Associations between baseline characteristics and QTc using different correction formulas
In the univariate linear regression analysis using the Bazett’s formula, the QTc interval was negatively associated with BMI (β: −0.87; p = 0.09), dyslipidemia (β: −0.97; p = 0.06), serum bicarbonate (β: −2.52; p < 0.001), and blood pH (β: −73.6; p < 0.001). Positive associations were observed with anion gap (β: 0.93; p = 0.04) and heart rate (β: 0.47; p < 0.001). Using Fridericia’s formula model, the QTc interval showed negative associations with serum bicarbonate (β: −1.61; p = 0.003), blood pH (β: −48.9; p = 0.003), and heart rate (β: −0.29; p = 0.01). The relationship between serum bicarbonate and QTc interval is illustrated in Figure 2. Correlation between serum bicarbonate levels and QTc intervals using (a) Bazett’s formula and (b) Fridericia’s formula (Blue dots: QTc intervals; Red lines: Fitted values).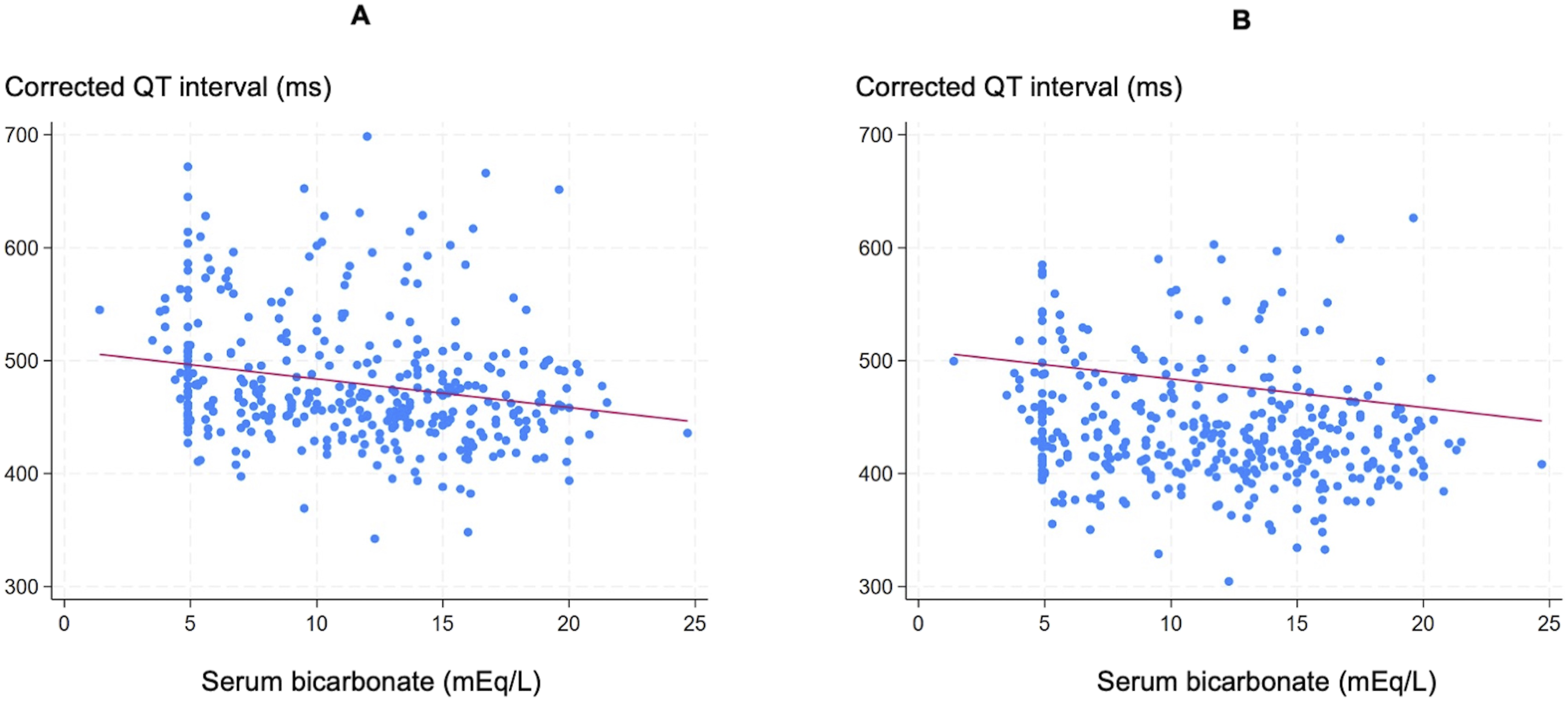
For standard QTc prolongation, variables negatively associated under Bazett’s formula included dyslipidemia (OR: 0.64; p = 0.04), ischemic stroke (OR: 0.48; p = 0.05), serum bicarbonate (OR: 0.93; p = 0.001), and blood pH (OR: 0.16; p = 0.02). Positive associations were observed with ischemic heart disease (OR: 2.11; p = 0.07), anion gap (OR: 1.04; p = 