
Abstract
A young woman in late pregnancy (31 weeks of gestation) was diagnosed with diffuse large B-cell lymphoma, presenting with bilateral cervical and upper thoracic paratracheal lymphadenopathy that led to superior vena cava syndrome. Her clinical presentation included progressively worsening dyspnea and an inability to lie flat. The initial treatment consisted of a combination of rituximab, cyclophosphamide, pirarubicin, vincristine, and dexamethasone and etoposide chemotherapy. After tumor shrinkage and symptomatic improvement, the pregnancy was terminated via cesarean section, yielding a healthy neonate. Although the patient was classified as high-intermediate risk, consolidated autologous hematopoietic stem cell transplantation was not performed due to her young age. Notably, NKG2C+ natural killer cells—potentially representing antitumor reactive lymphocytes—were detected during the initial treatment but eventually became undetectable. Overall, the patient achieved a satisfactory and notable treatment outcome.
Keywords
Introduction
Diffuse large B-cell lymphoma (DLBCL) is an aggressive malignancy that uncommonly manifests with superior vena cava (SVC) syndrome (SVCS) and airway compression in women during late pregnancy. 1 Symptoms such as dyspnea, orthopnea, and impaired venous return resulting from compression by enlarged lymph nodes can be life-threatening to both the mother and the fetus. Prompt and effective diagnosis and treatment are crucial to optimizing outcomes and reducing maternal and fetal mortality.
Case presentation
A young woman, who had given birth to two children, presented to the hospital at 31 weeks of her third pregnancy on June 28, 2022. Her medical history included right cervical lymphadenopathy persisting for more than 2 months. Initially asymptomatic, she did not seek medical attention at that time. Over the following weeks, she developed bilateral cervical lymph node enlargement, which progressed to shortness of breath 1 week prior to admission. On admission, the patient was in respiratory distress requiring upright positioning and was found to have hypertension (155/103 mmHg). The color Doppler ultrasound examination revealed multiple enlarged lymph nodes in the bilateral cervical regions, with the largest measuring ~1.9 × 1.4 cm on the left and 4.6 × 4.4 × 2.2 cm on the right (Figure 1). These lymph nodes caused compression of the SVC and airway, resulting in dyspnea, orthopnea, and inability to lie flat. Fine-needle aspiration cytology of a cervical lymph node confirmed the diagnosis of DLBCL, germinal center B-cell subtype. Immunohistochemistry (IHC) showed positivity for MYC, BCL2, and BCL6, but no specific expression ratios were determined. Fluorescence in situ hybridization revealed negative results for rearrangements of the MYC, BCL2, and BCL6 genes. Additionally, the patient was diagnosed with mild preeclampsia.
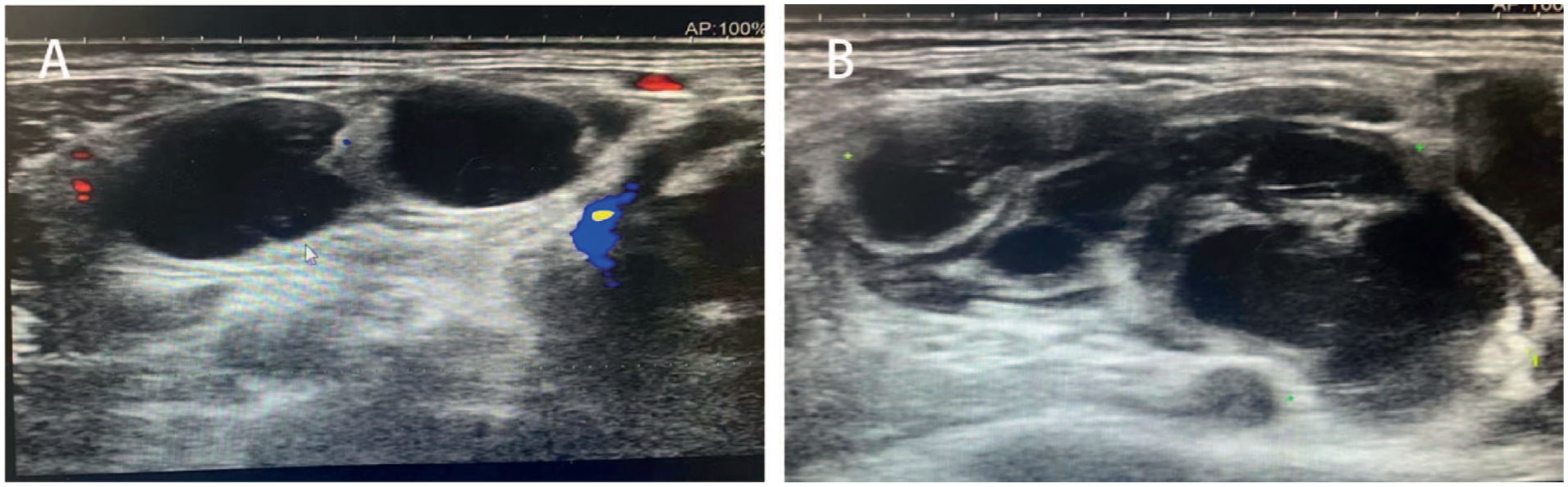
Color Doppler ultrasound images of cervical lymph nodes. (a) Lymph nodes in the left neck with a larger size of 1.9 × 1.4 cm. (b) Lymph nodes in the right neck with a larger size of 4.6 × 4.4 × 2.2 cm. This ultrasound examination took place on June 30, 2022.
