
Abstract
Acquired ptosis may result from multiple etiologies, including aponeurotic, neurogenic, myogenic, traumatic, and mechanical causes. When structural eyelid abnormalities are prominent, the clinical signs of underlying neuromuscular disorders may be physically masked and difficult to recognize. A patient in her 70s presented with an acute onset of unilateral ptosis. Neuroimaging revealed an incidental aneurysm of the left middle cerebral artery that was anatomically independent of the oculomotor nerve. Ophthalmic examination suggested aponeurotic ptosis, and surgical repair restored eyelid height immediately. However, fluctuating ptosis with diurnal variation was observed 1 week postoperatively. Electromyography showed a postsynaptic neuromuscular junction disorder. Together with positive acetylcholine receptor antibodies, ocular myasthenia gravis was diagnosed. Treatment with oral pyridostigmine resulted in marked clinical improvement. Severe aponeurotic disinsertion can obscure the fatigability typical of ocular myasthenia gravis and delay recognition of the underlying disorder. In patients with atypical presentations such as acute-onset ptosis, additional evaluation, including electrophysiological testing, is essential to identify coexisting neuromuscular dysfunction.
Background
Acquired ptosis is a common condition encountered in ophthalmology clinics. It is defined as the drooping of the upper eyelid that was previously in a normal anatomical position. 1 While involutional aponeurotic ptosis is the most common subtype among all types of acquired ptosis, accounting for over 60% of cases, 2 the possibility of dual etiology must be considered.
The evaluation of acquired ptosis requires careful etiological differentiation and often involves multiple specialties. For example, acute ptosis caused by oculomotor nerve compression from an intracranial aneurysm requires neurosurgical intervention, while aponeurotic ptosis typically requires eyelid surgery performed by ophthalmologists. 3 By contrast, the diagnosis and medical management of myasthenia gravis (MG) rely primarily on neurologist consultation. This report highlights the “mechanical masking effect” where severe mechanical eyelid drop obscures the fluctuating signs of an underlying neuromuscular disorder.
Case presentation
A patient in her 70s presented to the emergency department with an acute onset of left upper eyelid drooping that had persisted for ~5 h. She had a history of hypertension, while her family and psycho-social histories were unremarkable. Neurological examination revealed isolated left-sided ptosis with no other focal deficits. An emergent non-contrast computed tomography (CT) of the brain was unremarkable. However, magnetic resonance angiography identified a 4.5 mm aneurysm at the bifurcation of the left middle cerebral artery (M1 segment; Figure 1). Neurosurgical consultation determined that the aneurysm was unlikely to be compressive, given its distal location from the third cranial nerve.

(a, b) Magnetic resonance angiography showing a 4.5 mm aneurysm at the bifurcation of the left middle cerebral artery (M1 segment), deemed unrelated to the ptosis. White arrows indicate the aneurysm.
Ophthalmic examination revealed bilateral dermatochalasis and left upper eyelid ptosis. A high eyelid crease and deep superior sulcus were observed on the left side. Margin reflex distance-1 was initially reported as stable, measuring 3 mm on the right and 0 mm on the left (Figure 2(a)). Levator function was 13 mm in the right and 10 mm in the left eye, and Bell’s phenomenon was normal. Pupils remained equal and reactive, and ocular motility was full. Given the findings, a diagnosis of aponeurotic ptosis was made. The patient underwent bilateral upper eyelid blepharoplasty combined with left levator aponeurosis advancement. Intraoperatively, the levator aponeurosis was found detached from the tarsus and was reattached with non-absorbable 5-0 sutures. Marked improvement in left palpebral fissure height was observed, with reduction of contralateral compensatory elevation attributed to Hering’s law (Figure 2(b)).
