
Abstract
Background
Viral non-suppression is still a major obstacle to putting an end to the epidemic, although Antiretroviral Therapy (ART) has made HIV a chronic illness that can be managed. Ethiopia has made strides, but there are still regional differences and particular structural obstacles that rural populations must overcome. The purpose of this study was to determine the factors that contribute to adult HIV-positive patients in public health facilities in Ambo town, Ethiopia, not having their viral loads suppressed.
Methods
A facility-based unmatched case-control study was carried out from March to May 2023. There were 376 participants in all (131 cases and 245 controls). Trained data collectors conducted secondary reviews of patient charts and electronic records in addition to structured interviews. Data were entered into EpiData version 3.1, then exported to SPSS version 26 for additional statistical analysis. Both bivariate and multivariable logistic regression analyses were performed. In the multiple logistic regression analysis, a p-value of less than 0.05 paired with a 95% confidence interval was utilized to determine statistical significance.
Results
According to the multivariable logistic regression analysis, marital status (AOR = 0.232, 95% CI: 0.065–0.830), complexity of the treatment regimen (AOR = 7.333, 95% CI: 3.357–16.017), treatment interruption (AOR = 2.298, 95% CI: 1.146–4.609), follow-up schedule (AOR = 3.721, 95% CI: 2.033–6.812), and adherence (AOR = 16.568, 95% CI: 5.587–49.129) were found to be significantly associated with the viral non-suppression.
Conclusion
Viral non-suppression in Ambo is primarily associated with behavioral and treatment-related factors, including poor adherence, high pill burden, and irregular follow-ups. One protective factor observed to have an inverse association is social support, particularly through marriage. A single-tablet regimen and improved adherence support systems, especially for a single group category patients, to meet the 95-95-95 targets.
Introduction
Since the advent of antiretroviral therapy (ART), HIV has transitioned from a fatal illness into a manageable chronic condition. To eliminate this significant threat to public health, the Joint United Nations Programme on HIV/AIDS (UNAIDS) established the 95-95-95 targets. These targets mandate that by 2030, 95% of people living with HIV (PLHIV) should know their status, 95% of those diagnosed should receive sustained treatment, and 95% of those on treatment should achieve viral suppression. 1
Clinically, viral non-suppression is defined as two consecutive viral load measurements ≥ 1,000 copies/mL taken at least six months apart, with enhanced adherence support in between. 2 Achieving virologic suppression is critical to diagnosing treatment failure early and guiding subsequent therapeutic decision-making. 3 While the majority of patients on treatment achieve an undetectable viral load within six months, some may require more time. 4
According to a World Health Organization (WHO) report, 27% of all HIV-positive individuals and 6% of those actively on treatment failed to achieve viral suppression in 2024, demonstrating that viral non-suppression remains a primary barrier to ending the epidemic. 5 Although suppression rates in Eastern and Southern Africa are closer to the 95% target than those in Western and Central Africa, Africa remains the most severely affected region, with viral non-suppression rates ranging from 15% to 20%. 6
In Ethiopia, national data from the Ethiopian Public Health Institute indicated that by early 2024, 8.8% of individuals on treatment nationwide were virally unsuppressed, though significant regional disparities exist—ranging from 15.1% in the Amhara region to 20.3% in Jimma.7,8
Factors contributing to viral load non-suppression include clinical and biological variables (such as drug resistance, advanced baseline disease severity like WHO stage 3 or 4, low baseline CD4 counts, and regimen type)7,9,10; behavioral and psychosocial factors (such as suboptimal adherence, mental health challenges, and substance use)6,9; and structural, socioeconomic, and healthcare access barriers.10,11
To achieve the UNAIDS targets by 2030, the Ethiopian Ministry of Health and the Federal HIV/AIDS Prevention and Control Office have implemented several targeted strategies. These include Differentiated Service Delivery (DSD) models—such as 6-month Multi-Month Dispensing (6-MMD) and Community ART Refill Groups (CAGs) for rural patients—point-of-care (POC) viral load testing via GeneXpert machine, home-based adherence support from Health Extension Professionals, and localized stigma reduction initiatives. 12
Despite these interventions, the burden of non-suppression remains disproportionately higher among rural communities due to structural constraints, including low health literacy and prolonged travel times to the healthcare facilities. 13 While previous research has well established general clinical predictors such as WHO stage and baseline CD4 count, a significant knowledge gap persists regarding the influence of rural-specific DSD models, like CAGs, on long-term virological stability. If left unaddressed, these gaps risk undermining Ethiopia’s goal of eradicating the AIDS epidemic by 2030 by driving up healthcare expenditures via second-line treatment switches, fueling the transmission of drug-resistant viral strains, and perpetuating localized transmission in underserved rural areas. Therefore, this study aimed to identify the factors associated with viral load non-suppression among adult HIV patients attending public health facilities in Ambo Town, Ethiopia.
Methods and materials
Study design and setting
A facility-based, unmatched case-control study was conducted from March to May 2023 across public health facilities in Ambo Town, located in the West Shewa Zone of the Oromia Region. Ambo, the capital of West Shewa, is located 114 kilometers west of Ethiopia’s capital, Addis Ababa. Based on the 2022 population projections, the town’s total population was estimated to be 97,317. 14 There were four public health facilities in the town: Ambo University Referral Hospital, Ambo General Hospital, Ambo Health Center, and Awaro Health Center. According to facility-based data from the Data for Accountability, Transparency, and Impact Monitoring (DATIM) system in December 2022, approximately 10,619 people living with HIV within the catchment area were actively receiving antiretroviral therapy (ART) across these facilities (facility-based DATIM data, December 2022).