0.04), and heart rate (OR: 1.01; p = 0.08). Using the Fridericia formula, significant associations persisted for serum bicarbonate (OR: 0.92, p = 0.001) and blood pH (OR: 0.21, p = 0.03), while a marginal trend was observed for ischemic stroke (OR: 0.37, p = 0.07).
For high-risk QTc prolongation, Bazett’s formula identified negative associations with BMI (OR: 0.95; p = 0.02), HbA1c (OR: 0.94; p = 0.08), serum bicarbonate (OR: 0.91; p < 0.001), and blood pH (OR: 0.09; p < 0.001), while anion gap (OR: 1.04; p = 0.04) and heart rate (OR: 1.01; p = 0.004) were positively associated. Under Fridericia’s formula, associations were observed for serum bicarbonate (OR: 0.90; p = 0.001), blood pH (OR: 0.12; p = 0.01), serum calcium (OR: 0.78; p = 0.08), and anion gap (OR: 1.04; p = 0.09).
Regarding very high-risk prolongation, Bazett’s formula showed associations with serum bicarbonate (OR: 0.89; p < 0.001), blood pH (OR: 0.08; p = 0.001), and heart rate (OR: 1.02; p = 0.001). Under Fridericia’s formula, associations included serum bicarbonate (OR: 0.92; p = 0.03) and blood pH (OR: 0.13; p = 0.04).
Multivariable logistic regression analysis of predictors for prolonged QTc interval in patients with DKA.
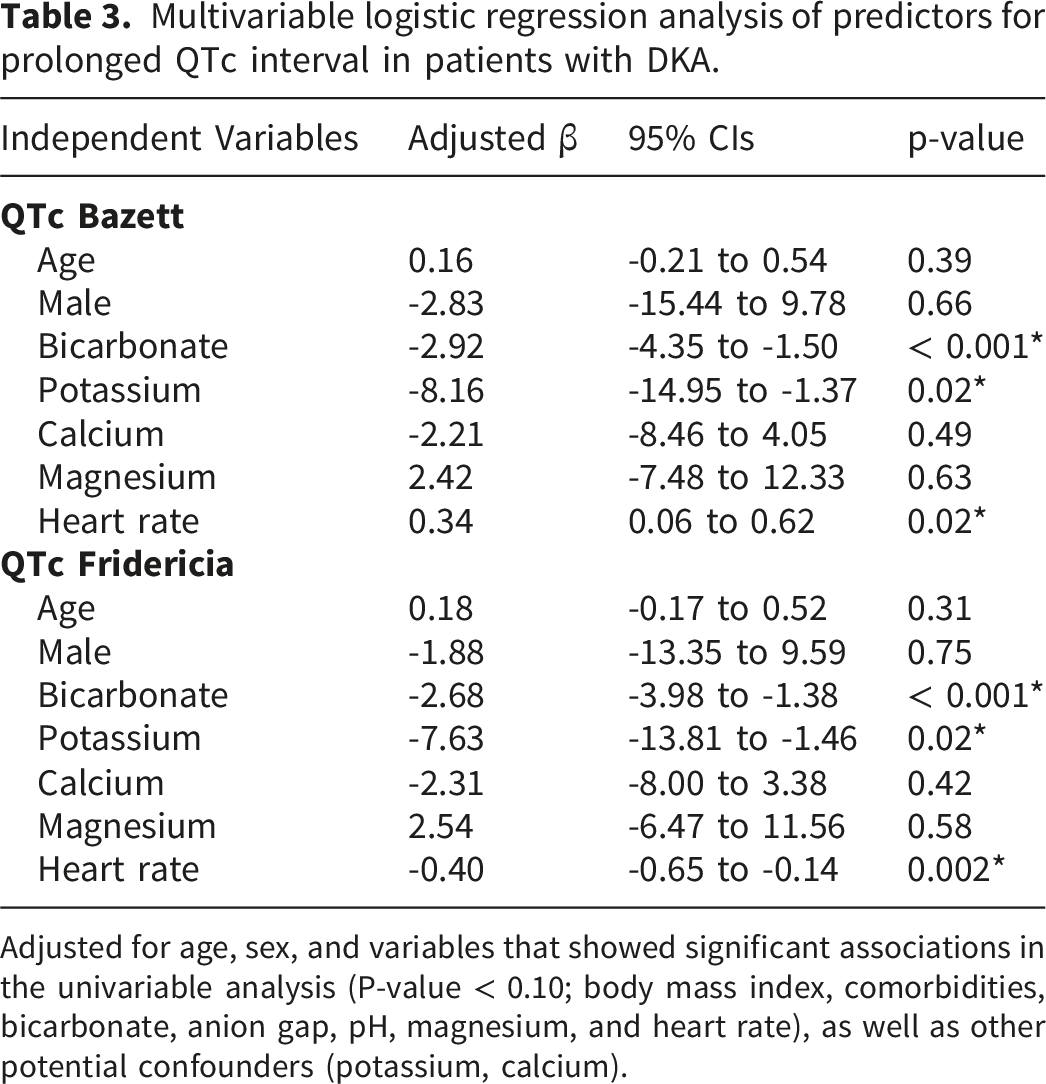