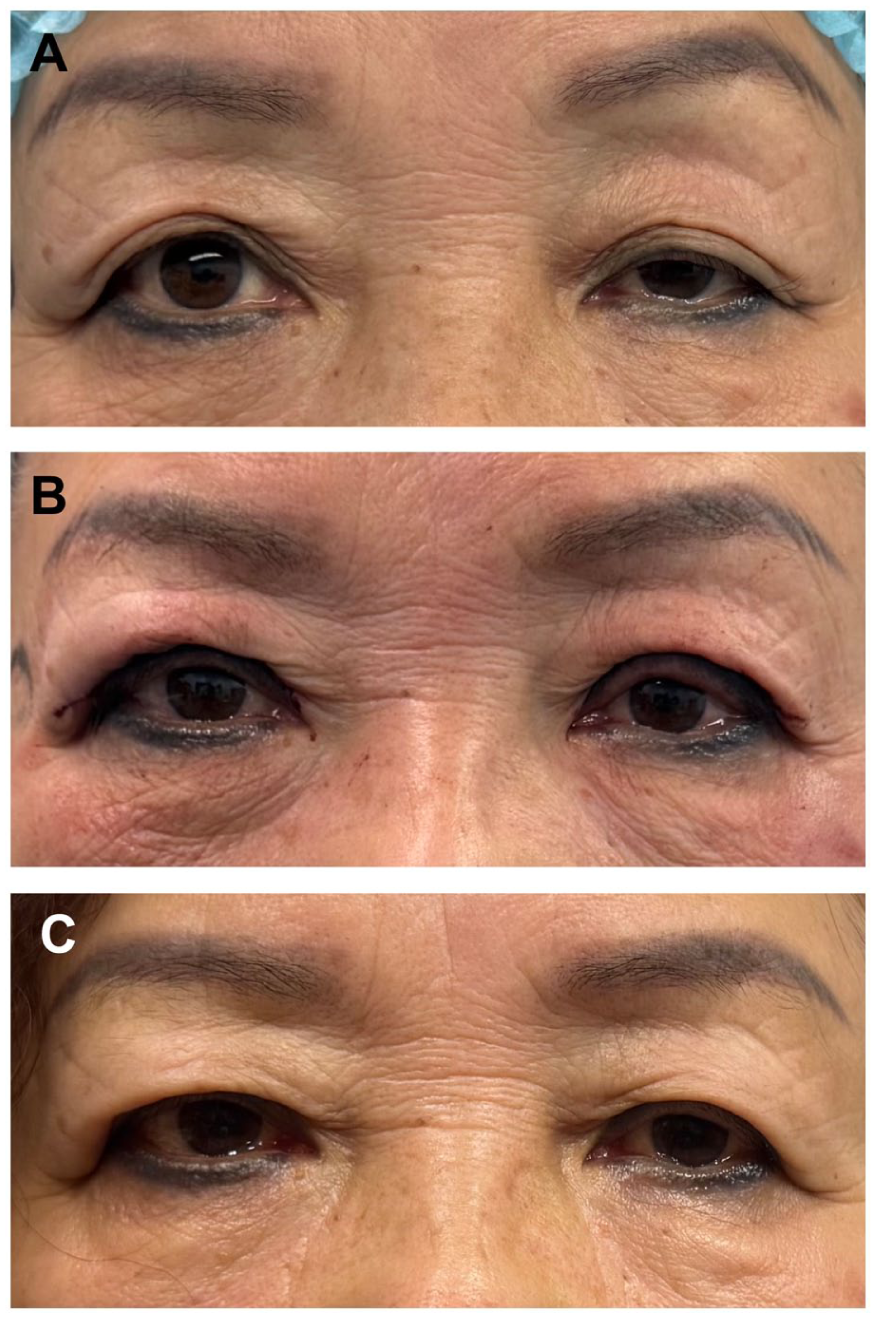
(a) Preoperative photograph showing asymmetric ptosis. The MRD-1 was 3 mm on the right and 0 mm on the left. A high eyelid crease and deep sulcus were observed on the left side. (b) Immediate postoperative result after levator aponeurosis advancement. A marked improvement in left palpebral fissure height was observed, with a reduction of contralateral compensatory elevation attributed to Hering’s law. (c) Three months postoperative result. Palpebral fissure height is symmetric bilaterally.
