
Abstract
Complete fused renal ectopia, also known as pancake kidney, is a rare congenital renal fusion anomaly characterized by complete fusion of both kidneys within the pelvis. Most patients remain asymptomatic and diagnosis is often incidental. I report a 49-year-old woman from a low-resource setting who presented with lower urinary tract symptoms and dyspareunia. Initial management was directed toward recurrent cystitis; however, further evaluation with computed tomography and intravenous urography revealed a pancake kidney located in the pelvis with two distinct collecting systems and normally draining ureters. No evidence of obstructive uropathy, renal mass lesion, or associated complications was identified. This case highlights the diagnostic challenge posed by nonspecific clinical presentation and limited access to advanced imaging in low-resource settings, which may contribute to delayed or incidental diagnosis of congenital renal anomalies.
Keywords
Introduction
Congenital anomalies of the kidney and urinary tract comprise a heterogeneous group of developmental disorders arising from abnormalities in the embryological interaction between the ureteric bud and metanephric blastema. These anomalies may remain clinically silent for many years and are often discovered incidentally during imaging performed for unrelated conditions. 1
Pancake kidney, also known as cake kidney, disc kidney, or complete fused pelvic renal ectopia, is one of the rarest renal fusion anomalies. It is characterized by complete fusion of both kidneys into a single lobulated renal mass, usually located within the pelvis. Despite complete parenchymal fusion, two separate collecting systems are typically present, and the ureters usually remain uncrossed with normal insertion into the urinary bladder.2–4
Most patients with pancake kidney are asymptomatic; however, some may present with lower urinary tract symptoms (LUTSs), recurrent urinary tract infections, nephrolithiasis, hydronephrosis, or nonspecific abdominal and pelvic pain related to abnormal renal position and urinary drainage. 2 Adult diagnosis is not uncommon because many cases remain undetected until imaging is performed for evaluation of persistent symptoms or unrelated conditions.3,4
In low-resource settings, ultrasonography is frequently the initial imaging modality because of its availability, affordability, and lack of ionizing radiation. However, complex renal fusion anomalies may be misclassified on ultrasound, particularly when the kidneys are ectopically located within the pelvis. Cross-sectional imaging with computed tomography (CT) urography provides superior anatomical delineation of the renal parenchyma, collecting systems, ureters, and associated abnormalities, facilitating accurate diagnosis and management planning.4,5
I report a case of pancake kidney diagnosed in a 49-year-old woman presenting with LUTSs in a low-resource setting. This case highlights the diagnostic challenges associated with rare congenital renal fusion anomalies and underscores the value of CT urography in establishing the correct diagnosis when initial ultrasonographic findings are inconclusive.
Case presentation
Clinical presentation
A 49-year-old female presented to the urology clinic with a 1-year history of urinary frequency associated with other LUTSs. One month prior to presentation, she developed intermittent lower abdominal pain and dysuria. She also reported painful coitus (dyspareunia). There was no history of hematuria, abnormal per-vaginal bleeding, fever, weight loss, or other constitutional symptoms. The patient had regular menstrual cycles and was married. Obstetric history was gravida 4, para 4 (P4L4), with no history of obstetric complications relevant to the current presentation.
Her past medical history revealed no known chronic kidney disease, diabetes mellitus, or hypertension. She had no prior history of urological surgery or known congenital abnormalities. The patient reported having received multiple courses of antibiotics for presumed urinary tract infections at primary healthcare facilities prior to referral. However, details regarding the specific antibiotics, treatment duration, and microbiological investigations were unavailable, and the patient was unable to provide treatment records or recall the medications used.
On clinical examination, the patient was hemodynamically stable. Abdominal examination revealed no palpable masses, no tenderness, and no organomegaly. Pelvic gynecological examination was performed and was unremarkable, with no evidence of pelvic mass, cervical abnormality, adnexal tenderness, or abnormal vaginal bleeding. A urine pregnancy test was performed and was negative.
Initial clinical impression included uncomplicated cystitis versus overactive bladder syndrome. She was managed symptomatically and investigated further.
Laboratory investigations
The laboratory findings demonstrated mild pyuria without microbiological confirmation of urinary tract infection. Urine culture showed no bacterial growth, and the vaginal swab was negative for significant pathogens. Hematologic parameters were within normal limits, and renal function was preserved (Table 1).
Laboratory investigations at presentation.