Following biopsy at 31 + 4 weeks, dexamethasone 10 mg daily was initiated to reduce tumor burden. However, after 6 days, the patient’s dyspnea showed no improvement. On color Doppler ultrasound, the right pleural effusion had a maximum depth of 5.3 cm at the 8th to 10th intercostal spaces along the scapular line, indicating disease progression despite steroid therapy. Urgent antitumor intervention was therefore warranted. Fetal assessment, however, showed growth ~1–2 weeks behind gestational age, accompanied by signs of intrauterine hypoxia. The obstetrics team recommended expedited delivery via cesarean section, given the fetus’s likely viability outside the uterus. Nevertheless, the presence of significant SVCS and airway obstruction posed substantial risks for anesthesia, whether epidural or general, as emphasized by the anesthesiology team. A multidisciplinary discussion was held to review the risks and benefits of initiating R-CHOP (rituximab 500mg d0, cyclophosphamide 1.2g d1, pirarubicin 80mg d1, vincristine 2mg d1, and dexamethasone 10mg Qd) chemotherapy for both the patient and the 32-week fetus. The patient was presented with the option of either terminating the pregnancy or proceeding with DLBCL treatment. Ultimately, she elected to continue the pregnancy and pursue R-CHOP chemotherapy, considering its relative safety for the fetus.
R-CHOP chemotherapy was initiated at 32 + 3 weeks of gestation (July 8, 2022). Three days later, the patient developed a fever. Given the presence of moist rales in the right lung, exudative shadows on chest X-ray, and a markedly elevated hypersensitive C-reactive protein level of 162.32 mg/L, the fever was attributed to pneumonia. The patient’s breathing difficulty also worsened. Color Doppler ultrasound also indicated no reduction in the size of the cervical lymph nodes following the initial cycle of R-CHOP. Given the patient’s poor or nonresponse to the initial 5 days of R-CHOP therapy, etoposide (150 mg/day for 3 days) was incorporated into the regimen beginning at 33 + 1 weeks, resulting in the R-CHOEP regimen, with the goal of achieving better disease control and improved efficacy. Considering that the patient had lymphoma and was receiving chemotherapy and immunotherapy, which resulted in an immunocompromised state susceptible to severe concurrent infections, meropenem was administered as de-escalation anti-infective therapy. Within 1 week, her dyspnea gradually improved, and she was able to lie flat without distress. A magnetic resonance imaging scan performed at 34 weeks of gestation for preoperative assessment prior to cesarean section and for anesthesia evaluation demonstrated enlarged lymph nodes surrounding the esophagus, trachea, and vasculature (Figure 2). A lower segment cesarean section was successfully performed at 35 weeks of gestation. Bilateral tubal ligation was also performed following the patient’s provision of full informed consent.

