
Abstract
Soft tissue injuries of the foot are common in scenarios such as traffic accidents and construction site incidents, involving damage to the plantar fat pad, blood vessels, nerves, and important tendon tissues. The treatment of these injuries faces significant challenges. A 46-year-old male patient suffered soft tissue injuries to the plantar and calcaneus of his right foot due to trauma, without any fractures. Following injury, the patient developed spasms in the right gastrocnemius muscle for unknown reasons. Nevertheless, after undergoing several sessions of negative pressure wound therapy to treat the soft tissue injury on the foot, the spasms in the gastrocnemius muscle resolved, and the soft tissue damage on the plantar and calcaneus of the right foot was effectively treated. This research presents a case of utilizing negative pressure wound therapy to treat a trauma patient with a foot injury-induced gastrocnemius spasms. By explaining and discussing the changes in spasm symptoms post-treatment, the clinical significance and potential mechanism of negative pressure wound therapy in managing foot soft tissue injuries causing gastrocnemius spasms are investigated.
Introduction
Soft tissue injuries in the foot are more likely to occur in scenarios such as traffic accidents and construction site accidents, commonly seen in cases of severe external trauma such as crushing and smashing. The foot serves as a major support and force-bearing point for the entire body, with important functions such as weight-bearing and walking, making it essential for frontline clinicians to pay attention to foot injuries.1,2 The soft tissues of the foot mainly consist of the plantar fat pad, muscles and tendons, ligaments, cartilage, and crucial blood vessels and nerves. Injuries to the soft tissues of the foot often accompany damage to the nerve endings around the toes, and even damage to the tibial and peroneal nerves, leading to loss of sensation and motor function in the toes.3,4 However, it is extremely rare and has not been reported in the literature that stimulation of proximal nerves by soft tissue foot injuries can induce spasms in the calf muscles. After soft tissue injury, a vicious cycle often forms between pain and muscle spasm, hindering recovery and functional restoration. The intense pain signal from tissue damage triggers protective muscle contractions in the affected and surrounding areas, leading to muscle spasm. Prolonged muscle spasms increase intramuscular pressure, compressing capillaries and arterioles, significantly reducing local tissue blood flow. Local ischemia results in inadequate tissue oxygen and nutrient supply, along with the accumulation of metabolic waste products like lactate, activating or sensitizing pain receptors, exacerbating ischemic pain, and increasing the frequency of muscle spasms. This pain–spasm–ischemia–inflammation cycle delays wound healing and impedes functional recovery. Breaking this cycle is crucial in treating foot trauma and secondary muscle spasms. Nambi proposed the “pain–spasm–inflammation–stimulus” cycle in his research on piriformis syndrome. 5
The case report involves a man who sustained significant soft tissue injuries on the plantar and dorsal sides of his right foot in a car accident. Subsequent to the initial debridement, he developed involuntary spasms in the posterior muscle group of his right lower leg, with a predominance of spasms in the soleus muscle. Following several rounds of surgical debridement and treatment with negative pressure wound therapy (NPWT) at our facility, the spasms subsided, and there was successful healing of the soft tissue wound on his right foot.
Case report
A 46-year-old male presented with a soft tissue defect and spasm of the gastrocnemius muscles in the right foot for 20 days. The injury occurred when he accidentally got caught in a harvester, causing the right foot to rupture, bleed, and have a soft tissue defect, resulting in pain and limited movement. X-ray examination at the local hospital did not reveal any obvious fractures in the right foot. He underwent debridement and NPWT in the emergency room. Six days post-operation, he developed spasm of the right gastrocnemius muscles, which was frequent and persistent. Despite another round of debridement and NPWT 2 days later, the spasm in the right gastrocnemius muscles did not improve. Upon examination, it was noted that the right foot NPWT is well-positioned. Following the removal of the NPWT device, extensive skin defects are observed on the dorsal and plantar surfaces of the right foot, reaching deep into the bone with some tendons and soft tissues exposed. The muscle color appears gray–red (Figure 1). The dorsalis pedis artery on the right foot is not palpable. Sensation, movement, and blood flow in the skin of the right toes are functional. The Achilles tendon on the right side is slightly tense, with tenderness in the walking area. Pain level: visual analog scale at level 8.