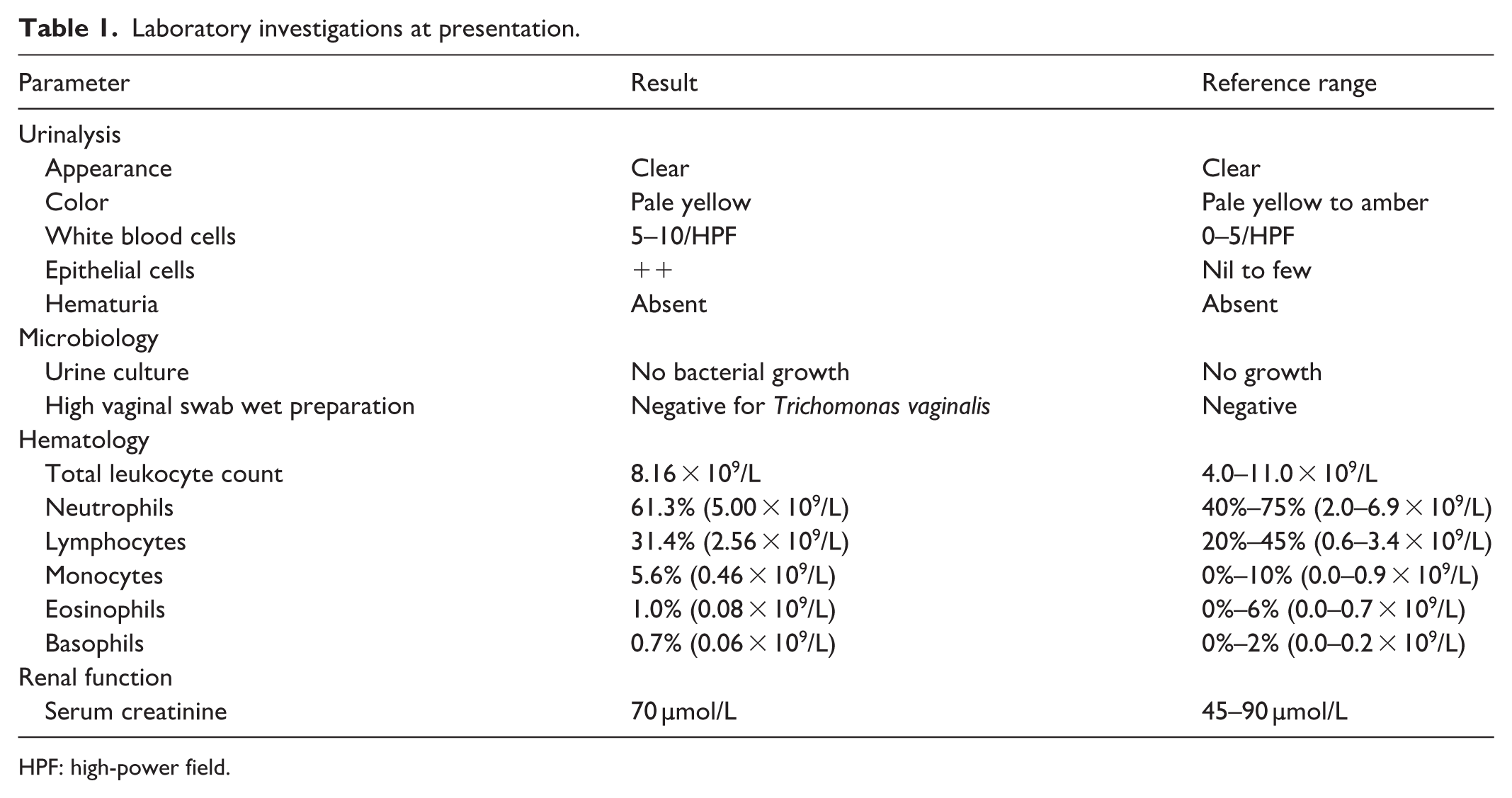
HPF: high-power field.
Imaging findings
Initial Ultrasound Evaluation
Kidney–ureter–bladder (KUB) ultrasound was performed as the initial imaging investigation. Ultrasound demonstrated empty right and left renal fossae. A renal structure with preserved corticomedullary differentiation was identified within the pelvis. The urinary bladder was well distended with smooth walls and no intravesical mass lesion.