MRI of the cervical and thoracic regions. Coronal (a) and transverse (b) images show diffusely enlarged lymph nodes in the bilateral neck, bilateral supraclavicular and infraclavicular fossa, mediastinum, pulmonary hila, chest walls, and axillae, with the largest node measuring 4.6 × 2.8 cm. This MRI was performed on July 21, 2022.
The mother recovered well and was discharged 72 h postpartum. She returned to the hospital as scheduled 3 days later to continue treatment. Prior to the second cycle, bone marrow aspiration and hydrothorax were collected for further analysis. No immunophenotypically abnormal B lymphocytes were identified by flow cytometry in either the bone marrow or hydrothorax samples, whereas an abnormal population of natural killer (NK) cells was observed in both. Bone marrow flow cytometry identified ~19.8% NK cells with the following immunophenotype: sCD3−, cCD3−, CD56+, CD2+, CD7dim, CD16+, CD4−, CD5−, CD8dim, CD94+, CD158b−, CD158e−, CD161−, NKG2A−, NKG2C+. Due to suspicion of high-risk DLBCL, including possible lung involvement and the possibility of double or triple expression, the treatment regimen was switched to R-hyper-CVAD (rituximab 500mg d0, cyclophosphamide 450mg Q12h d1-3, pirarubicin 75mg d4, vincristine 2mg d4 11, dexamethasone 40mg d1-4, d11-14). After the completion of the second chemotherapy cycle, the patient was evaluated at Sun Yat-sen University Cancer Center. Pathology consultation of lymph node specimens confirmed DLBCL, with IHC showing 30% positivity for MYC. The final diagnosis was DLBCL, stage Ⅱ, with an age-adjusted International Prognostic Index (aa-IPI) score of 2 and a National Comprehensive Cancer Network (NCCN)–IPI score of 2. Disease involvement included multiple lymph node regions: bilateral neck, supraclavicular fossa, subclavian fossa, axilla, mediastina, and chest wall. The posttreatment post-treatment positron emission tomography-computed tomography (PET-CT) imaging indicated complete remission after two cycles of chemotherapy. After completing two cycles of R-CHOEP and R-hyper-CVAD, the patient’s PET-CT scan yielded a Deauville score of 3, indicating complete remission.
Given her DLBCL was stage Ⅱ and did not meet the criteria for high-grade lymphoma, she continued to receive four cycles of R-CHOP chemotherapy supplemented with two additional doses of rituximab administered every 21 days (Table 1). After six cycles of therapy, PET-CT scan demonstrated a Deauville score of 2, reflecting a state of sustained complete remission. Additionally, flow cytometric analysis of the bone marrow at that time showed that the previously detected NK cells with abnormal immunophenotype had resolved. There was no strong evidence to suggest that autologous hematopoietic stem cell transplantation (ASCT) would provide significant benefit in the first-line treatment of her low-stage DLBCL, particularly in the absence of double/triple expression or rearrangement. Therefore, the recommended management consisted of regular follow-up and monitoring.
Treatment plan for the patient with DLBCL.

DLBCL: diffuse large B-cell lymphoma; R-CHOP: rituximab, cyclophosphamide, pirarubicin, vincristine, and dexamethasone.
The neonate received Apgar scores of 10 at both 1 and 5 min after birth. Birth weight was 2350 g and height was 46 cm. Within several hours of delivery, the newborn exhibited mild cyanosis, shallow respirations, frothing at the mouth, and mildly decreased muscle tone. He was diagnosed with neonatal respiratory distress syndrome and required continuous positive airway pressure ventilation for at least 24 h. Although T- and B-cell lymphocyte subsets were not analyzed, the total lymphocyte count was within normal range. No infectious complications were observed during the neonatal period.
As of September 2025, the patient remains in complete remission, having maintained this status for more than 2 years since diagnosis. Her son is in good health with age-appropriate physical and intellectual development.
Discussion
This young female developed SVCS and airway obstruction at 31 weeks of gestation due to progressively enlarging lymph nodes, concurrent with preeclampsia and fetal intrauterine hypoxia. Given the lack of response to dexamethasone monotherapy, should antitumor therapy or cesarean section have been prioritized in the management of her DLBCL?
