
Abstract
Recreational drug use in Canada is not uncommon, but as with most societies, illegal drug use carries harsh penalties resulting in a criminal record when an individual is successfully prosecuted. Popular drugs of use in Canada include ecstasy, cannabis (including some synthetic cannabinoids sold as ‘Spice’ and ‘Incense’) and several emerging psychoactive ‘legal highs’. Surprisingly, Canada is a major manufacturer and exporter of the popular club drug ecstasy, with criminal gangs organising the synthesis and distribution of this club drug worldwide. Over the last 18 months, there has been much interest in and use of alternatives to ecstasy due to contamination of ecstasy during synthesis. One particular contaminant, paramethoxymethamphetamine (PMMA), has resulted in several deaths. Other alternatives include piperazines and mephedrone analogues. With regard to cannabis, some is home grown within people’s properties, but there is also large-scale cultivation in British Columbia where the climate is more temperate. With the introduction of corporate drug screening, there is increasing use of synthetic cannabinoids to avoid detection of marijuana use. This article discusses the problems and trends of synthetic drug use in Canada and reflects on the limited education available to youth in this regard.
Keywords
Ecstasy use in Canada
Canada is the second largest country in the world and has a relatively small population of 35 million people, with many citizens from diverse ethnocultural backgrounds, including a rapidly rising Aboriginal population (Statistics Canada, 2012). Given this small population and Canada’s international profile as a peaceful and friendly nation, Canada is not the first nation that comes to mind when one thinks of ecstasy use. According to the Canadian Alcohol and Drug Use Monitoring Survey (CADUMS), the use of the street drug known as ecstasy (3,4-methylenedioxymethamphetamine or MDMA) by young adults has not increased in recent years and in 2011 was down to 0.7% of participants surveyed compared to 1.1% admitting use in 2004 (CADUMS, 2011). To put this figure into perspective, in 2011, 9.1% of respondents surveyed aged 15 years or older admitted using cannabis (CADUMS, 2011). Therefore, it may come as a surprise to learn that Canada is one of the largest manufacturers and exporters of ecstasy tablets. As the Royal Canadian Mounted Police (RCMP), Canada’s national police force, states, ‘Within a two year period, Canada has reversed its Ecstasy supply pattern status from an import and consumer nation since the mid-1990s, to a major production and export country’ (RCMP, 2006). As an example, at that time, the seized amount of MDMA (the main component drug in ecstasy) by the authorities was 65 kg with a street value of just over $13 million and around 3 million pills valued at $15 million (RCMP, 2006). In this same time period, there was also a major seizure of 2.5 metric tonnes of 3,4-methylenedioxyphenyl-2-propanone (the precursor material for synthesising MDMA), from a marine cargo vessel (RCMP, 2006). That year, the RCMP reported numerous organised crime groups of Asian origin that were running the synthesis and distribution of ecstasy across Canada.
A more recent report by the RCMP (2009) indicates that the situation with respect to synthesis, distribution and export of ecstasy is rapidly escalating. For example, the RCMP state that ‘practically all of the MDMA seizures at Canadian points of entry in 2009 involved outbound shipments en route to global destinations, as seen in previous years’ (RCMP, 2009). Other police statements detail how MDMA is shipped from Canada to cities in the United States, for example, from Windsor, Ontario to Detroit, Michigan and that Taiwanese authorities seized over a quarter of a million ecstasy tablets from an air cargo shipment delivered from Vancouver (RCMP, 2009). The RCMP also describes how N-benzylpiperazine (BZP) shipments were being imported into Canada and how piperazines were being used as legal substitutes for MDMA. For further discussion of the drug BZP see below, but as a previously legal alternative to MDMA, BZP and related piperazines have represented a thriving and very lucrative business in the ‘party pill’ scene (http://party-pill.biz/html/pfpp__parafluorophenylpiperazi.html).
Despite the prevalence of laboratories involved in the illicit synthesis of ecstasy, reports from the Canadian Centre on Substance Abuse indicate that ecstasy use is still not that common, with several key Canadian cities having more problems with alcohol and cannabis use (Bell et al., 2011; Toronto Drug Strategy Secretariat, 2010; Winnipeg Site Network Team, 2011). Such reports support the notion that a stable home grown market for ecstasy exists, and the over-production of MDMA in Canada is being used for very profitable export. This finding is confirmed by a recent United Nations Office on Drugs and Crime report, which states, ‘Currently, the main source of Ecstasy on the North American market is organized crime groups in Canada’ (UNODC, 2011; see also www.unodc.org/documents/data-and-analysis/WDR2010/AllLabSeizures.pdf).