The initial sonographic impression was right renal ectopia with possible left renal agenesis. CT intravenous urography was subsequently requested for further anatomical characterization and evaluation of the genitourinary tract.
CT intravenous urography demonstrated the absence of both kidneys within the expected renal fossae, with no renal tissue identified in the upper retroperitoneum. Instead, a single fused renal mass was visualized in the midline of the pelvis, located posterior to the uterus (Figures 1 and 2).
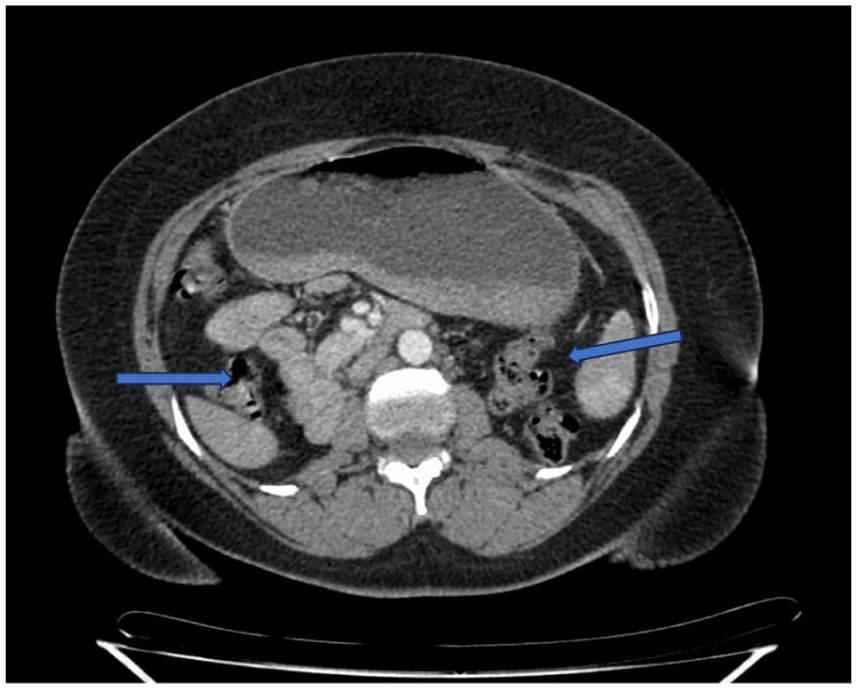
Axial contrast-enhanced CT image demonstrating absence of both kidneys from the renal fossae (blue arrows).

Coronal CT urography image showing a fused pelvic renal mass with preserved corticomedullary (white arrow).
The fused renal unit showed asymmetric configuration with fusion of the renal moieties at the mid and lower poles. The renal parenchyma demonstrated preserved corticomedullary differentiation, with no focal cortical scarring, mass lesion, or calcification identified.
Two distinct ureters were seen originating from the fused renal mass (Figure 3). Both ureters exhibited mild tortuosity along their course but without evidence of dilatation, obstruction, or delayed excretion. The ureters followed a normal anatomical course and inserted separately and appropriately into the urinary bladder.
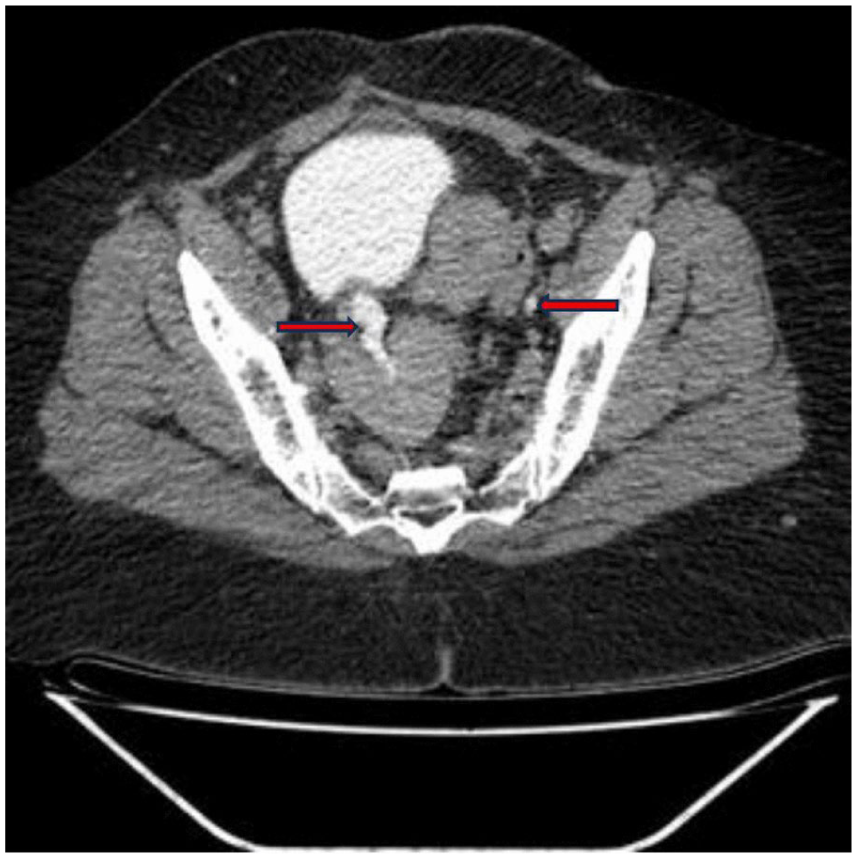
Excretory-phase CT urography demonstrating two ureters arising from the fused pelvic renal unit and draining separately into the urinary bladder without evidence of obstruction or delayed excretion (red arrows).
