
Abstract
Coronavirus disease 2019 (COVID-19) swab testing has been commonplace since the onset of the pandemic, with few reported adverse effects beyond general discomfort. We report a rare clinical presentation of a cerebrospinal fluid leak following a nasopharyngeal COVID-19 swab. The patient, a 49-year-old female with a history of migraines, idiopathic intracranial hypertension (pseudotumor cerebri), fibromyalgia, depression, and prior traumatic brain injury, presented to the emergency department with a headache. The patient underwent nasopharyngeal swab testing 10 days before her visit. She experienced the immediate postprocedure onset of a global headache and clear nasal discharge that persisted until presentation. Physical examination revealed continuous clear rhinorrhea from the left nostril. Associated symptoms included blurry vision, nausea, vomiting, and postural instability. The patient was managed conservatively; the leak and associated symptoms resolved within 24 h. Computed tomography of the head and paranasal sinuses showed no overt skull base defect but revealed subtle dehiscence along the right optic canal and right foramen rotundum, as well as dilation of the optic nerve sheaths. These findings suggest elevated intracranial pressure, which may have predisposed the patient to a cerebrospinal fluid leak. Given the clinical history and temporal relationship, this is a presumptive cerebrospinal fluid leak secondary to the COVID-19 swab; however, no confirmatory testing was performed. Increased awareness of this adverse effect, particularly in patients with pre-existing risk factors, is essential for early diagnosis. Anterior nasal or mid-turbinate swabs may be safer for vulnerable patients, as nasopharyngeal swabs are more frequently linked to iatrogenic skull base injuries according to reported cases. To our knowledge, this represents the 15th reported instance of a post-swab cerebrospinal fluid leak and includes a comprehensive literature review.
Introduction
Since its 2019 onset, the global pandemic has made SARS-CoV-2 testing a cornerstone of disease control. The virus, a member of the Coronavirinae subfamily, colonizes the human nasopharyngeal tract during both active infection and asymptomatic carriage. 1 Prompt testing is essential to differentiate coronavirus disease 2019 (COVID-19) from other respiratory illnesses, such as influenza, which require different isolation protocols. While the CDC recommends several specimen collection methods including anterior nasal and mid-turbinate swabs, the nasopharyngeal swab has remained the preferred method due to its high diagnostic yield.2 –4
Nasopharyngeal COVID-19 testing carries a very low complication rate (0.0012%–0.026%). Common issues include epistaxis, retained swabs, and cerebrospinal fluid (CSF) leaks, typically occurring in patients with high-risk anatomical factors like severe septal deviations or prior sinonasal and pituitary procedures. 5 While several reports have discussed individual complications, this review provides a broad and detailed analysis of currently documented iatrogenic CSF leaks following COVID-19 testing.
Case description
A 49-year-old woman with a history of migraines, idiopathic intracranial hypertension (pseudotumor cerebri), fibromyalgia, depression, and prior traumatic brain injury presented with headache and clear left-sided rhinorrhea. She had undergone a bilateral COVID-19 nasopharyngeal swab approximately 10 days earlier, after which she developed a constant, diffuse headache (Numeric Rating Scale 7), exacerbated by upright posture and head movement. Clear nasal discharge began immediately following the procedure, worsened with standing and activity, and improved when supine. Associated symptoms included blurry vision, nausea, vomiting, and imbalance. Briefly, following the nasopharyngeal swab, the patient experienced the immediate onset of clear nasal discharge and a diffuse headache. These symptoms persisted continuously for 10 days. The patient initially attributed the discomfort to her baseline migraines, but the persistence of the orthostatic headache eventually prompted her to visit the emergency department. Her medications included acetazolamide (dosage: 1000 mg twice daily) for pseudotumor cerebri, as well as treatments for migraines, posttraumatic stress disorder, and depression.
Physical examination was notable for clear fluid draining from the left nostril. The patient was managed conservatively with bed rest and elevation of the head-of-bed to 30°. Computed tomography (CT) of the head showed no acute skull base fracture, but revealed subtle dehiscence along the right optic canal and right foramen rotundum within the sphenoid sinus. Additionally, dilation of the optic nerve sheaths was noted, consistent with the patient’s history of elevated intracranial pressure. Magnetic resonance imaging (MRI) demonstrated nonspecific mild white matter signal changes and a stable, small left middle cerebral artery aneurysm, unchanged from prior imaging.