Study participants, sample size, and sampling procedures
The source population consisted of all adult HIV-positive individuals actively accessing ART services at public health facilities in Ambo Town between March 2023 and May 2023. The cases were adult HIV-positive patients whose plasma viral load was ≥ 1,000 copies/mL after at least 6 months of continuous ART, and the controls were adult HIV-positive patients whose plasma viral load was < 1,000 copies/mL after at least 6 months of continuous ART. All adult HIV-positive patients on ART for ≥ 6 months who actively attended care during the study period were eligible for inclusion. Conversely, patients who had transferred out, died, or were lost to follow-up at the time of data collection were excluded due to the absence of active viral load data. The sample size was calculated using Epi Info 7 Stat Calc for an unmatched case-control design. Based on the following statistical assumptions: a 5% level of significance, 80% statistical power, a 1:2 case-to-control ratio, an expected odds ratio of 1.9 for history of opportunistic infection, and 53% exposure rate among controls 15 the required sample size was determined to be 396 participants (132 cases and 264 controls). Ambo General Hospital and Ambo Health Center were selected using a simple random sampling technique. Systematic sampling was then employed to select the individual study units. Patient data preceding two years (March 2021 to February 2023) were thoroughly reviewed.
Study variables
The outcome variable for this study was viral load status, categorized dichotomously as either suppressed or non-suppressed. The independent variables comprised five main categories: socio-demographic characteristics, treatment-related factors, health service-related factors, clinical and health status characteristics, and patient behavioral factors.
Operational definitions
Viral load non-suppression
A plasma viral load ≥ 1,000 copies/mL, as determined by two consecutive viral load assays taken at least six months after ART initiation, with adherence support in between. 2
Adherence
Participants were asked about the number of missed doses in the 30 days and measured by the ART clinician during a patient’s routine follow-up appointments and labelled as good if it is ≥ 95% (<2 doses of 30 doses missed), it is fair if it is between 85% - 94% (2-4 doses of 30 doses missed), and it is poor if it is < 85% ((> 4 doses of 30 doses missed) as documented by ART provider. 16
Social support
Defined as the patient’s self-reported access to emotional support, informational support, instrumental (tangible support), and appraisal support from family, friends, or treatment supporters when needed.
17
It consists of It was operationally dichotomized as:
Data collection methods, tools, and procedures
Data were gathered using a pretested, structured interviewer-administered questionnaire adapted from relevant literature.18,19 To ensure linguistic consistency and validity, the questionnaire was originally developed in English, translated into the local language (Afan Oromo), and subsequently back-translated into English by an independent language specialist. One supervisor and two data collectors—both Bachelor of Science (BSc) nurses with extensive clinical experience in ART services—were recruited for the data collection process. The team underwent a one-day training session focusing on the objectives of the study and the mechanics of the data-gathering tool. Two weeks before the main data collection period, the questionnaire was pretested on 5% of the total sample size at Ginchi Health Center to evaluate clarity and formatting. Insights from the pretest were used to refine and reformat the final tool. Primary data were obtained through face-to-face interviews with the sampled participants. This was robustly supplemented by secondary data extracted from patient charts, electronic medical records, and the facility ART registers.
Data processing and analysis
Data were entered into EpiData version 3.1 and subsequently exported to SPSS version 26 for statistical analysis. Descriptive statistics, including frequencies and percentages, were used to summarize the study variables. Bivariate logistic regression analysis was performed to evaluate the crude associations between the independent variables and the outcome; variables with a p-value < 0.25 were selected as candidates for the final model. A multivariable logistic regression model was then constructed to control for confounding and identify independent predictors of viral load non-suppression. Adjusted odds ratios (AOR) with corresponding 95% confidence intervals (CI) and a p-value ≤ 0.05 were utilized to determine the strength and statistical significance of the associations. Multicollinearity among the independent variables—specifically medication adherence, treatment interruption, and unscheduled follow-up visits—was assessed using the Variance Inflation Factor (VIF). No significant collinearity was detected, as the VIF values were 1.20 for adherence level, 1.10 for treatment interruption, and 1.12 for unscheduled follow-ups, all of which fall well below the standard conservative threshold of 10. Finally, the analyzed data were presented using tables, figures, frequencies, and descriptive text.
Ethical consideration
This study was conducted per the Declaration of Helsinki. Ethical clearance was obtained from Ambo University College of Medicine and Health Sciences ethical review board. A letter of permission was obtained from West Shewa Zone Health Office. Written informed consent was obtained from each study participant and the respondent’s confidentiality was maintained. For participants who had no formal education or unable to read and write, informed consent was obtained using a structured verbal and witnessed protocol. First, the information sheet and consent form were read aloud verbatim and explained in the participant’s local language (Afan Oromo) by a trained data collector. The explanation covered the study’s purpose, procedures, risks, benefits, and the voluntary nature of participation. To ensure comprehension, a “teach-back” method was utilized. Once understanding was confirmed, an impartial literate witness (who was not a member of research team) verbally verified that the information was accurately communicated and that the participant consented freely. Documentation of consent was finalized by the participant applying their right/left thumbprint on the consent form, which was then signed and dated by both impartial witness and data collector.