Legal status of MDMA
In Canada, MDMA is illegal under the Controlled Drugs and Substances Act (S.C. 1996, c. 19) (The Act). The Act places drugs under different schedules such that Ecstasy is Schedule III, which means being found guilty of possession carries potentially harsh consequences. The Act states:
Every person who contravenes subsection (1) where the subject-matter of the offence is a substance included in Schedule III
is guilty of an indictable offence and liable to imprisonment for a term not exceeding three years; or is guilty of an offence punishable on summary conviction and liable for a first offence, to a fine not exceeding one thousand dollars or to imprisonment for a term not exceeding six months, or to both, and for a subsequent offence, to a fine not exceeding two thousand dollars or to imprisonment for a term not exceeding one year, or to both (http://laws-lois.justice.gc.ca/eng/acts/C-38.8/FullText.html).
Not surprisingly, Canadian legislation with reference to amphetamines mimics, to some extent, United Kingdom law. However, there is a critical difference in that the Canadian Act contains the following wording ‘Amphetamines, their salts, derivatives, isomers and analogues and salts of derivatives, isomers and analogues including’ which is followed by a list of many substances, many of which are not amphetamines, for example: lysergic acid diethylamide (LSD), harmaline, psilocin and psilocybin. As of 2012, the list also includes the piperazines 1-benzylpiperazine (BZP) and trifluoromethylphenylpiperazine (TFMPP).
In Canada, researchers must have specific and detailed scientific exemptions from Health Canada to engage in research on each of the above named substances, including research involving MDMA and piperazines. To a pharmacologist, the idea of an analogue being compared in pharmacological terms to the parent molecule may be problematic. The basis of pharmacology is that small changes to the structure of a drug can result in a new molecule with remarkably different therapeutic properties. For example, phenylethylamine (PEA) is a simple molecule found in many foods including chocolate. PEA differs from amphetamine by a lone methyl group (Figure 1). Clearly, PEA is a closer structural analogue to amphetamine than MDMA; however, that does not mean it fits within the legal control framework. PEA is rapidly broken down after ingestion and has no pharmacological or therapeutic actions under normal circumstances. Figure 1 shows the chemical structures of several PEAs which have a diverse pharmacology with psychopharmacological effects ranging from mild stimulation to hallucinogenic activity through to acute severe toxicity (Hill and Thomas, 2011). This diverse pharmacology reflects a multitude of actions at different targets, which range from inhibition of reuptake of or stimulation of release of one or more monoamine neurotransmitter [serotonin (5-hydroxytryptamine, 5-HT), noradenaline and dopamine], inhibition of monoamine oxidase activity, potent affinity for subtypes of serotonin receptors and also affinity for adrenoceptors. This diversity of pharmacology also makes the health risks of the PEAs hard to pinpoint; but reported adverse effects induced by some PEAs include nausea, vomiting, tachycardia and hypertension (Wood et al., 2007, 2011). Bupropion (Figure 1) is a PEA with a structure very close to that of mephedrone (Figure 2). It is an extremely useful drug, used as an antidepressant and also may be an effective agent for smoking cessation (Stahl et al., 2004). Despite the similarities in structure between mephedrone and bupropion, recreational use of bupropion is very rare (McCormick, 2002), demonstrating that like structures do not necessarily have similar pharmacological properties. In summary, the Canadian Controlled Drugs and Substances Act (S.C. 1996, c. 19) has been amended to take into account some of the emerging new psychoactive substances such as the piperazines and methylenedioxypyrovalerone by specifically naming them in the Act. However, given the rate at which these new designer drugs appear via the web or by other means, it will be interesting to determine if regular amendment is a viable long-term solution or whether new legal sanctions are needed.