Neurology and otolaryngology were consulted in the emergency department and followed the patient throughout her hospitalization. Neurology suspected a CSF leak and ordered a cisternogram. An attempt was made to collect nasal fluid for beta-2 transferrin testing; however, neither the cisternogram nor fluid collection was performed, as the nasal drainage resolved spontaneously within 24 h following transfer to the inpatient medicine ward.
Findings suggestive of elevated intracranial pressure on the head CT were unchanged from prior imaging and presumed chronic. While the patient’s history of idiopathic intracranial hypertension is a recognized risk factor for spontaneous skull base attenuation, the etiology in this case appears multifactorial. The chronic elevation of intracranial pressure likely created a preexisting subclinical weakness, which the nasopharyngeal swab then acted upon as an acute mechanical trigger. This distinction acknowledges the underlying physiological vulnerability while highlighting the swab as the inciting event for the symptomatic breach. Acetazolamide was suspended, given the presumptive CSF leak, while other home medications were continued. Following the cessation of nasal drainage, the patient’s associated orthostatic symptoms resolved. Both neurology and otolaryngology services recommended continued conservative management; the patient was treated supportively with bed rest, caffeine, and aggressive hydration. No recurrence of rhinorrhea was observed during the remainder of the hospital course.
Outpatient follow-up with neurology and otolaryngology was recommended for repeat clinical assessment, CT of the paranasal sinuses, and long-term management of migraines and idiopathic intracranial hypertension; delayed cisternography was also planned should symptoms recur.
At approximately 2 weeks postdischarge, the patient followed up with neurology and otolaryngology. CT of the paranasal sinuses without contrast (Figure 1) demonstrated mucosal thickening in the bilateral maxillary, sphenoid, and right frontal sinuses. The skull base appeared previously noted subtle dehiscence, with no evidence of acute fracture or posttraumatic change. No osteitis or osseous erosion was identified. Dilation