
Abstract
Although thrombotic events are common complications after cardiac arrest, the rapid formation of intracardiac thrombi is rarely directly observed. Here, we report a 57-year-old male who underwent laparoscopic bladder flap ureteral replacement surgery for a right ureteral fistula. During the surgery, indocyanine green was injected into the ureter, resulting in sudden respiratory and cardiac arrest. Immediate cardiopulmonary resuscitation was initiated, and transesophageal echocardiography revealed right atrial mass formation. After cardiopulmonary resuscitation, the patient’s vital signs remained stabilized. Repeat cardiac ultrasound demonstrated rapid mass resolution. The patient was successfully extubated in the intensive care unit and was subsequently discharged without complications. This case directly documents the rapid formation of intracardiac mass following cardiac arrest, highlighting the need to promptly rule out thrombotic events after successful resuscitation to enable timely management.
Introduction
Masses in the right atrium are relatively rare in clinical practice but may lead to severe complications. Differential diagnoses of right atrial mass include benign tumors, metastatic diseases, and thrombosis, which often present with similar imaging features, making a definitive diagnosis challenging.1,2
Clinical manifestations of a right atrial mass may include respiratory and cardiac arrest. Conversely, blood flow stasis during cardiac arrest may also contribute to thrombus formation in the right atrium. 3 Rapid assessment of intracardiac changes in patients with respiratory and cardiac arrest is critical for improving the prognosis.
Echocardiography is commonly used for initial evaluation of cardiac masses. However, limitations in imaging planes may prevent accurate assessment of the full extent and origin of the mass, and artifacts may lead to misinterpretation. 4
In this study, we report the rescue process and imaging findings of a patient with respiratory and cardiac arrest, documenting rapid thrombus formation in the right atrium following circulatory arrest and its rapid resolution after hemodynamic stabilization. The findings suggest that early screening for thrombotic events is essential after resuscitation.
Case
A 57-year-old man was diagnosed with rectal cancer at an external hospital 5 months prior to presentation. The tumor was located 3 cm above the anus and with lymph node metastasis but no distant metastasis. The patient has no other history of chronic diseases. After diagnosis, he underwent total rectal resection with colostomy. Postoperatively, a ureteral injury was identified, and he was referred to our hospital for ureteral repair.
The patient was admitted on May 10, 2025. Preoperative examinations, including electrocardiography and echocardiography, showed no significant abnormalities. Laboratory tests, including liver and kidney function and coagulation parameters, were within normal limits. No invasive procedures such as central venous catheterization had been performed prior to surgery.
On April 17, 2025, the patient underwent ureteral repair under general anesthesia with tracheal intubation. During the surgery, approximately 4 mL of indocyanine green (2.5 mg/mL) was injected into the ureter to identify the fistula. Suddenly, electrocardiogram monitoring showed cardiac arrest, and blood pressure became unmeasurable.
Indocyanine green injection was immediately stopped, and cardiopulmonary resuscitation (CPR) was performed. The patient received intravenous adrenaline (1 mg) and dexamethasone (5 mg). After approximately 3 min of resuscitation, spontaneous circulation returned, with a heart rate of 110 bpm and blood pressure of 140/70 mmHg.
During the resuscitation process, blood samples for hematological analysis, liver and kidney function, coagulation parameters were obtained. Intraoperative arterial blood gas analysis revealed metabolic acidosis, with a base excess of approximately −10 and partial pressure of oxygen of 72 mmHg, without carbon dioxide retention. Sodium bicarbonate was administered to correct acidosis.
Based on the clinical presentation, respiratory and cardiac arrest secondary to anaphylactic shock was considered; however, other possible causes needed to be excluded. Intraoperative transesophageal echocardiography revealed a mobile mass in the right atrium measuring approximately 4 cm. The mass was free within the atrial cavity and demonstrated marked mobility with tricuspid valve motion (Supplemental Video).
Given the patient’s unstable condition, the procedure was terminated, and the patient was transferred to the intensive care unit (ICU) for further treatment.
After transfer to the ICU, the patient remained intubated and received mechanical ventilation (pressure support 14 cm H2O; FiO2 60%). Repeat arterial blood gas analysis showed resolution of metabolic acidosis, with a partial pressure of oxygen of 326 mmHg and no carbon dioxide retention. Ventilator settings were gradually reduced. Laboratory reassessment revealed markedly elevated D-dimer and fibrin degradation product levels (99.27 and 325 µg/mL, respectively), whereas liver and kidney function and other coagulation parameters remained within normal limits.
Given the life-threatening condition of the patient, repeat bedside transthoracic echocardiography was performed and showed complete resolution of the right atrial mass (Figure 1). Pulmonary and cranial computed tomography angiography (CTA) were immediately performed to exclude pulmonary and cerebral embolism (Figures 2 and 3), with no significant abnormalities detected. Electrocardiogram was also unremarkable.