Chemical structures of MDMA, PMMA, PEA, bupropion, BZP and TFMPP.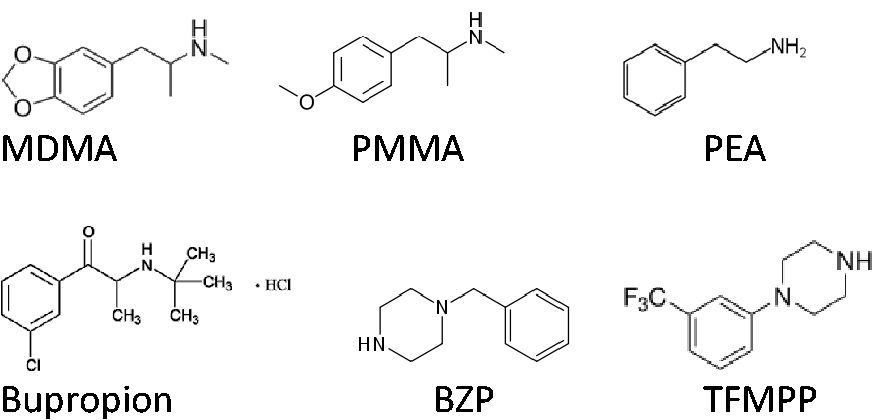
Ecstasy-related toxic syndromes
Death from overdose of ecstasy or MDMA may include serotonin syndrome, which if left untreated can lead to organ failure and death (Silins et al., 2007). Central hyperthermia is a key component of the serotonin syndrome. There is also evidence to indicate that MDMA can mediate peripheral vasoconstriction via activation of alpha-1-adrenoceptors, so reducing heat loss (see Docherty and Green, 2010). Ecstasy use can also affect the hypothalamic pituitary adrenal axis and therefore cortisol secretion (Parrot et al., 2013; Wolff and Aitchison, 2013; Wolff et al., 2012) and also increase secretion of antidiuretic hormone (Wolff et al., 2006). It may also induce malignant hyperthermia-like syndrome with rhabdomyolosis, a condition in which skeletal muscle breaks down to release toxic by-products (Demirkiran et al., 1996). This article does not review the various serotonin toxic syndromes, but there are numerous case reports detailing the symptoms and treatment of adverse reactions to ecstasy (Burgess et al., 2000; Silins et al., 2007) and evidence of genetic factors that may increase the vulnerability to these (Aitchison et al., 2012; Russell et al., 2012; Wolff et al., 2012).
Clinical use of MDMA
In contrast, there is evidence that MDMA administered in a clinical setting may have therapeutic value, particularly in the treatment of post-traumatic stress disorder (Mithoefer et al., 2011; Oehen et al., 2013). The risks of ingestion remain a hot topic, with many debatable observations with regard to the efficacy and safety of the use of MDMA (Green et al., 2012). Several preclinical papers have examined the effects of MDMA on the serotonin system, including some reports indicating serotonin depletion in the brain and long-term changes in serotonergic transmission (for reviews, see Green et al., 2004; Lyles and Cadet, 2003). At the clinical level, there are concerns that the regular use of MDMA may result in psychological problems and cognitive impairments that are not reversible (Morgan, 2000). There are several major misconceptions concerning the modern day use of ecstasy or ‘E’. One such misconception is that only excess serotonin released in the brain gives the user the psychostimulant effect. Importantly, dopamine and noradrenaline are also released and probably contribute not only to the euphoric effects but also the toxic effects of MDMA (Docherty and Green, 2010; Green et al., 2004; Hudson et al., 2011).