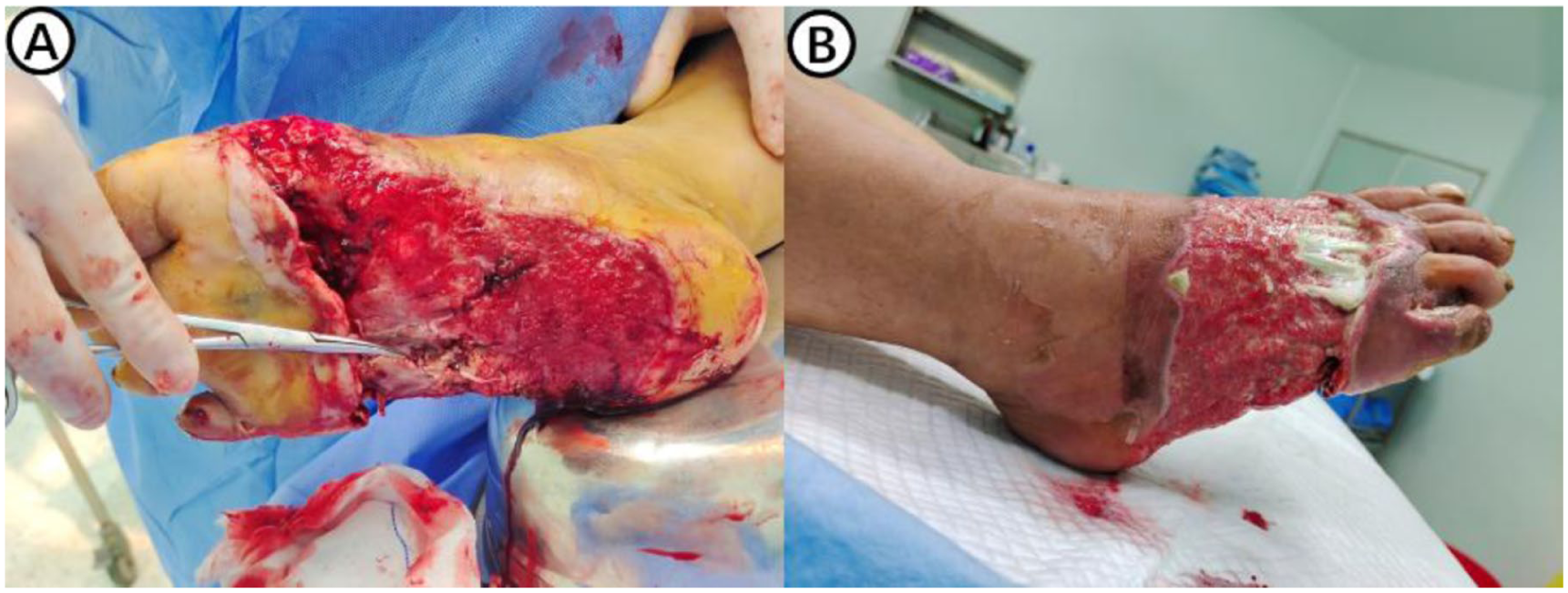
(a) Soft tissue defect in the sole of the foot begins proximally at the slightly distal side of the heel and extends distally to the heads of the metatarsal bones of each toe. (b) Soft tissue defect in the dorsum of the foot starts proximally at the tarsal bones and ends distally at the webbing between the toes.