Postoperative sternal echocardiography and two-dimensional view of the apical four-chambered view of the heart showed no significant abnormalities in resting cardiac structure and systolic function. No mass was detected in the right atrium.
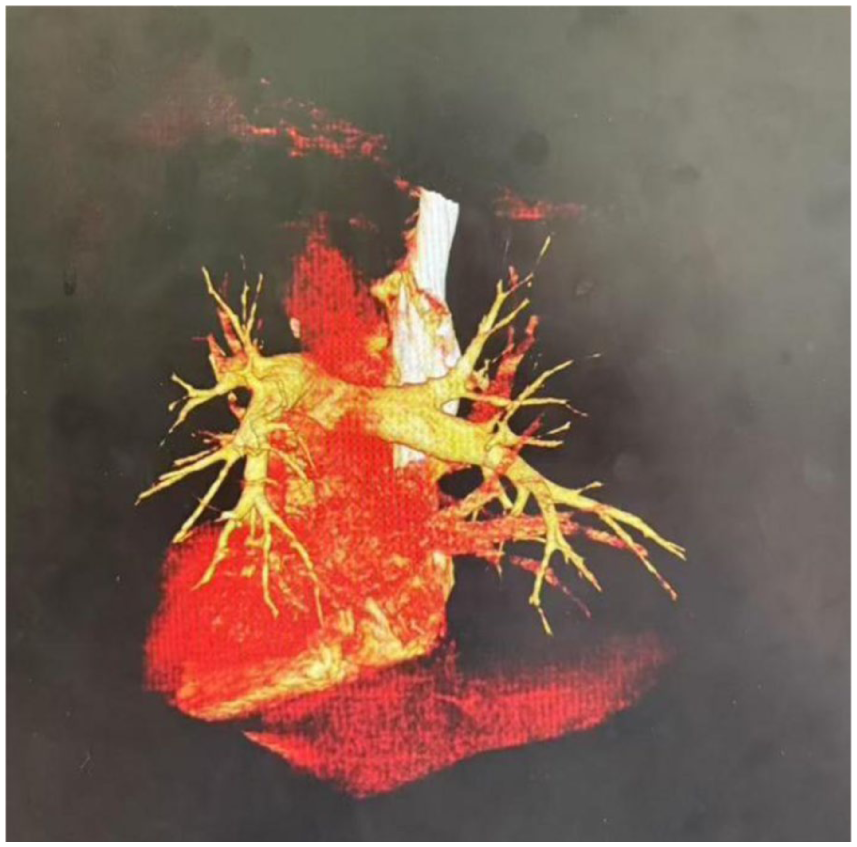
Pulmonary artery CTA performed after ICU admission showed no evidence of pulmonary artery embolism. Low-density shadows were observed in the middle and lower lobes of the right lung, without clear thromboembolic findings.
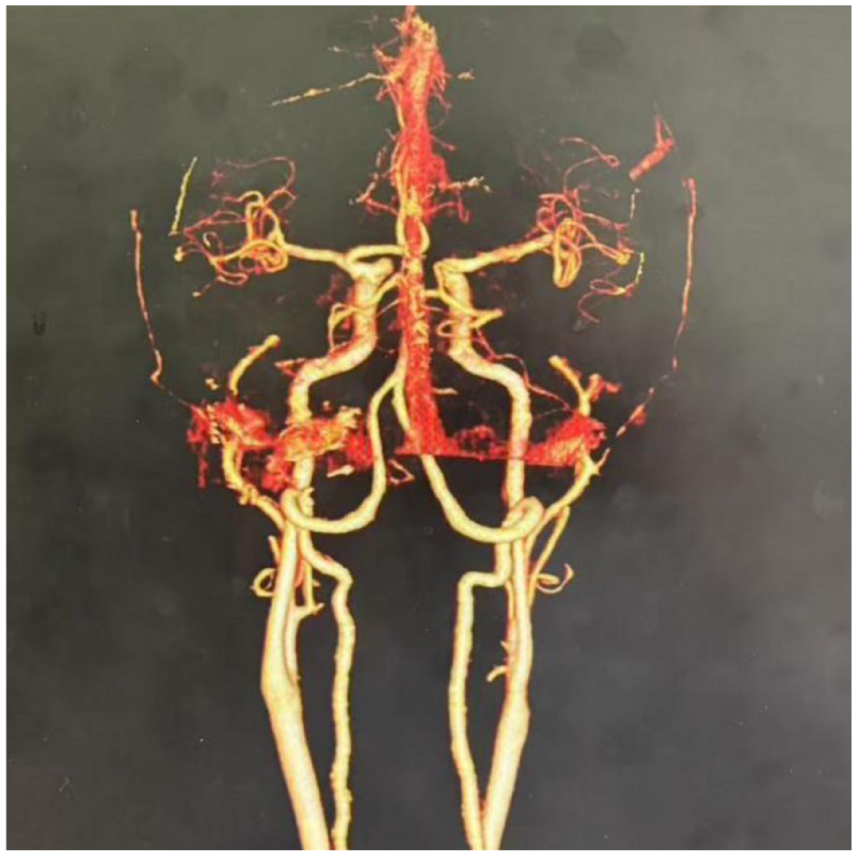
Intracranial CTA showed plaque formation at the origin of the right vertebral artery and in the A3 segment of the left middle cerebral artery, with moderate luminal stenosis and no evidence of thromboembolism.