Contaminated ecstasy
We know that MDMA is used on a regular basis by many youths and yet relatively few deaths occur; however, tragically some first time users do suffer serious side effects. There may be a genetic component due to some people being poor metabolisers of MDMA and more susceptible to the drug’s toxic effects (Aitchison et al., 2012). Contaminants of ecstasy exist and are associated with mortalities. A major misconception is that ecstasy bought on the street contains only MDMA. In fact, street ecstasy is rarely pure MDMA; rather, MDMA is often combined with other stimulants. In 2007, according to the Health Canada Drug Analysis Service, only 3% of seized ecstasy tablets contained pure MDMA compared to 69% in 2001. One such common stimulant is para-methoxymethamphetamine (PMMA), which has been associated with several recent deaths in Canada and is a confirmed contaminant found in some ecstasy pills. In the past two years, it has caused severe serotonin toxicity in some users of ecstasy (Lurie et al., 2012; Vevelstad et al., 2012). PMMA is a close analogue of MDMA (Figure 1) and tablets inscribed with a Mitsubishi 3 diamond logo often contain another contaminant, para
Our increasing interest in ecstasy use followed the deaths in Edmonton of several young girls who had taken the drug for recreational use. In 2009, a group of teenagers on a First Nations Reserve east of Edmonton were at a wedding party. Several girls aged 14 and 15 years took ecstasy pills and rapidly became sick and two girls later died after admission to hospital. At the court case where a 17-year-old was prosecuted for supplying the ecstasy pills, Parkland County paramedic Anya Howard stated that before one of the girls lost consciousness she was able to speak with her. ‘I asked her how many pills she had taken, she replied that she took three ecstasy pills’. The following court testimony is from a girl who survived the incident despite taking ecstasy at the same party. ‘She was telling me that something was wrong and that she was going to die’. The girl also reported seeing another 15-year-old girl in the same washroom. According to her statement, that individual was already high at that point. The girl said they each took another pill (Edmonton CTV news, 2010. http://edmonton.ctvnews.ca/grandmother-of-victim-testifies-in-overdose-case-1.499733 and http://edmonton.ctvnews.ca/trial-commences-for-youth-in-overdose-case-1.499422#ixzz2CQVbHtV1).
That a person so young would take three ecstasy pills suggests that better education is needed to inform youth of the serious harms of ingesting recreational drugs. The following month, two more young girls, this time even younger, at 14 years old, overdosed on ecstasy tablets at a popular West Edmonton Mall ‘Rock “n” Ride’ dance party. Tragically, one of the girls died. At the court case where the dealer was prosecuted, a friend of the girls reported that they took six pills each at the dance prior to collapsing. Why any youth would take so many pills is unclear; however, the risks of drug use are very clear and need to be taught at some level and clearly during early teenage years. Around the same time period as these tragic deaths, the authors became aware that ecstasy tablets were increasingly contaminated with other substances. As far as we can ascertain, the aforementioned deaths were from complications arising from overdose of MDMA and not from contaminants, although local press were quick to publish rumours of ‘tainted ecstasy’ circulating on the streets of Edmonton. In contrast over the past two years, as many as eight deaths in the province of Alberta may be related to PMMA- and PMA-contaminated ecstasy pills (Jones, 2013, personal communication). Next door in British Columbia, the most reliable figure is most likely five cases out of 18 recent deaths associated with ecstasy use. Interestingly, this is not the first time PMA-related deaths have occurred in Canada. Almost 40 years ago, there was a spate of deaths where PMA was identified as a toxic form of ecstasy (Cimbura, 1974).
Given these tragic and well-publicised ecstasy-related deaths, the RCMP in both Alberta and British Columbia has launched a very successful public awareness campaign about the dangers of using ecstasy. With the ensuing widespread media coverage and ongoing warnings from the RCMP about contaminated ecstasy, perhaps it is not surprising that ‘users’ have turned to alternative ‘legal highs’ where the products are sold as ‘pure’, but ‘not for human consumption’, thus circumventing laws pertaining to controlled substances.