Adjusted for age, sex, and variables that showed significant associations in the univariable analysis (P-value < 0.10; body mass index, comorbidities, bicarbonate, anion gap, pH, magnesium, and heart rate), as well as other potential confounders (potassium, calcium).
For categorical QTc prolongation across different thresholds, lower serum bicarbonate remained independently associated with standard, high-risk, and very high-risk QTc prolongation for both correction formulas (Table S2.1 and S2.2). Furthermore, lower serum potassium was independently associated with high-risk and very high-risk QTc prolongation specifically when using the Fridericia correction (Table S2.2). For the logistic regression models, Hosmer–Lemeshow test p-values were > 0.05 for all models, and AUC values ranged from 0.62 to 0.68.
3.5 Associations between baseline characteristics and ECG finding with clinical outcomes
In univariate linear regression analysis, LOS was positively associated with age (β: 0.16; p = 0.008), hypertension (β: 4.13; p = 0.05), dyslipidemia (β: 4.80; p = 0.02), chronic kidney disease (β: 4.50; p = 0.09), serum bicarbonate (β: 0.60; p = 0.006), blood pH (β: 19.0; p = 0.004), and QRS complex interval (β: 0.16; p = 0.004). In contrast, LOS was negatively associated with serum beta-hydroxybutyrate (β: -0.85; p = 0.04), and anion gap (β: -0.53; p = 0.001).