Results
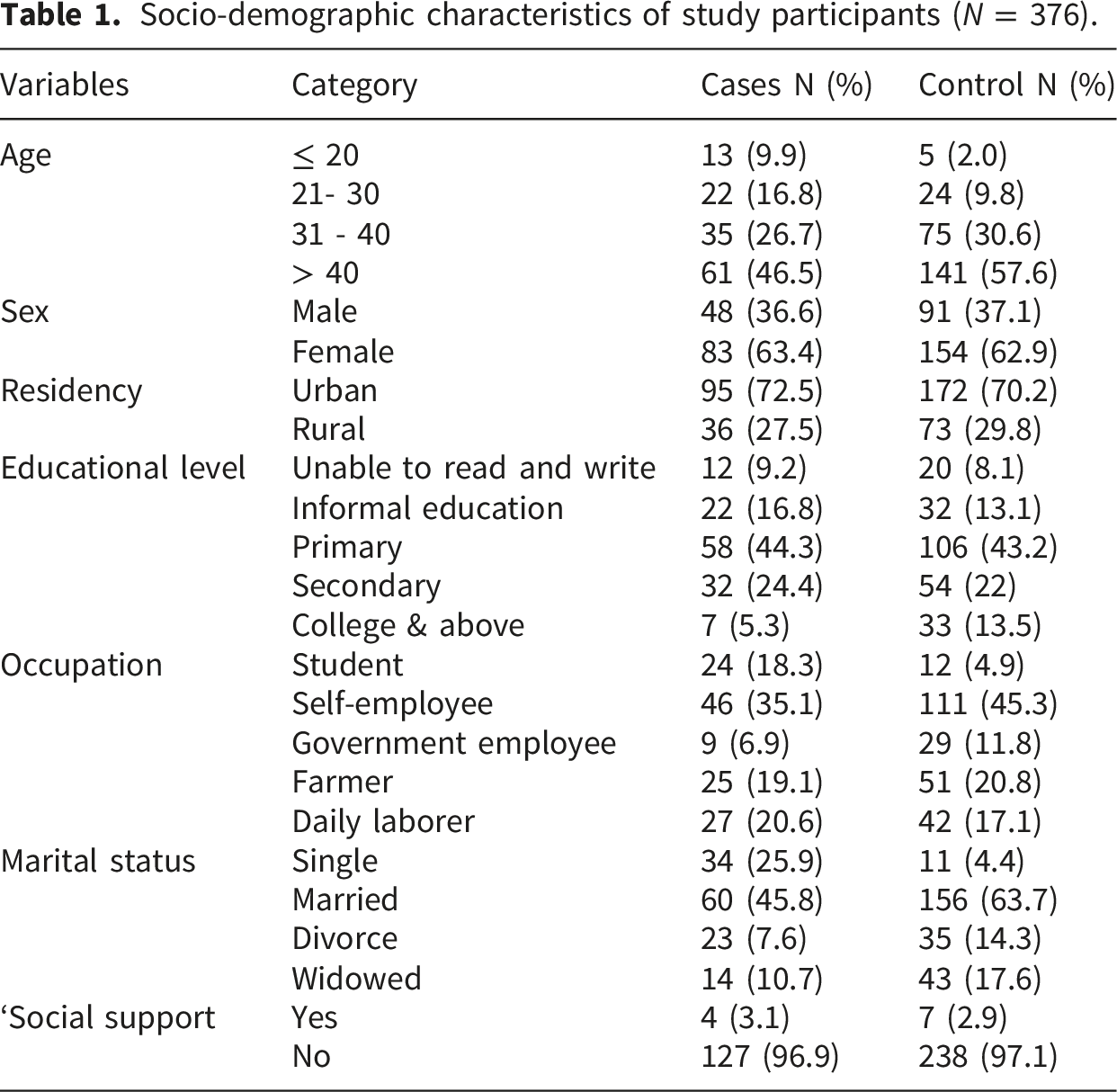
Socio-demographic characteristics
A total of 376 respondents (131 cases and 245 controls) participated, resulting in a response rate of 95% (Figure 1). The mean age of study participants was 39.7 (SD ±10.0) years old. The majority of the study participants resided in urban areas (70%) and had no formal education (56%). Nearly two-thirds (63%) of the participants were female, and around 57% were married in their marital status (Table 1). Participant flow diagram. Socio-demographic characteristics of study participants (N = 376).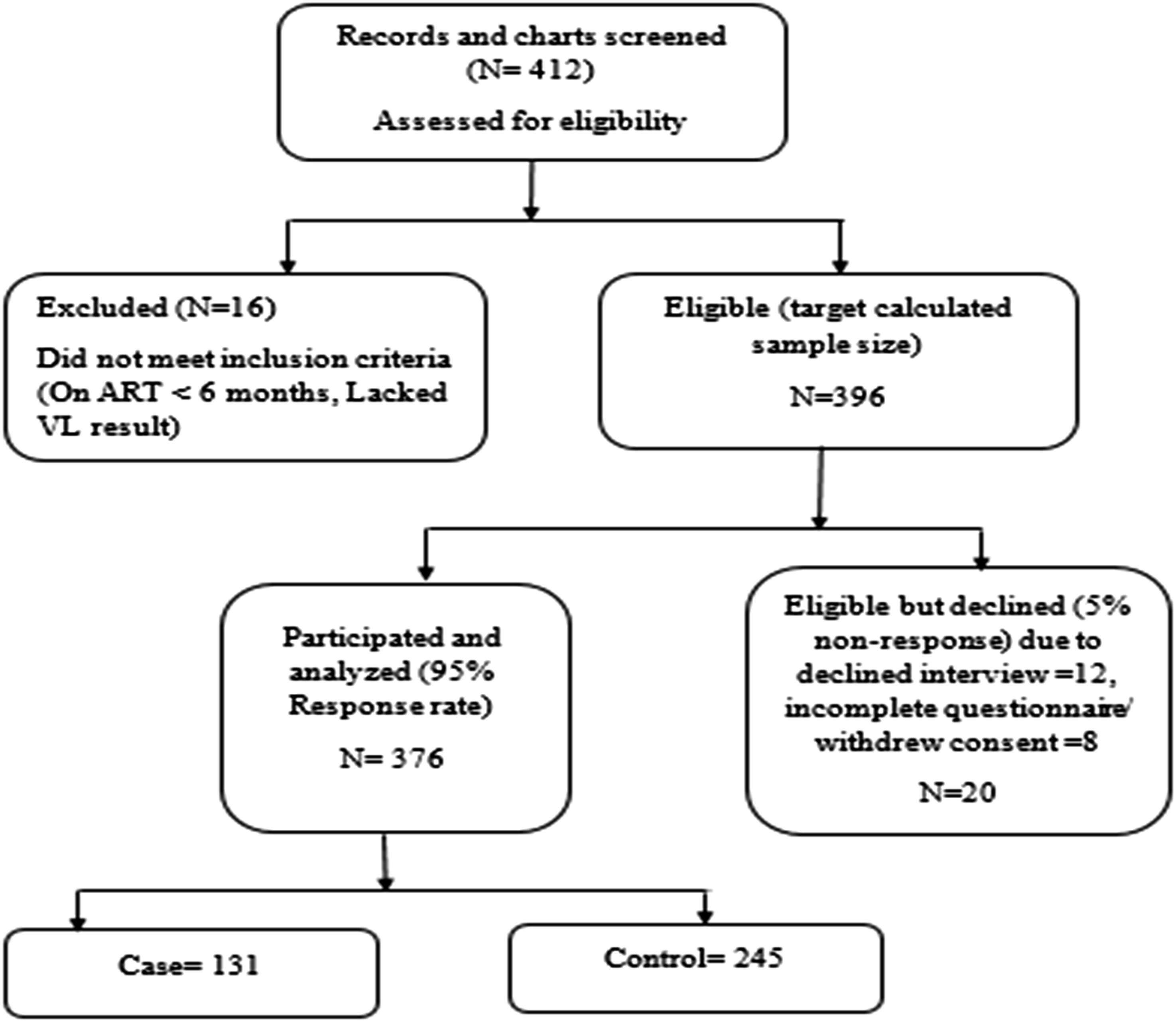
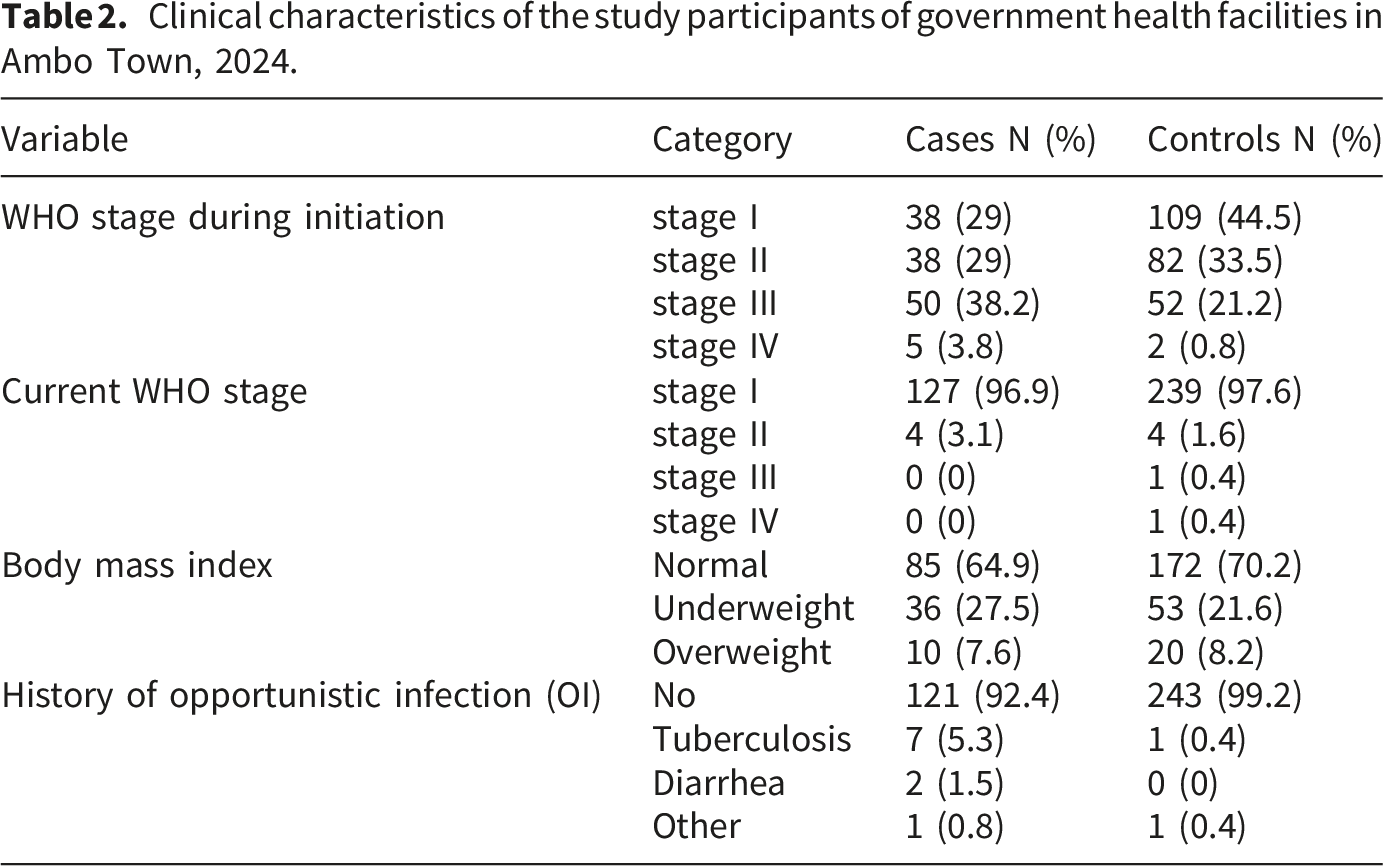
