
Abstract
Caroli’s disease is a rare congenital disorder of the intrahepatic bile ducts that may be complicated by congenital hepatic fibrosis, portal hypertension, and recurrent variceal bleeding. We report the 10-year clinical course of a 29-year-old woman with Caroli’s disease and portal hypertension who was managed in the Department of Gastroenterology. At initial presentation in 2015, she had splenomegaly, severe esophagogastric fundal varices, preserved liver biochemistry, Child-Pugh class A disease, and a low model for end-stage liver disease score. Symptoms improved after nonselective beta-blocker therapy; however, longitudinal follow-up showed persistent portal hypertension, recurrent gastrointestinal bleeding, and progressive impairment of hepatic reserve. From 2023 onward, she experienced recurrent hematemesis and melena despite sequential endoscopic variceal ligation and beta-blocker therapy, including conversion from propranolol to carvedilol. During the most recent admission on May 25, 2024, laboratory and imaging findings indicated progressive cholestasis, portal hypertension, Child-Pugh class B disease, and a model for end-stage liver disease score of 9.9. After multidisciplinary team evaluation, liver transplantation was considered clinically indicated, and the patient was activated on the transplant waiting list. This case demonstrates the limitations of long-term endoscopic and pharmacological therapy in Caroli’s disease complicated by portal hypertension and supports timely transplant referral before advanced hepatic decompensation occurs.
Keywords
Introduction
Caroli’s disease, also known as congenital intrahepatic cholangiectasis, is a rare ductal plate malformation characterized by segmental or multifocal cystic dilatation of the intrahepatic bile ducts. 1 It is generally classified as simple Caroli’s disease, in which ductal dilatation occurs without congenital hepatic fibrosis, or Caroli syndrome, in which ductal abnormalities are accompanied by periportal fibrosis and may progress to portal hypertension.1 –3 Diagnosis is supported by compatible clinical manifestations, such as cholangitis, intrahepatic bile duct stones, jaundice, and portal hypertension, together with characteristic cross-sectional imaging and histological findings when biopsy is clinically indicated.2,3 Portal hypertension and variceal bleeding are clinically important complications. Current portal hypertension guidance supports risk stratification using liver function, noninvasive markers, and endoscopic findings, with