When lymphoma is combined with SVCS caused by lymph node aggregation, under general anesthesia, severe hemodynamic impairment due to the compression of major blood vessels can led to significant risks. Positive-pressure ventilation increases intrathoracic pressure, leading to a rapid reduction in venous return, thereby exacerbating hemodynamic instability and potentially compromising the already narrowed airway in parturients. 2 Furthermore, inhalational induction may cause muscle relaxation, resulting in the loss of chest wall tension and impairment of active inspiratory effort, which can further precipitate airway collapse. 3 In general, regional anesthesia is preferred over general anesthesia in the obstetric population to avoid the adverse effects of positive-pressure ventilation and potentially difficult endotracheal intubation. Epidural anesthesia, administered via incremental dosing of local anesthetic, allows for compensatory hemodynamic mechanisms and minimizes abrupt hemodynamic changes.4,5 However, parturients with SVCS remain at risk of hemodynamic instability even under epidural anesthesia. While spinal block is technically simpler to perform and manage, it frequently causes hypotension due to preganglionic sympathetic blockade. 6 Additionally, abnormally elevated central venous pressure may lead to substantial venous blood loss, presenting a significant risk in this patient population. Although several reports describe successful cesarean deliveries under regional anesthesia in late-term pregnant patients with mediastinal masses, including some with SVCS without airway obstruction, 7 or cases where lymphoma-related anterior mediastinal masses responded well to steroids, 1 Thereby relieving severe obstruction prior to delivery, careful individualized risk assessment remains essential (Supplemental Material).
The “watch and wait” strategy is generally appropriate for indolent lymphomas with low tumor burden, whereas aggressive lymphomas such as DLBCL often require antepartum treatment. 8 According to a multicenter collaborative study, standard chemotherapy regimens administered during the second and third trimesters resulted in a low incidence of maternal and fetal complications. 9 Following multidisciplinary discussion, it was concluded that initiating chemotherapy to reduce lymph node masses and alleviate SVCS and airway obstruction would improve the safety of delivery for this patient. According to the NCCN guidelines version 2.2022 B-cell lymphomas, R-CHOP remains the first-line treatment for newly diagnosed DLBCL regardless of disease stage. For patients diagnosed with aggressive non-Hodgkin lymphoma during pregnancy, CHOP-based regimens, with the inclusion of rituximab for B-cell subtypes, are recommended as the first-choice treatment after the first trimester in most guideline recommendations.9,10
The addition of rituximab during pregnancy was reported to increase the risk of neonatal B-cell depletion, but B-cell counts typically normalize within 6 months. Existing evidence does not indicate an elevated incidence of significant neonatal infections or congenital anomalies linked to rituximab exposure. 11 Furthermore, no causal relationship has been established between rituximab use in the second or third trimester and preterm birth.12,13 Regarding anthracycline-based chemotherapy, Gziri et al. reported that children with in utero exposure exhibited reduced heart fractional shortening and mildly decreased left ventricular wall thickness; however, these values remained within normal limits according to tissue Doppler and strain measurements, and did not differ significantly from those of unexposed controls. 14 Another small cohort study found no evidence of acute maternal or fetal cardiac dysfunction following antenatal anthracycline exposure. 15 Additionally, Aviles and Neri observed normal cardiac morphology and function in 81 children who had been exposed to anthracycline-containing chemotherapy in utero, over a median follow-up period of 17.1 years. 16
The implementation of cyclophosphamide in early pregnancy has been associated with congenital malformations in live births. 17 However, its administration during the second and third trimesters has been shown to be safe. For instance, it is reported that among infants born to mothers who received four cycles of cyclophosphamide-containing chemotherapy during mid-to-late pregnancy, none exhibited congenital malformations. 18 Based on these limited but consistent data, the R-CHOP regimen appears to be an acceptable treatment option during the second and third trimesters. 19 It is generally recommended that delivery be scheduled no fewer than 2 weeks after the last chemotherapy session to allow for recovery of maternal and fetal blood counts and to ensure complete metabolism of chemotherapeutic agents by the fetus and placenta. 1 In this case, although our patient delivered 11 days after receiving etoposide chemotherapy, no neonatal cytopenia was observed.
