
Abstract
Parotid gland malignancies are rare and represent less than 5% of all head and neck cancers. Squamous cell carcinoma of the parotid gland is an uncommon subtype and is often associated with aggressive clinical behavior. While regional lymphatic spread is common, distant metastases to organs such as the lungs, brain, and liver are rare but indicate advanced disease and poor prognosis. We report a 60-year-old male with primary right parotid squamous cell carcinoma who initially presented with facial nerve paralysis and locally advanced infiltrative disease requiring debulking parotidectomy followed by chemoradiotherapy. Despite multimodal treatment, the patient developed progressive metastatic disease with respiratory symptoms, ocular pain, and worsening clinical status. Computed tomography imaging revealed extensive metastatic involvement including multiple bilateral pulmonary nodules with a dominant left perihilar mass, multiple cerebral metastases demonstrating ring-enhancing lesions with marked surrounding vasogenic edema, pleural metastatic involvement, and multiple hepatic hypodense lesions. An incidental left thyroid lobe nodule was also identified and subsequent fine-needle aspiration cytology confirmed benign colloid goiter. The patient received palliative chemotherapy with carboplatin and paclitaxel alongside supportive therapy. This case highlights the aggressive metastatic potential of parotid squamous cell carcinoma, the possibility of progressive systemic dissemination despite multimodal therapy, and the importance of comprehensive imaging in detecting disease progression and guiding management.
Keywords
Introduction
Parotid gland malignancies are rare, accounting for less than 5% of all head and neck cancers, with an estimated annual incidence of 1–3 cases per 100,000 population. 1 Squamous cell carcinoma (SCC) of the parotid gland is an uncommon histologic subtype, representing less than 5% of salivary gland malignancies, and is generally associated with aggressive clinical behavior, high locoregional recurrence rates, and poor prognosis.2,3 Primary parotid SCC is particularly rare and remains a diagnosis of exclusion because a substantial proportion of cases initially classified as primary tumors are later found to represent metastatic cutaneous SCC involving intraparotid lymph nodes. 4 Therefore, careful dermatologic examination, endoscopic evaluation, cross-sectional imaging, and histopathologic assessment are essential to exclude other primary sources before confirming the diagnosis of primary parotid SCC. 4
Patients commonly present with rapidly enlarging parotid swelling, pain, facial nerve dysfunction, cervical lymphadenopathy, or local invasion into adjacent soft tissues and skull base structures. 5 Facial nerve paralysis is considered an important clinical indicator of aggressive disease and advanced local tumor infiltration. 6 Although regional lymphatic spread is relatively common, distant metastases involving the lungs, liver, brain, and pleura are uncommon and usually indicate advanced-stage disease with poor survival outcomes.7,8 Previous studies have reported median survival of less than 12 months in patients with systemic metastatic disease. 8
Comprehensive imaging plays a central role in diagnosis, staging, treatment planning, post-treatment surveillance, and assessment of disease progression in parotid malignancies. Contrast-enhanced computed tomography (CT) and magnetic resonance imaging are particularly useful for evaluating tumor extent, skull base invasion, nodal involvement, and intracranial extension, while PET(Positron Emission Tomography)/CT may assist in detecting occult metastatic disease and excluding other primary SCC sources.4,9,10 Despite multimodal treatment approaches including surgery, chemotherapy, and radiotherapy, advanced parotid SCC may demonstrate persistent locoregional disease and progressive distant dissemination. 11
We report a rare case of aggressive primary parotid SCC with persistent locoregional progression despite multimodal therapy, followed by pulmonary, cerebral, pleural, and hepatic metastases. This case highlights the aggressive metastatic potential of parotid SCC and underscores the importance of comprehensive radiologic evaluation in detecting disease progression and guiding oncologic management.
Case presentation
Initial clinical presentation
A 60-year-old male initially presented with a 6-month history of progressively enlarging right-sided facial swelling associated with ipsilateral otalgia, purulent ear discharge, and progressive facial asymmetry. Clinical examination prior to surgery demonstrated right-sided lower motor neuron facial nerve paralysis, suggesting advanced local disease with perineural involvement.
A thorough head and neck dermatologic examination was performed and did not reveal any cutaneous primary lesion, reducing the likelihood of metastatic cutaneous SCC.
Preoperative imaging and staging
Preoperative contrast-enhanced CT of the head, neck, chest, and abdomen demonstrated a heterogeneous cystic right parotid mass measuring approximately 1.2 × 2.1 × 1.0 cm. No intracranial lesions, pulmonary nodules, or abdominal metastases were identified at that time. Brain parenchyma appeared normal.