For all-cause mortality, univariate analysis identified significant positive associations with age (OR: 1.04; p = 0.003), male sex (OR: 2.14; p = 0.03), hypertension (OR: 2.41; p = 0.02), and serum creatinine (OR: 1.16; p = 0.02).
Multivariable logistic regression analysis for clinical outcomes. Predictors for length of hospital stay in patients with DKA.
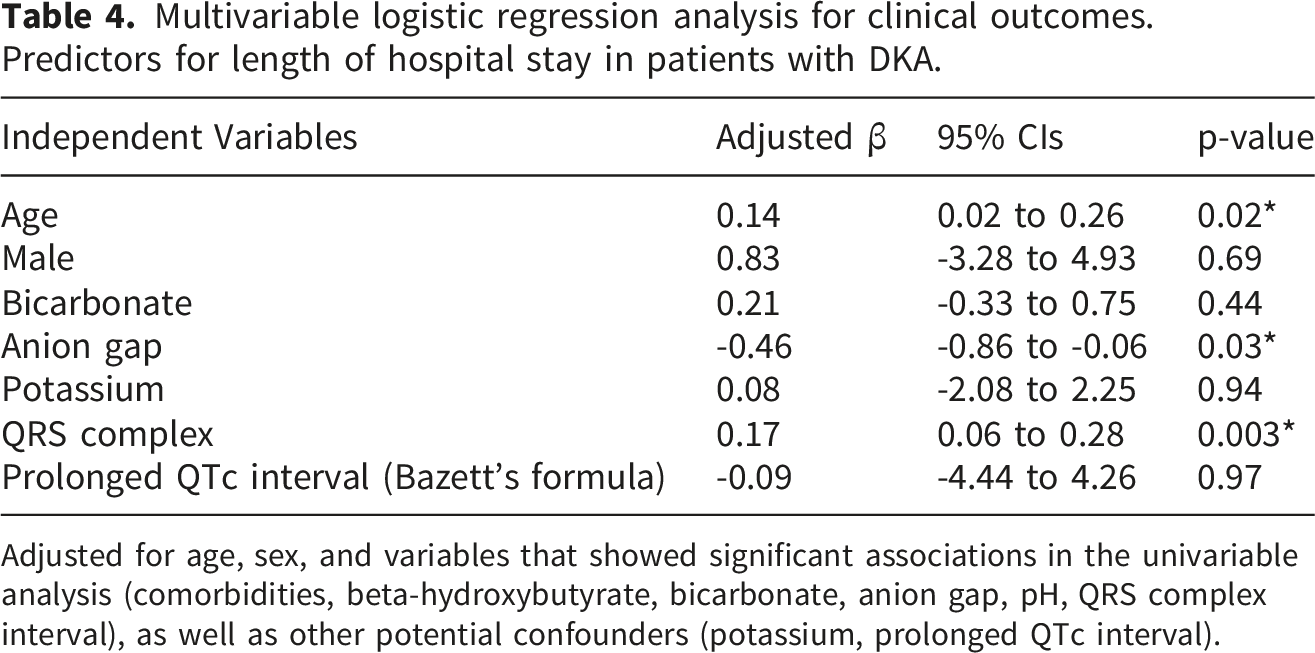
Adjusted for age, sex, and variables that showed significant associations in the univariable analysis (comorbidities, beta-hydroxybutyrate, bicarbonate, anion gap, pH, QRS complex interval), as well as other potential confounders (potassium, prolonged QTc interval).
Multivariable logistic regression analysis for clinical outcomes. Predictors for mortality in patients with DKA.
