
Abstract
Galactocele is a rare clinical finding in males and is even more uncommon in the context of prolactin-secreting pituitary adenomas. Its occurrence raises important questions about the effects of hyperprolactinemia in men, especially when there is poor treatment adherence. We describe a 34-year-old man with type 2 diabetes who presented with erectile dysfunction, gynecomastia, and galactorrhea. Investigations confirmed hyperprolactinemia secondary to a pituitary macroadenoma. He was started on cabergoline, which improved his symptoms. However, after discontinuing therapy for several months, he developed a painful breast mass. Ultrasound and aspiration confirmed a galactocele—a finding rarely reported in adult males. The mass resolved after aspiration, and dopamine agonist therapy was resumed. This case highlights the importance of recognizing galactocele as a potential complication of untreated or poorly managed hyperprolactinemia in men. It underscores the need for sustained adherence to dopamine agonists and vigilance in evaluating male patients with gynecomastia and galactorrhea.
Key clinical message
Hyperprolactinemia should be considered in male patients with erectile dysfunction, gynecomastia, and galactorrhea, especially those with type 2 diabetes. This case emphasizes recognizing galactocele as a rare complication. Timely diagnosis and treatment with cabergoline can improve symptoms and prevent further complications, highlighting the hormone’s significant impact across genders.
Introduction
Prolactin-secreting pituitary adenomas (prolactinomas) are the most common type of secretory pituitary tumors. According to the Pituitary Society International Consensus Statement, their diagnosis and management require a comprehensive approach encompassing biochemical evaluation, pituitary imaging, and individualized medical therapy. 1 Hyperprolactinemia is a condition characterized by high levels of prolactin, which may be caused by various factors, including pituitary tumors, medications, and systemic diseases, or it could be idiopathic. Hyperprolactinemia could be associated with various clinical manifestations, including sexual dysfunction, gynecomastia, and galactorrhea. 1
In the presence of hyperprolactinemia, the mammary glands are stimulated to produce milk, even in the absence of pregnancy or lactation. The continuous secretion of milk leads to the accumulation of fluid within the breast ducts, forming a cystic mass, which is known as galactocele. Galactocele is a benign breast cyst containing milk fluid that commonly develop in lactating females. The relationship between hyperprolactinemia and galactocele formation is rooted in the actions of prolactin on the breast tissue, irrespective of gender. 2 In male patients with hyperprolactinemia, this process can result in the development of a galactocele despite the absence of the typical female hormonal environment. 3
The relationship between galactocele and prolactin overproduction, a growth factor for breast epithelium, is not well-defined, prompting the need for further investigation. 4
This relationship highlights the diverse effects of hyperprolactinemia on various body systems and the importance of recognizing galactocele as a possible complication in patients with elevated prolactin levels. Prompt diagnosis and appropriate management of hyperprolactinemia can help resolve symptoms and prevent further complications, including the development of galactocele. 5 However, it is essential to note that galactoceles have rarely been reported in males, especially those with hyperprolactinemia. Here, we present a case of male patient with prolactinoma, who was treated with dopamine agonist, with which he has not been compliant, which resulted in formation of a unilateral galactocele.
Case history/examination
A 34-year-old gentleman with type 2 diabetes mellitus was first evaluated in October 2021 when he presented with intermittent erectile dysfunction for the preceding 5–6 months, along with dry ejaculation and an inability to achieve an erection despite sexual arousal. He also reported an increase in the size of his breasts. On general examination, the patient was found to be morbidly obese with a body mass index greater than 40 and had sizable bilateral gynecomastia of stage V. Expressible galactorrhea was also observed. Genital examination revealed an adequately sized penis, but both testicles had a volume between 8 and 10 mL.
Initial laboratory tests, including complete blood count, renal function tests, and liver function tests, were unremarkable. A comprehensive evaluation of all pituitary hormone axes was performed. Given the patient’s comorbidities of type 2 diabetes mellitus and morbid obesity, co-secretion of Adrenocorticotropic Hormone (ACTH) and Cushing’s syndrome were clinically and biochemically evaluated and excluded. Endocrinology tests confirmed hyperprolactinemia and low testosterone, with otherwise normal pituitary function (Table 1).
