
Abstract
This is a care of endophthalmitis following XEN45 Gel Stent implantation managed with combined corneal transplant and pars plana vitrectomy, and to review reported cases of endophthalmitis after minimally invasive glaucoma surgery. A 67-year-old male with primary open-angle glaucoma developed endophthalmitis 2 months after XEN45 implantation. Upon referral to our tertiary care center, he underwent urgent implant removal, penetrating keratoplasty with temporary keratoprosthesis, and pars plana vitrectomy with intravitreal antibiotics. Cultures grew Streptococcus gordonii. A second corneal transplant with fresh donor tissue was performed 4 months later. Despite vision limited to light perception, the infection resolved and the eye was preserved. This is the first reported case of XEN45 Gel Stent-associated endophthalmitis which was successfully controlled with combined keratoplasty and vitrectomy. Our review of published cases identified 45 minimally invasive glaucoma surgery-related endophthalmitis cases, with XEN45 accounting for 58%. Potential risk factors included the XEN45 stent’s susceptibility to exposure after conjunctival erosion, pool water exposure, and ab externo insertion during implantation. In cases of XEN45 Gel Stent-associated endophthalmitis, corneal transplant with pars plana vitrectomy could be a successful strategy to control infection and spare the globe.
Introduction
Minimally invasive glaucoma surgery (MIGS) has emerged as a promising approach for the management of glaucoma, offering a potentially safer alternative to traditional filtering surgeries. Among these procedures, the XEN45 Gel Stent (Allergan, an Abbvie Company, Irvine, CA, USA) has gained popularity due to its safety and efficacy in lowering intraocular pressure (IOP). 1 The XEN45 Gel Stent, a 6 mm long, 45 μm lumen tube is designed to channel aqueous humor between the anterior chamber and the subconjunctival space, creating a new subconjunctival drainage pathway, non-reliant on Schlemm’s canal. 1
While MIGS procedures are associated with a lower risk of complications compared to traditional glaucoma surgeries, post-operative infections, including endophthalmitis, remain a concern. Endophthalmitis is a rare but severe, sight-threatening complication that can occur following any intraocular surgery. The incidence of endophthalmitis after traditional glaucoma filtering surgery has been reported to be approximately 0.1% for trabeculectomy. 2 Starr et al. reported an incidence of 0.25% (one out of 406 cases) for endophthalmitis after XEN45 Gel Stent implantation. 3 In contrast, Burggraaf-Sánchez de las Matas et al. found a higher rate of 1.7% (five out of 293 cases) for late-onset endophthalmitis following XEN45 implantation in their retrospective case series. 4 These varying results highlight the need for further research to establish a more definitive risk profile.
In this report, we describe a case of a patient with endophthalmitis following XEN45 Gel Stent implantation, who underwent combined corneal transplant and pars plana vitrectomy. Additionally, we present a review of endophthalmitis in all MIGS cases reported in the literature to provide context and insight into this rare but serious complication. By analyzing these cases collectively, we aim to better understand the risk factors, clinical presentation, management strategies, and outcomes of endophthalmitis following MIGS procedures.
Case report
A 67-year-old gentleman with a history of primary open-angle glaucoma after XEN45 implant surgery in his left eye 2 months prior was referred to our clinic for endophthalmitis. Other relevant medical history includes a remote mitral valve repair/ring placement. He first presented to local eye providers with eye irritation after swimming in a pool 6 weeks post-XEN45 implant and was prescribed prednisolone eye drops every hour. The patient discontinued the drops after a week, feeling asymptomatic for the next 2 days. However, he soon experienced progressive vision loss, worsening pain, and redness in his left eye, prompting him to visit an outside local emergency room 3 days later, where he was thought to have corneal edema secondary to increased IOP and started on a regimen of moxifloxacin, dorzolamide, timolol, and brimonidine. Three days later, he followed up with his eye provider with worsened light perception (LP) visual acuity and IOP of 20 mmHg. His exam showed a diffuse corneal ulcer of his left eye with no view into the anterior chamber (shown in Figure 1). A B-scan ultrasound showed vitreous opacities overall consistent with endophthalmitis. He underwent an anterior chamber tap with intravitreal injections of vancomycin, ceftazidime, and voriconazole and started on fortified vancomycin and tobramycin drops every 1 h. Cultures from the aqueous tap later grew Streptococcus gordonii, a type of viridans Streptococcus.