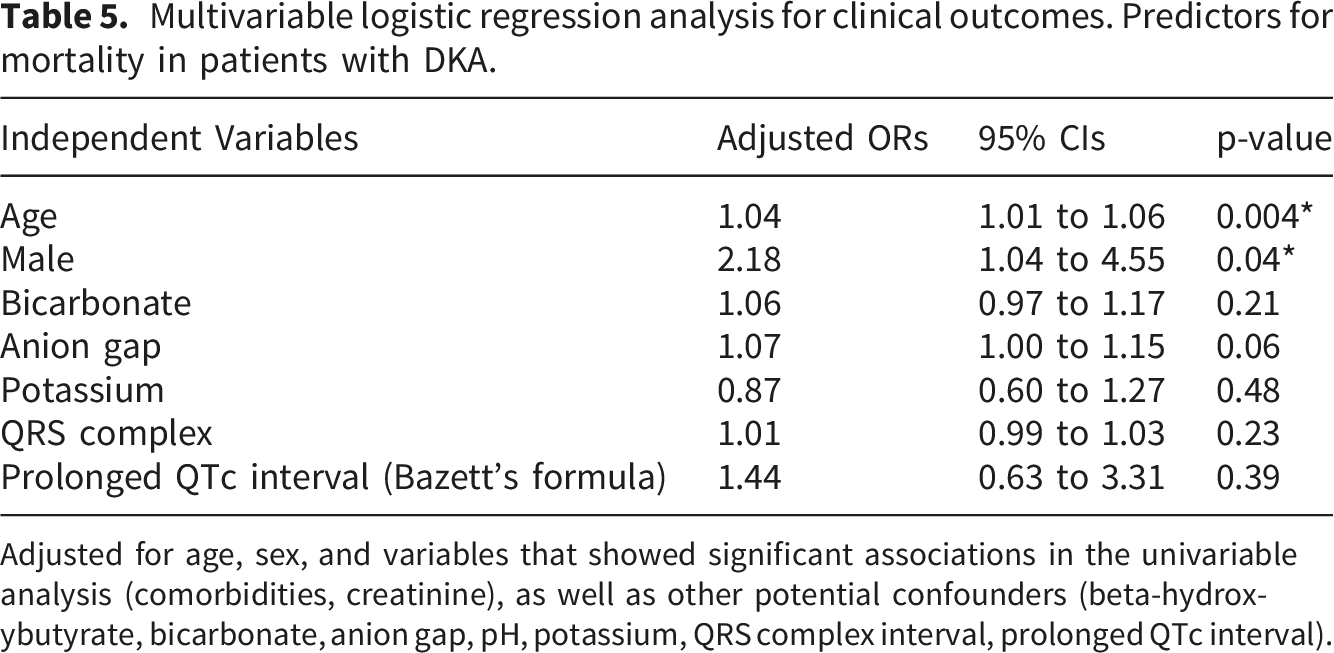
Adjusted for age, sex, and variables that showed significant associations in the univariable analysis (comorbidities, creatinine), as well as other potential confounders (beta-hydroxybutyrate, bicarbonate, anion gap, pH, potassium, QRS complex interval, prolonged QTc interval).
4. Discussion
This retrospective cohort study evaluated the associations between baseline clinical characteristics, metabolic parameters, and ECG findings in patients with DKA. Our results demonstrate a high prevalence of ECG abnormalities, most notably sinus tachycardia (mean heart rate ≈ 110 beats/minute) and QTc prolongation. A substantial disparity was observed between correction formulas, with QTc prolongation identified in 65% of patients using the Bazett’s formula compared with 28% using the Fridericia’s formula. Multivariable regression analysis demonstrated that QTc prolongation across all thresholds was primarily driven by the severity of metabolic acidosis, as represented by lower serum bicarbonate levels. Furthermore, lower serum potassium was independently associated with a longer QTc interval, a relationship particularly evident when using the Fridericia’s formula, which is more reliable in the setting of tachycardia.23–25 Regarding clinical outcomes, while advanced age was an independent predictor of both longer LOS and increased all-cause mortality, QTc prolongation was not significantly associated with these endpoints.