These findings were consistent with a localized parotid gland malignancy without radiologically detectable distant metastatic disease.
Initial surgery and histopathology
The patient underwent partial right parotidectomy at Muhimbili National Hospital in April 2024. Intraoperatively, the procedure was converted to debulking surgery due to extensive tumor infiltration into adjacent deep soft tissue structures, limiting the feasibility of complete oncologic resection.
Histopathological examination revealed well-differentiated SCC (grade 1) of the parotid gland. The tumor was staged as pT3N0M0 based on available surgical and imaging findings. However, complete details regarding margin status and perineural invasion were not fully retrievable from outside records.
Postoperative reassessment at Ocean Road Cancer Institute
Following referral to the Ocean Road Cancer Institute (ORCI) in May 2024, repeat contrast-enhanced CT of the head and neck demonstrated a residual infiltrative enhancing soft tissue mass in the right parotid region, measuring approximately 45 × 33 mm. The lesion extended medially into the parapharyngeal space and involved the styloid process, eustachian tube region, and medial and lateral pterygoid muscles, with extension toward the skull base (fossa lacerum), though without definite intracranial invasion.
Right level IV cervical lymphadenopathy with central necrosis was also present.
Initial systemic staging with chest radiograph and abdominal ultrasonography at ORCI showed no evidence of distant metastasis.
Multimodal oncologic treatment
Following multidisciplinary tumor board discussion, the patient received:
Induction chemotherapy: Cisplatin (75 mg) and docetaxel (120 mg) for six cycles
Followed by definitive external beam radiotherapy: 66 Gy in 33 fractions
Treatment completion: December 2024
The treatment intent was curative at this stage, given the absence of radiologically detected distant metastases.
Early post-treatment assessment
In January 2025, approximately 1 month after completion of chemoradiotherapy, the patient re-presented with persistent right ear pain and discharge.
Follow-up CT imaging demonstrated:
Persistent right parotid region soft tissue mass measuring 5.3 × 3.9 × 2.1 cm
Right level IVb cervical lymphadenopathy
No new distant metastases at that time
These findings were consistent with persistent locoregional disease rather than a complete response.
Development of distant metastatic disease
In June 2025, routine follow-up chest radiography revealed multiple rounded soft tissue nodules in the right hemithorax, consistent with pulmonary metastases. The patient was subsequently commenced on palliative chemotherapy (carboplatin and paclitaxel), completing multiple cycles between 2025 and early 2026.
Presenting illness and disease progression
The patient later presented with progressive chest pain, dry cough, and worsening functional status.
Contrast-enhanced CT imaging demonstrated multiple intracranial metastatic lesions involving both cerebral hemispheres and deep gray nuclei, predominantly at the gray–white matter junction, showing ring and heterogeneous enhancement with marked vasogenic edema (Figure 1). The largest lesion in the right temporo-occipital region measured approximately 3.0 × 2.9 cm and produced mass effect with effacement of the ipsilateral lateral ventricle. In the head and neck region, there was residual infiltrative disease involving the right external auditory canal (Figure 2), middle ear, and mastoid with associated bony destruction of the temporal and spheno-occipital bones, extending toward the cavernous sinus, along with necrotic right level II cervical lymphadenopathy measuring 3.0 cm (Figure 3). In the chest, multiple bilateral pulmonary nodules and masses were present, including a dominant left perihilar mass measuring 6.0 × 7.5 × 6.0 cm with pleural nodular thickening suggestive of metastatic involvement (Figure 4). Abdominal imaging revealed multiple hypodense hepatic lesions, the largest measuring 4.6 cm, consistent with hepatic metastases (Figure 5). An incidental left thyroid lobe nodule measuring 2.3 × 2.0 × 2.9 cm was also identified, which on fine-needle aspiration cytology was confirmed to be benign colloid goiter.