Endocrinology tests showed hyperprolactinemia, low testosterone.
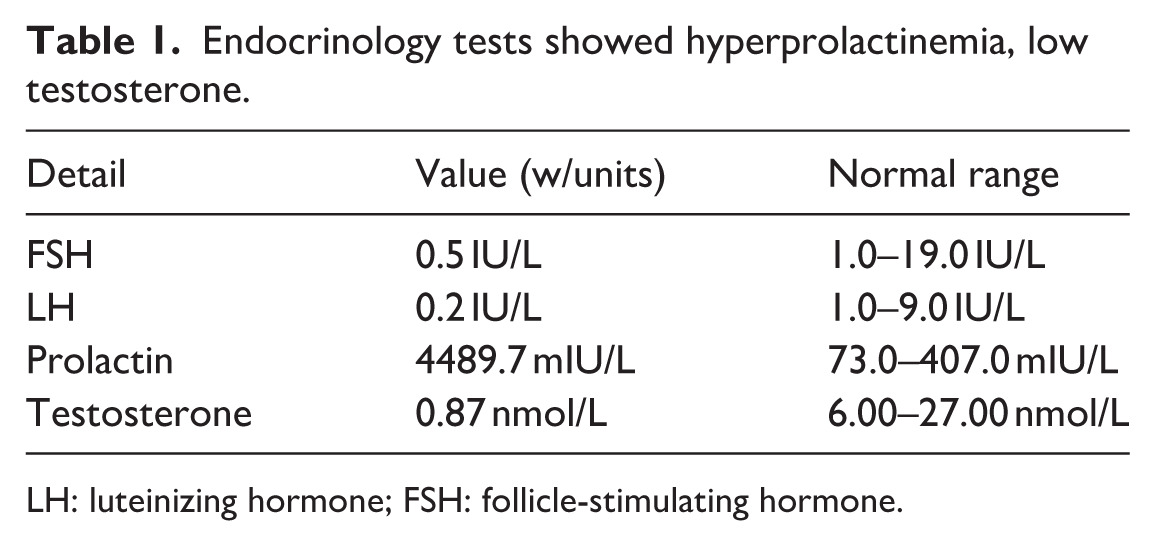
LH: luteinizing hormone; FSH: follicle-stimulating hormone.
Further investigation with an magnetic resonance imaging of the pituitary confirmed a pituitary macroadenoma measuring 1.4 cm, which led to the correct diagnosis (Figure 1).
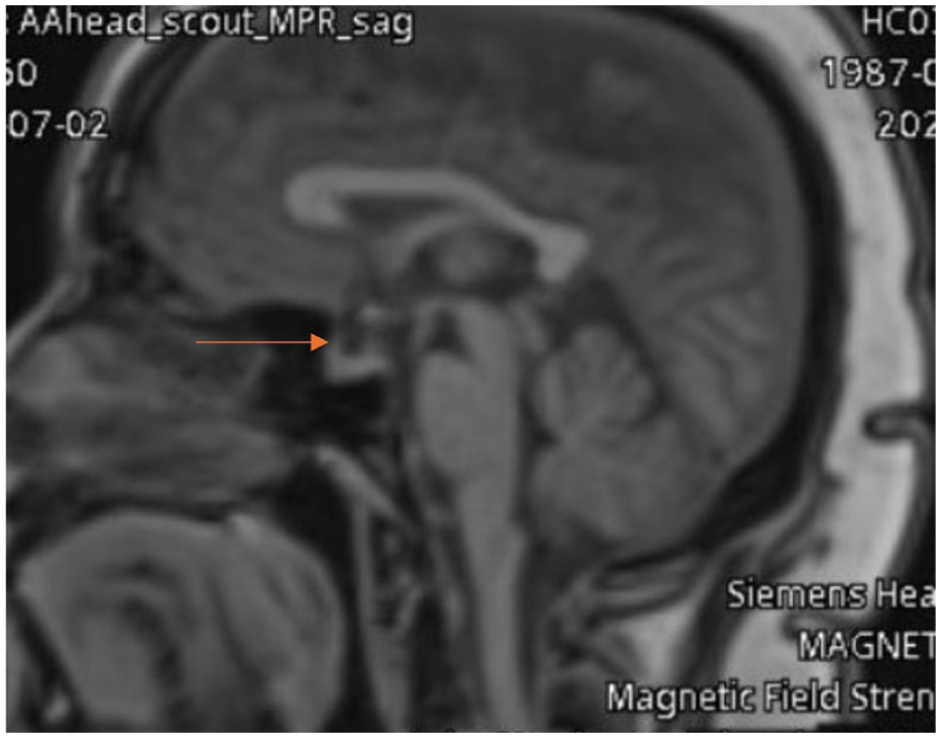
MRI of the pituitary gland: A well-defined and homogenously enhancing pituitary macroadenoma is visible on the right aspect, measuring 1.1 × 1.3 × 0.4 cm (brown arrows indicate the macroadenoma).
The patient was started on cabergoline, a long-acting dopamine D2 receptor agonist that effectively inhibits prolactin secretion and promotes tumor size reduction. The initial dose was 0.25 mg orally, once a week, to treat the hyperprolactinemia and shrink the pituitary macroadenoma.
Follow-up period
The patient reported improvement of his erectile dysfunction. He remained on dopamine agonists for over 18 months. He then went on leave to his home country for 6 months, where he ran