
Abstract
Lophomoniasis is a new emerging parasitic disease caused by Lophomonas spp., a protozoan that predominantly resides in a commensal relationship within the hindgut of cockroaches. This pathogen is known to affect the lower respiratory tract in humans, resulting in clinical manifestations such as cough, sputum production, and shortness of breath. We present two case studies involving a 54-year-old- and a 38-year-old male, both with a history of cigarette smoking but no known underlying medical conditions. These individuals presented at the emergency room with respiratory symptoms and were subsequently evaluated. No significant abnormalities were shown on the lung computed tomography scan in Case 1, whereas empyema was observed in the right lung in Case 2. Analysis of bronchoalveolar lavage fluid from each patient revealed Lophomonas spp., an emerging protozoan pathogen, by microscopic examination. Based on these findings, metronidazole was administered to both patients, resulting in successful treatment of the infection. These cases highlight that Lophomonas spp. is a significant respiratory pathogen capable of causing a spectrum of disease in immunocompetent individuals, from mild bronchitis to severe pneumonia with complications. They emphasize the critical importance of including lophomoniasis in the differential diagnosis for persistent or atypical respiratory infections. Timely treatment with metronidazole was effective, resulting in clinical resolution.
Introduction
Lophomonas is an extracellular flagellated protozoan that has recently emerged as an infectious agent capable of colonizing the human respiratory tract, particularly the lower respiratory tract. Interestingly, this pathogen is commonly found in a commensal relationship with the lower intestines of cockroaches and termites, highlighting its potential for zoonotic transmission and raising concerns about its spread within human populations.1,2 In recent decades, reports of respiratory infections caused by Lophomonas have emerged in various regions of the world, particularly in China and Iran, where the latter has the highest number of documented cases globally. 3 Patients with Lophomonas infections typically present with a range of respiratory symptoms, including chronic cough, sputum production, and shortness of breath. 4 Of note, Lophomonas spp. has recently been identified in cockroaches from Mazandaran province in northern Iran, highlighting the potential for transmission of this parasitic infection in this region. 2 Although co-infections involving Lophomonas and other infectious diseases have been reported sporadically worldwide, the literature on this topic remains limited. Previous studies have suggested a potential link between Lophomonas infections and other infections, such as HIV and tuberculosis.5,6 While Lophomonas appears to be the cause of significant acute lower respiratory infection in immunocompetent patients,7,8 it has been mostly reported as an opportunistic infection in patients with impaired immune status. 9 Clinical presentation, laboratory findings, and radiologic features of Lophomonas spp., lower tract infections are nonspecific and cannot be readily differentiated from lung infections caused by common pathogens. 4 Diagnosis may be established by the identification of protozoa in tracheal aspirates or bronchoalveolar samples through direct microscopy in the presence of clinical and radiologic signs of bronchitis or pneumonia.4,9 Moreover, one of the diagnostic challenges is the morphological similarity between Lophomonas and ciliated epithelial cells, which can lead to misidentification. 3 The two can be distinguished based on differences in shape, the presence of flagella versus cilia, and nuclear characteristics. 4
Recently, a method for diagnostic confirmation by molecular diagnosis, multiplex-PCR, has been developed by a research team at the Iranian National Registry Centre for Lophomoniasis (INRCL) at Imam Khomeini Hospital, Mazandaran University of Medical Sciences, Sari, Iran, and is now available. 10 This case study reports the diagnosis and treatment of two immunocompetent patients from northern Iran who were infected with Lophomonas and presented with various respiratory symptoms.