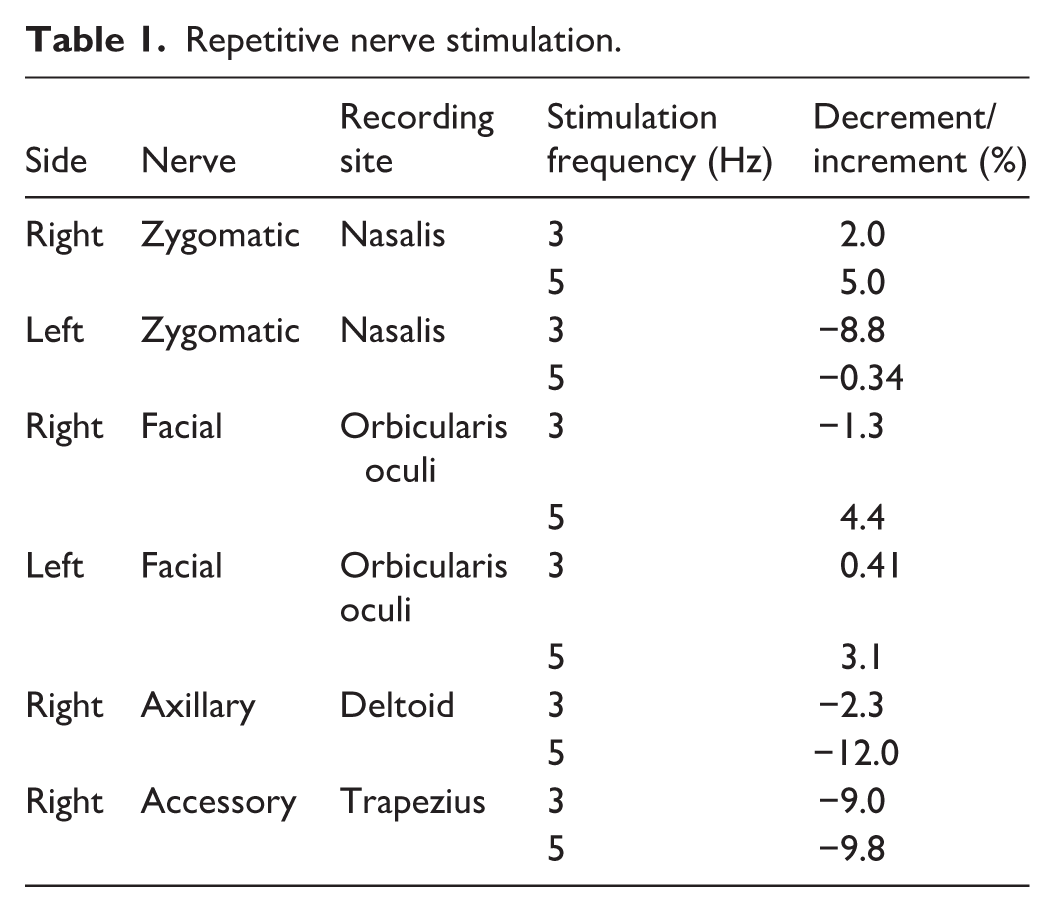
At follow-up, 1 week later, the patient exhibited fluctuating ptosis of the left upper eyelid. The ptosis was particularly noticeable toward the end of the day or with sustained use. On further questioning, she reported diurnal variation and worsening with fatigue. A fatigue test was positive, and serologic testing revealed positive acetylcholine receptor antibodies at a titer of 1:32. Electromyography (EMG) was performed to evaluate neuromuscular transmission. Repetitive nerve stimulation demonstrated a 12% decremental response in the right axillary nerve recording from the deltoid muscle (Table 1). A facilitation test showed no significant post-exercise amplitude increase in the right ulnar or median nerves (Table 2). These electrophysiological findings were suggestive of a neuromuscular junction disorder, likely a postsynaptic membrane lesion. A diagnosis of ocular MG (OMG) was confirmed.