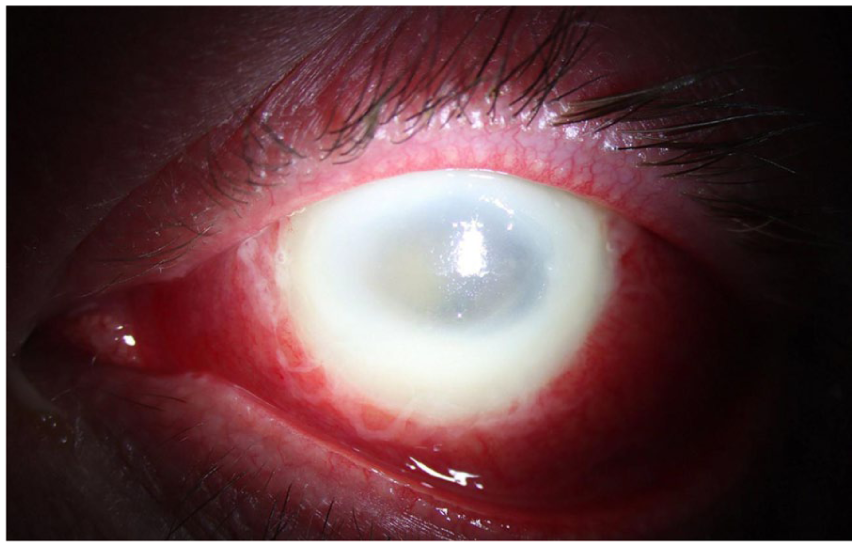
Initial presentation in the emergency room showing a diffuse corneal ulcer of the left eye with no view into the anterior chamber.
The patient was immediately referred to our tertiary care center. Visual acuity in the left eye was still LP upon presentation. His exam showed diffuse corneal infiltrate without posterior view. B-scan ultrasound revealed extensive vitreous debris and concern for a retinal detachment. The patient was brought to the operating room where a visible portion of the XEN45 implant was removed. He then underwent penetrating keratoplasty with placement of an 8.2 mm Landers Wide Field temporary keratoprosthesis, anterior chamber washout, inferior peripheral iridectomy, and removal of dislocated posterior chamber intraocular lens. Intraoperatively, a nasal retinal detachment with multiple holes was visualized. Pars plana vitrectomy with vitreous biopsy, endolaser, air fluid exchange, silicone oil placement, and injection of intravitreal antibiotics and dexamethasone were performed. Finally, the keratoprosthesis was removed and replaced with irradiated corneal tissue, a sterilized non-viable alternative to fresh donor tissue, given the extent of infection and unclear visual potential.
Post-operatively, the patient’s vision was LP, with an IOP of 18 mmHg. Intraoperative cultures grew pan-sensitive Streptococcus viridans and oral levofloxacin was added to his treatment regimen.