Case presentation
Case 1
On November 21, 2024, a 54-year-old male with no history of pre-existing medical conditions and a 15-year history of smoking (known as slight smokers; fewer than 10 cigarettes/day) presented to the emergency room with a 2-day history of coughing and bloody sputum. Upon arrival at the emergency room, the patient’s vital signs were within normal limits, with no fever or shortness of breath reported. Notably, the patient’s oxygen saturation was 96%. Subsequent laboratory tests and a lung computed tomography (CT) scan revealed no significant abnormalities (Figure 1), while the sputum culture identified no pathogen. Upon conducting a fiberoptic bronchoscopy (FOB), minimal secretions were identified within the right and left bronchi. A bronchoalveolar lavage (BAL) specimen was obtained; approximately 10 mL of the BAL fluid (BALF) was collected in a sterile container under ambient conditions and transported to the INRCL within 1–2 h for cytological analysis, smear preparation, and various cultures including acid-fast bacilli, fungi, and Lophomonas parasites in order to rule out lophomoniasis. While the cytology specimens and cultures for acid-fast bacillus and fungus were negative, numerous viable and pleomorphic multiflagellated, Lophomonas was observed on wet mount smears using light microscopy at 10× and 40× magnification. Additionally, to assess the severity of the infection, the density of Lophomonas was also calculated using a light microscope. By evaluating parasite density per high-power microscopic field (HPF; ×400) as developed by Fakhar et al., 5 an inventive severity index for Lophomonas infection was classified into mild to severe parasite density. Mild density was classified as 1–10 parasites/100 HPF, moderate density as 1–10 parasites/10 HPF, and severe density as 1–10 parasites/HPF. Accordingly, the infection severity was classified based on parasite density, ranging from mild to severe. Given the positive Lophomonas smear and mild infection density, the patient was treated on a course of metronidazole at a dosage of 500 mg three times daily (TDS) for a period of 2 weeks. Following this treatment regimen, the patient reported significant improvement in their respiratory symptoms and was discharged from the hospital in stable, good general condition. In our patient’s BALF sample, Lophomonas was the only identified cause of lung infection and respiratory failure since hospital admission. This leads us to believe that these protozoa also have the potential to cause an infectious process severe enough to warrant emergency department admission.
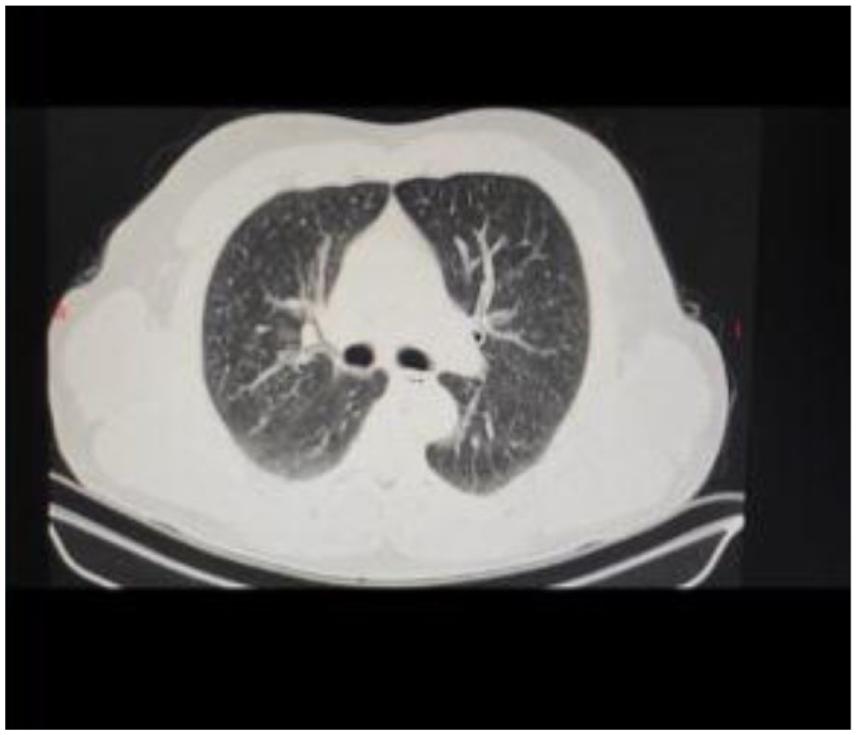
A lung CT scan from an immunocompetent patient with Lophomonas infection, showing no abnormal findings.