The discrepancy in QTc prolongation prevalence between Bazett’s and Fridericia’s formulas may reflect the influence of heart rate on QT correction. In our cohort, sinus tachycardia was common, affecting approximately 55% of patients, with a mean heart rate of 110 beats/minute. Under these conditions, Bazett’s formula may overcorrect QTc, resulting in a higher estimated prevalence of QTc prolongation. This phenomenon is further supported by our Bland-Altman analysis, which revealed a substantial mean difference of approximately 42 ms, and the Cohen’s kappa coefficient (κ=0.334), indicating only a fair agreement between the two formulas. Despite the lower prevalence obtained with Fridericia’s formula, QTc prolongation remained a frequent finding.
Metabolic acidosis is a key diagnostic feature of DKA. The associated reduction in serum bicarbonate may contribute to QTc prolongation through a potential mechanism involving pH-dependent inhibition of the human ether-à-go-go-related gene (hERG) potassium channel. Inhibition of this channel, which mediates the cardiac rapid delayed rectifier current (IKr), delays ventricular repolarization and increases arrhythmogenic risk. 26 In addition, hypokalemia, which is common in DKA, may further contribute to QTc prolongation. Reduced extracellular potassium decreases the IKr current, thereby delaying ventricular repolarization and increasing ventricular arrhythmia risk.26–28
From a clinical perspective, our study highlights the importance of QTc monitoring in patients with DKA. Low serum bicarbonate levels, together with the risk of hypokalemia—particularly following insulin therapy, the mainstay of DKA treatment—may predispose patients to QTc prolongation. Therefore, careful QTc monitoring is especially warranted in patients with severe acidosis, marked hypokalemia, or those receiving QTc-prolonging medications, as well as individuals with pre-existing cardiac conditions associated with QTc prolongation.
For clinical outcome, in hospital settings with limited monitoring of metabolic and ECG parameters, QTc prolongation may increase the risk of adverse outcomes, such as longer hospital stay or all-cause mortality, particularly in patients at high or very high-risk of QTc prolongation.29,30 In our cohort, however, QTc prolongation was not associated with these outcomes. This may be attributable to the rapid and dynamic improvement of DKA with appropriate management, including fluid resuscitation, insulin infusion, and close monitoring with timely potassium replacement, which may mitigate the potential adverse effects of QTc prolongation.
In addition to older age, which was consistently associated with increased LOS and mortality, a lower anion gap was associated with longer LOS. The mechanism underlying this association remains uncertain. It is possible that a lower anion gap reflects concurrent clinical conditions that contribute to prolonged hospitalization. Therefore, this finding should be interpreted cautiously, as LOS may be influenced by multiple factors beyond DKA severity and anion gap, including underlying comorbidities, precipitating illnesses, and inpatient complications. Additionally, a broader QRS complex was associated with increased LOS, possibly due to electrolyte imbalances, concomitant coronary artery disease, or other conduction abnormalities. 31
Compared with previous study, 11 the prevalence of QTc prolongation in our cohort, calculated using the Bazett’s formula, was approximately 60%, consistent with prior reports. 11 Similar to earlier findings, QTc prolongation was associated with lower serum potassium, highlighting the critical role of electrolyte disturbances in cardiac repolarization during DKA. 11 Other earlier studies in adult populations showed a similar trend, where QTc prolongation was highly prevalent and frequently associated with hypokalemia or hypocalcemia. These ECG changes were reversible, disappearing completely after the resolution of DKA in most cases.10,32,33 Our study also showed a trend toward association with lower serum bicarbonate, which reached statistical significance in this larger cohort, emphasizing the impact of metabolic acidosis on ventricular repolarization.
The impact of metabolic acidosis on ventricular repolarization is more evident in pediatric cohorts, where type 1 diabetes is the primary focus. Existing literature in these populations reports a QTc prolongation prevalence between 17% and 50%, with a significant correlation between DKA severity—including lower serum bicarbonate levels—and QTc duration.12–15,34 Although DKA is more prominent in children, our study focused on an adult population, with only 0.8% (3 of 374) of patients aged under 18. Our findings demonstrate that adults with DKA—the majority of whom have type 2 diabetes—similarly exhibit a high prevalence of QTc prolongation. This indicates that these repolarization abnormalities are a consistent feature of DKA across different age groups and diabetes types.