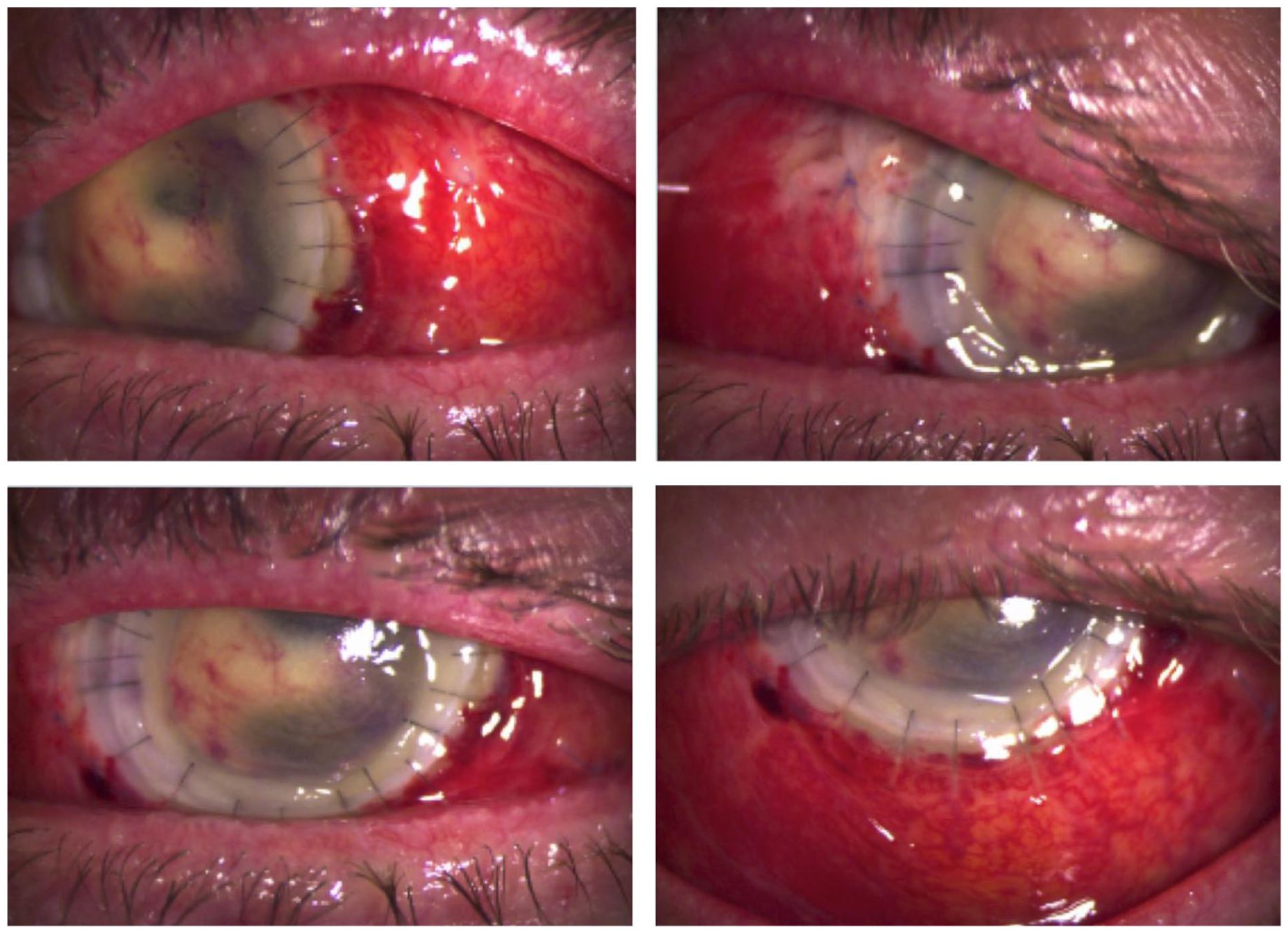
Subsequent follow-up visits showed a stable exam without signs of corneal melt or worsening infiltrate (shown in Figures 2 and 3). There was limited view past the cornea and visualization of the posterior chamber with B-scan was limited due to placement of silicone oil. The patient’s visual acuity was consistently LP. The patient was maintained on a regimen of topical vancomycin, moxifloxacin, prednisolone acetate, atropine, dexamethasone/neomycin/polymyxin B ointment, and oral levofloxacin.