Case 2
On September 7, 2024, a 38-year-old man with a slight smoking habit was admitted to the emergency room without any underlying or comorbid conditions due to shortness of breath and fever, which had been preceded by a common cold a month prior to admission. During a physical examination, decreased breath sounds were noted at the lung bases, and the patient’s functional class III shortness of breath was identified. The patient’s oxygen saturation was 86% on room air and 96% with nasal oxygen administration. A CT scan of the patient’s lungs revealed evidence of pneumonia and empyema in the right hemithorax with loss of right lung volume (Figure 2). Following consultation with the infectious diseases service, a course of vancomycin 1 g twice daily and tazosin 4.5 g TDS was initiated. Under the guidance of ultrasound, a thoracoentesis (pleural tap) was performed, and the collected pleural fluid was analyzed. The analysis of the pleural fluid revealed blood and a substantial white blood cell count (14,800), with 90% polymorphonuclear cells and 10% lymphocytes, 15,000 red blood cells, and an elevated adenosine deaminase level at 107.7 U/L. All other laboratory tests were within normal limits, with the exception of an elevated erythrocyte sedimentation rate at 92, C-reactive protein at 41, blood urea nitrogen at 20, and creatinine at 1.3. To drain the purulent fluid from the pleural space, a chest tube was inserted on the right side of the chest, and a significant volume of fluid was drained. For further workup, a FOB was performed, revealing the presence of purulent secretions. BALF specimens were collected for cytological analysis and examination for acid-fast bacilli, fungi, and Lophomonas. The pleural fluid examination was negative for Lophomonas infection, whereas the BALF cytology was positive for