There was no evidence of hydronephrosis, obstructive uropathy, or perinephric collection. The urinary bladder appeared normal in outline and wall thickness, with no intraluminal mass lesion or filling defect. Adjacent pelvic organs, including the uterus and adnexa, showed no associated abnormality.
Final diagnosis and differential diagnoses
The differential diagnosis included crossed fused renal ectopia, horseshoe kidney, and solitary pelvic kidney. Crossed fused renal ectopia was excluded because no renal moiety or ureter was seen crossing the midline, and both collecting systems remained within a single completely fused pelvic renal mass. Horseshoe kidney was considered unlikely because the kidneys were not located in their normal retroperitoneal position and there was no identifiable isthmus connecting two separate renal units. Solitary pelvic kidney with contralateral renal agenesis was excluded by the demonstration of two distinct collecting systems and two ureters arising from the fused renal mass. The presence of a single midline pelvic renal mass with complete parenchymal fusion, preserved bilateral collecting systems, and separate ureteric drainage was most consistent with pancake kidney (complete fused pelvic renal ectopia).
Management and outcome
The patient was initially managed as uncomplicated cystitis with empirical nitrofurantoin for 14 days, alongside symptomatic treatment for LUTSs. Additional investigations, including urine culture and swab studies, were requested while awaiting imaging.
CT intravenous urography later confirmed pancake kidney with no obstructive uropathy or mass lesion, shifting management to conservative urological care. No surgical intervention was required.
At 1-month follow-up, the patient reported significant improvement in urinary symptoms with resolution of dysuria and dyspareunia. Residual urinary frequency was less severe than at presentation. Renal function remained normal (creatinine 70 µmol/L).
The patient was counseled regarding the congenital nature of the anomaly and reassured that no surgical intervention was required in the absence of obstruction, nephrolithiasis, or renal impairment. She was advised regarding the possibility of recurrent urinary symptoms and the need for periodic clinical follow-up to monitor renal function and potential future complications.
Discussion
Pancake kidney, also known as complete fused pelvic renal ectopia, is one of the rarest congenital renal fusion anomalies. It results from abnormal fusion of both metanephric blastemas during early embryogenesis, accompanied by failure of normal renal ascent, leading to the formation of a single fused renal mass within the pelvis.1,2 Unlike crossed fused renal ectopia, pancake kidney is characterized by complete fusion of both kidneys without crossing of a renal moiety or ureter across the midline.2,4
Most individuals with pancake kidney remain asymptomatic and are diagnosed incidentally during imaging performed for unrelated conditions.2,3 However, reported clinical manifestations include LUTSs, recurrent urinary tract infections, nephrolithiasis, hydronephrosis, abdominal pain, and pelvic discomfort resulting from abnormal renal position or impaired urinary drainage. 2 In the present case, the patient presented with a one-year history of urinary frequency, LUTSs, and lower abdominal discomfort. Although she had previously received treatment for presumed urinary tract infections, urine culture obtained during the current evaluation demonstrated no bacterial growth. Therefore, a direct causal relationship between the congenital anomaly and recurrent infection could not be conclusively established.