of the optic nerve sheaths was again noted. This is consistent with findings on prior imaging. These results support a diagnosis of elevated intracranial pressure, which likely predisposed the patient to a traumatic CSF leak during the nasal swab. Although idiopathic intracranial hypertension (pseudotumor cerebri) is a known driver of spontaneous CSF leaks, the strict temporal relationship between the swab and symptom onset points toward a traumatic trigger. The swab likely exacerbated a preexisting subclinical dehiscence or an area of osseous thinning. This resulted in a presumptive CSF leak by transforming a chronic anatomical vulnerability into an acute breach.
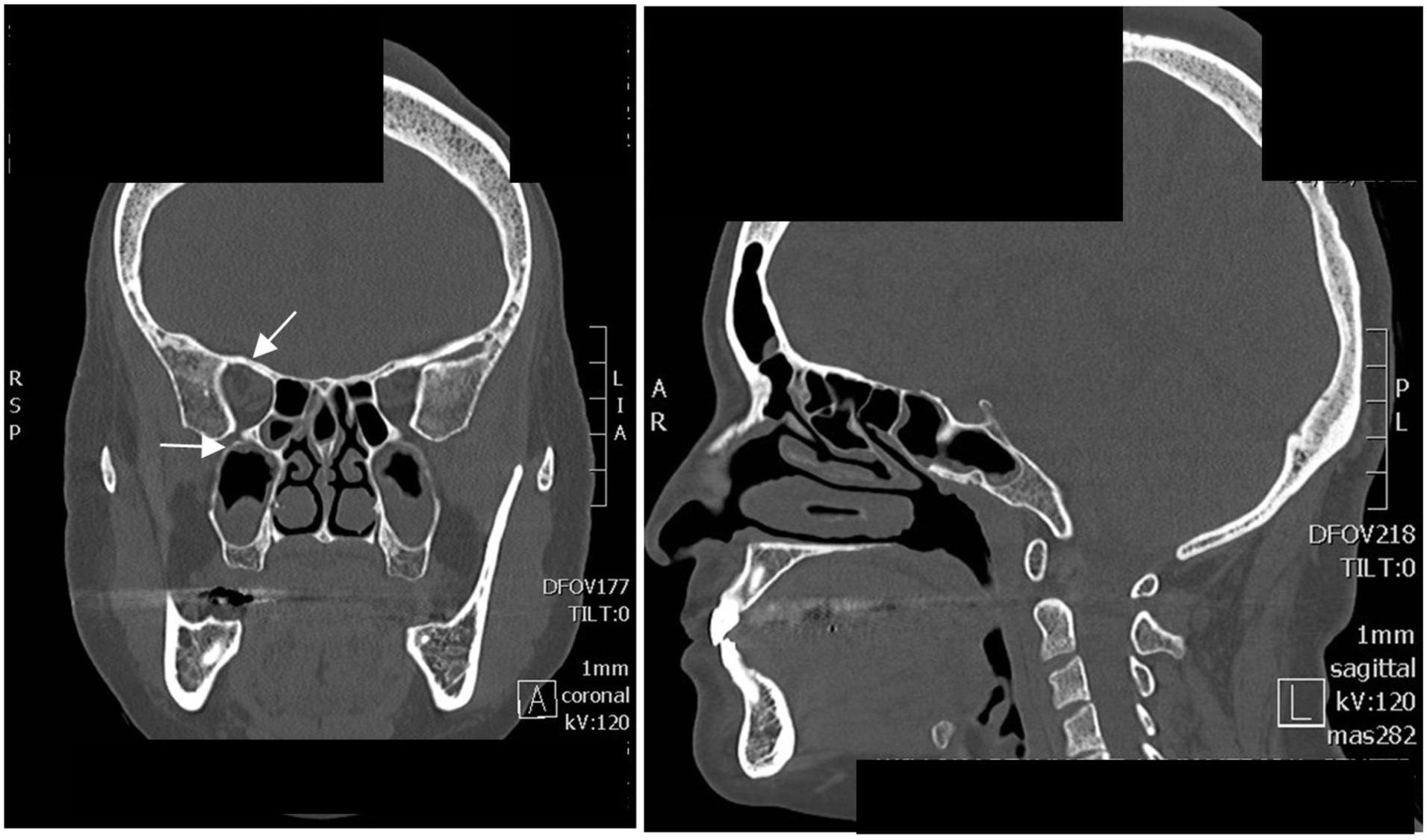
Coronal (a) and sagittal (b) CT scan of the paranasal sinuses without contrast of our patient only demonstrating previously noted subtle dehiscence along the right optic canal, and the right foramen rotundum in the sphenoid sinus. The upper arrow (a) points to the superolateral aspect of the right sphenoid sinus, where the optic canal shows thinning/dehiscence. The lower arrow (a) points to the inferolateral area corresponding to the foramen rotundum. There was no discrete evidence of posttraumatic changes.
The follow-up neurologist recommended butalbital/acetaminophen/caffeine (Fioricet; one or two tablets/capsules every 4 h as needed), continued suspension of acetazolamide, and maintenance of aggressive hydration in the outpatient setting. Otolaryngology advised no further acute intervention but recommended obtaining a fluid sample for beta-2 transferrin testing should the nasal drainage recur.
Discussion
Classification and management strategies
While this case involves a SARS-CoV-2 test, iatrogenic CSF leak during nasopharyngeal sampling is a procedural risk rather than a pathogen-specific one. Nasopharyngeal swabs are the diagnostic standard for various infections, including Influenza A and B, Respiratory Syncytial Virus, Adenovirus, Parainfluenza, Human metapneumovirus, Rhinovirus, Bordetella pertussis, and Neisseria meningitidis. Therefore, the safety considerations discussed here apply to any clinical setting requiring nasopharyngeal access, regardless of the suspected underlying infection.