Clinical characteristics
Clinical characteristics of the study participants of government health facilities in Ambo Town, 2024.
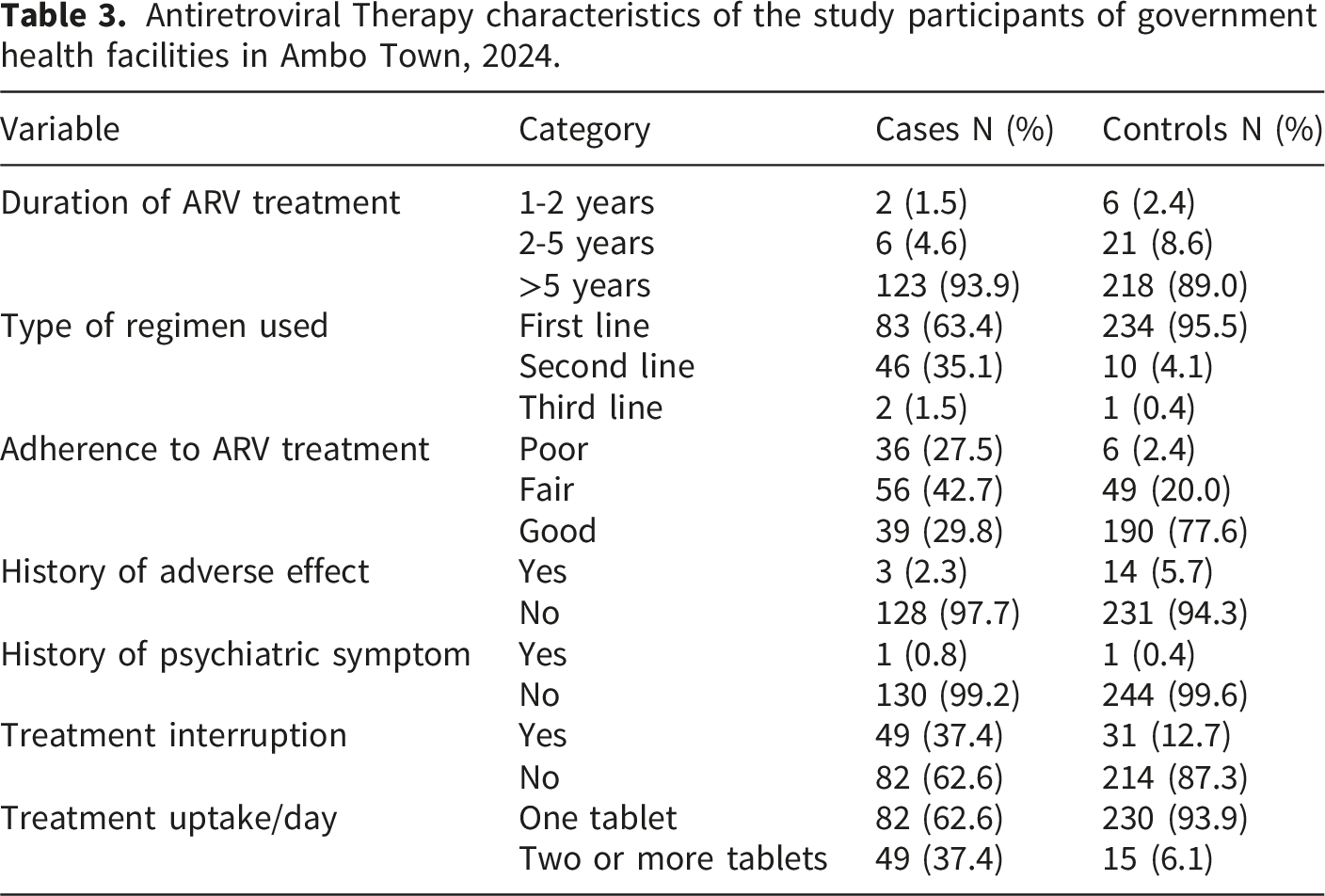
Antiretroviral therapy characteristics
Antiretroviral Therapy characteristics of the study participants of government health facilities in Ambo Town, 2024.