Repetitive nerve stimulation.
Amplitude changes pre- and post-exercise (facilitation test).
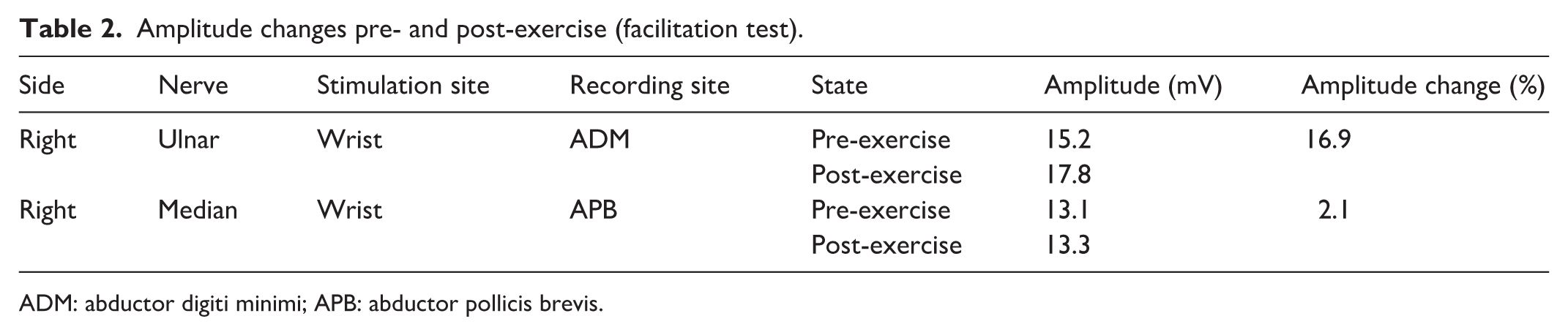
ADM: abductor digiti minimi; APB: abductor pollicis brevis.
Subsequent chest CT showed no evidence of thymoma. Additional immunological tests, including antinuclear antibody profile, anti-neutrophil cytoplasmic antibody panel, immunoglobulins, complement, erythrocyte sedimentation rate, and thyroid function tests, were all within normal limits. The patient was started on oral pyridostigmine (30 mg, three times daily). She demonstrated excellent adherence to the medication and reported no adverse cholinergic side effects. At the 3-month follow-up, her condition remained stable with no signs of generalized MG, indicating a favorable prognosis (Figure 2(c)).
Discussion
Acquired ptosis may arise from several mechanisms, including neurogenic, aponeurotic, myogenic, traumatic, and mechanical causes. 2 In patients presenting with sudden unilateral ptosis, excluding neurological emergencies such as intracranial hemorrhage or aneurysmal compression of the oculomotor nerve is the first priority. 4 In the present patient, the aneurysm was located at the middle cerebral artery bifurcation, anatomically distant from the oculomotor nerve pathway, and therefore unlikely to explain the ptosis.
Aponeurotic ptosis is the most common subtype of acquired ptosis and typically develops gradually in elderly individuals due to levator aponeurosis dehiscence or detachment. 5 OMG is an autoimmune disorder characterized by fluctuating weakness of the levator palpebrae superioris and extraocular muscles. 6 Although previous literature has documented concurrent etiologies of acquired ptosis, 7 recognizing both conditions at the initial presentation remains challenging due to their overlapping clinical features. For instance, the coexistence of MG and thyroid eye disease often presents with mixed structural and functional abnormalities that complicate the diagnosis. 8 Beyond concurrent etiologies, diagnostic confusion also arises when structural factors mislead clinical judgment. Some reports have detailed instances where MG masquerades as isolated congenital ptosis, primarily because the classic fluctuating weakness may be subtle. 9 Furthermore, a history of mechanical injury, such as levator traction during recent cataract surgery, can provide a deceptive structural explanation that confounds the differential diagnosis of acquired ptosis. For instance, in a case reported by Wong and Cullen, suspected surgical trauma acted as a clinical distractor masking metastatic infiltration that mimicked a neuromuscular condition. 10 However, in most of these scenarios, the dynamic signs of MG are still clinically detectable, albeit subtle. Our case represents a rare example demonstrating a complete mechanical masking effect.