Legal highs
Legal highs, including the aforementioned piperazines (Figure 1), have been increasingly used as alternatives to illegal drugs so that users can seek out a psychoactive experience without fear of being criminally prosecuted. Contact with the local RCMP revealed that piperazines were found in tablets that had been seized and analysed in Alberta and British Columbia (Sergeant Lorne Adamitz, 2011, personal communication). BZP was found mixed with MDMA in some pills; also pills containing BZP and TFMPP, but no MDMA have been identified. Internet websites that offer an analytical service on a fee basis, but publicly report their findings, also reported the presence of BZP and TFMPP in tablets, particularly those shaped like the heads of Bart and Homer Simpson (Ecstasydata.org, 2009). One assumes such designs are used to attract a younger market where users can covertly ask for a ‘Bart’. Few, if any, deaths are reported to have occurred in Canada from BZP and TFMPP poisoning, although it is possible that toxicological tests are frequently not requested for these contaminants. Until early 2012, BZP and TFMPP were uncontrolled substances in Canada and were thus widely available on the Internet and from Headshops selling ‘party pills’. There are also web-based companies selling ‘research chemicals’, typically in 1 g quantities. These companies sold an array of piperazines and PEAs including cathinones. To ascertain the quality of these legal substances, one of the authors purchased some research chemicals online and found them to be of high purity. Until very recently, one could also freely import large quantities of piperazines from Asia and process them into pills that were then labelled ‘not for human consumption’. Although once legal in Canada, there have been several seizures and prosecutions of persons attempting to export these same substances from Canada into the US, where BZP and TFMPP have been banned for several years. Perhaps one of the most striking cases was that of a Canadian citizen Krysta Edwards who was prosecuted in a U.S. District Court in Seattle for taking 26 kg of BZP across the border from Canada into the States. At the time of her arrest in June 2009, BZP was still legal in Canada but controlled in the U.S. According to the prosecution, the trip was one of a dozen border crossings to smuggle drugs (The United States Attorney’s Office, Western District of Washington, 2010; http://www.justice.gov/usao/waw/press/2010/mar/edwards.html). Edwards is now serving five years in prison for possession of BZP with intent to distribute. This appears to be a harsh sentence, but apparently Krysta Edwards was part of a team of organised smugglers who were transporting up to 50,000 pills per trip and in her sentencing memo Assistant United States Attorney Ms Crisham wrote ‘she was entrusted with picking up the proceeds and managing (others)….Edwards was clearly given a significant amount of responsibility within this organisation and played a much greater role than the typical drug “mule”’.
Until recently, there has been little systematic study of these ‘legal highs’. While the effects of MDMA on brain neurochemistry have been widely studied in animals, there are few studies on the effects of the piperazines BZP, TFMPP and meta-chlorophenylpiperazine (mCPP) (Baumann et al., 2005). Brain microdialysis in rodents involves implantation of minute probes into specific brain areas under anaesthesia. Probes are perfused with artificial cerebrospinal fluid and small molecules pass through the membrane and can be collected for analysis by high-performance liquid chromatography. In this manner, researchers receive a much better understanding of what legal highs are doing to brain monoamines such as serotonin, dopamine and noradrenaline (which are chemical messengers in the brain) and are also able to record how these substances affect rat behaviour. To date, Baumann’s group have used this technique to show that BZP mimics the neurochemical effects of MDMA in rats in vivo (Baumann et al., 2005). However, that study only observed effects on dopamine and serotonin release. In our own brain dialysis studies, we have found that BZP elevated not only extrasynaptic levels of dopamine and serotonin, but also of noradrenaline in rat frontal cortex (Hudson et al., 2011). Furthermore, we found that combining BZP with MDMA had additive effects on these monoamine levels (Hudson et al., 2011). Our data would suggest that combining piperazines with MDMA in a pill form could, when directly ingested, lead to serotonin syndrome coupled with sympathotoxicity.
While BZP and TFMPP are still popular, over the past couple of years other legal highs have emerged. For example, there have been numerous media stories of people taking ‘Bath Salts’ or ‘Plant Food’ to get high. These packages of substances have been sold openly and over the counter in many legitimate businesses and usually contain cathinone analogues such as mephedrone (4-methylmethcathinone) or methylone (Figure 2) (Carhart-Harris et al., 2011; Kelly, 2011; Spiller et al., 2011; Wood et al., 2011). Mephedrone was synthesised in 1929 but was used in Israel in 2000s to control aphids on plants (hence the term ‘plant food’). It was then used by young people in Israel initially as a legal high until it was banned, then appearing in the UK with names such as ‘miaow miaow’ and ‘drone’ (Nutt, 2012). Other legal highs in Canada include other cathinone derivatives such as butylone and ethylone (Figure 2), both of which have a strong structural resemblance to MDMA (see Figure 2). In fact, several of these cathinones were not and are not legal; they are considered by Health Canada to be covered by the Controlled Drugs and Substances Act (S.C. 1996, c. 19). Methylenedioxypyrovalerone (MDPV, Figure 2), which is often found in ‘bath salts’, has received much recent attention for inducing a ‘Zombie like state’, which has been played up by the press following a high profile case in the US where an individual was reported to have eaten the face of a homeless person. The ‘zombie-like’ individual was shot by police and later tested negative for MDPV. Indicative of this media-induced ‘zombie panic’, when another suspected case of bath salts poisoning appeared in Halifax in June 2012, a public warning was issued by The Canadian Centre on Substance Abuse Use (see http://www.ccsa.ca/2012%20CCSA%20Documents/CCSA-CCENDU-Drug-Alert-Bath-Salts-2012-en.pdf).
