
Abstract
This report describes a rare case of a woman whose tubal pregnancy was unexpectedly identified during a caesarean section, resulting in the delivery of a live infant at a gestational age of 42 + 0 weeks. Despite multiple antenatal visits, three ultrasound examinations, and the presence of clinical signs, the tubal pregnancy was not recognized preoperatively. This case highlights the diagnostic challenges of advanced tubal pregnancy, the clinical overlap with abdominal pregnancies, and the importance of careful abdominal examination and improved ultrasonographic awareness, particularly in low-resource settings.
Introduction
Tubal pregnancy is the most common form of ectopic pregnancy, accounting for over 90% of all ectopic pregnancies. 1 Although advanced ectopic pregnancies are rare overall, several case reports of abdominal pregnancies have described liveborn infants delivered at term.2–5 Advanced tubal pregnancies resulting in live birth are exceedingly uncommon. Tubal pregnancies are almost always diagnosed and treated early, given the high likelihood of symptoms such as abdominal pain and haemorrhage due to tubal rupture, combined with the widespread availability of early ultrasonography and laboratory testing. 1 In recent years, a few case reports have been published on advanced tubal pregnancies; only one reported delivery of a liveborn infant at term, though the gestational age remained unclear because the patient could not recall her last normal menstrual period (LNMP) and no ultrasound had been performed prior to presentation. 6 In contrast, in our case, the gestational age was reliably established from a certain LNMP and subsequently supported by ultrasound. To our knowledge, no recent report has documented a tubal pregnancy progressing to 42 + 0 weeks with neonatal survival. Although the outcome for both mother and child was good, advanced tubal pregnancies carry substantial risks. This case highlights key diagnostic pitfalls, essential learning points, and the similarities and distinctions between advanced tubal and abdominal pregnancies.
Case presentation
A 20-year-old woman, gravida 2 para 1, presented to our referral hospital in Western Tanzania at 41 + 6 weeks of gestation with mild labour-like pain, which subsided upon arrival. On examination, the foetal head was not engaged but was palpated at the umbilical level. Bedside ultrasound showed a viable foetus in longitudinal lie, with findings suggestive of placenta praevia centralis. No foetal biometry was performed. An elective caesarean section was scheduled for the following day.
The gestational age was calculated based on the LNMP, of which the patient was certain. Although no first-trimester ultrasound was performed, a scan done at her first antenatal visit at 17 + 5 weeks showed an intrauterine, viable foetus with a fundal posterior placenta, with foetal growth consistent with the gestational age estimated from the LNMP. The patient attended an antenatal clinic five times at a different health facility, with haemoglobin levels recorded at each visit, but no documentation regarding fundal height or abdominal examination. A second ultrasound at 40 + 5 weeks reported a single intrauterine feotus in cephalic presentation, with adequate amniotic fluid and a posterior placenta. She reported no abdominal pain or vaginal bleeding during pregnancy.
Surgical findings
At 42 + 0 weeks, an elective caesarean section was performed. After opening the fascia, membranes were visible through the peritoneum, containing meconium-stained amniotic fluid (Figure 1). A female neonate weighing 3.0 kg was delivered with Apgar scores of 5, 7, and 9. Intraoperative inspection revealed that the gestational tissue was not attached to the uterus. Instead, the placenta was attached to the enlarged and highly vascular distal end of the right fallopian tube, with no identifiable ipsilateral ovarian tissue (Figure 2). The uterus appeared small and non-gravid, while the left adnexa were normal. A right salpingo-oophorectomy was performed. Histopathology was not obtained due to financial constraints.

Membranes visible through the peritoneum.