In this patient, intraoperative findings confirmed complete detachment of the levator aponeurosis from the tarsus. This structural defect produced a marked mechanical limitation that reduced the effective transmission of levator muscle force. As a consequence, neuromuscular fatigability could not be observed clinically before surgery. After surgical reattachment restored mechanical continuity, the underlying neuromuscular transmission deficit became apparent, and fluctuating ptosis was observed during follow-up.
Two factors likely contributed to the delayed recognition of OMG. First, the presence of a clear anatomical defect directed clinical attention toward a structural diagnosis. Typical features, such as a high eyelid crease and deep superior sulcus, supported the diagnosis of aponeurotic ptosis. However, the acute onset over several hours was atypical for isolated aponeurotic ptosis, which usually develops gradually. 2 Second, the characteristic signs of OMG, including fatigability and diurnal fluctuation, were masked by the mechanical restriction caused by the detached aponeurosis. We believe the primary educational value of this case report lies in demonstrating the specific phenomenon in which a definitive structural defect completely masks a concurrent neuromuscular disorder.
Several practical considerations may help avoid similar diagnostic delays. Previous photographs can help determine the chronicity of eyelid drooping. Clinical tests such as the fatigue test should be considered when evaluating ptosis, although their sensitivity may be reduced when eyelid movement is mechanically restricted. In patients with atypical presentations, particularly those with an acute onset of ptosis despite presenting clear anatomical defects, clinicians should maintain a high index of suspicion for concurrent etiologies. In such scenarios, additional investigations, including serological testing and EMG, may assist in detecting underlying neuromuscular disorders. When both aponeurotic ptosis and OMG are suspected, medical stabilization of neuromuscular transmission should generally precede eyelid surgery in order to achieve more predictable surgical outcomes.
Despite the educational value of this case, certain limitations must be acknowledged. As a single retrospective report, the clinical findings cannot be broadly generalized. Furthermore, because the severe aponeurotic disinsertion provided a structural explanation at the initial presentation, specific preoperative evaluations for MG were not performed. Consequently, the precise presurgical baseline of her neuromuscular junction function remains unrecorded (Supplemental Material).
Conclusion
Severe aponeurotic disinsertion may obscure the fatigability typical of OMG and delay recognition of the underlying disorder. In patients with atypical presentations such as acute-onset ptosis, clinicians should suspect concurrent etiologies even when a clear anatomical defect is present. Careful evaluation and appropriate neurological testing may help identify coexisting neuromuscular disease.
Patient perspective
I am highly satisfied with the medical care I received. Once the correct diagnosis was made and the daily medication was started, my eyelid position stabilized completely. I am very happy with both the final functional and cosmetic results.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X261459530 – Supplemental material for Delayed diagnosis of ocular myasthenia gravis in a patient with aponeurotic ptosis: A case report
Supplemental material, sj-docx-1-sco-10.1177_2050313X261459530 for Delayed diagnosis of ocular myasthenia gravis in a patient with aponeurotic ptosis: A case report by Jiajun Xie, Huina Zhang and Juan Ye in SAGE Open Medical Case Reports
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board of the Second Affiliated Hospital, Zhejiang University School of Medicine (no. 2025-1457).
Consent for publication
The patient provided written informed consent for the publication of this case report and the associated clinical images. This consent was obtained in accordance with the institutional guidelines of the Second Affiliated Hospital, Zhejiang University School of Medicine.
Author contributions
Jiajun Xie wrote the main manuscript text, and Huina Zhang prepared Figures 1, 2, and Supplementary. All authors reviewed the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by the Natural Science Foundation of China (82000938 and 82330032) and Educational Reform Project of the Second Clinical Medical College, Zhejiang University (20240218).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.