The strengths of this study include its larger sample size compared to previous research, 11 which provides greater statistical power and more robust insights into ECG parameters in adults with DKA. Additionally, our analysis was comprehensive, integrating ECG findings, laboratory data, and clinical outcomes. However, several limitations should be acknowledged. This study was a single-center retrospective study. The single-center setting may limit the generalizability of our findings to other healthcare settings, while the retrospective design, relying on existing medical records, may have introduced incomplete or inaccurate data and limited control over potential confounding variables. Residual confounding from unmeasured factors, such as unmeasured concomitant medications and the severity of comorbid illnesses, may also have influenced the study results. The multiple statistical comparisons performed in this study may have increased the risk of type I error. Regarding clinical outcomes, the relatively low number of mortality events may have limited the statistical power of the study to detect an association between QTc prolongation and mortality and increased the risk of overfitting in the multivariable mortality model. The absence of life-threatening arrhythmias in this cohort also limited our ability to evaluate the clinical impact of QTc prolongation on arrhythmic outcomes. Additionally, excluding patients without available ECG recordings (approximately 10% of the initially screened patients) may have introduced selection bias. These patients may have had different clinical characteristics, including potentially milder disease severity, which could have influenced the observed associations and study findings. Moreover, the absence of follow-up ECG after DKA resolution precluded assessment of the reversibility of QTc prolongation and its temporal relationships with metabolic correction. Future prospective studies with ECG monitoring are warranted to validate these findings and further clarify the clinical implications of QTc changes in DKA.
5. Conclusion
QTc prolongation is a common ECG abnormality in patients with DKA, particularly when calculated using the Bazett’s formula. It is independently associated with lower serum bicarbonate and lower serum potassium but was not associated with LOS or all-cause mortality in this study. Nevertheless, assessment of QTc prolongation during the initial evaluation of DKA may be considered, particularly in patients with severe acidosis and hypokalemia. Although the clinical impact of QTc prolongation remains uncertain, timely correction of metabolic derangements and adherence to standard DKA management protocols may help normalize QTc intervals. Further studies are needed to determine whether QTc prolongation is associated with clinically significant arrhythmic outcomes in patients with DKA.
Supplemental material
Supplemental material - Prevalence of electrocardiographic abnormalities and predictors of QTc prolongation in patients with diabetic ketoacidosis: A retrospective cohort study
Supplemental material for Prevalence of electrocardiographic abnormalities and predictors of QTc prolongation in patients with diabetic ketoacidosis: A retrospective cohort study by Winpob Kovichsakul, Varinsawat Prakongwong, Kitti Thammakosol, Chutintorn Sriphrapradang in Sage Open Medicine
Footnotes
Acknowledgments
We thank Sukanya Siriyotha from the Department of Clinical Epidemiology and Biostatistics for her valuable suggestions regarding the statistical analysis.
Ethical considerations
This study was approved by the Human Research Ethics Committee of the Faculty of Medicine Ramathibodi Hospital, Mahidol University (ethical approval number MURA2024/279).
Consent to participate
The requirement for written informed consent was waived due to the retrospective nature of the study.
Author contributions
W.K.: Conceptualization, Methodology, Investigation, Formal Analysis, Writing – Original Draft. V.P.: Conceptualization, Methodology, Investigation, Writing – Review & Editing. K.T.: Conceptualization, Investigation, Formal Analysis, Writing – Original Draft. C.S.: Conceptualization, Methodology, Investigation, Formal Analysis, Writing – Review & Editing, Supervision. All authors reviewed and approved the final manuscript. W.K. and C.S. are guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated and analyzed during this study are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.