After ruling out contraindications, the patient was given carbamazepine to treat the symptoms of gastrocnemius spasms. Intravenous infusion of 10% calcium gluconate solution was administered for fluid replacement therapy. And then, under general anesthesia, the patient underwent debridement and exploration of a wound on the right foot using NPWT. During the procedure, a tourniquet was applied at the root of the right thigh, and the wound was irrigated with normal saline, hydrogen peroxide, and povidone–iodine solution. The circular skin defect on the right foot was ~35 × 11 cm in size, with non-viable granulation tissue on the wound surface. Gastrocnemius spasms were observed at the metatarsal heads of the toes upon palpation with hemostatic forceps under general anesthesia. The spasms were suspected to be due to inflammatory tissue stimulating the nerves at the metatarsal heads. The treatment plan included thorough debridement to remove necrotic tissue and establish a fresh wound bed. Inflammatory changes in the tissue at the plantar metatarsal heads were addressed through incision and exploration, revealing purulent discharge, tissue necrosis, nerve degeneration, and partial bone destruction at the metatarsal heads. Thorough debridement was performed, and the transected nerve was mobilized proximally by ~1.5 cm, with the nerve sheath appearing intact and no evidence of post-degeneration sharp dissection. Upon palpation of the soft tissues of the sole of the foot, there was no reactive muscle spasm in the calf. A wound was observed on the inner side of the little toe, with poor blood supply and exposure of bone and tendon, which had undergone degeneration and was treated with wound debridement. The wound was repeatedly irrigated with normal saline, hydrogen peroxide, and chlorhexidine until clean, and the surgical incision was thoroughly hemostatic. The skin edges were sutured to reduce the wound size. Negative pressure sponge and sterile film were applied, along with irrigation and suction devices. Capillary refill time in the fingertip skin is <2 s. Several days later, the right foot wound was debrided and explored using NPWT. Following satisfactory granulation tissue growth, the right foot underwent debridement and skin grafting using NPWT. The patient recovered well postoperatively, with good healing of the skin graft on the right foot and resolution of gastrocnemius muscle spasms. After a follow-up examination 6 weeks later, the patient’s right foot showed good skin healing. Furthermore, there was slight tightness in the right gastrocnemius muscles tendon, with the resolution of tenderness in the walking area. Pain level: visual analog scale at level 2.
Discussion
Muscle spasms occur as sudden, involuntary, and painful contractions of skeletal muscles. 6 Spasticity is a movement disorder caused by upper motor neuron lesions, resulting in increased muscle tone, that is, velocity-dependent. It is commonly seen in upper motor neuron syndromes such as stroke, spinal cord injury, etc. Isolated gastrocnemius muscle spasms are usually unrelated to upper motor neuron lesions.7–9 The gastrocnemius muscle spasm in this case is a sudden, involuntary, and painful muscle contraction, classified as a muscle spasm rather than spasticity caused by upper motor neuron damage. Among the various types of skeletal muscle spasms, gastrocnemius spasms is a common occurrence, with causes and risk factors widely discussed, including nighttime leg cramps, hypocalcemic seizures, and epileptic seizures. 10 However, there is currently no literature on gastrocnemius spasms induced by foot soft tissue injuries. This article describes a case of a 46-year-old middle-aged man who developed gastrocnemius spasms in his right leg due to foot trauma for 20 days. X-rays showed no fractures or fractures in the foot. The skin on the calf gastrocnemius muscles was intact, with only soft tissue damage on the sole of the foot and part of the dorsum. The patient experienced unexplained spasms in the affected gastrocnemius muscles after the injury, and after multiple debridement surgeries combined with NPWT, the foot soft tissue injury healed and the gastrocnemius spasms resolved.
NPWT is a clinical adjunct therapy used to treat complex wounds or infections. Several domestic and international studies have demonstrated the significant benefits of NPWT in complex soft tissue wound management.10,11 For example: (1) timely drainage of wound exudate, necrotic tissue, and inflammatory factors reduces inflammation and nerve stimulation 12 ; (2) promotes angiogenesis and fibroblast proliferation, accelerates granulation tissue growth, shortens the preparation time for skin grafts/flaps 13 ; (3) isolates external bacteria in a closed environment, reduces infection risk, suitable for heavily contaminated foot soft tissue defects 14 ; (4) reduces tissue edema, improves local microcirculation and oxygen supply, facilitates peripheral nerve and soft tissue repair 15 ; and (5) reduces dressing changes, decreases wound mechanical damage and patient pain, suitable for patients with severe trauma and long treatment courses. 16
In a comparative study conducted by Lv, it was found that NPWT was significantly more effective in treating complex foot fractures with severe soft tissue injuries compared to traditional wound dressings. Not only did it shorten the wound healing time, but it also effectively sealed the wound, preventing bacterial infection. 17 Cibula et al. successfully cured a lower limb severe degloving injury patient with neurovascular damage using NPWT and performed successful surgical reconstruction. 18 Due to the severe soft tissue injuries and contamination in this patient, NPWT after surgical debridement can reduce the concentration of wound inflammation mediators and promote soft tissue reconstruction (Supplemental Material).