Chemical structures of mephedrone, methylone, butylone, ethylone, MDPV and 6-APB.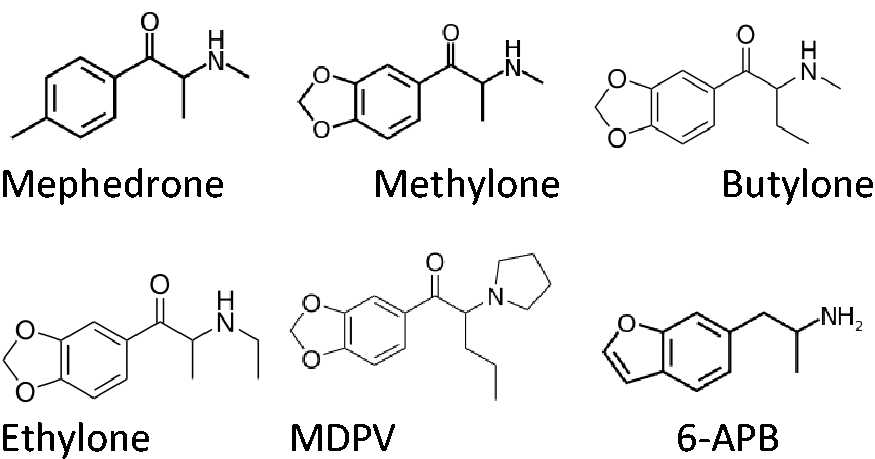
More recently, and perhaps directly because of this reported ‘zombie effect’, MDPV was specifically added to the list of controlled substances in Canada. Perplexingly so since, as a pyrovalerone structure, it is not considered a close analogue of 4-methylmethcathinone. Pyrovalerone analogues were synthesised as medications to treat cocaine dependency (Meltzer et al., 2006) but it seems unlikely following the adverse publicity surrounding MDPV that any of the 38 analogues synthesised will be developed further. Perhaps the move to classify and control MDPV was driven more by the numerous, and often sensational, stories about people turning into ‘zombies’ than by good science. This media sensationalism in part mimics recent events in the UK where press reports appear to have influenced politicians and the law-making process (Nutt, 2011).
It would appear that a game of ‘cat and mouse’ is now under-way, as there are several other designer drugs that are close analogues of these compounds designed to keep ahead of criminal legislation. Exactly what is now covered is open to interpretation of the Act. In fact, some of these legal highs are not all that new. Many were synthesised and published on several years ago (Glennon et al., 1985; Monte et al., 1993). In several studies, several methylenedioxy substituted analogues were examined and shown to be amphetamine-like (Dal Cason et al., 1997; Glennon et al., 1987, 1988; Monte et al., 1993). Why these substances have become popular now is open to debate, but one can surmise that impure ecstasy may have played a determining role for some users, while others may be seeking a chemical-induced ‘legal high’ without the threat of criminal prosecution.
Currently, ‘Spice’ and ‘K2’ have become popular alternatives to cannabis and are sold in Headshops or widely available online in Canada as ‘incense for burning’. Given the availability of cannabis in Canada, the popularity of these alternatives is at first glance somewhat surprising. Cannabis is available in Canada for medical use and is subject to Federal law (http://laws-lois.justice.gc.ca/eng/regulations/SOR-2001-227/), but it is not available for recreational use.. Cannabis is classified as Schedule II by law, and being guilty of non-medical use carries significant penalties:
Punishment
(4) Subject to subsection (5), every person who contravenes subsection (1) where the subject-matter of the offence is a substance included in Schedule II is guilty of an indictable offence and liable to imprisonment for a term not exceeding five years less a day; or is guilty of an offence punishable on summary conviction and liable for a first offence, to a fine not exceeding one thousand dollars or to imprisonment for a term not exceeding six months, or to both, and for a subsequent offence, to a fine not exceeding two thousand dollars or to imprisonment for a term not exceeding one year, or to both (http://laws-lois.justice.gc.ca/eng/acts/C-38.8/FullText.html).