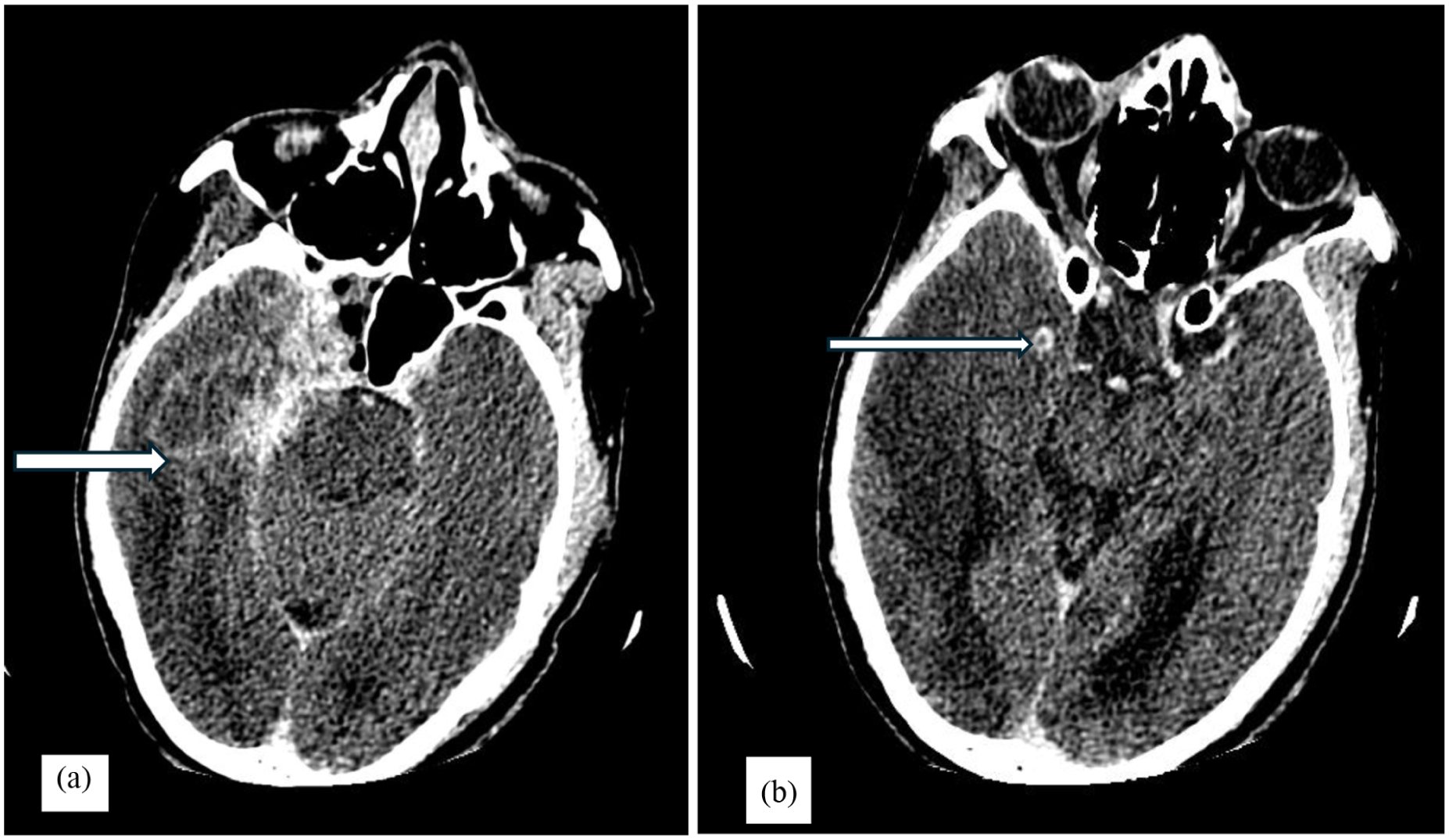
Brain metastasis. Axial contrast-enhanced CT images of the brain (a and b) demonstrating cerebral ring-enhancing lesions at the gray–white matter junction with surrounding vasogenic edema (white arrows), consistent with cerebral metastasis.