out of the dopamine agonist, which he did not take for over 5 months. On return in January 2023, he complained of a new issue – a sizable swelling in his right breast associated with discomfort and pain.
On examination, bilateral gynecomastia was still present (Figure 2), but he had a 4–6 cm mass in his right breast, which exhibited skin edema and mild redness. There were no clinical signs of infection in the galactocele, and no lymph node enlargement was noted. An ultrasound scan of the breasts revealed a 5–6 cm mass in the right breast. He was referred to a breast surgeon, who decided to perform a fine-needle aspiration of the breast and scheduled the patient for a multidisciplinary tumor board meeting. The mass was successfully aspirated under ultrasound guidance, yielding milk fluid, which led to the disappearance of the mass. Based on these findings, a diagnosis of galactocele was confirmed (Figure 3).

Clinical presentation: (a) bilateral gynecomastia; (b) expressible galactorrhea.
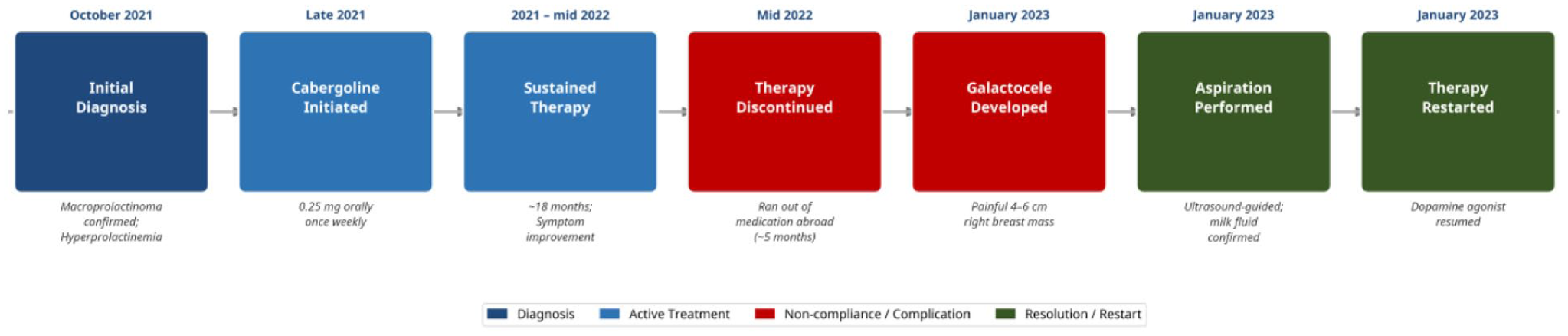
Clinical timeline.