Currently, there is no robust evidence to suggest that consolidative ASCT provides superior outcomes compared with R-CHOP alone in young patients with high-intermediate-risk DLBCL (defined as aa-IPI ⩾2 points). Results from the randomized intergroup trial SWOG 9704, 20 which included 165 high-intermediate-risk B-cell lymphoma patients, showed no significant difference in the 2-year progression-free survival (PFS) rate between the control group (who received three additional cycles of R-CHOP after five initial cycles of R-CHOP-21) and the transplantation group (who underwent one consolidation cycle followed by ASCT after the same induction; 66% vs 63%, p = 0.32). The 2-year overall survival (OS) rates were 75% and 70%, respectively (p = 0.48). Furthermore, two phase 3 trials indicated no statistically significant differences in 3-year PFS or 5-year OS between patients with aa-IPI scores of 2–3 treated with chemotherapy alone (R-CHOP or R-CHOEP) and those receiving chemotherapy followed by ASCT.21,22 Therefore, high-dose chemotherapy with ASCT as first-line consolidation may only be considered in selected high-risk cases. 23
In this case, a cluster of NK cells with an abnormal immunophenotype (CD56+, partially CD8+, CD16+, CD94+, NKG2A−, NKG2C+) was detected by flow cytometry in both the bone marrow and hydrothorax prior to the second cycle of chemotherapy. As is well established, NK cells are innate lymphocytes that primarily surveil the body for virally infected and malignant cells. Upon full activation by target cells, NK cells secrete cytokines and cytolytic molecules, thereby inducing apoptosis in the target cells. The NKG2C+ population represents a distinct subset of NK cells, predominantly expressed on resting NK cells that lack NKG2A, referred to as adaptive NK cells. 24 NKG2C+ NK cells contain high levels of effector molecules, exhibit an enhanced capacity for IFN-γ production, and demonstrate stronger antibody-dependent cellular cytotoxicity. 25 A previous study has reported that highly active NKG2C+ NK cells can mediate cytotoxicity against primary acute myeloid leukemia blasts through redirected targeting. 24 Furthermore, the expansion of adaptive NK cells has been associated with reduced relapse rates in hematological malignancies following hematopoietic cell transplantation. 26 Additionally, research has shown that NKG2C+ NK cells display increased cytotoxicity toward glioblastoma multiforme (GBM) cells compared with conventional NK cells, suggesting their potential therapeutic value in GBM treatment. 27 Therefore, it is reasonable to speculate that this population of immunophenotypically abnormal NK cells—NKG2C+ NK cells, may represent reactive cells targeting tumor cells in this patient with DLBCL. Notably, this cluster of cells disappeared after the patient achieved complete remission.
Conclusion
The R-CHOP chemotherapy regimen was found to be safe for both late-term pregnant women with DLBCL and their fetuses. Additionally, it helped avoid the potential risks associated with increased surgical anesthesia due to compression of the SVC and airway by enlarged lymph nodes. Furthermore, there is currently no strong evidence to suggest that ASCT provides superior outcomes compared with R-CHOP alone in ASCT. Finally, the NKG2C+ NK cells identified during the initial treatment in this patient may represent a population of antitumor reactive cells.
Footnotes
Acknowledgements
The authors gratefully acknowledge all members of our lymphoma multidisciplinary team for their expert clinical management of the patient.
Ethical considerations
Patient privacy has been safeguarded through the de-identification of personal data. In accordance with the Ethical Review Measures for Research on Human Life Sciences and Medicine (2023), formal ethics approval is not required for the publication of this case report.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report.
Author contributions
Guocai Wu conceived the study. Haiyan Liang and Tian Xia collected the clinical data. Haiyan Liang drafted the manuscript. Guocai Wu and Haiyan Liang revised and finalized the manuscript. All authors read and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Non-funded Science and Technology Research Projects of Zhanjiang, Grant Number: 2020B01196.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data of this study are available upon reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.