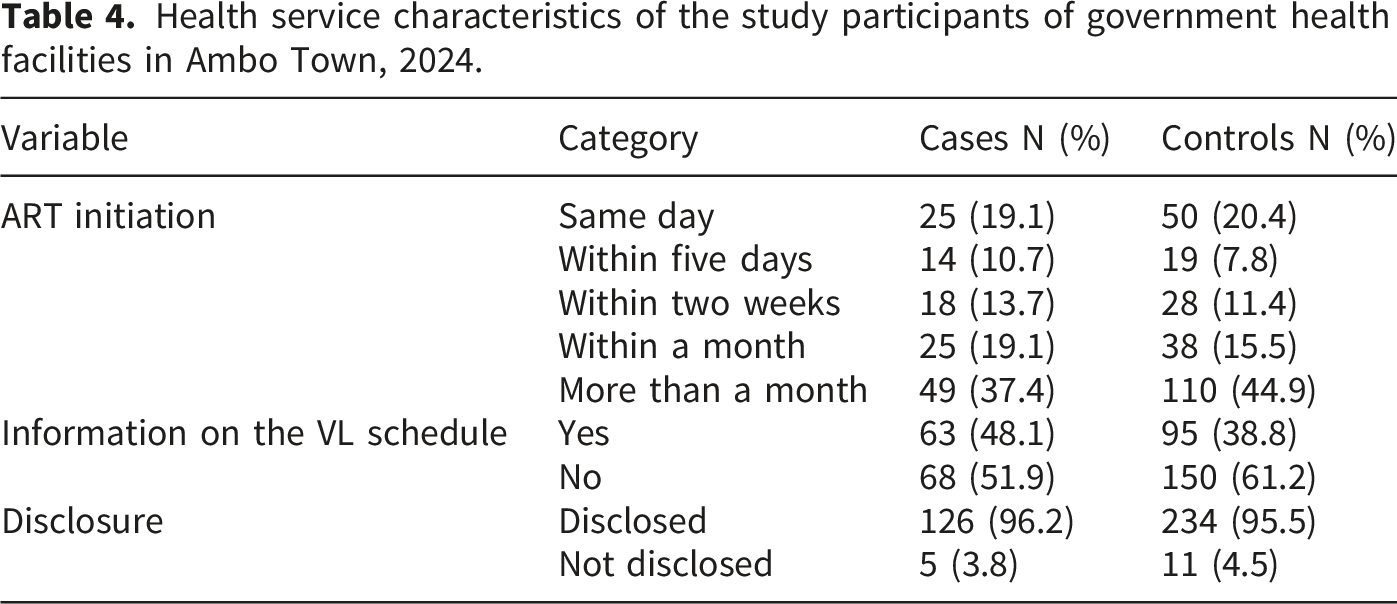
Health service characteristics
Health service characteristics of the study participants of government health facilities in Ambo Town, 2024.
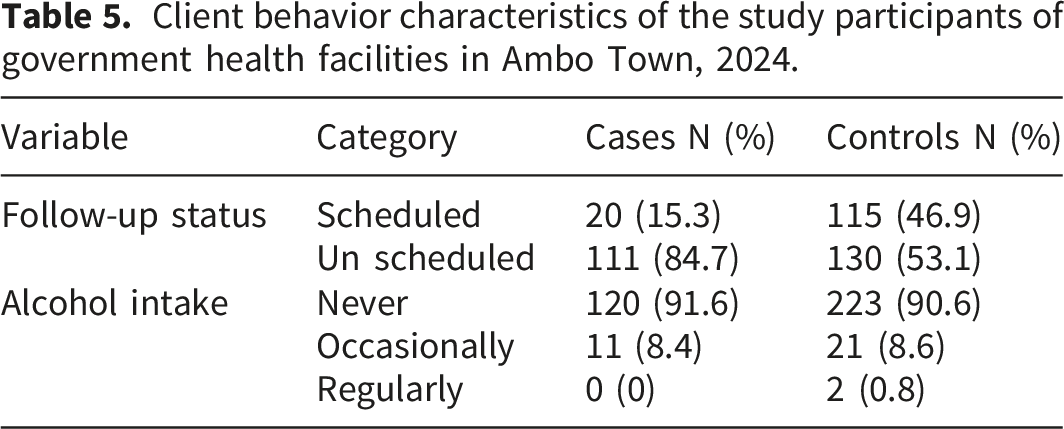
Client behavior characteristics
Client behavior characteristics of the study participants of government health facilities in Ambo Town, 2024.
Determinants of HIV viral non-suppression
Multivariable Logistic Regression Analysis Showing Association of Variables with viral un-suppression among the study participants of government health facilities in Ambo Town, 2024.
