
Abstract
Hidradenitis suppurativa is typically found in intertriginous areas such as the axillae and groin. As incidence rates rise, however, hidradenitis suppurativa is increasingly identified in unexpected locations. As this phenomenon has been underreported, these patients experience diagnostic delays and inappropriate or inadequate treatment. This case involves a man in his 60s who presented with an inflamed earlobe that had waxed and waned without diagnosis or treatment for many years. Recognition of the signs and symptoms of hidradenitis suppurativa led to diagnosis, effective therapy, and improved quality of life; however, due to diagnostic delay related to the atypical location, tunneling and scarring had already developed. This case highlights auricular and periauricular hidradenitis suppurativa to promote earlier recognition and timely intervention to limit progression of this highly morbid disease.
Keywords
Introduction
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disorder characterized by follicular occlusion that often begins with acneiform lesions followed by painful nodules and malodorous draining abscesses. As the disease progresses, sinus tracts and fibrotic scars form. Sites of increased skin and clothing friction such as the axillae, inframammary folds, inguinal creases, inner thighs, and gluteal region are commonly affected. 1
The global prevalence of HS has been estimated to be as high as 4.1% with typical onset in young adulthood. 2 HS imposes a significantly negative impact on quality of life and is associated with increased risk of suicide. 2 Thus, clinicians should maintain a high index of suspicion when HS signs and symptoms occur in nontraditional locations including the face, neck, chest, abdomen, back, and feet.3,4 Failure to recognize HS outside its classic distribution may result in delayed diagnosis, leading to increased morbidity and mortality.
Case
A man in his 60s presented for a routine skin examination during which his right earlobe was found to have a pitted appearance with mildly erythematous induration. When queried about these findings, the patient reported itchy, burning, swollen lesions with intermittent bleeding that waxed and waned in that area for nearly 30 years, and around the left ear for the last 6 years which he reported to several clinicians without receiving a diagnosis.
As the patient had become accustomed to the condition, he was not motivated to submit to a biopsy at that time, but empiric treatment was initiated. Given the erythematous, edematous appearance upon initial presentation, pseudolymphoma and granuloma faciale were among the differential diagnoses and treatment was directed toward reducing inflammation and pruritus with 0.2 ml of triamcinolone 5 mg/ml administered intralesionally.
When the patient returned the following month, he reported partial improvement following the injection and application of previously prescribed desonide 0.05% topical cream, so the concentration of intralesional triamcinolone was increased to 10 mg/ml and the patient was advised to continue desonide twice a day as needed.
At the subsequent visit a month later, the patient reported exacerbation with new crusted pustular lesions in the right postauricular crease and bilateral preauricular regions. While a severe acne flare or furunculosis may have been considered, the pits that previously appeared to be scars were producing purulent drainage consistent with sinus tracts, leading to a presumptive diagnosis of HS and a shift toward antimicrobial treatment with sulfacetamide/sulfur 10%/5% wash, clindamycin 1% lotion, and doxycycline 100 mg twice a day. The patient was also advised to taper the desonide as pruritus improved.
At follow-up, his symptoms were well controlled. He was advised to continue the topicals as maintenance and take the doxycycline only as needed for flares.
The patient presented 1 year later for annual skin cancer surveillance and reported continued control with weekly application of clindamycin lotion. The cleanser was changed to benzoyl peroxide 4% wash for cost savings. The following year the condition remained controlled on topical therapy alone.
However, the patient returned 3 months later reporting exacerbation coinciding with increased stress. He admitted to applying the clindamycin twice a day without an antimicrobial cleanser. An extended course of doxycycline was prescribed, and the patient was advised to restart the benzoyl peroxide wash daily.
When he followed up 6 months later, his stress level remained high and the disease was uncontrolled. A punch biopsy was performed, and the histology showed dense mixed inflammatory cell infiltrate in the dermis with abscess formation, marked fibrosis, and cellular debris, and significant inflammation and destruction of pilosebaceous follicles and apocrine and eccrine glands.
As these findings are consistent with HS, a mutual decision was made to escalate treatment with the dual IL-17A and IL-17F inhibitor bimekizumab 320 mg subcutaneously every 2 weeks through week 16 then 320 mg every 4 weeks thereafter. Since initiating biologic therapy in March 2025, the patient has reported significantly reduced disease activity without adverse effects.
