
Abstract
Discrepancies in platelet counts between laboratories may lead to diagnostic confusion and unnecessary interventions. We report a case in which platelet counts were consistently normal in an in-house laboratory but repeatedly decreased in external laboratory testing. The patient had no bleeding symptoms, and coagulation findings were normal. Peripheral blood smear examination revealed platelet aggregation in externally processed samples, whereas no aggregation was observed in samples processed immediately in-house. These findings strongly support ethylenediaminetetraacetic acid (EDTA)-dependent pseudothrombocytopenia associated with pre-analytical factors, particularly processing delay. Recognition of this phenomenon is essential to avoid unnecessary investigations and inappropriate management.
Keywords
Introduction
Platelet counts are essential hematologic parameters in clinical practice; however, they are susceptible to various pre-analytical factors, including anticoagulants, transport conditions, and time to analysis.1 –3 These factors may lead to spurious thrombocytopenia and potentially misleading clinical interpretations.
Here, we report a case of marked discrepancy in platelet counts between in-hospital and external laboratory testing, ultimately attributed to EDTA-dependent pseudothrombocytopenia, highlighting an important pre-analytical pitfall in routine clinical practice.
Case presentation
A male patient in his 70s was found to have a markedly reduced platelet count of 6.2 × 104/µL measured by an automated hematology analyzer at an external laboratory. Despite this finding, he exhibited no bleeding symptoms, and his hemoglobin, white blood cell count, lactate dehydrogenase, and potassium levels were within normal ranges. The patient had no history of medication use associated with thrombocytopenia.
Simultaneous measurements at our in-hospital laboratory consistently demonstrated normal platelet counts (17.0–18.5 × 104/µL). A chronological comparison showed persistent discrepancies between laboratories: the external laboratory repeatedly reported decreased platelet counts, whereas in-house measurements consistently remained within the normal range. Detailed time-series data are presented in Table 1.
Time-series comparison of platelet counts between in-hospital and external laboratory measurements.
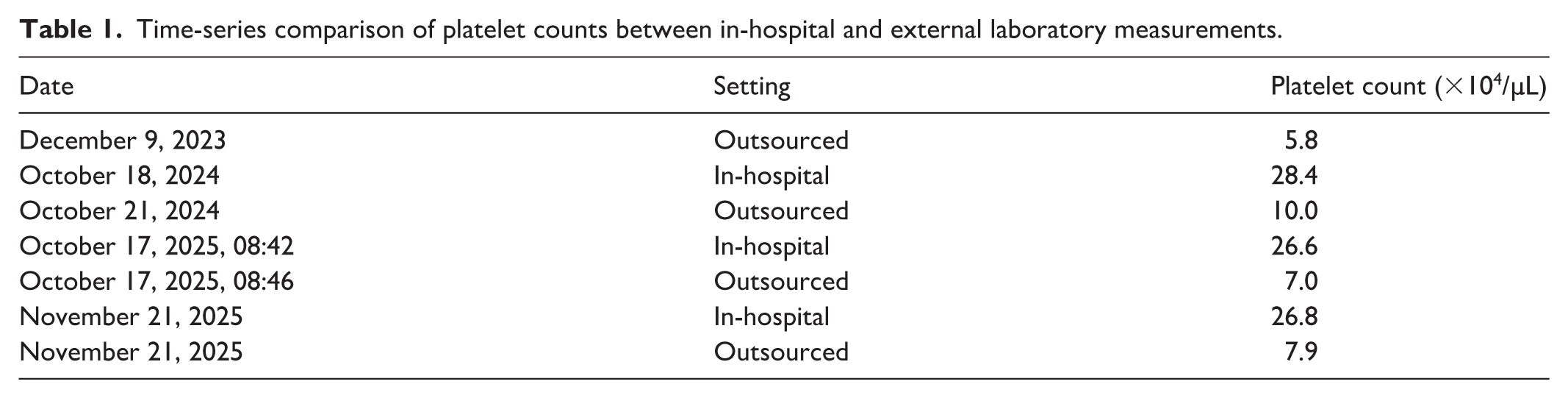
In our institution, blood samples obtained in the outpatient clinic are processed immediately in the in-house laboratory, whereas samples obtained through the Health Management Department are routinely outsourced to an external laboratory service. Therefore, platelet counts from the two settings were analyzed under different pre-analytical conditions despite using the same hematology analyzer model Sysmex XN-1000 (Sysmex Corporation, Kobe, Japan).