nonselective beta-blockers and endoscopic therapy used to prevent or control variceal bleeding in appropriate patients.9,10 However, the durable effectiveness of these measures in Caroli’s disease with progressive cholestatic liver injury remains uncertain. This case report describes a patient with Caroli’s disease complicated by portal hypertension who was followed for 10 years and ultimately required activation on the liver transplantation waiting list after recurrent gastrointestinal bleeding despite repeated endoscopic and pharmacological therapy.
Case presentation
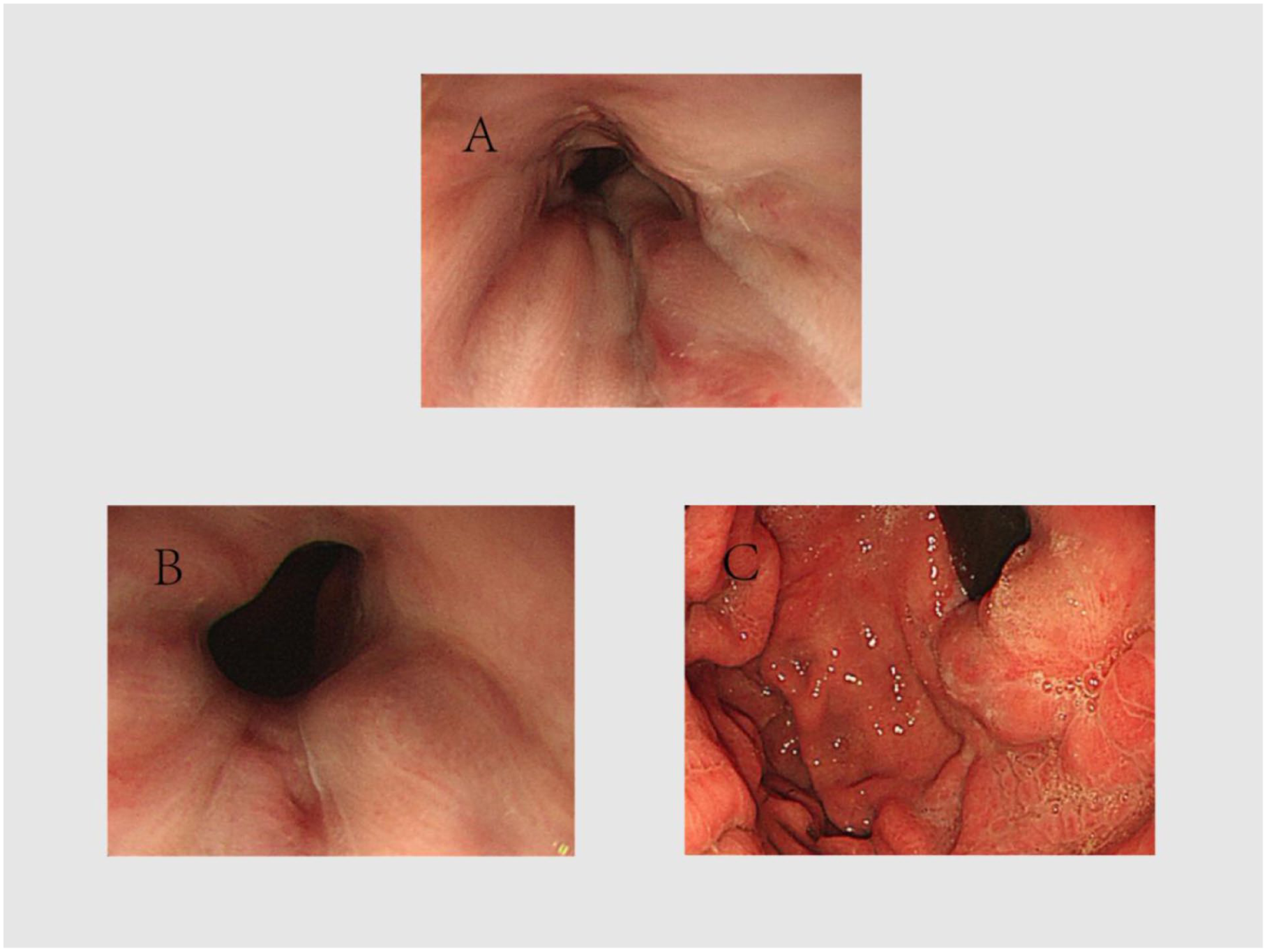
The clinical course is presented chronologically to clarify disease progression, therapeutic decisions, and the timing of transplant referral. The patient was initially diagnosed with Caroli’s disease and concomitant portal hypertension at 29 years of age. She had no relevant prior treatment history before admission on March 30, 2015 for intermittent abdominal bloating and anorexia. Physical examination revealed splenomegaly and mild lower-extremity edema; other findings were unremarkable. Liver function tests were within normal limits. Routine blood testing showed anemia, with a hemoglobin level of 95 g/L, and coagulation testing showed a prothrombin activity of 61.6%. Contrast-enhanced abdominal magnetic resonance imaging (MRI) demonstrated cirrhosis, portal hypertension, and cystic dilatation of the intrahepatic bile ducts; liver biopsy confirmed marked dilatation of the intrahepatic bile ducts (Figure 1). Upper gastrointestinal endoscopy (UGIE) revealed severe esophagogastric fundal varices. Varices were recorded using the Location, Diameter, and Risk Factor (LDRF) system, which documents variceal location, maximal diameter, and endoscopic risk factors for bleeding. For international readers, this notation should be interpreted together with conventional endoscopic descriptors of variceal size, location, and high-risk stigmata. At baseline, the LDRF stage was Le,g D1.0 Rf0, indicating esophageal and gastric varices without active bleeding, erosion, or thrombus; elective endoscopic variceal ligation (EVL) or repeat endoscopic surveillance every 6 months was recommended (Figure 2). The Child-Pugh classification was grade A, and transient elastography showed a liver stiffness measurement (LSM) of 49.4 kPa, consistent with fibrosis stage F4.
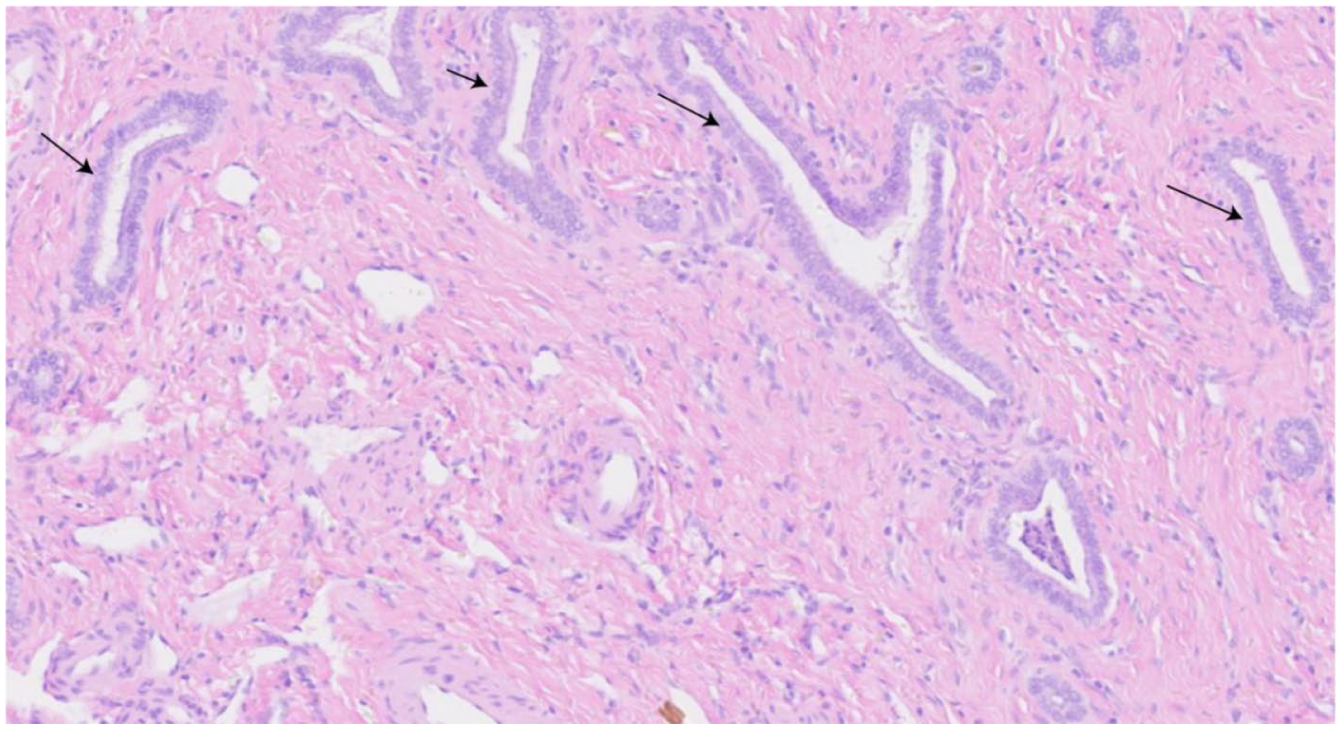
Liver biopsy with hematoxylin and eosin staining (original magnification, ×100). The arrow indicates dilated intrahepatic bile ducts.