Following monitoring and supportive care, the patient was successfully extubated on postoperative day 2. Post-extubation blood gas analysis was normal. D-dimer and fibrin degradation product levels decreased to 25.99 and 88.7 μg/mL, respectively. The patient remained hemodynamically stable and was transferred to the general ward without neurological deficits.
The patient was discharged on April 28, 2025. He was readmitted on May 16, 2025, for percutaneous nephrolithotomy and fistula repair, with a favorable outcome.
Discussion
A mass within the right atrial cavity observed on echocardiography may represent benign, malignant, or non-neoplastic etiologies, with mural thrombi being the most common, accounting for approximately 44% of the cases.5–8 Right atrial thrombosis is less common than left-sided thrombosis and is typically associated with blood stasis, endothelial injury, and hypercoagulability. 9
In this case, the patient developed anaphylactic shock following exposure to indocyanine green. Such a reaction has been reported in multiple cases, typically with successful CPR. 10 Although circulation was rapidly restored, transient blood flow stasis likely occurred.
The marked elevation in D-dimer and fibrin degradation products after ICU admission indicated a hypercoagulable state with active fibrinolysis, fulfilling the conditions for right atrial thrombus formation. Therefore, the right atrial mass is most consistent with an early thrombus that formed after respiratory and cardiac arrest.
No pulmonary or cerebral embolism events were observed, possibly due to the short duration of thrombus formation and its loose structure. After fibrinolysis, the fibrin components are completely dissolved and have no subsequent effects on other blood vessels.
Similar cases have been reported. In 2021, a patient experienced sudden circulatory collapse after tranexamic acid administration during surgery. Circulatory function was restored after CPR. However, echocardiography revealed extensive thrombus formation in the right atrium and ventricle. Subsequently, thrombolytic therapy was employed to dissolve the thrombus, which disappeared after echocardiography review. 11
Such pathological changes have also been reported in animal models. Budhram et al. found that in a Yorkshire pig model of cardiac arrest, 86.7% of animals developed intracardiac thrombosis 6 min after cardiac arrest, and 73.8% of these thrombi resolved within 2 min after CPR. 12
These findings suggest that, consistent with our clinical observations, right atrial thrombus formation may occur early after cardiac arrest and rapidly resolve following restoration of blood flow through chest compressions.
Further studies have shown that thrombotic events are also common following CPR, with an incidence rate of 23.5%, including venous thrombosis (11%) and arterial thromboembolism (15.5%). 13 Despite the widespread use of anticoagulant therapy, thrombotic complications continue to occur.
In this study, we observed rapid thrombosis formation following cardiac arrest, highlighting the need to reassess anticoagulation strategies in this clinical context.
Conclusion
Although the patient had a favorable outcome, the rapid formation of intracardiac thrombotic masses caused by blood flow stasis following cardiac arrest should not be overlooked.
Although current findings suggest that such thrombotic masses may resolve rapidly after blood flow restoration, prompt examinations with imaging modalities such as echocardiography and CTA should still be performed to assess for subsequent thromboembolic events and facilitate early treatment if needed.
Supplemental Material
Footnotes
Ethical considerations
Ethical approval was not required for this retrospective case report. All identifiable data were removed to protect privacy.
Consent to participate
Written informed consent was obtained from the patient.
Author contributions
Zhenghong Chen: conceptualization, data curation, writing – original draft. Qixuan Li: formal analysis, methodology, validation. Zhongzhao Yuan: formal analysis, methodology, validation. Tian Wang: formal analysis. Chengwei Yin: conceptualization, methodology, writing – review and editing. Peihua Geng: conceptualization, methodology.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Shanghai “13th Five-Year Plan” Clinical Key Specialty Construction Project (SHSLCZDZK04402).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
CARE compliance statement
This case report was prepared in accordance with the CARE (CAse REport) guidelines (![]() ) for transparent reporting of clinical case reports. The completed CARE checklist is provided as Supplemental Material. Particular attention was given to transparency in clinical presentation, diagnostic assessment, and outcome reporting.
) for transparent reporting of clinical case reports. The completed CARE checklist is provided as Supplemental Material. Particular attention was given to transparency in clinical presentation, diagnostic assessment, and outcome reporting.
Supplemental material
Supplemental material for this article is available online.