Lophomonas. In addition to the previously administered antibiotics, the patient was prescribed a course of metronidazole, at a dosage of 500 mg TDS for 2 weeks. After completing the treatment regimen and demonstrating significant improvement in respiratory symptoms, the patient was discharged from the hospital in stable, good general condition. However, due to persistent cough and tracheal secretions, a mini-BAL procedure, a less invasive, safe, and quick approach, was performed using a sterile suction catheter of size 12 French. About 20 mL of 0.9% sodium chloride was instilled through the catheter, and the aspirate was collected in a sterile polypropylene tube by suction. After that, based on the microscopic and the specific PCR techniques described below, we confirmed lophomoniasis (Table 1). Genomic DNA was extracted from BALF samples and an in-house conventional PCR assay was conducted as described in our previous work (10).
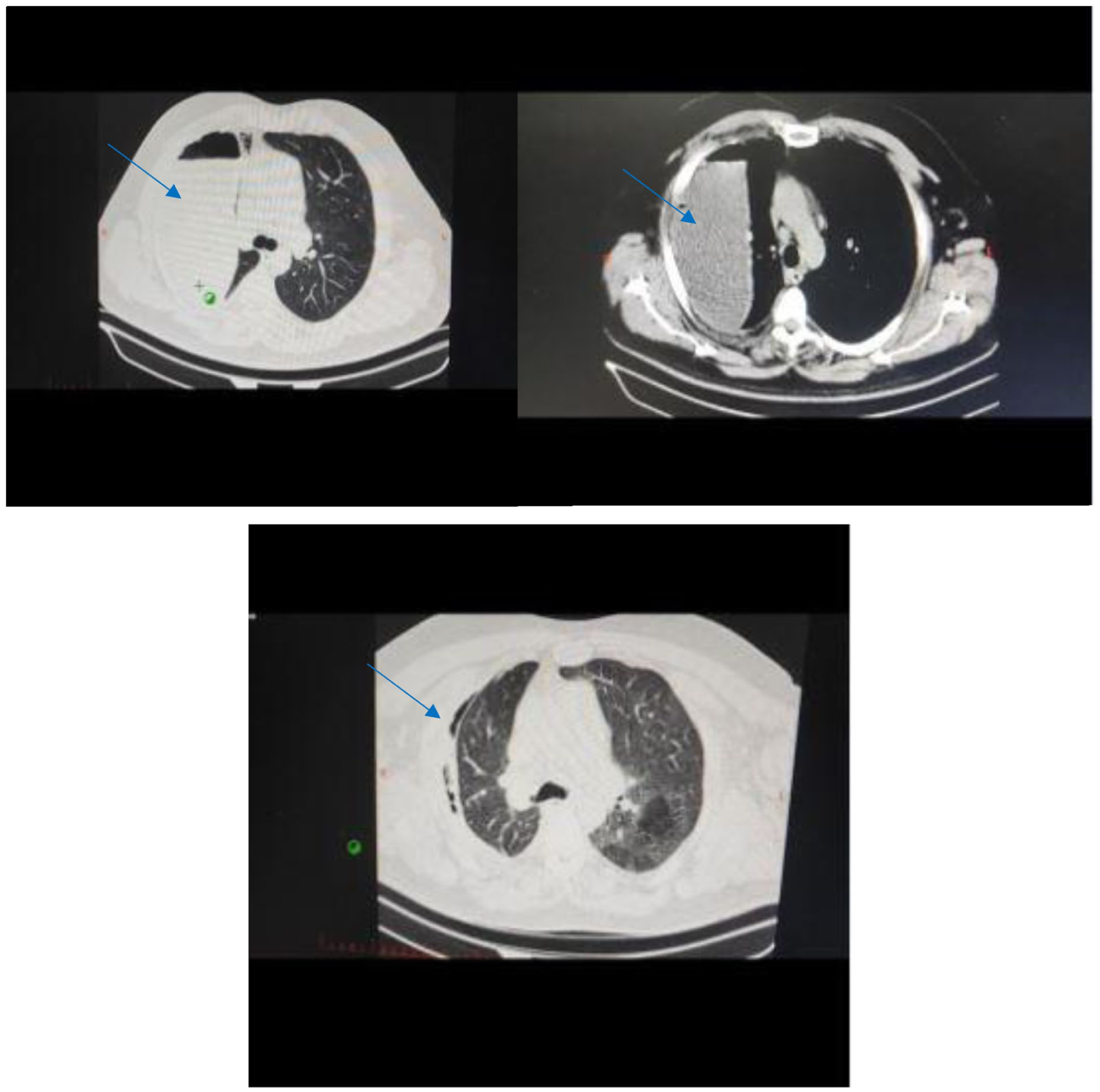
A lung CT scan from an immunocompetent patient with Lophomonas infection, showing empyema (blue arrowhead) in the right hemithorax with loss of right lung volume.
Characteristics of two immunocompetent patients with lophomoniasis.

TDS: three times daily.
Thus, metronidazole 500 mg TDS for 2 weeks was added to treat Lophomonas infection. It is important to remember that these patients were likely to be under antibiotic treatment at the time of hospitalization, which could have negatively impacted proper microbiological identification. Also, the presumption that a positive therapeutic response to metronidazole initiation should be interpreted with caution, since metronidazole has antimicrobial activity against other anaerobic or microaerophilic bacteria. This study adheres to the Case Report (CARE) guidelines (Supplemental Material).