To what extent this law is enforced is difficult to ascertain, but a recent report indicates that since the Conservative party gained power in Canada in 2006, arrests for possession have jumped 41% (MacQueen, 2013). The same report states that since then there have been 405,000 marijauna-related arrests and that in 2010 of 75,000 arrests only around 10% of those resulted in conviction. It further states that according to a public opinion survey by Angus Reid, 66% of Canadians expect marijuana to be legalised within the next 10 years (MacQueen, 2013). The cultivation and use of cannabis is common, and for British Columbia, located on the west coast of Canada, which has a temperate climate, production of marijuana is ranked second place for its contribution to the provincial gross domestic product. Companies such as Island Harvest (http://www.islandharvest.ca/) openly advertise that they ‘cultivate and distribute a range of medical cannabis hybrids to suit your therapeutic needs’. Recently, there has been a surge in drug testing of heavy equipment workers in the Oil sands of Fort McMurray, Alberta (MacDermott, 2012). Currently, these tests do not detect JWH-018 (naphthalen-1-yl-(1-pentylindol-3-yl)methanone), which is a cannabinoid agonist found in Spice and K2. To avoid detection, individuals are using this cannabis alternative JWH-018, without fear of losing their job.
Future legal highs
In 1993, David Nichols’s group published a series of MDMA analogues they had synthesised with the aim of developing an entactogen without serotonergic neurotoxic effects (Monte et al., 1993). One particular analogue, 6-(2-aminopropyl)benzofuran (6-APB), perhaps better known as Benzo fury (Figure 2) has become a popular replacement for MDMA. Based on a benzofuran structure it is not an analogue of amphetamine, but it does inhibit the accumulation of the biogenic amine neurotransmitters serotonin, dopamine and noradrenaline into brain synaptosomes (nerve endings) (Monte et al., 1993). 6-APB is unscheduled in the US and may or may not be legal in Canada depending on how one interprets the current Act. As an example, we have been able to purchase 6-APB from a commercial drug retailer (Toronto Research Chemicals) that supplies academic institutions with a wide range of substances including controlled drugs that require an exemption from Health Canada as part of the purchasing process. The purchase of 6-APB did not require an exemption from Health Canada, indicating that 6-APB is not covered by legislation. Other substances have recently appeared on web sites. For example, adrafinil is openly sold online (http://peaknootropics.com/shop/adrafinil/).. It is legal and is metabolised to modafinil which is a behavioural stimulant (Milgram et al., 2000). Whether adrafinil has quite the desired properties of a recreational drug remains to be seen.
As has been discussed by many others, legislation does not deter drug use and has prompted calls for improved education rather than criminalisation (Nutt, 2011). In 2011, a number of experts in drug policy formed the Canadian Drug Policy Coalition (CDPC). Based at Simon Fraser University in British Columbia, the Coalition has published a document titled ‘Changing the Frame: A New Approach to Drug Policy in Canada’ (Oscapella, 2012), which puts into perspective Canada’s current legislation, its challenges and the problem of recreational drug use in Canada. Insightfully, the CDPC sets out five key points and areas for open public debate:
Adopting a comprehensive health, social and human rights approach to substance use. Providing leadership in harm reduction. Pressing for an end to the criminalisation of people who use drugs. Looking beyond drug prohibition to alternative approaches to regulating and controlling drugs. At the local, national and international level, promoting the human rights of people who use drugs.
In some respects this is a similar stance taken by David Nutt and colleagues in the UK where they have pointed out the problems of banning substances without evidence and the effects of criminalising users of less harmful drugs (Nutt et al., 2011, 2013). Whether change will happen under the current government in Canada is debatable, but it is interesting to note that while this article was being written, two US states voted to regulate the recreational use of cannabis (and retain President Obama for a second term of office). Canadian recreational drug use appears to be a hybrid of European and United States problems, a plentiful supply of drugs and not too many users combined with little public education about the realities of substance use; and this is perhaps the most toxic mix.
Footnotes
Acknowledgements
The authors thank Gail Rauw for technical assistance and the analysis of ‘legal highs’.
Conflicts of interest statement
The author(s) declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Alan Hudson and Glen Baker received funding from Canadian Institutes of Health Research (CIHR No 105833) to investigate the neurochemical effects of designer drugs in rodents. Dr. Aitchison holds an Alberta Centennial Addiction and Mental Health Research Chair, funded by the Government of Alberta.