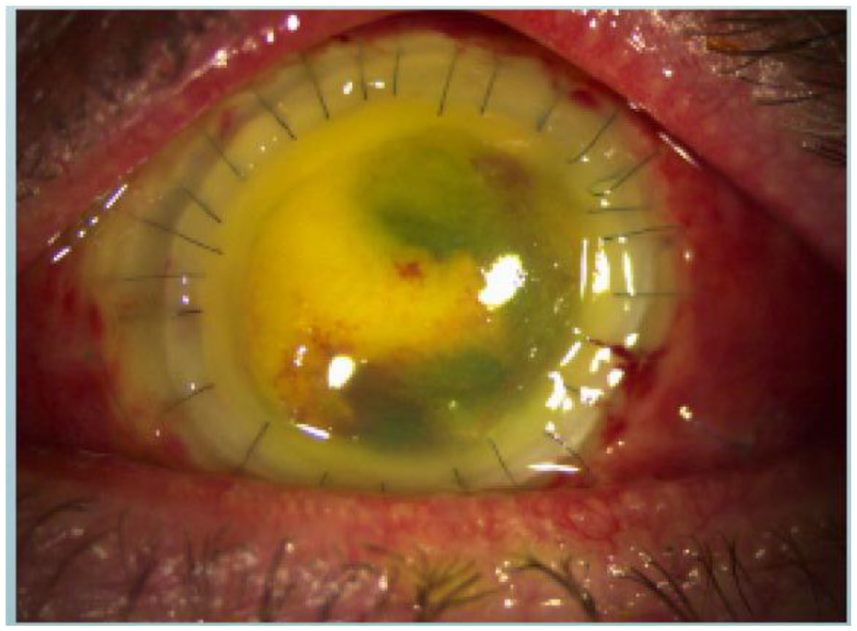
Post-operative day 3 after pars plana vitrectomy and therapeutic penetrating keratoplasty. There is a 360° subconjunctival hemorrhage with superonasal Vicryl sutures. The penetrating keratoplasty has an endothelial plaque of mixed blood and hypopyon. Residual infiltrate was present on the peripheral corneal limbus.
Post-operative week 2. The cornea tissue appears yellow due to fluorescein. The endothelial plaque appears improved, but other exam features are unchanged.
Approximately 4 months after the initial surgery, the eye appeared to be free of infection. At this point, there was persistent corneal scarring from graft failure without view to the retina. The patient underwent a second procedure with penetrating keratoplasty, lysis of anterior synechiae, excision of cyclitic membrane, and more silicone oil placement in the left eye. Intraoperatively, there were dense cyclitic membranes in the anterior segment. A tan-brown 2 mm cylindrical foreign body identified as part of the XEN45 implant was removed from within the fibrotic tissue. Dense neovascular fibrotic membranes were partially dissected, but an adequate view was not achievable and the decision to pursue a vitrectomy was abandoned. The irradiated corneal graft was then replaced with fresh donor tissue.
The patient’s treatment was adjusted to include topical steroids, antibiotics, and sodium chloride hypertonic ointment. In follow-up visits, the graft remained intact and visual acuity in the left eye remained stable at LP with normal IOP. His overall visual prognosis remains guarded; however, the eye was able to be preserved.
Discussion
This is the first reported case of combined corneal transplant and pars plana vitrectomy for successful treatment of endophthalmitis after XEN45 surgery. It highlights the potential risk for severe endophthalmitis following XEN45 Gel Stent implantation, a complication that, while rare, can have devastating consequences. To better understand the landscape of endophthalmitis associated with XEN45 Gel stent and other MIGS implantation, we performed a PubMed search using the terms “endophthalmitis,” “MIGS,” “XEN45,” and “glaucoma.” Included reports described cases of endophthalmitis associated with MIGS devices, including the XEN45 Gel Stent, iStent, CyPass, and Ex-PRESS devices. Both single-case reports and case series were included; when case series were identified, each individual case of endophthalmitis was counted separately. Our review identified 31 cases of endophthalmitis following XEN45 stent implantation summarized in Table 1 and 14 cases of endophthalmitis associated with other MIGS implants summarized in Table 2.
Endophthalmitis cases associated with XEN Gel Stent.