CSF leaks can be subdivided into two broad categories: traumatic (further divided into iatrogenic and noniatrogenic) and nontraumatic (further divided into high-pressure and low-pressure). There are two main treatment strategies for CSF leaks: conservative versus interventional therapy. These approaches aim to prevent complications, including recurrent meningitis, intracranial abscess, pneumocephalus, and refractory epilepsy. Based on clinical presentation and timing, the findings in this patient likely represent a traumatic, iatrogenic skull base CSF leak resulting from a COVID-19 nasopharyngeal swab, despite the absence of acute fracture on noncontrast CT of the head and paranasal sinuses. The patient received conservative care, typically consisting of bed rest with head-of-bed elevation to 30° for 7–14 days. It is also important to avoid Valsalva maneuvers that increase intracranial pressure. Additional conservative management includes symptomatic control of nausea, vomiting, constipation, and coughing.
Review of reported cases
A study shows that patients predisposed to CSF leaks often present with high-risk anatomical or surgical histories, such as severe septal deviation, skull base defects, or previous transsphenoidal pituitary procedures. 5 To identify comparable cases, a literature search was conducted using PubMed and Google Scholar databases. Keywords included COVID-19 swab, nasopharyngeal swab complications, iatrogenic CSF leak, and skull base injury. We included English-language case reports and series that specifically detailed CSF rhinorrhea following nasal swab testing. There have been 14 reported cases of iatrogenic CSF leaks following nasal or nasopharyngeal swabs for COVID-19.6–19 The clinical history and findings of these 14 cases, along with our case, are summarized in Table 1. Among the 15 total patients, 2 underwent multiple nasal swabs. Patient ages ranged from 40 to 67 years; 10 (66.7%) were female and 5 (33.3%) were male. Four patients (26.7%) had a past medical history involving risk factors for CSF leak, including idiopathic intracranial hypertension, bacterial meningitis, or prior head trauma. All 15 patients presented with unilateral clear rhinorrhea, with the exception of 1 patient who presented with straw-colored nasal discharge. 18
Literature review of iatrogenic CSF leak after a nasal swab for COVID-19 including the current case.
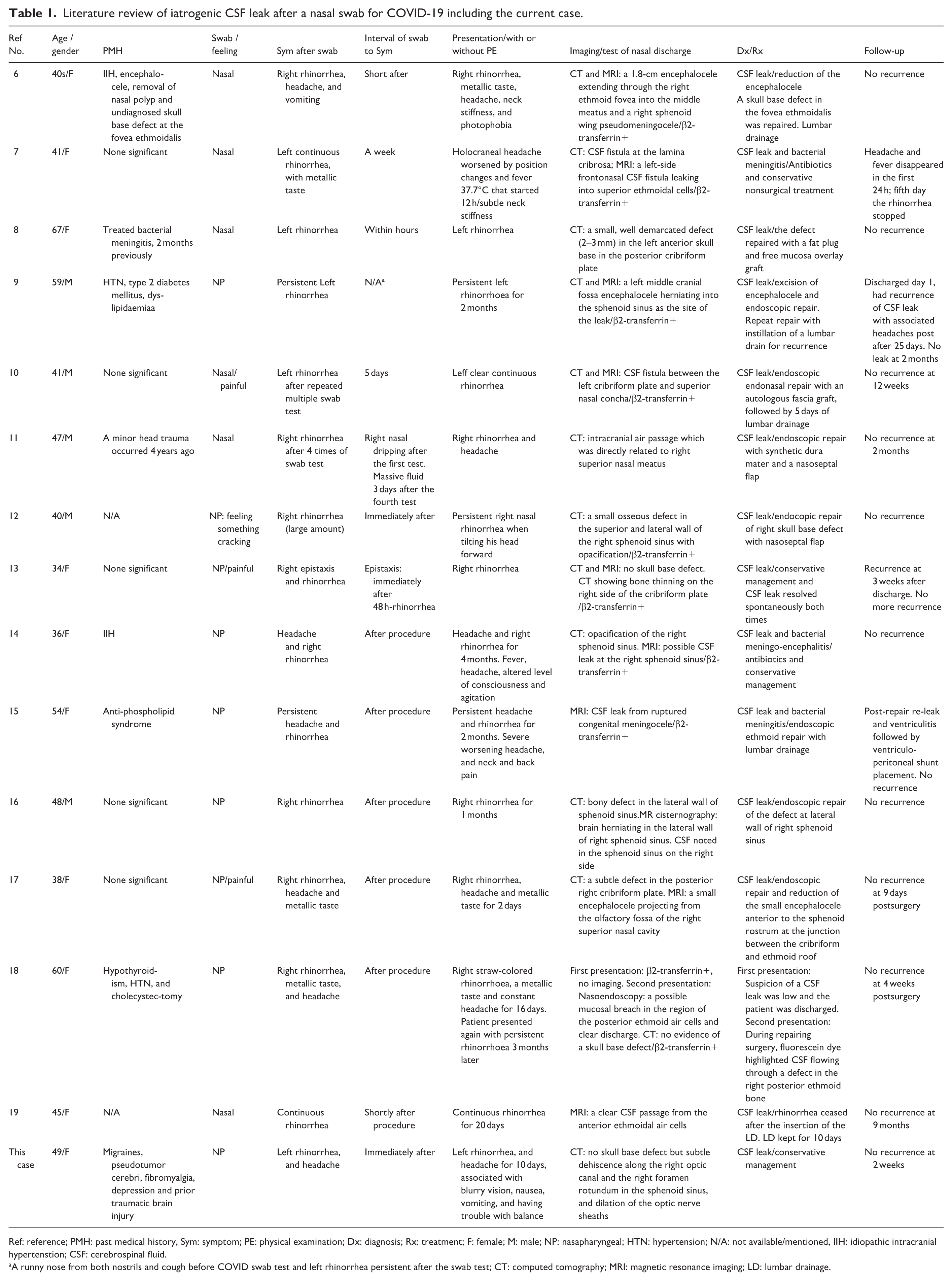