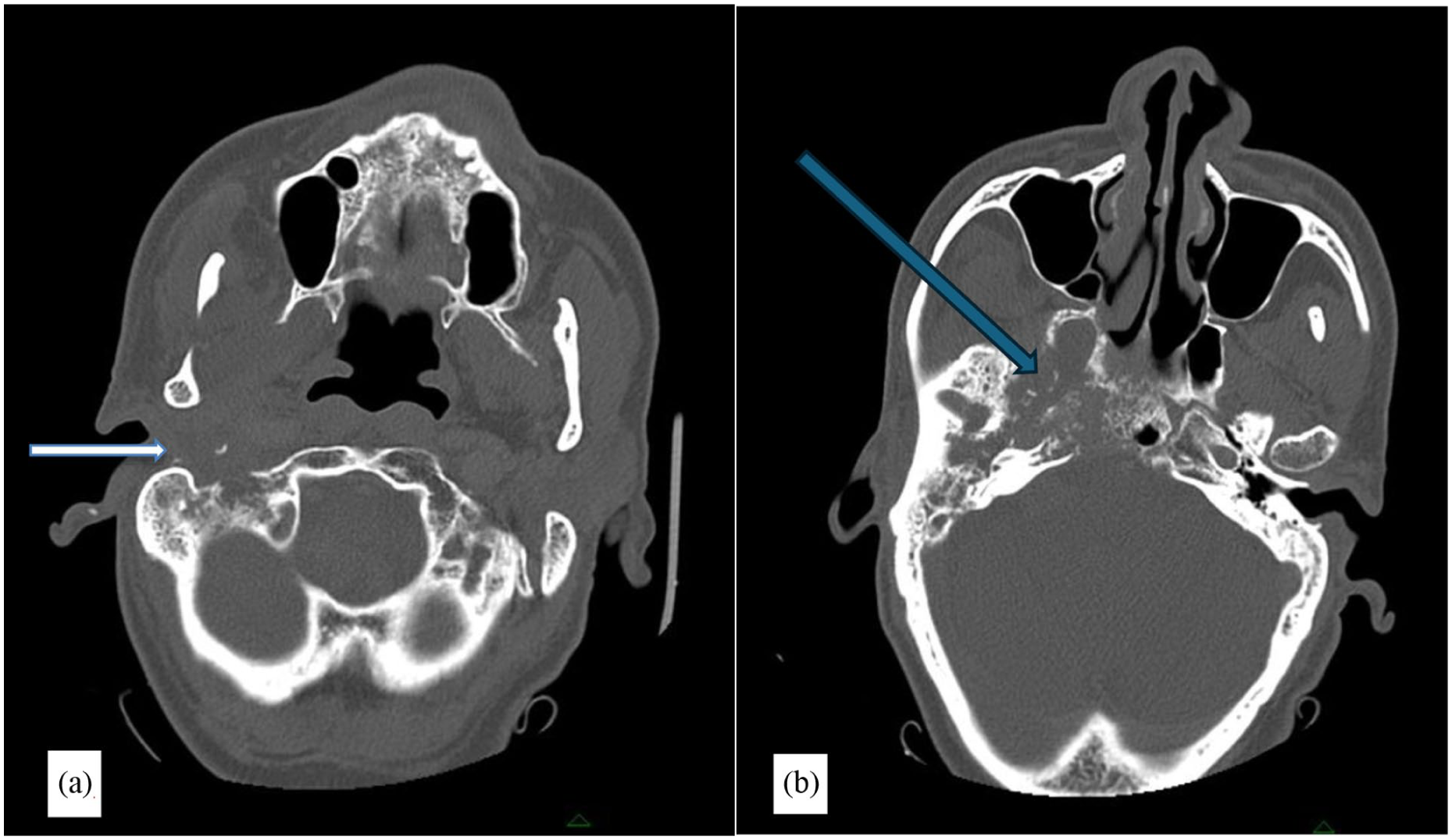
Skull base tumor extension. Axial CT images (bone window) at the level of the skull base demonstrating soft tissue density filling the right external auditory canal and middle ear cavity (white arrow in image a) with lytic destruction of the adjacent skull base structures (blue arrow in b), consistent with local tumor extension of parotid squamous cell carcinoma.