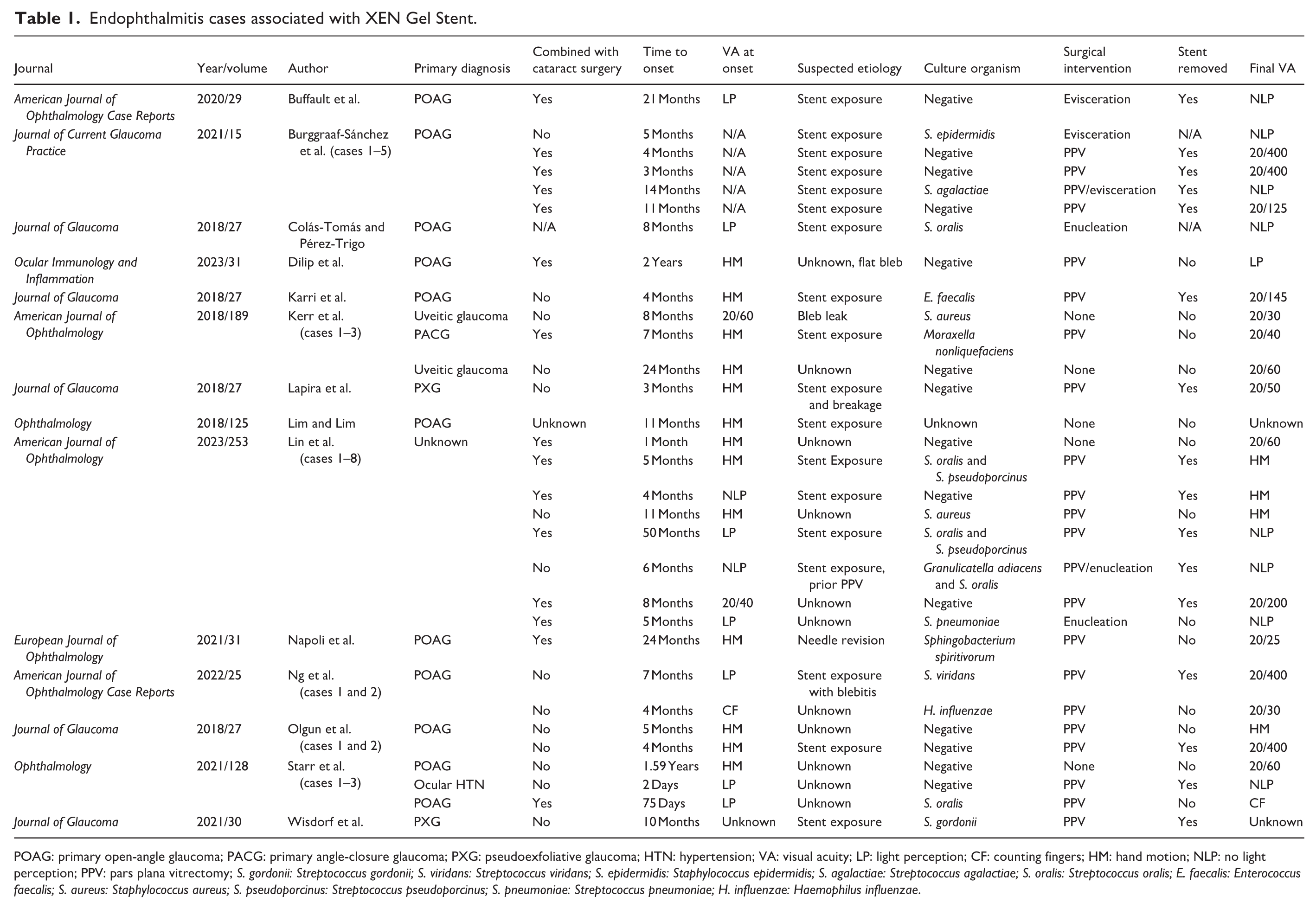
POAG: primary open-angle glaucoma; PACG: primary angle-closure glaucoma; PXG: pseudoexfoliative glaucoma; HTN: hypertension; VA: visual acuity; LP: light perception; CF: counting fingers; HM: hand motion; NLP: no light perception; PPV: pars plana vitrectomy; S. gordonii: Streptococcus gordonii; S. viridans: Streptococcus viridans; S. epidermidis: Staphylococcus epidermidis; S. agalactiae: Streptococcus agalactiae; S. oralis: Streptococcus oralis; E. faecalis: Enterococcus faecalis; S. aureus: Staphylococcus aureus; S. pseudoporcinus: Streptococcus pseudoporcinus; S. pneumoniae: Streptococcus pneumoniae; H. influenzae: Haemophilus influenzae.