Diagnosis of pancake kidney may be challenging, particularly in low-resource settings where ultrasonography is often the primary imaging modality. In our patient, initial KUB ultrasonography demonstrated empty renal fossae and a pelvic renal structure, resulting in a provisional diagnosis of right renal ectopia with possible left renal agenesis. Although ultrasonography is widely available and free from ionizing radiation, it may have limited ability to accurately characterize complex renal fusion anomalies and associated collecting systems. 6 CT intravenous urography was subsequently performed because of persistent LUTSs and inconclusive sonographic findings. CT urography provided detailed anatomical characterization, demonstrating a completely fused pelvic renal mass with two distinct collecting systems and normally draining ureters, thereby establishing the correct diagnosis.
Several adult cases of pancake kidney have been reported in the literature. Tiwari et al. 2 described an incidental diagnosis in an adult patient during evaluation for abdominal symptoms, while Lomoro et al. 3 reported a radiologically confirmed case initially mistaken for another pelvic pathology. Similar to these reports, our patient remained undiagnosed until adulthood despite longstanding symptoms. However, unlike many published cases, the diagnosis in our patient was established in a low-resource setting following an initial sonographic misclassification, highlighting the diagnostic challenges encountered in such environments.
The differential diagnosis included crossed fused renal ectopia, horseshoe kidney, and solitary pelvic kidney. Crossed fused renal ectopia was excluded because no renal moiety or ureter crossed the midline. Horseshoe kidney was excluded because both kidneys were not located in their usual retroperitoneal position and there was no connecting isthmus between normally situated renal units. Solitary pelvic kidney was excluded by the presence of two distinct collecting systems and two ureters arising from the fused renal mass.4,7
Recognition of pancake kidney is clinically important because affected individuals may develop complications including urinary tract obstruction, nephrolithiasis, recurrent infection, and difficulties during abdominal or pelvic surgery due to anomalous vascular anatomy. Accurate preoperative identification is therefore essential to avoid inadvertent injury during surgical or interventional procedures.
This case highlights the importance of considering congenital renal fusion anomalies in adults presenting with persistent LUTSs, particularly when symptoms are unexplained or imaging findings are atypical. It also underscores the complementary role of CT urography in accurately characterizing complex urinary tract anomalies when ultrasound findings are inconclusive.
Conclusion
Pancake kidney (completely fused pelvic renal ectopia) is an exceptionally rare congenital renal fusion anomaly that may remain undiagnosed until adulthood. Its clinical presentation can be nonspecific, including LUTSs and pelvic discomfort, which may lead to delayed recognition and misdiagnosis. This case highlights the limitations of ultrasonography in characterizing complex renal fusion anomalies and demonstrates the value of CT urography in establishing an accurate diagnosis. Increased awareness of such rare congenital anomalies is important, particularly in low-resource settings, to facilitate appropriate evaluation, avoid diagnostic delays, and guide long-term clinical management.
Patient perspective
The patient reported that she had experienced bothersome urinary symptoms for approximately 1 year before the definitive diagnosis was made. These symptoms affected her daily comfort and caused concern due to repeated visits to different health facilities with only temporary improvement after treatment. She expressed relief after the final diagnosis was explained, particularly after being reassured that the condition was congenital and not malignant. The patient appreciated understanding the cause of her symptoms and reported improved confidence in her ongoing follow-up care.
Take-home points
Pancake kidney (completely fused pelvic renal ectopia) is an extremely rare congenital renal fusion anomaly that may remain undiagnosed until adulthood.
Clinical presentation is often nonspecific and may include LUTSs, recurrent urinary infections, or pelvic discomfort.
Ultrasonography may be limited in characterizing complex pelvic renal anomalies, leading to diagnostic uncertainty in low-resource settings.
CT intravenous urography provides definitive anatomical delineation of renal fusion anomalies, including collecting systems and ureteric drainage patterns.
Awareness of rare congenital renal anomalies is important to prevent delayed diagnosis and inappropriate management of urinary symptoms.
Footnotes
Acknowledgements
The author would like to acknowledge the management and staff of Mbeya Zonal Referral Hospital for their support in the diagnosis and multidisciplinary management of the patient included in this case report.
Consent to participate
Written informed consent was obtained from the patient included in this case report for publication of her clinical information and accompanying imaging. The patient was informed that all identifying details would be anonymized, and that the data would be used solely for academic and scientific publication purposes. Consent was obtained prior to submission of the article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.