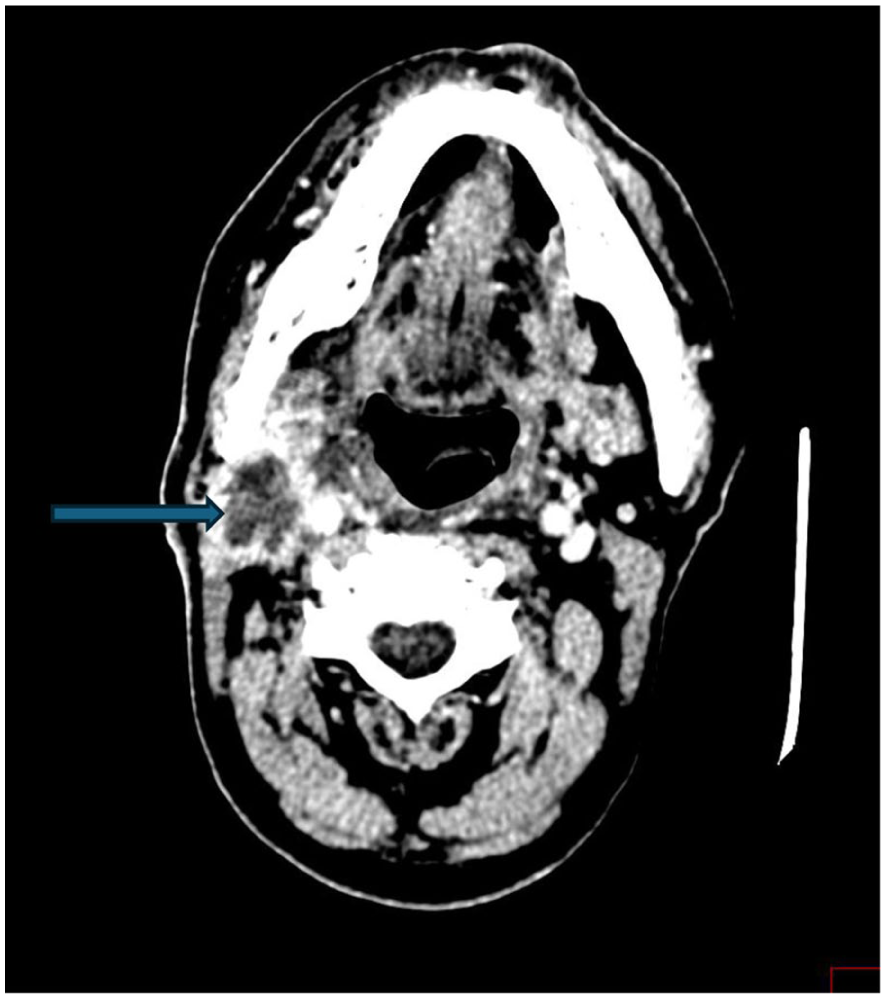
Cervical nodal metastasis. Axial CT image at the level of the mandible demonstrating an enlarged necrotic right level I (submandibular) cervical lymph node (blue arrow), consistent with nodal metastasis.
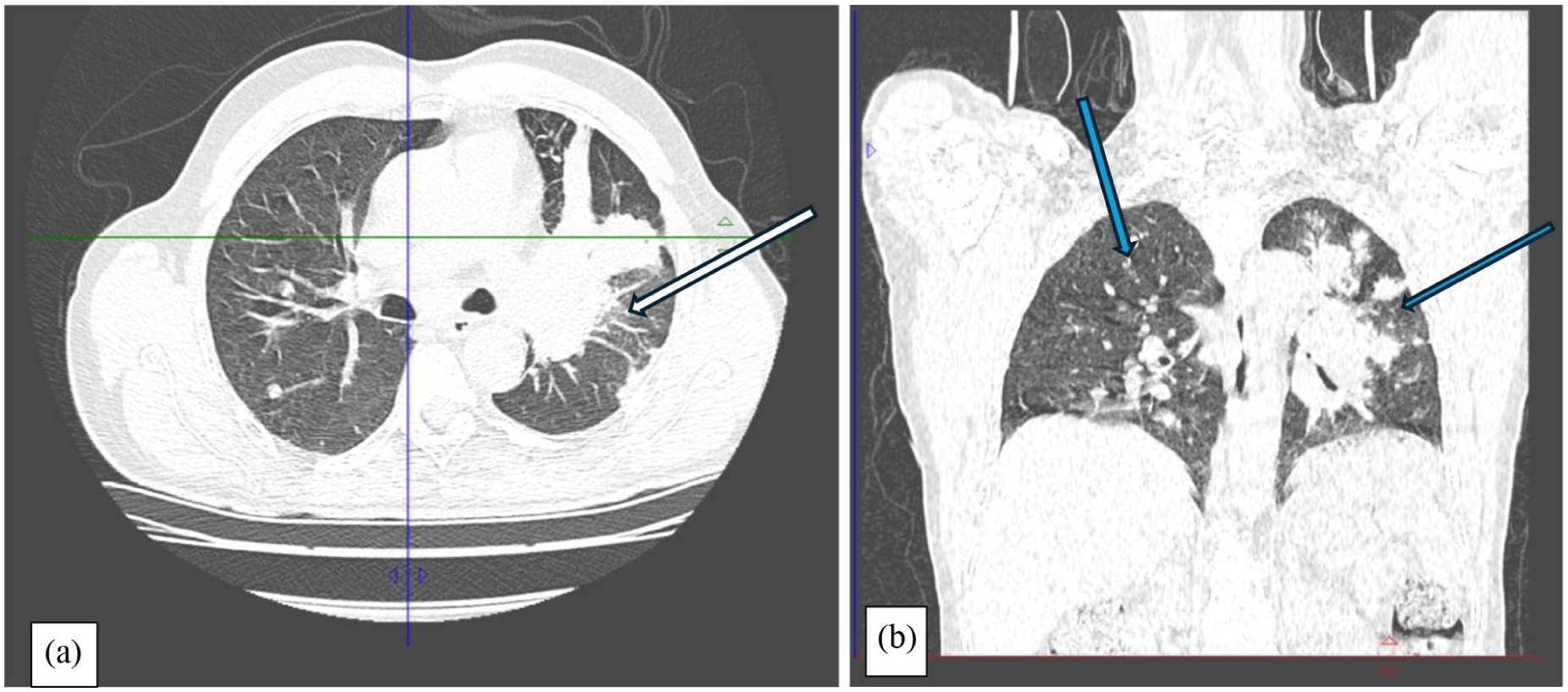
Pulmonary metastases. Axial (a) and coronal (b) CT images of the chest (lung window) demonstrating a large left perihilar mass (white arrow) and multiple bilateral pulmonary nodules (blue arrows), consistent with pulmonary metastatic disease.