Endophthalmitis cases associated with non-XEN Gel Stent MIGS implants.
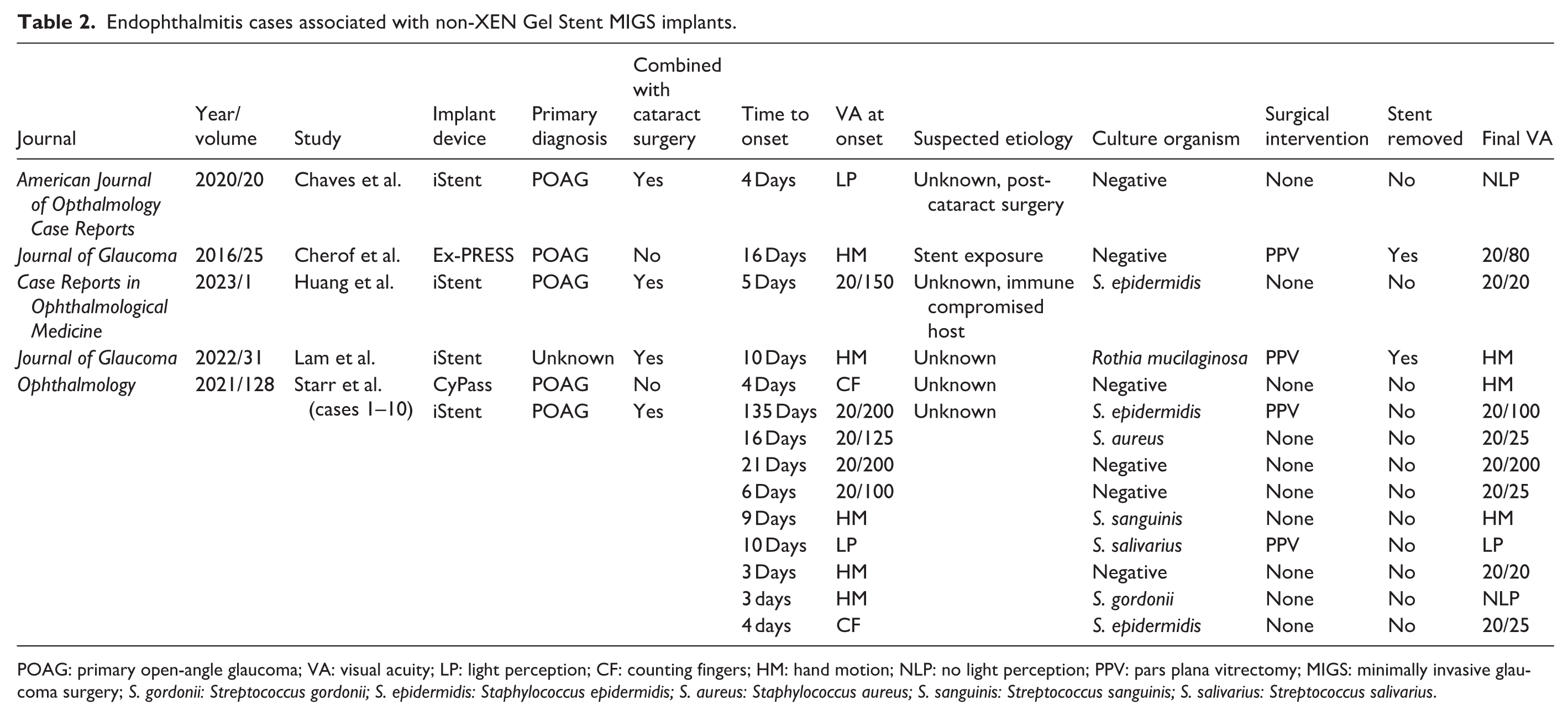
POAG: primary open-angle glaucoma; VA: visual acuity; LP: light perception; CF: counting fingers; HM: hand motion; NLP: no light perception; PPV: pars plana vitrectomy; MIGS: minimally invasive glaucoma surgery; S. gordonii: Streptococcus gordonii; S. epidermidis: Staphylococcus epidermidis; S. aureus: Staphylococcus aureus; S. sanguinis: Streptococcus sanguinis; S. salivarius: Streptococcus salivarius.