This case highlights the need to consider hyperprolactinemia as a potential cause of erectile dysfunction and gynecomastia in male patients, particularly those with type 2 diabetes mellitus. It emphasizes identifying galactocele as a possible complication of hyperprolactinemia. Prompt diagnosis and appropriate treatment with cabergoline can lead to significant improvement in symptoms and successful resolution of associated complications, underscoring the importance of thorough evaluation in affected individuals.
Discussion
Hyperprolactinemia may be due to variety of causes, including prolactin-secreting pituitary adenomas (prolactinomas), other pituitary tumors or lesions, hypothalamic dysfunction, certain medications, chronic kidney disease, and hypothyroidism. It may present with diverse clinical manifestations, depending on the underlying cause and the extent of hormone elevation. 1
Hyperprolactinemia is known to have diverse effects on various organs and systems, and its association with gynecomastia is well documented. In this case report, the patient presented with symptoms of intermittent erectile dysfunction, dry ejaculation, and an inability to achieve an erection despite sexual arousal. These symptoms were consistent with the impact of hyperprolactinemia on male sexual function. 6
The elevated prolactin levels suppress the secretion of gonadotropin-releasing hormone from the hypothalamus, subsequently reducing the production of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) by the pituitary gland. The decrease in LH and FSH levels leads to decreased testosterone production, which can result in erectile dysfunction and reduced libido. 7
Hyperprolactinemia can lead to various complications, including sexual dysfunction and gynecomastia. In this case, the patient’s gynecomastia progressed to the formation of galactocele, a rare but possible consequence of sustained hyperprolactinemia. The galactocele resolved successfully with ultrasound-guided aspiration of the milk fluid. 1 We hypothesize that the patient’s lack of compliance with the dopamine agonist cabergoline for several months, in the context of persistent sizable gynecomastia, may be temporally associated with the formation of the galactocele in his right breast. The surge of sudden and sustained high prolactin may have contributed to the formation and retention of milk in the right breast, leading to the galactocele.
While the case report highlights the relationship between hyperprolactinemia and the development of galactocele in a male patient, it is essential to consider other possible causes of gynecomastia and galactocele in the differential diagnosis. Breast abscess, fibroadenomas, and other breast tumors can present with similar clinical findings, necessitating careful examination and diagnostic investigations to establish the correct diagnosis. 8
To date, cases of galactocele in the male breast reported in the medical literature are predominantly from the pediatric population, making its occurrence in an adult male exceptionally rare. 9
The development of a galactocele should be recognized as a potential complication of hyperprolactinemia, and prompt intervention, such as ultrasound-guided aspiration, can provide relief and prevent further complications.4,10
Clinicians should be vigilant in evaluating male patients with gynecomastia for possible hyperprolactinemia and consider the management of the underlying hormonal imbalance to improve patient outcomes. 11
Conclusion
The development of a galactocele should be recognized as a potential complication of patients with hyperprolactinemia and gynecomastia when symptoms of incongruous swelling and pain superimposed. This may be accentuated with problems of compliance with dopamine agonists which may lead to rebound significant hyperprolactinemia which may trigger milk production and its retention.
Footnotes
Acknowledgements
The authors want to acknowledge the internal medicine residency program for scientific support.
Author note
Ethical considerations
This case was approved by the Hamad Medical Corporation’s Medical Research Center.
Consent to participate
A written informed consent was obtained from the patient/patients.
Author contributions
Tarik Elhadd: Proposed the original idea and concept, writing, editing and final approving.
Elabbass A. Abdelmahmuod: Writing, editing and final approving.
Haider Bustanji: Initial writing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Qatar Foundation funded this work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.