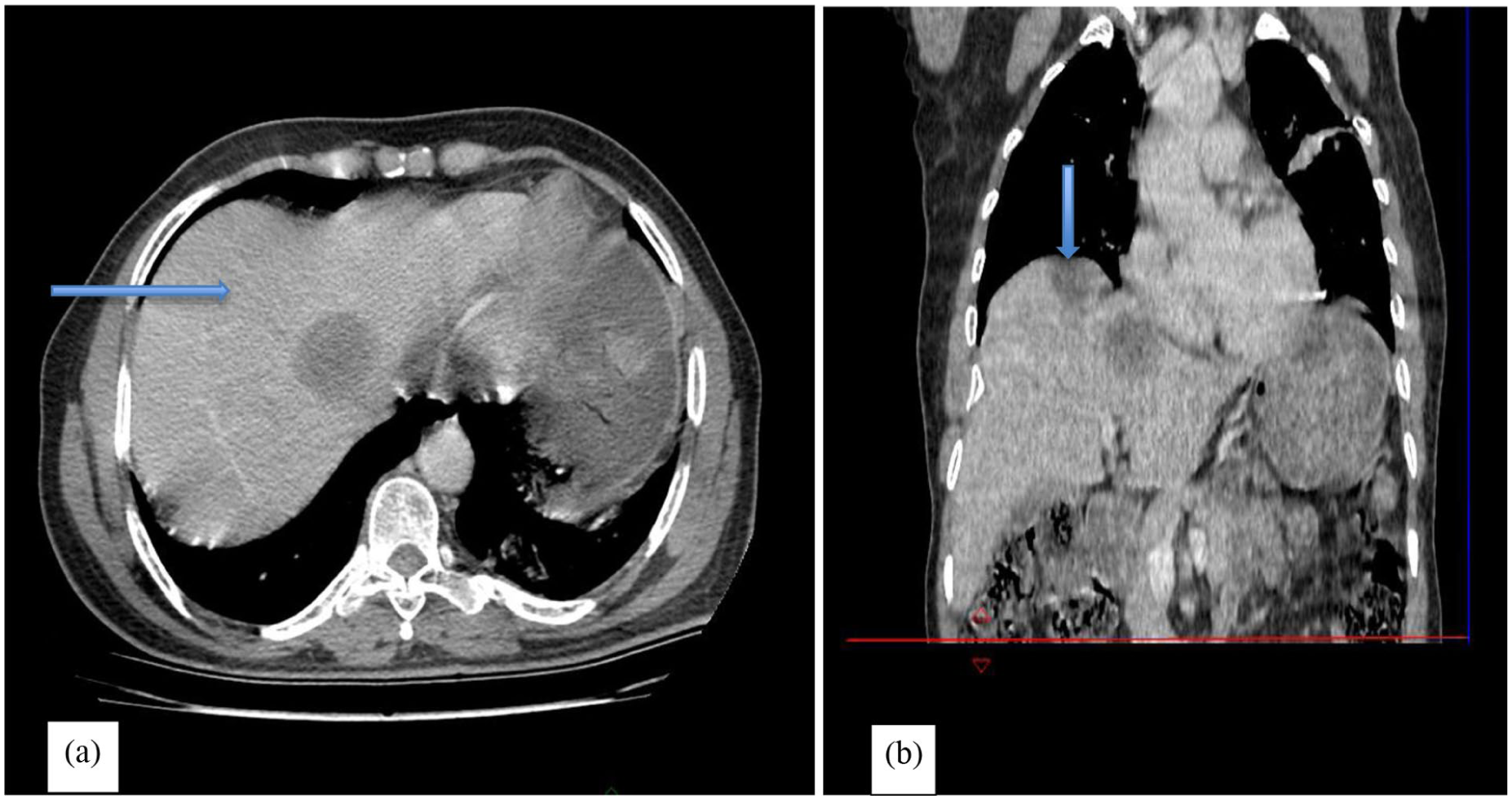
Hepatic metastases. Contrast-enhanced axial (a) and coronal (b) CT images of the abdomen demonstrating multiple hypodense lesions within the hepatic parenchyma (blue arrows), consistent with hepatic metastases.