Larger studies, while still limited in scope, have provided important context for understanding the overall risk of endophthalmitis with MIGS. Starr et al. review of 3055 MIGS procedures at their institution resulted in an overall incidence of endophthalmitis in 0.13% of patients. 3 Sabharwal et al. reviewed over 40,000 surgeries in the Medicare database and found 44 cases of endophthalmitis (0.11%) following MIGS procedures. 5 Burggraaf-Sánchez de las Matas et al. reported five cases of endophthalmitis out of 293 XEN45 implantations, yielding an incidence of 1.7%. 4 While supporting data are still limited, the possible increase in incidence of endophthalmitis in XEN45 stents could be supported by the unique mechanism of the implant.
The XEN45 stent is unique among MIGS devices in that it creates a new subconjunctival drainage pathway, resulting in a bleb. However, much like traditional trabeculectomy and tube shunts, erosion of the conjunctiva overlying the bleb can lead to exposure of the stent to the outside environment. This infection risk mirrors that of a tube shunt, where tube exposure has been identified as a significant risk factor for endophthalmitis. 6 A review of 38 studies by Stewart et al. showed that conjunctival exposure occurred in 64 cases of 3255 tube shunts, or 2% of all cases. 7 In most case reports involving the XEN45 stent, exposure of the stent was the suspected etiology behind the infection. Other FDA-approved MIGS devices avoid traditional filtering blebs. The iStent and Hydrus MicroStent lower IOP by directly cannulating Schlemm canal. The CyPass Micro-stent creates a drainage canal into the suprachoroidal space; however, it was withdrawn from market due to concerns of corneal endothelial cell loss. 8 While fewer cases of endophthalmitis have been reported with iStent (n = 12), Hydrus (n = 0), and Cypass (n = 1) implantation compared to the XEN45 stent, the exact frequency of endophthalmitis in other devices has not been well reported in the literature.
In bleb-dependent glaucoma surgeries such as XEN45 and Ex-PRESS, long-term filtration and IOP control are limited by subconjunctival fibrosis and have often required bleb needle revision with antifibrotic agents such as mitomycin-C and 5-fluorouracil. 9 Yook et al. reported that rates of needle revision after XEN45 implant ranged from 12/37 eyes (32%) to 7/15 eyes (47%) across early published studies. 10 These agents are crucial for reducing the risk of bleb fibrosis and failure, but contribute to thinner, avascular blebs that can leak and place patients at risk of endophthalmitis. In studies of trabeculectomies with adjunctive mitomycin C, bleb leakage was a common postoperative complication. 11 While cases of endophthalmitis are still rare after bleb leakage, this known risk factor in trabeculectomies is likely relevant in XEN45 implantation as well.