Discussion
A PubMed search returned seven previously reported cases of auricular or periauricular HS. The first, published in 2005 in MedGenMed, described a 38-year-old man with a 20-year history of HS in the axillae, hip, scrotum, perineum, and inguinal regions with inactive lesions behind the ears and periumbilical region. 5 In 2006, the Archives of Dermatology published a case involving a 67-year-old who also had a 20-year history of HS involving the ears, axillae, buttocks, and groin. 6 The same journal published a case series in 2011 that included a 49-year-old woman with bilateral postauricular HS. 7 Two cases were published in 2012, one in the Dermatology Online Journal regarding a man who had HS in both earlobes and the periauricular region since puberty that went undiagnosed until age 28. 8 The other, published in the Indian Journal of Dermatology, involved a 30-year-old man with preauricular HS that had been misdiagnosed for 2 years. 9 In 2020, JAAD Case Reports published the case of a 12-year-old boy with Trisomy 13 and HS in the periauricular region in addition to several classic sites. 10 Finally, in 2023, the Archives of Craniofacial Surgery described the excision and reconstruction of bilateral postauricular HS in a 32-year-old man following a 5-year diagnostic delay. 11
With limited reporting of auricular and periauricular HS, clinicians may be inadequately prepared to identify HS in atypical locations, resulting in misdiagnosis and treatment delays. Moreover, underreporting perpetuates the conceptualization of nonintertriginous HS cases as isolated “ectopic” medical curiosities rather than statistically validated manifestations of a heterogeneous disease, as proposed in 2013 by Canoui-Poitrine et al., whose HS classification model recognized ear, neck, chest, and leg involvement as part of a follicular phenotype along with axillary-mammary and gluteal phenotypes. 12
While only a small number of peer-reviewed cases of auricular or periauricular HS have been published over the past two decades, patients’ anecdotal accounts describing signs and symptoms consistent with HS in these areas appear regularly in public forums such as Reddit, Inspire, and Quora, online support groups such as myHSteam, Patient.Info, and Pilonidal Support Alliance, and social media platforms such as Facebook, suggesting that rates of auricular and periauricular involvement are higher than depicted in the literature.
Conclusion
Cases such as this and others with diagnostic delays indicate that HS in atypical sites continues to go underrecognized in clinical practice, and should prompt clinicians to adopt a wider distribution model for HS. Identifying this increasingly common condition in nonintertriginous locations will improve quality of care through timely implementation of appropriate therapy, which may be especially important for head and neck HS as heightened visibility may increase patient distress (Figures 1 and 2).

HS lesions in the right ear lobe, preauricular region, and neck.
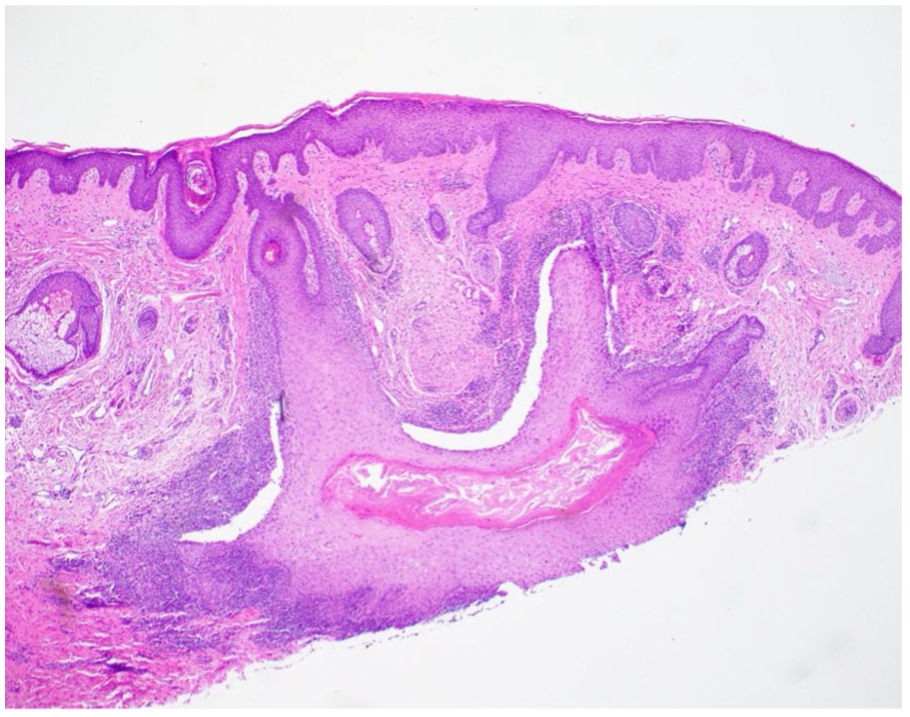
Histology of an inflamed follicle.
Footnotes
Consent for publication
Written informed consent for publication of this report and accompanying images was provided by the participant.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Seiter serves on UCB’s speakers’ bureau for bimekizumab (Bimzelx).
Claire Fortman declared no potential conflicts of interest with respect to the authorship and/or publication of this article.