Ref: reference; PMH: past medical history, Sym: symptom; PE: physical examination; Dx: diagnosis; Rx: treatment; F: female; M: male; NP: nasapharyngeal; HTN: hypertension; N/A: not available/mentioned, IIH: idiopathic intracranial hypertenstion; CSF: cerebrospinal fluid.
A runny nose from both nostrils and cough before COVID swab test and left rhinorrhea persistent after the swab test; CT: computed tomography; MRI: magnetic resonance imaging; LD: lumbar drainage.
Various associated symptoms were reported: 8 patients (53.3%) had headaches, 4 (26.7%) reported a metallic taste, 2 (13.3%) experienced vomiting, and 3 (20%) had neck stiffness, including 2 patients who presented with clinical evidence of meningitis.7,14 One patient reported photophobia, 6 and only our patient experienced blurry vision and balance difficulties. The interval between swab testing and symptom onset ranged from immediately after the procedure to 1 week. CT and/or MRI revealed skull base defects in 12 of 15 patients (80%), while 3 patients (20%), including ours, had no evidence of acute traumatic injury.13,18 Beta-2 transferrin testing of nasal discharge was conducted in nine patients (60%), all of whom tested positive. Surgical repair was performed in 10 patients (66.7%), while 5 (33.3%), including ours, were successfully managed with conservative therapy.
Following treatment, CSF leaks and associated symptoms resolved in all 15 patients. Recurrences occurred in two patients (13.3%): one following initial surgical repair 9 and another following conservative care. 13 These were managed with repeat surgical repair and continued conservative management, respectively, with no further recurrences noted during the follow-up period.
Risk of meningitis and prognosis
The incidence of meningitis ranges from 10% to 37% in patients with CSF leaks. 20 Prophylactic antibiotics are not routinely prescribed but should be considered in high-risk patients, such as those with an active sinonasal infection or a history of prior meningitis. 20 For patients with traumatic skull base defects and nondisplaced linear fractures less than 1 cm without acute intracranial complications, spontaneous healing occurs in 70%–80% of cases within 1 week,21,22 with nearly all patients healing within a few months.21,22 Our literature review identified two patients (13.3%, 2/15) who developed meningitis and meningoencephalitis, respectively, following COVID-19 nasal or nasopharyngeal swabs.7,14 Both cases achieved complete recovery with antibiotic therapy and nonsurgical management. If conservative treatment fails to resolve the leak, surgical intervention is indicated.