The gastrocnemius muscles is closely related to foot movements, as it is involved in ankle dorsiflexion, maintaining body balance, and protecting the sciatic nerve below it. Based on current research, the possible reasons for gastrocnemius spasms induced by soft tissue injury in the foot in this case may include: (1) Inflammatory mediators exudation: After trauma, the inflammatory response and tissue repair process may synthesize and release various inflammatory mediators such as proteases and cytokines, which may stimulate damaged neurons, leading to increased neuronal excitability and feedback; (2) Local distal nerve damage: After trauma, peripheral nerve function is disturbed or damaged, leading to muscle fatigue and spasms; (3) Water–electrolyte imbalance: During the postoperative recovery period, the balance of water and electrolytes in the body is disrupted due to trauma or surgical stress, leading to muscle spasms, especially ions such as sodium, potassium, and calcium play an important role in neuronal excitability; (4) Excessive stimulation of pain receptors: Pain receptors are overly active during the perioperative period due to pain, inflammation, or other factors, leading to abnormal neuronal excitation; and (5) Abnormal tendon reflex activity: Due to the lack of cushioning from the fat pad and soft tissues like muscles, the tendons in the foot are exposed, making them vulnerable to external factors that can induce abnormal tendon reflexes, specifically the ankle reflex.
The comprehensive treatment of debridement surgery combined with NPWT effectively relieved the symptoms of gastrocnemius spasms in the patient, while promoting good healing of the soft tissue wound. We speculate that NPWT alleviates gastrocnemius muscle spasms through various synergistic mechanisms: (1) eliminating neural stimuli by continuously draining inflammatory mediators, proteases, and metabolites to reduce abnormal nerve excitation and relieve reflex spasms; (2) reducing edema pressure by improving tissue edema and microcirculation, releasing nerve compression, and stabilizing nerve excitability; (3) clearing pathological stimuli by promoting clean wound healing, removing necrotic and infected tissues that continuously stimulate nerves and tendons, and blocking spasm triggers; and (4) enhancing perfusion and repair functions by promoting vascular and granulation tissue proliferation, optimizing blood supply and nutrition, restoring normal nerve–muscle conduction, and reducing abnormal spasms. Despite receiving appropriate electrolyte supplementation upon admission and being under general anesthesia to prevent pain stimuli, spasms of the gastrocnemius muscle continued to occur when stimulating the plantar wound. This rules out electrolyte imbalance or excessive stimulation of pain receptors as the sole causative factors. By utilizing NPWT, it is possible to effectively decrease the levels of inflammatory mediators in wound healing, which suggests that gastrocnemius spasms may be a result of the stimulation of damaged peripheral nerve endings and residual tendons by inflammatory mediators at the wound site. However, this finding is limited to a single case report, which may affect the overall credibility of the findings. Additionally, since the patient had already undergone initial debridement and NPWT treatment at another hospital, the specific debridement method used was not detailed, and there has been no systematic analysis of the composition and concentration of inflammatory mediators in the wound.
Footnotes
Ethical considerations
All protocols involving human subjects were approved by the Ethics Committee of the 960th Hospital of PLA (approval no. 202192).
Consent for publication
The patient has signed the consent form and kept a file for review.
Author contributions
A.W. and H.X. made substantial contributions to acquisition, analysis, and interpretation of data. H.X. and Z.J. were responsible for the conception and design of the study and the drafting and writing of this manuscript. All authors confirm the authenticity of all the raw data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data analyzed during this study are included in the manuscript. The datasets used in this article are available from the corresponding author (Z.J.) on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.