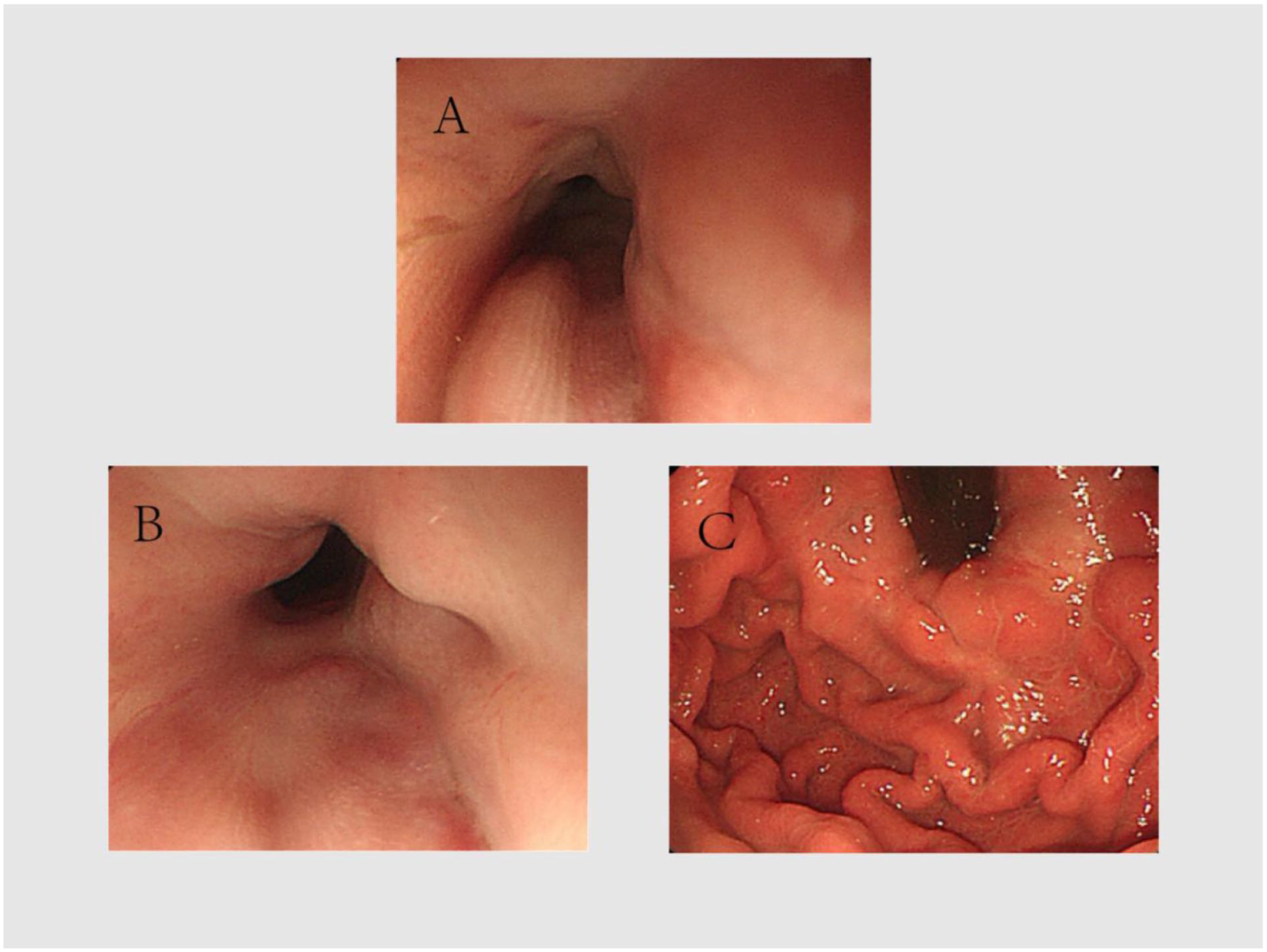
Baseline UGIE findings showing Le,g D1.0 Rf0 varices. (a, b) Esophageal varices. (c) Gastric varices.
Because there was no evidence of active gastrointestinal bleeding at that time, endoscopic intervention was deferred and the patient received oral propranolol (10 mg three times daily). Her abdominal bloating and anorexia improved, and she was discharged on April 12, 2015. During outpatient follow-up, she continued propranolol and underwent regular assessment with complete blood counts, liver biochemistry, coagulation testing, and transient elastography. Early follow-up showed persistent portal hypertension with only modest LSM fluctuation from 49.4 kPa in 2015 to approximately 50.7 kPa in 2021 (Figure 3). During subsequent follow-up, the patient did not achieve sustained improvement in liver function, and the overall trajectory suggested persistent portal hypertension despite temporary symptom control.
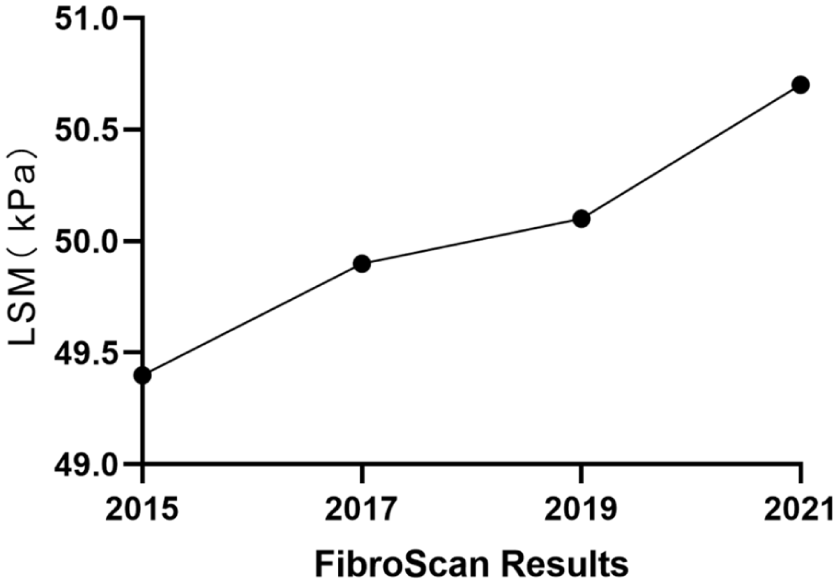
Longitudinal trend in liver stiffness measurement during early follow-up.