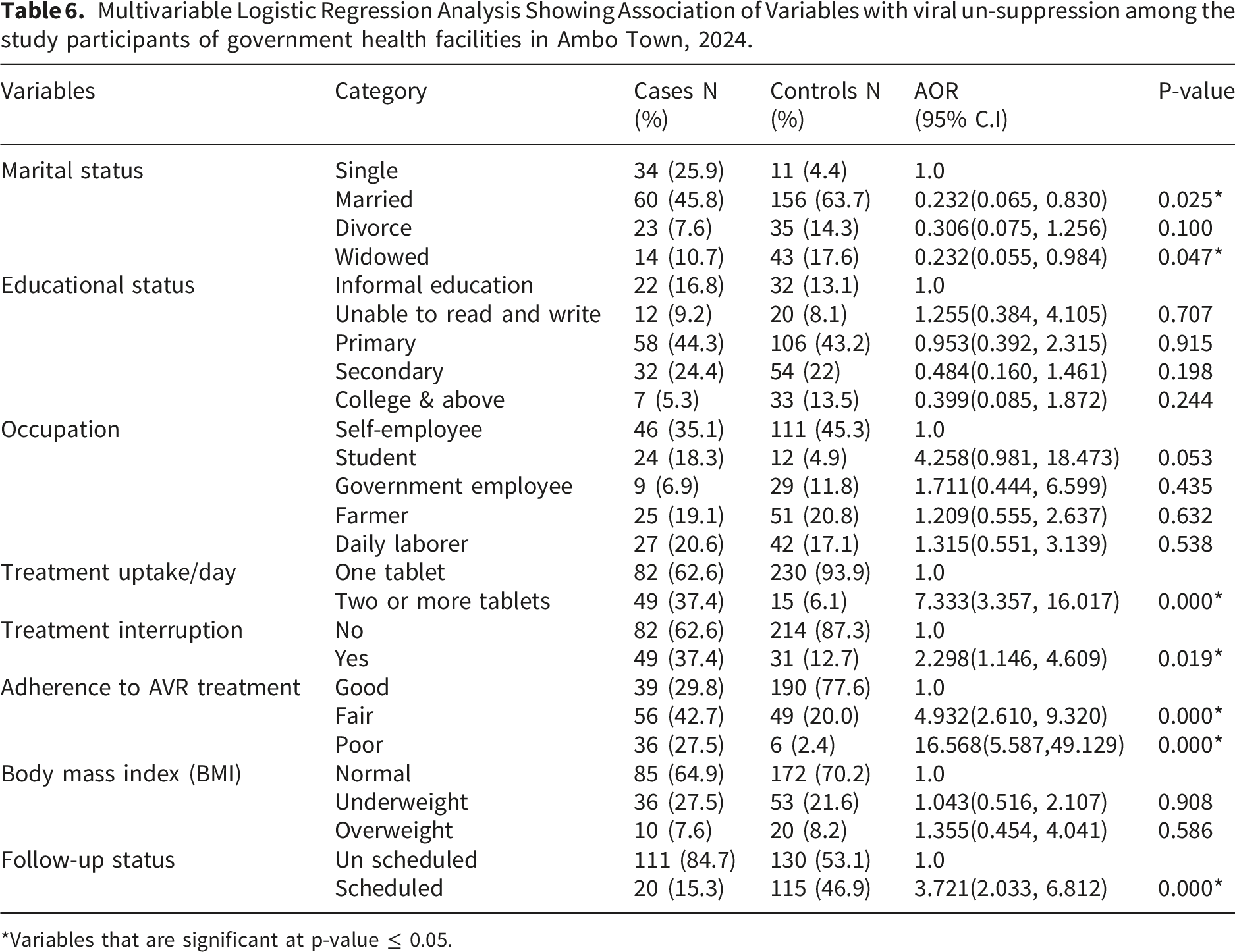
*Variables that are significant at p-value ≤ 0.05.
Discussion
According to this study, the primary factors consistently associated with viral load non-suppression among adult HIV patients in Ambo, Ethiopia, were poor adherence, a high pill burden, unplanned follow-up visits, treatment interruptions, and marital status.
Viral load non-suppression exhibited a strong statistical association with marital status. Married patients were approximately 76.8% less likely to experience viral non-suppression than their single peers (AOR = 0.232, 95% CI: 0.065–0.830). The results of this study are consistent with research from sub-Saharan Africa, which found that marital status is an important sociodemographic factor independently associated with viral suppression. 6 This statistical relationship may reflect the immediate social support network available to married individuals, who frequently benefit from treatment supporters within the household—such as partners who offer reminders, financial support, and emotional encouragement—which correlates with better adherence behavior. Conversely, studies from Ghana and Addis Ababa found no significant clinical advantage to being married.20,21 In highly urbanized settings, dispersed support structures—such as religious communities, non-governmental organizations, or peer networks— may diminish the relative impact of marital partners. Being widowed was also highly statistically significant and protective against viral non-suppression when compared directly to being single (AOR = 0.232, 95%CI: 0.055-0.984, P=0.047). Widowed individuals may have built long-standing support systems from adult children or community-based mutual aid groups like Iddir that single individuals lack. 22 Furthermore, widowed patients may possess a heightened perception of clinical risk and disease severity, motivating strict, long-term adherence to antiretroviral regimes to maintain health for surviving dependents.