Importance of prompt diagnosis
Awareness of the rare adverse effect of a CSF leak following COVID-19 swab testing is crucial for prompt diagnosis and intervention. In our case, with conservative management, the patient’s clear nasal discharge resolved spontaneously within 24 h. This resolution occurred prior to sample collection for beta-2 transferrin testing. In contrast, a previously published case involved a COVID-19 swab-induced CSF leak with a positive beta-2 transferrin test only identified after discharge. The patient was lost to follow-up for 3 months, suffering persistent symptoms until re-presentation and eventual surgical management. 18
A key limitation of this case is the absence of biochemical or radiographic confirmation. Although a cisternogram was planned, the resolution of the CSF leak following conservative management upon admission precluded both fluid collection and specialized imaging. Consequently, the diagnosis remains presumptive, based on the strong temporal relationship between the swab and the onset of symptoms. This underscores the diagnostic challenge when successful conservative management leads to a resolution of symptoms before confirmatory tests can be completed.
Comparison of swab methods and clinical recommendations
It has been observed that saliva, nasal, and oropharyngeal samples are, on average, less sensitive than nasopharyngeal samples obtained by healthcare professionals. It is therefore improbable that such sensitivity levels would meet the requirements for RT-PCR (Reverse Transricption Polymerase Chain Reaction)-based COVID-19 confirmation. 23 Among the 15 reviewed cases, 9 patients (60%) underwent nasapharyngeal (NP) swabs and 6 (40%) underwent nasal swabs. While these figures do not establish a definitive incidence rate, they reflect the distribution of sampling methods reported in cases of iatrogenic CSF leakage currently documented in the literature. Notably, three of the nine patients who received NP swabs reported a ‘cracking’ sensation or severe pain during the procedure.12,13,17 Similarly, one patient who received a nasal swab reported severe pain. 10 To mitigate the risk of skull base injury, clinicians should consider anterior nasal or mid-turbinate swabs as safer alternatives for patients with known risk factors. These methods minimize deep penetration toward the skull base in individuals with preexisting anatomical vulnerabilities.
A comprehensive analysis of the MAUDE database and literature has shown that while headache and epistaxis are relatively common, occurring at rates of 11% and 17%, respectively, the most severe reported complications of COVID-19 testing involve meningitis following CSF leaks. 24 Because iatrogenic injuries can lead to significant morbidity, contemporary management has shifted toward a multidisciplinary approach. 25 While the endonasal endoscopic technique is often required to localize and repair exact leak sites, such as those near the cribriform plate or sphenoid sinus, there is a growing recognition that conservative protocols must be more robustly integrated into the patient’s care path. 25 This includes not only physical measures such as bed rest but also advanced pharmacological strategies to manage the associated orthostatic pain, which our study highlights as a key clinical necessity often absent from larger systematic reviews.
Conclusion
The diagnosis of a CSF leak can be challenging, particularly when imaging does not reveal a definitive skull base defect, as seen in our patient. In such instances, a detailed clinical history and the recognition of characteristic symptoms such as unilateral clear rhinorrhea and positional headaches are essential to complement imaging for timely diagnosis. This case report, supported by a comprehensive literature review, highlights the complexities in diagnosing a post-swab CSF leak and establishing a clear clinical correlation. Our findings suggest that utilizing anterior nasal or mid-turbinate swabs instead of nasopharyngeal swabs may be a beneficial consideration for vulnerable patients, as nasopharyngeal swabs are more frequently represented in reported cases of iatrogenic skull base injury. However, because the total number of swabs performed is unknown, these observations do not establish definitive incidence rates or prove the superiority of one technique over another. Larger epidemiological studies are needed to further evaluate the relative safety profiles of different swabbing methods. To our knowledge, this represents the 15th case of a CSF leak following a COVID-19 nasal swab reported in the literature.
Footnotes
Ethical considerations
Our institution does not require ethics approval for reporting individual cases. This case report has been completely anonymized, and all data/imaging was obtained as part of the standard of care for the patient. Every effort was made to contact the patient to obtain written informed consent; however, the patient was lost to follow-up. The data have been fully anonymized to protect patient privacy.
Author contributions
Jeremy Shi collected the data. Jeremy Shi, Ya Xu, and Chinyere Mbagwu interpreted, edited, and wrote the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.