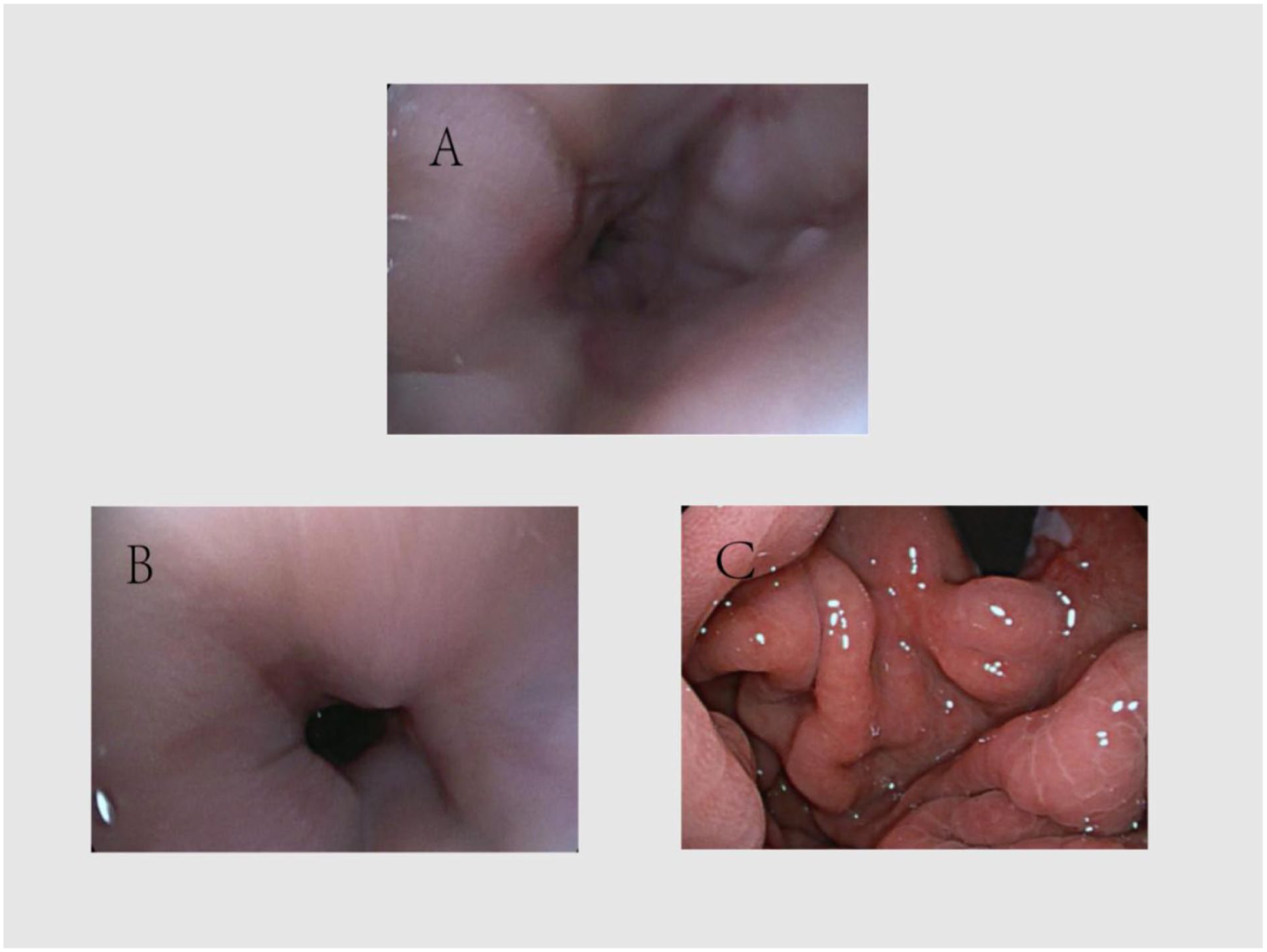
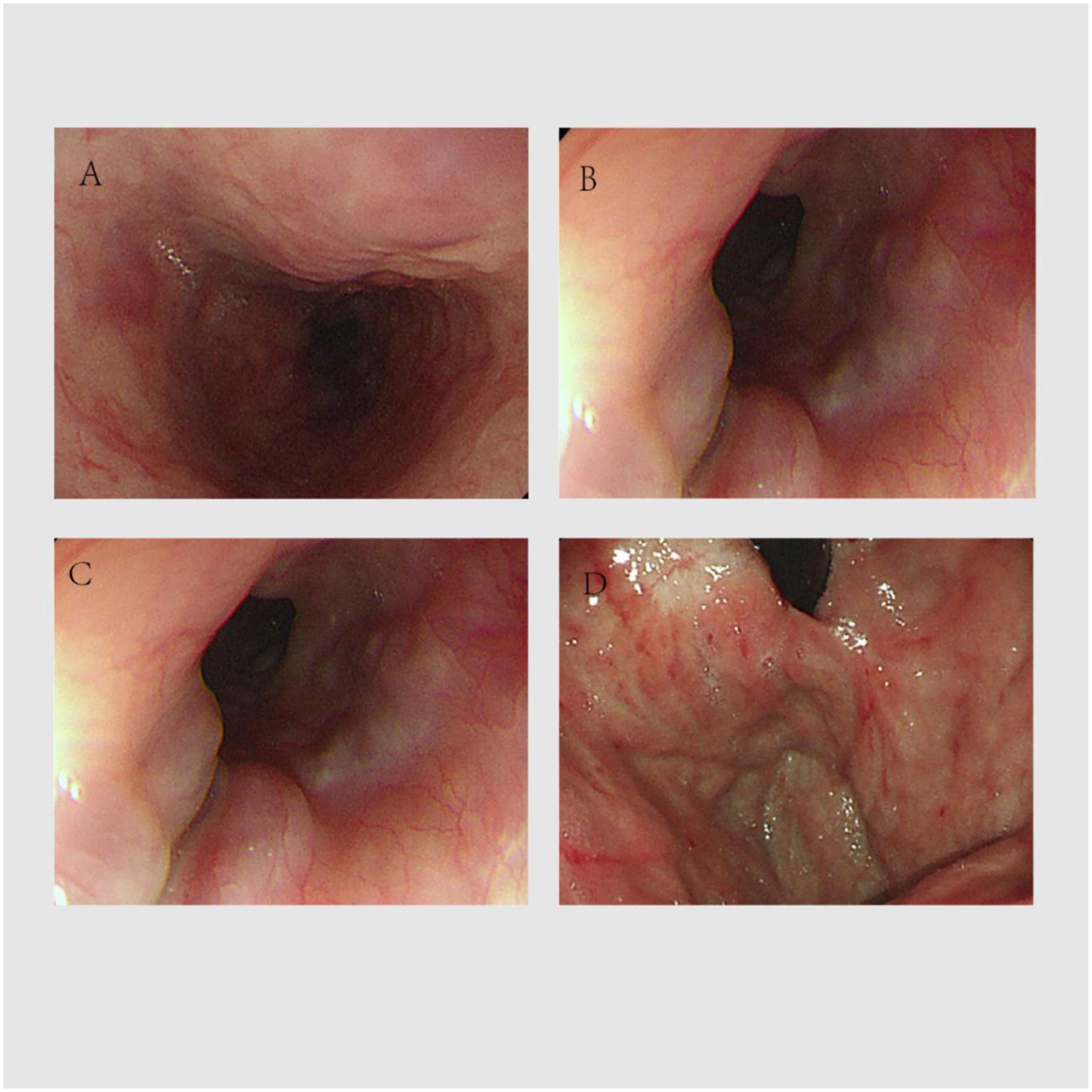
From 2023 onward, the patient developed recurrent hematemesis and melena. On March 28, 2023, UGIE showed severe esophagogastric fundal varices with LDRF staging of Le,g D1.5 Rf2, indicating enlarged varices and high-risk endoscopic features requiring urgent or sequential endoscopic therapy (Figure 4). EVL was performed, and propranolol was switched to carvedilol (10 mg daily) because carvedilol combines nonselective beta-adrenergic blockade with additional alpha1-adrenergic antagonism, thereby reducing portal pressure through both decreased cardiac output and reduced