Another difference between the XEN45 stent and other MIGS procedures is the route of injection. Like most MIGS devices, the stent was FDA approved to be placed via an ab interno approach, through a corneal incision. Recently, many surgeons have opted for an ab externo approach, disrupting the outside conjunctiva and inserting the stent through the sclera. 12 While some believe this method may allow for more precise positioning, there may be an increased risk of poor wound healing, especially when combined with antifibrotics. Limited comparisons so far have shown no significant difference in adverse events between the two approaches. 12 In our patient, an ab externo approach was described by the patient’s surgeon. Unfortunately, many cases in the literature are performed at outside institutions and are unclear regarding the approach.
The microbiology of MIGS-related endophthalmitis appears diverse. In our review, the majority of causative organisms included various streptococcal and staphylococcal species, including our patient that grew S. gordonii, a member of the viridans group streptococci, that is, commonly part of the oral flora. Most of these organisms are part of the normal skin/oral flora and have been implicated in cases of endophthalmitis following intraocular surgery. 13 The patient’s recent pool water exposure was another risk factor. While a recently placed XEN45 stent in our patient is strongly suggestive of an exogenous source of infection, we cannot completely rule out endogenous sources, such as the patient’s remote history of mitral valve repair. However, his prior echocardiograms without signs of valvular lesions and lack of systemic infection signs at the time of presentation make endocarditis a highly unlikely source.
Management of MIGS endophthalmitis typically involves a combination of intravitreal antibiotics and vitrectomy. Of the 45 cases in our review, 58% (n = 26) underwent pars plana vitrectomy. The decision to perform vitrectomy was often based on the severity of the infection and the clarity of the ocular media. In some cases, such as those reported by Olgun et al., vitrectomy was not performed due to corneal haziness or dense vitreous opacities, which precluded adequate visualization. 14 These cases were initially managed with intravitreal antibiotics alone, with vitrectomy reserved for cases that didn’t respond to initial treatment or where visualization improved. In our case of endophthalmitis with corneal ulcer post-XEN45 implantation, a cornea transplant was performed together with pars plana vitrectomy in order to clear infected tissue and provide a better view into the posterior chamber for surgical intervention. Similar strategies have been employed in cases of keratitis-associated fungal endophthalmitis as described by Wykoff et al. with 17 out of 18 of these patients undergoing penetrating keratoplasty as the result of severe corneal involvement or risk of perforation. 15
The visual outcomes in reported cases of MIGS-related endophthalmitis have been variable, ranging from 20/25 to no LP. Over half of the eyes had a final reported visual acuity of 20/200 or worse. Six cases resulted in evisceration/enucleation. Ultimately, our patient was able to preserve his eye. While 38 of 45 eyes (84%), including ours, developed endophthalmitis within the first year, cases of endophthalmitis ranged from 2 days to 4 years post implantation. This wide range highlights the need for long-term vigilance and comprehensive evaluation in patients post-MIGS (Supplemental Material).
Conclusion
While MIGS offers a minimally invasive approach to glaucoma management, the risk of endophthalmitis, though rare, remains a serious concern. Our case, along with others in the literature, demonstrates the potential for severe, vision-threatening infection following MIGS implantation. The XEN45 stent may also carry additional infection risks compared to the iStent and Hydrus, including bleb leakage, needle revision with antifibrotics, and ab externo approach. Long-term vigilance is important given that cases of endophthalmitis have been attributed as far out as 4 years post-implantation. In endophthalmitis patients with severe corneal comorbidity, treating with corneal transplant and pars plana vitrectomy together can be a good strategy for preserving the eye. Further research is needed to better understand the risk factors and optimize management and prevention strategies for this rare but serious complication of MIGS.
Supplemental Material
sj-pdf-1-sco-10.1177_2050313X261465147 – Supplemental material for Endophthalmitis in XEN45 Gel Stent: Case report and review of the literature
Supplemental material, sj-pdf-1-sco-10.1177_2050313X261465147 for Endophthalmitis in XEN45 Gel Stent: Case report and review of the literature by William Xu, Anjay Shah, Kristin Ates Hicks, Lauren Jeang and Jinghua Chen in SAGE Open Medical Case Reports
Footnotes
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author contributions
All authors attest that they meet the current ICMJE criteria for authorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.