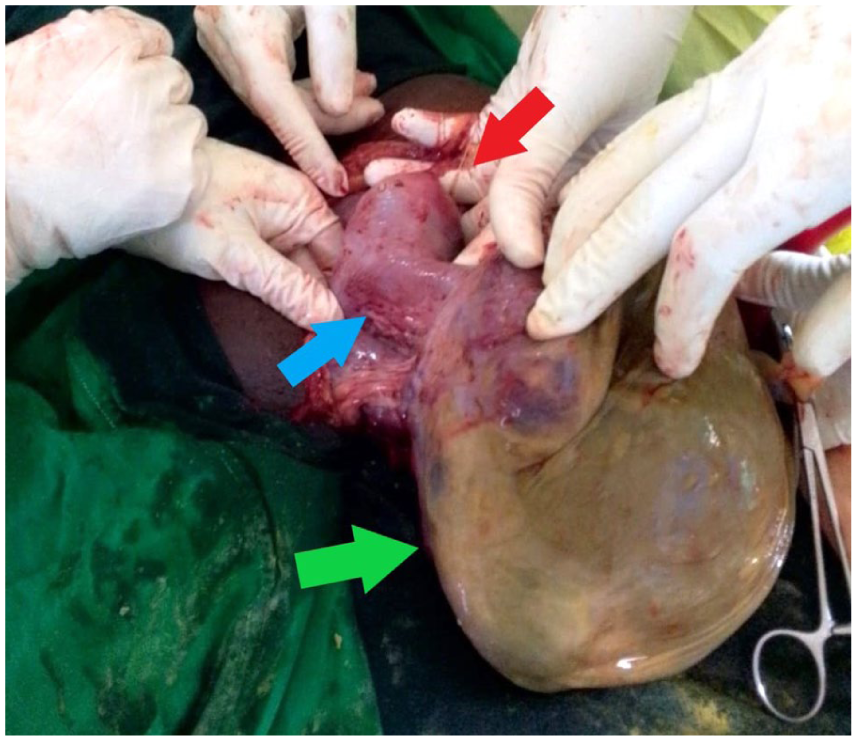
Intraoperative findings: top arrow (red) points to the uterus, the middle arrow (blue) shows the enlarged right fallopian tube, the bottom arrow (green) points to the placenta and membranes.
Outcome and follow-up
The maternal postoperative course was uneventful, and the mother was discharged 48 h postpartum.
Although the neonate cried immediately after delivery, the initial adaptation was suboptimal. Due to an oxygen saturation of 60%, the infant was admitted to the NICU for supplemental oxygen via nasal prongs. Due to persistent tachypnoea and an ongoing oxygen requirement, a chest X-ray was performed, which revealed features consistent with meconium aspiration syndrome. Empirical intravenous antibiotics were administered to cover for potential neonatal sepsis. The infant’s condition gradually improved, and oxygen therapy was discontinued after 13 days. The infant was discharged in a stable condition on postpartum day 15.
Discussion
In advanced ectopic gestation, abdominal and tubal pregnancies are distinguished based on Studdiford’s criteria. 7 In our patient, intraoperative involvement of the fallopian tube and ovary excluded abdominal pregnancy, supporting classification as a tubal pregnancy. 7 Both abdominal and tubal pregnancies are extremely rare and are associated with high foetal mortality and maternal morbidity.3,8–10 Term abdominal pregnancies are reported more frequently than term tubal pregnancies. Our search identified 5 recent third-trimester tubal pregnancies,6,8,9,11,12 of which only 2 progressed beyond 37 weeks.6,8 Van der Bijl and Mabesa 8 reported an intrauterine foetal death at 39 weeks, with tubal pregnancy diagnosed only after failed induction. Onuh et al., 6 reported a live birth from a term tubal pregnancy, though the gestational age remained unclear. In our case, the gestational age was accurately determined from a certain LNMP and supported by ultrasound, representing the first documented tubal pregnancy progressing to 42 + 0 weeks with neonatal survival.
Our case highlights the diagnostic difficulty of advanced tubal pregnancy. The pregnancy was initially misdiagnosed as normal and later as placenta previa. In previously reported third-trimester tubal pregnancies, diagnosis was established only upon hospital admission, reflecting the typically late recognition.6,8,9,11 In those cases, the diagnosis was established preoperatively by ultrasound, whereas in our case, the diagnosis was made only intraoperatively. However, perioperative diagnosis is frequently reported in abdominal pregnancy, even when antenatal ultrasounds suggested intrauterine gestation.2,4,5,10 Notably, several abdominal pregnancies were also misdiagnosed as placenta previa.2,10
Since advanced tubal pregnancy is rare, systematic data on its typical clinical presentation are lacking. Our patient was asymptomatic; however, reported symptoms range from severe abdominal pain to mild bleeding or a complete absence of symptoms.6,8,9,11 Although an earlier case by Radaelli et al. reported severe foetal growth restriction associated with tubal placental implantation, our case and other previously published cases demonstrate that this finding is not universal.6,8,9,11,12 A possible explanation is placental blood supply from the right ovarian artery, as described by Onuh et al. 6 Abnormal foetal position or superficial palpation of foetal parts should, in our view, raise suspicion for an extrauterine pregnancy. Notably, none of the published reports on tubal pregnancies comments on abdominal examination findings, whereas we consider this to be a key element in recognizing advanced ectopic pregnancy. However, this case also illustrates that such signs are often overlooked. In our patient, the foetal head was located in the umbilical region and palpated superficially beneath the abdominal wall, yet these atypical findings were not recognized as signs of a term ectopic pregnancy. This underscores the importance of thorough antenatal physical examination.