intrahepatic vascular resistance.9,10 Follow-up UGIE on May 26, 2023 showed improvement to Le,g D1.0 Rf1 (Figure 5), and repeat UGIE on February 23, 2024 again showed Le,g D1.0 Rf1 varices (Figure 6). Although symptoms improved after each intervention, recurrent bleeding and persistent portal hypertension indicated that endoscopic and pharmacological therapy had not achieved durable disease control (Tables 1 and 2).
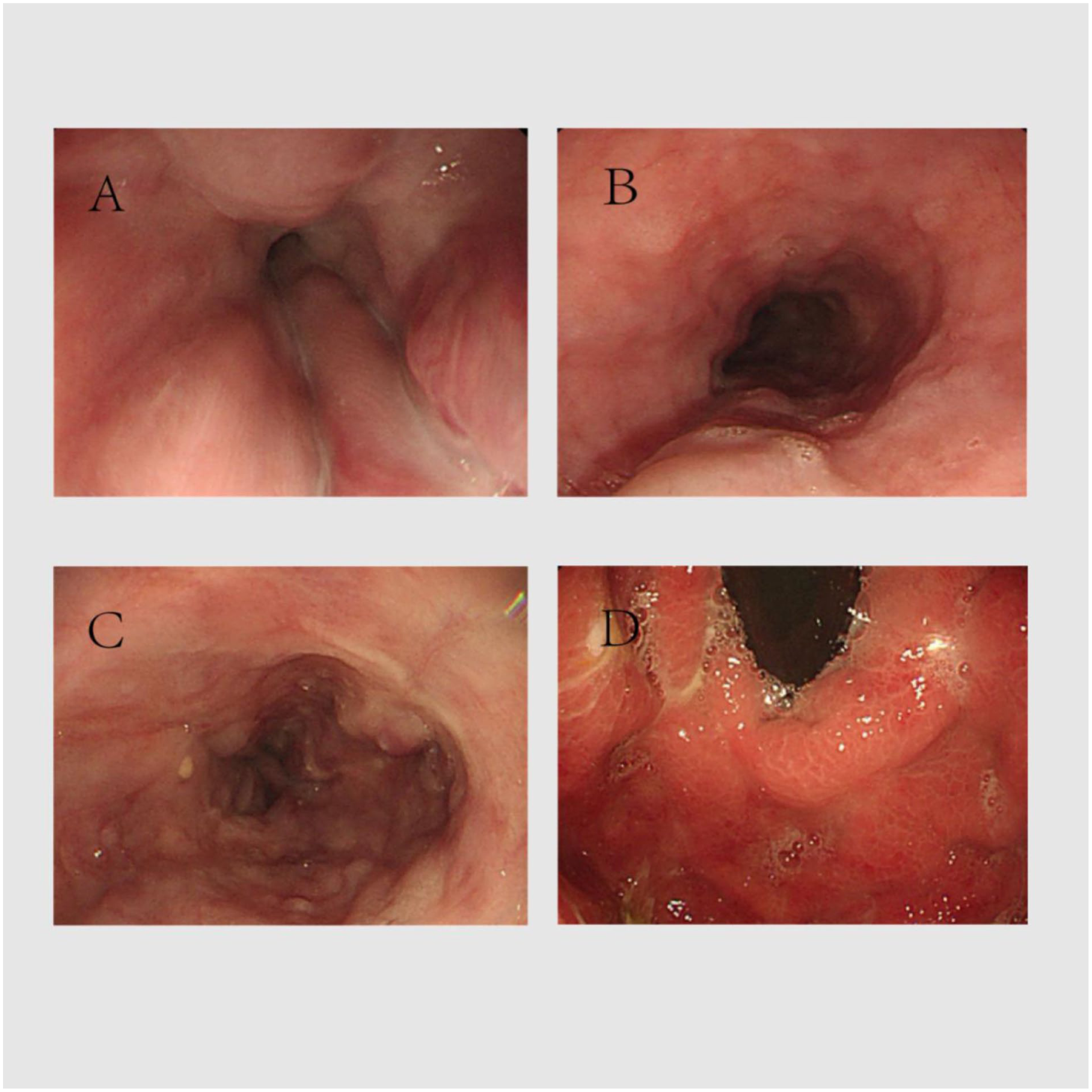
UGIE findings showing Le,g D1.5 Rf2 varices. (a–c) Esophageal varices. (d) Gastric varices.
UGIE findings after treatment showing Le,g D1.0 Rf1 varices. (a, b) Esophageal varices. (c) Gastric varices.