Clinical findings are presented in a structured chronological timeline to ensure clarity of disease progression and interventions (Figure 6).
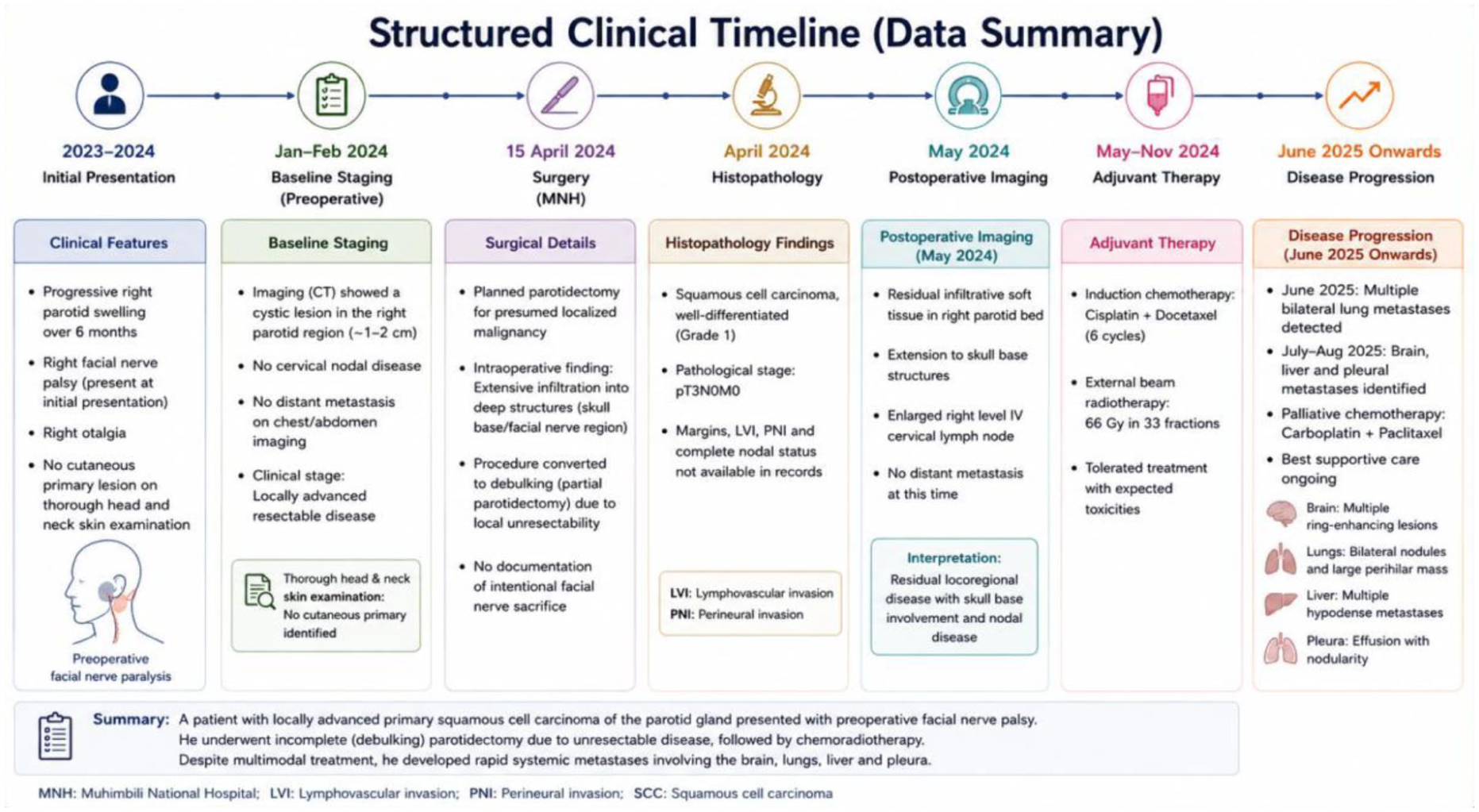
Structured clinical timeline.