Because platelet counts obtained from immediately processed in-house samples remained consistently within the normal range and the patient showed no bleeding tendency or coagulation abnormalities, additional coagulation studies or confirmatory testing using alternative anticoagulants such as sodium citrate were not performed by the attending physicians.
Because both laboratories used optical methodologies, the discrepancy could not be attributed to differences in analytical principles, implicating pre-analytical factors rather than true thrombocytopenia.
Peripheral blood smear examination performed during routine clinical practice suggested platelet aggregation in outsourced samples.
No treatment was required, and platelet counts measured at our institution remained stable during follow-up without clinical events.
Discussion
The present case highlights the importance of recognizing pre-analytical factors as a potential cause of marked discrepancies in platelet counts between laboratories. In this patient, platelet counts remained consistently within the normal range when analyzed immediately in our in-house laboratory, whereas repeatedly decreased values were reported by the outsourced laboratory. Because the patient had no bleeding symptoms and coagulation-related findings were unremarkable, true thrombocytopenia was considered unlikely.
EDTA-dependent pseudothrombocytopenia is a well-recognized in vitro phenomenon caused by platelet aggregation in blood samples anticoagulated with EDTA. EDTA-induced conformational changes in platelet membrane glycoproteins, particularly GPIIb/IIIa, may expose cryptic epitopes that react with naturally occurring autoantibodies, leading to platelet clumping and spuriously low automated platelet counts. Such aggregation does not reflect true thrombocytopenia in vivo.4,5
Several pre-analytical factors may influence the degree of platelet aggregation, including delayed analysis, transport conditions, storage temperature, and mechanical agitation during sample handling. In the present case, although blood collection times were close, the outsourced samples underwent transportation and delayed processing before analysis, whereas the in-house samples were processed immediately after collection. These differences in sample handling conditions may have contributed to the discrepancy in platelet counts observed between laboratories.
Importantly, both laboratories used the same automated hematology analyzer model (Sysmex XN-1000) with optical platelet counting methodology. Therefore, the discrepancy was less likely to be explained solely by differences in analytical principles and may instead have reflected differences in pre-analytical conditions associated with outsourced sample handling.
In the differential diagnosis of thrombocytopenia, conditions such as immune thrombocytopenia, drug-induced thrombocytopenia, bone marrow disorders, disseminated intravascular coagulation, and infection-related thrombocytopenia should be considered. However, the absence of bleeding manifestations, stable platelet counts in repeatedly analyzed in-house samples, and normal coagulation-related findings supported a non-pathological explanation in this case.
From a clinical perspective, failure to recognize EDTA-dependent pseudothrombocytopenia may lead to diagnostic confusion, unnecessary hematology referral, repeated blood testing, and inappropriate clinical interventions. Awareness of inter-laboratory discrepancies and pre-analytical variability is therefore important in routine clinical practice, particularly in settings where outsourced laboratory testing is frequently utilized.
This case also reflects the practical workflow of our institution. Blood samples obtained through the outpatient clinic are processed immediately in the in-house laboratory, whereas samples obtained through the Health Management Department are routinely outsourced for analysis. Because platelet counts repeatedly remained within the normal range in immediately processed in-house samples and the patient exhibited no bleeding tendency or clinically significant coagulation abnormalities, additional confirmatory testing using alternative anticoagulants such as sodium citrate was not performed by the attending physicians.
This case has several limitations. First, confirmatory testing using citrate-anticoagulated blood was not performed, and therefore a definitive diagnosis of EDTA-dependent pseudothrombocytopenia could not be established according to the strictest diagnostic criteria. Second, because this was an observational clinical case, the precise contribution of individual pre-analytical factors, including transport conditions and delayed sample processing, could not be independently verified.
Nevertheless, the persistent discrepancy between laboratories, the reproducible normalization of platelet counts in immediately processed in-house samples (Table 1), and the absence of clinical evidence of thrombocytopenia collectively support the interpretation that pre-analytical factors contributed substantially to the observed platelet count discrepancy.
Conclusion
Marked discrepancies in platelet counts between laboratories may reflect pre-analytical artifacts rather than true thrombocytopenia. Careful assessment of sample handling and time-course variation is essential to avoid misdiagnosis and unnecessary investigations or treatment. Awareness of pre-analytical factors remains crucial in hematologic diagnostics.
Footnotes
Ethical considerations
Ethical approval was not required for this case report according to institutional policy.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.