Follow-up UGIE findings showing Le,g D1.0 Rf1 varices. (a, b) Esophageal varices. (c) Gastric varices.
Longitudinal summary of laboratory tests, endoscopic findings, prognostic scores, and key treatment decisions. Results of routine blood tests, liver function tests, and routine coagulation tests reviewed by the patient.
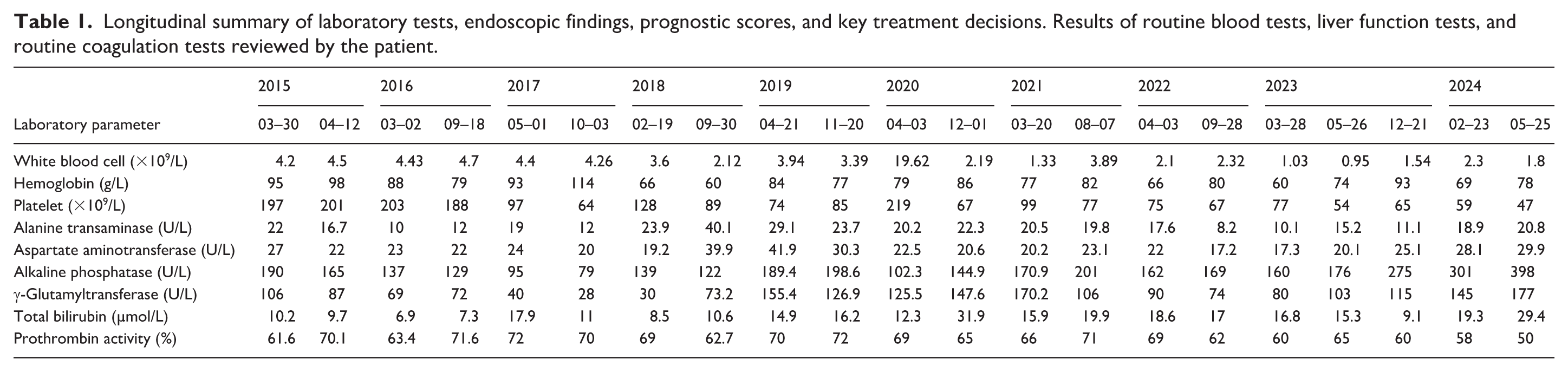
Longitudinal summary of clinical course and laboratory progression.

ALP: alkaline phosphatase; EVL: endoscopic variceal ligation; Gamma-GT: gamma-glutamyltransferase; LSM: liver stiffness measurement; MDT: multidisciplinary team; MELD: model for end-stage liver disease; MRI: magnetic resonance imaging; PA: Prothrombin activity; TB: total bilirubin; UGIE: upper gastrointestinal endoscopy.
Note. Values are extracted from the supplied manuscript files and newly added draft. Figure 3 depicts the early LSM trend through 2021; the final admission LSM is reported separately in the case description.
The patient presented again with hematemesis and melena on May 25, 2024. Liver function tests showed alkaline phosphatase of 398 U/L, gamma-glutamyltransferase of 177 U/L, and total bilirubin of 29.4 µmol/L. Routine blood testing showed a hemoglobin level of 78 g/L, and coagulation testing showed prothrombin activity of 62%. Abdominal MRI demonstrated portal hypertension and multiple dilated intrahepatic bile ducts (Figure 7). Transient elastography showed an LSM of 81.0 kPa, consistent with fibrosis stage F4. The Child-Pugh classification had progressed to grade B, whereas the model for end-stage liver disease (MELD) score remained relatively low at 9.9. UGIE demonstrated severe esophagogastric fundal varices with LDRF staging of Le,g D1.0 Rf1 (Figure 8), and EVL was performed. The patient’s acute bleeding symptoms improved after treatment. Longitudinal interpretation of the available laboratory, elastography, and endoscopic data indicated progression from compensated to decompensated disease: early preserved liver biochemistry and Child-Pugh class A status were followed by recurrent bleeding, anemia, worsening cholestatic parameters, Child-Pugh class B disease, and markedly increased LSM. The patient expressed significant concerns regarding operative complications, organ rejection, financial burden, adverse effects of immunosuppression, and the possibility of disease recurrence, which complicated shared decision-making.
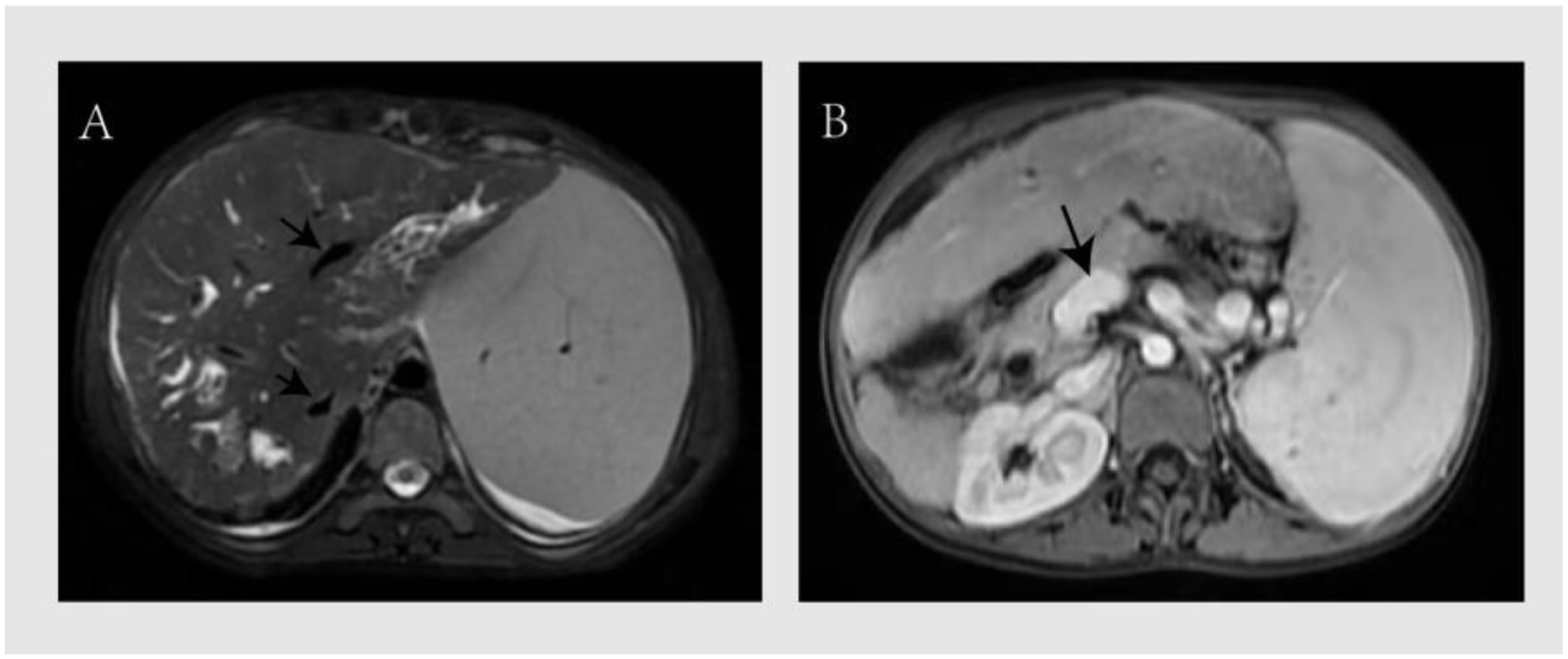
Abdominal MRI during the 2024 admission. (a) T2-weighted or cholangiographic image showing multiple dilated intrahepatic bile ducts (arrows). (b) Contrast-enhanced abdominal MRI showing dilatation of the portal vein (arrow).