However, abdominal examination alone does not distinguish between tubal and abdominal pregnancy. Early transvaginal ultrasonography remains the most reliable method for detecting ectopic implantation. 1 As the pregnancy advances, accurate diagnosis becomes increasingly challenging. Our case illustrates that the diagnosis may be overlooked despite multiple ultrasound examinations, as also reported by Koçak et al. 9 This may reflect limited awareness of the ultrasonographic signs of advanced tubal pregnancy. Although no specific criteria exist for the sonographic diagnosis of advanced tubal pregnancies, Allibone et al. 13 described ultrasound features suggestive of advanced abdominal pregnancy. These include visualization of pregnancy tissue outside the uterus with an empty uterine cavity, absence of myometrium between the membranes and the bladder, a fetus unusually close to the abdominal wall, or an abnormally located placenta. In our view, these findings may also contribute to the recognition of advanced tubal pregnancies, which have a nearly identical sonographic appearance.
Initial diagnostic considerations for tubal pregnancy are similar to those for abdominal pregnancy, but distinguishing between them is essential for appropriate management. In both, laparotomy is the treatment of choice. In all reported third-trimester tubal pregnancies, either salpingectomy or salpingo-oophorectomy has been performed.6,8,9,11 Although blood loss was often substantial, surgery is generally more straightforward than in abdominal pregnancy, where management depends heavily on the placental implantation site. 3 Preoperative mapping of placental attachment by CT or MRI is strongly recommended, but was not available in our setting, as in many published cases of both tubal and abdominal pregnancy. 3 Why the diagnosis of a term tubal pregnancy in our case was established only intraoperatively is difficult to determine. It illustrates that antenatal care is not merely a matter of quantity but also of quality. Despite improvements in antenatal care in Tanzania, many women still present late for their first antenatal consultation. Only 34% of Tanzanian women comply with the WHO recommendation to attend antenatal care before 12 weeks of gestation.14,15 Our patient first presented at 17 weeks and attended 5 antenatal visits, fewer than the 8 recommended. 15 Although she fulfilled the WHO recommendations by undergoing an early ultrasound and two additional scans, this diagnostic course failed to detect the tubal pregnancy, likely reflecting limited skills in recognizing advanced extrauterine gestations. The complete absence of documentation regarding abdominal examinations raises the question of whether physical examination was performed at all. Abdominal examination may provide the first clinical clue to advanced extrauterine pregnancy and remains an essential part of routine antenatal care.
Learning points
Advanced tubal and abdominal pregnancies can present with similar clinical and sonographic features, and both may be misinterpreted as an intrauterine pregnancy or placenta previa.
Abnormal foetal position or foetal parts palpated superficially should raise suspicion for an extrauterine pregnancy; abdominal examination remains essential.
Distinguishing tubal from abdominal pregnancy is important, as surgical management differs in complexity and associated risk.
Conclusion
A term tubal pregnancy with survival of the infant is exceptionally rare and poses considerable diagnostic challenges. In our patient, clinical signs were present but not recognized, underscoring the need for greater awareness and careful interpretation of atypical findings. Despite multiple antenatal visits and ultrasounds, the diagnosis was only made intraoperatively, highlighting that antenatal care depends not only on access but also on the quality of clinical assessment. Systematic attention to abdominal examination and improved ultrasonographic expertise are essential for earlier detection and improved outcomes.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
The patient has provided written informed consent for publication and the use of her data and photographs in this report.
Author contributions
C.M. Nelen: Contributed to the clinical management of the presented case and was the surgeon during the described surgical procedure. Responsible for the conception and design of the report, the literature search, and the drafting of the manuscript.
E.S. Bitabo: The assistant surgeon during the described surgical procedure, reviewed the manuscript draft, and provided critical feedback for revisions.
G.G. Kulikiza: Contributed to the clinical management of the presented case, reviewed the manuscript draft, and provided critical feedback for revisions.
B.S. Gumodoka: Supervised during clinical care, provided guidance and critical review of the manuscript.
All authors have approved the final version of the report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.