Discussion
Several studies have demonstrated that Lophomonas infections can affect both immunocompetent and immunocompromised patients, with a particular emphasis on the latter group. This indicates that while individuals with weakened immune systems are at higher risk for severe manifestations of the disease, this can also occur in those with normal immune function.3 –5,7,9 Briefly, our data support the evidence that Lophomonas spp. should not be regarded solely as an opportunistic infection. Therefore, it is essential to screen for Lophomonas in all patients presenting with respiratory symptoms, regardless of immune status.3,4 Persistent clinical, laboratory, and radiologic findings consistent with pneumonia, without documentation of other pathogens in lower airway microbiologic samples, and a lack of clinical improvement under empirical antibiotic therapy should prompt active pursuit of uncommon pathogens.9,10
Lophomonas is a parasite, that is, often overlooked and understudied, with reports limited to a small number of countries, and as such, remains largely unrecognized by many medical scientists.3,4,11 Despite this limited recognition, lophomoniasis is endemic in several regions of Iran.4,10,12 Interestingly, in contrast to the well-established association between lophomoniasis and immunodeficiency in other countries,4,9,11 cases in Iran have predominantly been reported among immunocompetent individuals.3 –8 Lophomoniasis, caused by the parasitic protozoan Lophomonas, is characterized by respiratory symptoms such as cough, fever, and dyspnea, which are often indistinguishable from those of other respiratory infections, making it challenging to diagnose and effectively treat.12,13
Adequate collection and processing of microbiological samples play an important role in the identification of Lophomonas spp.14,15 Smears stained with Trichrome or Giemsa allow a detailed morphological characterization and differentiation from bronchial ciliated cells. 4 Identification and careful analysis of cell motion in wet mounts is, in our experience, highly valuable in determining the presence of Lophomonas in respiratory samples. In order to properly identify the characteristic flagella motions of the protozoa, tracheal aspirates and BALF should be immediately sent to the laboratory so that a fresh examination can be performed.8,9,11
Improper sample handling, a lack of direct observation of fresh samples, and difficulties in proper differentiation from bronchial ciliated cells may all contribute to the under-recognition and underreporting of Lophomonas infection. In our experience, inadequate laboratory management likely plays a role in the underdiagnosis of Lophomonas spp. infection. Bacteriological, mycological, and viral tests performed in respiratory samples may be stored at 4 °C, but the characteristic flagellate movements cannot be identified in a sample that has been subject to these conditions.4,15
Given the association between respiratory symptoms and Lophomonas infection, it is imperative for healthcare practitioners to include lophomoniasis on the list of potential diagnoses for patients presenting with chronic or bloody coughs, persistent sputum, or other respiratory symptoms.8,9,11 Such consideration is essential to ensure timely and appropriate treatment, thereby improving patient outcomes and minimizing the risk of complications associated with this emerging parasitic disease.
Conclusion
Lophomonas spp. is an underdiagnosed emerging respiratory pathogen capable of significant morbidity in immunocompetent individuals. These cases underscore the necessity of including lophomoniasis in the differential diagnosis for persistent pneumonia or atypical respiratory presentations unresponsive to conventional therapy in immunocompetent patients and the importance of relatively quick microscopic examination of fresh respiratory samples. Moreover, molecular techniques can also be used to improve diagnosis accuracy. By raising awareness and improving diagnostic capabilities, such as using fresh sample, healthcare can enhance the identification and management of these infections. Timely administration of metronidazole remains the effective treatment. Heightened clinical suspicion and optimized laboratory protocols are critical for the accurate identification and management of this emerging infection.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X261464741 – Supplemental material for Pulmonary infection due to emerging Lophomonas pathogen in immunocompetent patients: Two case reports
Supplemental material, sj-docx-1-sco-10.1177_2050313X261464741 for Pulmonary infection due to emerging Lophomonas pathogen in immunocompetent patients: Two case reports by Zakaria Zakariaei, Eissa Soleymani, Hossein Mehravaran, Mahdi Fakhar, Elham Sadat Banimostafavi, Majidreza Adelani and Ali Sharifpour in SAGE Open Medical Case Reports
Footnotes
Consent for publication
Written informed consent was obtained from the legally authorized representative of the subject to publish this report in accordance with the journal’s patient consent policy.
Author contributions
E.S., H.M., and M.F. involved in interpretation and collection of data and writing the manuscript. Ash, E.S.B., M.F., Z.Z., H.M., and M.A. involved in editing and preparing the final version of the manuscript. All authors reviewed the paper and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.