UGIE findings during the 2024 admission showing Le,g D1.0 Rf1 varices. (a, b) Esophageal varices. (c, d) Gastric varices.
An multidisciplinary team (MDT) comprising specialists in gastroenterology, vascular surgery, hepatobiliary-pancreatic surgery, and critical care medicine was convened. The MDT clarified that the MELD score of 9.9 was low rather than high; therefore, the decision not to prioritize transjugular intrahepatic portosystemic shunt (TIPS) was not based on a high MELD score. Instead, the team considered the patient’s diffuse cholangiopathy, recurrent variceal bleeding despite optimized endoscopic and pharmacological therapy, progressive portal hypertension, Child-Pugh class B disease, and need for disease-modifying treatment. TIPS may reduce portal pressure in selected patients with preserved hepatic reserve and suitable anatomy, but it would not address the underlying congenital biliary disease or the long-term risk of progressive hepatic dysfunction. In this context, liver transplantation was considered clinically indicated, with recurrent variceal bleeding and progressive liver dysfunction as major clinical indications and no absolute contraindication identified. After written informed consent and shared decision-making, the patient was activated on the liver transplantation waiting list. A detailed clinical timeline is presented in Figure 9.
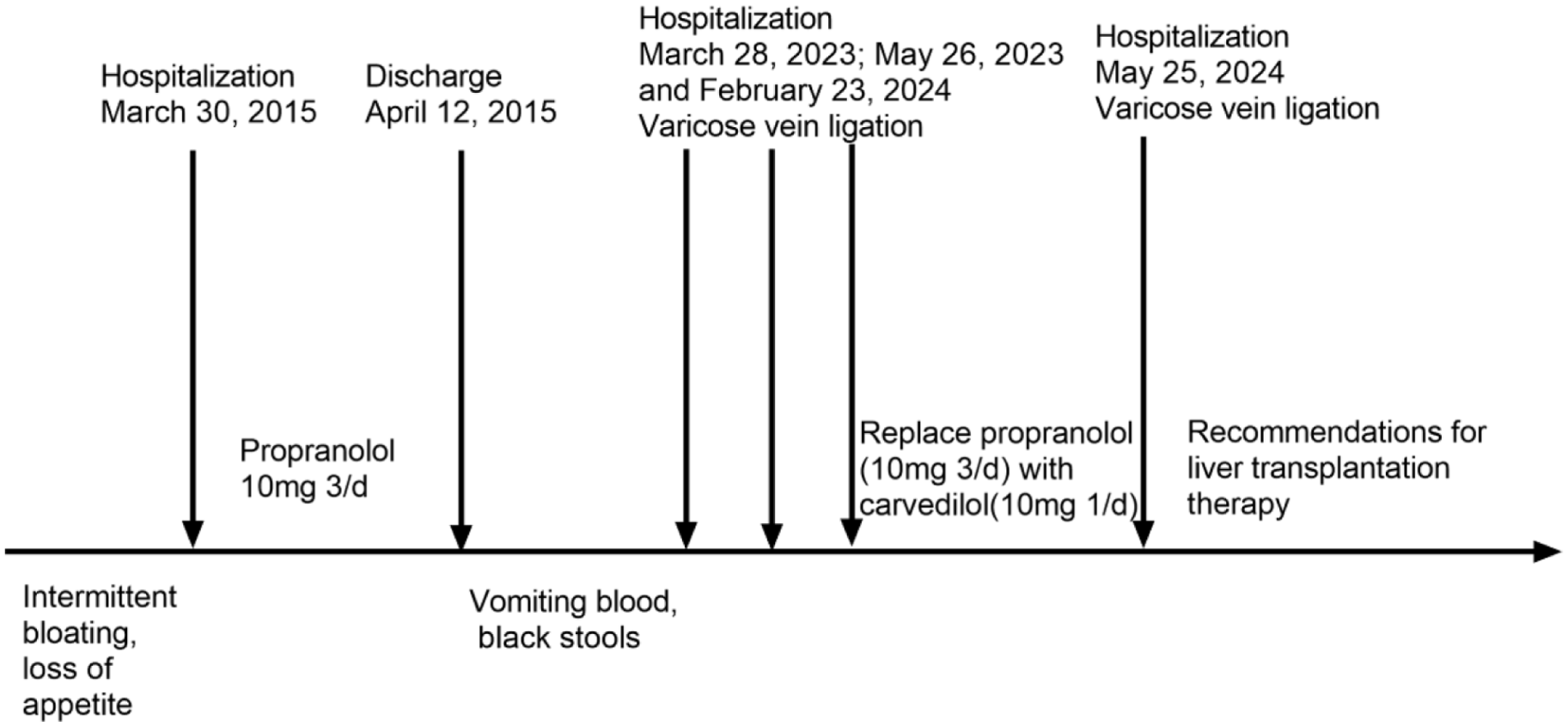
Chronological timeline of disease progression, recurrent variceal bleeding, endoscopic interventions, pharmacological therapy, and activation on the liver transplantation waiting list.