The complexity of the treatment plan was a strong predictor of viral non-suppression. Patients taking two or more tablets daily were 7.3 times more likely to experience viral non-suppression than patients on a single tablet regimen (AOR = 7.333, 95% CI: 3.357-16.017). This finding is highly consistent with data from public health facilities in Bahir Dar, where complex daily ART dosing regimens and a high pill burden were strongly associated with subsequent virological failure. 1 The day-to-day complexity caused by multi-drug regimens frequently leads to treatment fatigue. Maintaining multiple medications becomes a significant challenge in rural settings that lack digital reminders or well-organized pillboxes. 23
For effective viral management, regular drug administration and scheduled follow-ups are essential. Patients with unplanned follow-up visits had 3.7 times higher odds of viral non-suppression than those who kept their appointments (AOR = 3.721, 95% CI: 2.033, 6.812). Similarly, participants who reported treatment interruptions had 2.3 times higher odds of viral non-suppression than those who never interrupted their treatment (AOR = 2.298, 95% CI: 1.146, 4.609). In contrast to the findings of this study, a study from Uganda revealed that patients who missed their clinical follow-up dates under Multi-Month Dispensing but had a 6-month supply of medication maintained suppression at the same rate as those who attended clinics every two months. 24 Similarly, a retrospective study from Kenya revealed that patients who had a documented treatment interruption but re-engaged in care achieved suppression rates similar to those who never interrupted treatment. 25 This discrepancy could be because, under differentiated service delivery models, a patient may have enough medication at home to maintain suppression even if they miss a scheduled clinic visit. Furthermore, adherence to ART medication was one of the most critical determinants of viral non-suppression. Non-suppressed viral loads were 16.5 times more likely in patients with poor adherence than in those with good adherence (AOR = 16.568, 95% CI: 5.587, 49.129). The results of this study are supported by research conducted in Jimma, Northern Ethiopia, and Ghana.1,18,22 From a biological perspective, antiretroviral therapy requires a high and sustained plasma drug concentration to effectively inhibit HIV replication. When doses are missed, plasma drug levels drop below the therapeutic threshold, allowing the virus to resume active replication in peripheral blood.
Strengths and limitations
A key strength of this study was the utilization of a facility-based, unmatched case-control design, which is highly efficient for investigating the multidimensional factors associated with viral load non-suppression. Additionally, the data gathered through primary structured interviews were robustly triangulated with secondary clinical data extracted from patient medical charts and electronic medical records. However, several limitations must be acknowledged. First, because this study relied on a facility-based design where exposure variables and clinical outcomes were evaluated concurrently or retroactively from existing registers, a strict temporal sequence could not be established. Consequently, these findings demonstrate statistical associations rather than definitive causal relationships. Second, medication adherence was measured solely through patient self-reports of missed doses per month that may overestimate true adherence levels. Furthermore, this study did not assess acquired drug resistance or certain structural barriers, such as distance to healthcare facilities, transportation costs, and experienced stigmatization, which remain critical potential predictors of viral non-suppression. Finally, patients who were lost to follow-up were excluded from the analysis due to a lack of active viral load data. Their exclusion may underestimate the true strength of association for specific sociodemographic and structural barriers to care, as these individuals often face the most severe obstacles to maintaining long-term treatment.
Conclusion
This study demonstrates that the primary factors associated with viral load non-suppression within the public health facilities of Ambo town were suboptimal adherence to medication, a high pill burden, a history of treatment interruptions, and a failure to maintain scheduled clinical follow-up appointments. Conversely, being married or widowed provides protective benefits against viral non-suppression, likely due to stronger, immediate household or community-based social support networks. To address these challenges, it is highly recommended to optimize regimen complexity, enhance adherence counseling, proactively trace patients with unscheduled follow-ups, and strategically leverage existing social support structures.
Supplemental material
Supplemental material - Determinants of viral load non-suppression among adult HIV positive patients on antiretroviral therapy in public health facilities in Ambo town, Ethiopia: A case-control study
Supplemental material for Determinants of viral load non-suppression among adult HIV positive patients on antiretroviral therapy in public health facilities in Ambo town, Ethiopia: A case-control study by Bedilu Hirpa Negeri, Gemechu Tulu Gemeda, Habtamu Oljira Desta and Belay Tafa Regassa in Sage Open Medicine.
Footnotes
Acknowledgements
The authors are grateful to Ambo University College of Medicine and Health Sciences for the approval of the ethical clearance, Ambo Town Health Office, Health Centers, and Hospitals for permitting us to collect the data. The authors also forward their gratitude to the study participants, data collectors, and a supervisor who participated in the study.
Ethical considerations
Ethical approval to conduct this study was obtained from the Ethical Review Board (ERB) of Ambo University college of Medicine and Health Sciences with protocol number AU/PGC/766/2023.
Consent to participate
All participants signed an informed consent form before study participation. They were given assurance about the data confidentiality.
Author contributions
All authors contributed significantly to the conception, study design, execution, data acquisition, analysis, and interpretation; participated in drafting the manuscript, critical review of the manuscript; agreed on the journal to which the article was submitted; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be available upon request from the corresponding author.
Significance for public health
The findings of this study offer critical, actionable insights into optimizing local health systems and improving patient outcomes with public health facilities in Ambo town.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.