Discussion
Parotid SCC is a rare and clinically aggressive malignancy, accounting for a small proportion of salivary gland tumors, with reported local recurrence rates of up to 50%. 12 Primary parotid SCC is particularly uncommon and remains a diagnosis of exclusion, requiring careful evaluation to rule out metastatic cutaneous SCC from the head and neck region.1,2
Distant metastases in salivary gland malignancies are uncommon but represent a major determinant of prognosis. Overall, systemic metastatic disease has been reported in approximately 15%–30% of patients with advanced salivary gland carcinomas, depending on stage and histologic subtype. 4 Among patients who develop distant spread, the lungs are the most frequently involved organ, accounting for approximately 60%–80% of metastatic cases, followed by bone and liver involvement, while brain metastases are considerably less frequent, occurring in less than 10%–15% of cases.4,5 Pleural and synchronous multi-organ metastases, as observed in the present case, are particularly rare and generally reflect advanced hematogenous dissemination with poor clinical outcome.
Distant metastases involving the lungs, brain, and liver are uncommon in parotid SCC but are strongly associated with poor prognosis.5,8 Pulmonary metastases typically present as multiple bilateral nodules, occasionally with cavitation, while cerebral metastases commonly localize at the gray–white matter junction and demonstrate ring-enhancing lesions with surrounding vasogenic edema. 10 Hepatic metastases usually appear as hypodense lesions on contrast-enhanced CT, reflecting hematogenous spread. 3 In the present case, the combination of bilateral pulmonary nodules, a dominant perihilar mass, multiple brain metastases with marked edema, pleural involvement, and hepatic lesions reflects widespread systemic dissemination.
Prognosis in parotid SCC is primarily determined by tumor stage, margin status, perineural invasion, nodal disease, and facial nerve involvement at presentation.2,3 Early facial nerve paralysis, skull base invasion, and deep tissue infiltration are well-established indicators of aggressive tumor biology and poor outcome. Inadequate local control or incomplete resection in advanced disease may contribute to persistent locoregional tumor burden, which can subsequently facilitate systemic metastatic spread.
Accurate initial staging and aggressive multidisciplinary management are essential in optimizing outcomes. Comprehensive imaging and meticulous histopathological assessment play a central role in defining disease extent and guiding treatment planning. In the present case, extensive local infiltration at the time of surgery necessitated debulking rather than complete resection, highlighting the advanced nature of the disease at presentation.
Treatment options for metastatic parotid SCC remain limited, with platinum-based chemotherapy regimens forming the backbone of palliative systemic therapy. 8 Radiotherapy plays an important role in locoregional control and symptom palliation, particularly in cases with skull base involvement or neurological compromise. Supportive measures, including corticosteroids for cerebral edema and palliative care integration, are essential in advanced disease to optimize quality of life. 13
Recent studies highlight emerging roles for immunotherapy and targeted agents in salivary gland malignancies; however, evidence in parotid SCC remains limited, and no standardized systemic therapy beyond cytotoxic chemotherapy currently exists.14,15 Overall, this case underscores the aggressive biological behavior of parotid SCC, the potential for rapid multi-organ metastatic dissemination, and the critical importance of comprehensive radiologic evaluation in staging, follow-up, and treatment guidance.
Conclusion
This case illustrates the highly aggressive biological behavior of parotid SCC, with potential for persistent locoregional disease and subsequent widespread multi-organ metastasis despite multimodal treatment. The pattern of pulmonary, cerebral, pleural, and hepatic involvement underscores the unpredictable and advanced metastatic potential of this malignancy. Comprehensive cross-sectional imaging is essential not only for accurate staging and early detection of disease progression but also for guiding timely multidisciplinary and palliative management strategies aimed at optimizing symptom control and patient quality of life in advanced-stage disease.
Footnotes
Ethical Considerations
This case report was prepared in accordance with institutional and ethical standards for publication. Patient confidentiality and privacy were maintained throughout the preparation of the manuscript, and all identifying information was removed.
Consent to Participate
Written informed consent was obtained from the patient for publication of this case report and the accompanying clinical and radiological images.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.