Discussion
Segmental cystic dilatation of the intrahepatic bile ducts is the pathological hallmark of Caroli’s disease. Clinical manifestations include abdominal pain, recurrent cholangitis, cholestasis, jaundice, intrahepatic stones, and biliary obstruction. 4 Clinically important long-term complications include portal hypertension, variceal bleeding, recurrent infection, liver abscess, cholangiocarcinoma, pancreatitis, choledocholithiasis, cirrhosis, liver failure, and amyloidosis.4,5 The present case illustrates how portal hypertension can dominate the clinical course even when early liver biochemistry and MELD score are relatively preserved. Diagnosis and follow-up should therefore integrate cross-sectional imaging, endoscopic assessment of varices, histology when indicated, and serial prognostic evaluation rather than relying on a single laboratory value.
Therapeutic options for Caroli’s disease include medical therapy, endoscopic management of portal hypertensive complications, interventional radiology, hepatic resection for localized disease, and liver transplantation for diffuse or progressive disease. Previous surgical series and transplant registry analyses suggest that liver transplantation may provide durable disease control in selected patients with diffuse Caroli’s disease or Caroli syndrome when conservative or local therapies fail.6 –8,11 Contemporary portal hypertension guidance emphasizes individualized risk stratification, nonselective beta-blockers, endoscopic therapy, and selective consideration of TIPS or transplantation according to liver function, bleeding recurrence, portal hypertension severity, and overall prognosis.9,10 In this context, the present case is clinically relevant because repeated EVL plus nonselective beta-blocker therapy controlled acute bleeding episodes but did not prevent recurrent bleeding or long-term progression in a patient with diffuse cholangiopathy and progressive portal hypertension.
In this patient, the transition from compensated to decompensated disease was supported by concordant clinical, endoscopic, imaging, and laboratory findings. At the initial presentation, Child-Pugh class A status, relatively preserved bilirubin and coagulation parameters, and a low MELD score were consistent with compensated disease despite severe varices and elevated LSM. Over 10 years, recurrent variceal bleeding, worsening cholestatic markers, anemia associated with bleeding, progression to Child-Pugh class B disease, and LSM elevation to 81.0 kPa indicated escalating portal hypertension and impaired hepatic reserve. The switch from propranolol to carvedilol was pharmacologically reasonable because carvedilol exerts additional alpha1-blocking activity and may achieve greater portal pressure reduction than traditional nonselective beta-blockers in selected patients.9,10 Nevertheless, recurrent bleeding despite sequential EVL and beta-blocker therapy indicated failure of conventional long-term management and supported MDT-based transplant referral. Importantly, the MELD score of 9.9 should not be interpreted as a high MELD score. Rather, this case underscores that recurrent portal hypertensive bleeding, progressive cholangiopathy, and deteriorating Child-Pugh class may justify early transplant evaluation before the MELD score reaches conventional high-priority thresholds.
The novelty of this case lies in the duration and granularity of follow-up. Long-term reports that integrate serial clinical events, endoscopic findings, laboratory trends, elastography, prognostic scores, and transplant decision-making in Caroli’s disease complicated by portal hypertension remain limited. This report documents a 10-year course from initial compensated disease with severe varices to recurrent gastrointestinal bleeding, progressive portal hypertension, Child-Pugh class B disease, and activation on the liver transplantation waiting list. The case therefore adds longitudinal clinical evidence that endoscopic and pharmacological therapy may be insufficient as a durable strategy in selected patients with Caroli’s disease complicated by portal hypertension. It also highlights the need for early transplant referral when recurrent variceal bleeding occurs despite optimized therapy, even if the MELD score remains relatively low. The main limitation is that this is a single case report; therefore, its implications should be interpreted cautiously and validated through larger cohorts or multicenter case series.
Conclusion
For patients with Caroli’s disease complicated by decompensated cirrhosis and portal hypertension, endoscopic therapy and nonselective beta-blockers remain important for controlling variceal bleeding. However, recurrent bleeding despite optimized therapy should prompt reassessment of disease trajectory and early referral for liver transplantation. In patients with preserved hepatic reserve and appropriate anatomy, TIPS may be considered for portal pressure reduction, but the decision should be individualized and integrated with the underlying biliary disease, Child-Pugh class, MELD score, bleeding recurrence, and transplant candidacy. In the present case, liver transplantation was clinically indicated and the patient was activated on the waiting list; therefore, transplantation should be described as a potential definitive treatment option rather than an achieved cure. Early multidisciplinary evaluation may improve the timing of referral and long-term outcomes in selected patients.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X261467162 – Supplemental material for Ten-year progression of Caroli’s disease with portal hypertension despite endoscopic and pharmacological therapy: Implications for liver transplantation—A case report
Supplemental material, sj-docx-1-sco-10.1177_2050313X261467162 for Ten-year progression of Caroli’s disease with portal hypertension despite endoscopic and pharmacological therapy: Implications for liver transplantation—A case report by Han Meng, Ruiyu Xie and Chuanjie Yang in SAGE Open Medical Case Reports
Footnotes
Ethical considerations
This study was approved by the Medical Ethics Committee of the Second Hospital of Hebei Medical University and was conducted in accordance with the Declaration of Helsinki, its currently applicable amendments, and applicable Chinese laws and regulations.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report, including all clinical details and accompanying images.
Author contributions
Han Meng and Ruiyu Xie analyzed the clinical data and drafted the manuscript. Chuanjie Yang conceived the study and critically revised the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Reporting guideline
This case report was prepared in accordance with the CARE reporting guideline. The completed CARE checklist will be uploaded as a separate Supplemental Material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.