
Abstract
Background
The potential benefits of ayahuasca on mental health conditions are well documented. This pilot study is the first to explore whether there is an association with ayahuasca use and reductions in inattention, hyperactivity and impulsivity, the core features of attention-deficit/hyperactivity disorder.
Methods
In this exploratory, observational pilot study, the Adult Attention-Deficit/Hyperactivity Disorder Self-Report Scale was administered to 49 adults (23 males, 24 females, two participants did not report their sex) prior to and following the completion of ayahuasca retreats facilitated by the Ayahuasca Foundation in Iquitos, Peru. Only four participants self-reported having a diagnosis of attention-deficit/hyperactivity disorder. Participants attended either an 8-day (four to five ceremonies), 2-week (six ceremonies), 3-week (eight ceremonies) or 4-week (three to 11 ceremonies) retreat.
Results
Inattention, hyperactivity/impulsivity and total scores significantly reduced following an ayahuasca retreat, irrespective of the length of that retreat and the number of ceremonies participants attended.
Conclusions
This pilot study is the first to find reductions in self-reported inattention, hyperactivity and impulsivity in a sample of mostly non-attention-deficit/hyperactivity disorder adults following the use of ayahuasca. However controlled trials are required to determine causality. Research and clinical implications are considered.
Introduction
Ayahuasca is commonly used by the indigenous peoples of the Northwestern Amazon for a variety of beneficial purposes, including healing and divination. Traditionally a curandero (shaman) prepares a brew made by mixing the Banisteriopsis caapi vine with another plant agent, most often the leaves of the Psychotria viridis shrub. The main active ingredient of ayahuasca is dimethyltryptamine (DMT).
Only relatively recently has empirical research attempted to explore the benefits of ayahuasca on conditions recognised in Western diagnostic handbooks such as the Diagnostic and Statistical Manual, 5th Edition Text Revision (DSM-5 TR) (American Psychiatric Association (APA), 2022) and International Classification of Diseases, 11th revision (ICD-11) (World Health Organization (WHO), 2019). Benefits of ayahuasca use have been found within clinical and non-clinical populations. For example, depression (Sanches et al., 2016), suicidality (Zeifman et al., 2019), anxiety, panic (Santos et al., 2007) and substance use disorders (Fábregas et al., 2010). Additionally, increases in subjective wellbeing have also been found with ayahuasca use (Lawn et al., 2017). It should be noted that these studies were based on small sample sizes, and, to date, there has only been one placebo-controlled trial exploring ayahuasca's effects on depressive symptoms (Palhano-Fontes et al., 2019). A much larger cross-sectional analysis recently completed by Sarris et al. (2021) found that 78% of those reporting depression (n = 1571) and 70% of those reporting anxiety (n = 1125) prior to taking ayahuasca reported substantial reductions or that their depression or anxiety was ‘completely resolved’ after taking ayahuasca.
Many of these changes have been attributed to the effects of DMT. DMT is responsible for the psychoactive effects of ayahuasca consumption and is known to affect serotonergic receptors (Carhart-Harris and Nutt, 2017). Changes within the serotonergic system may be associated with a number of the mental health conditions referred to previously, such as anxiety (Gordon and Hen, 2004), depression and suicidality (Mann, 1999).
Despite research into the effects of ayahuasca and mental health conditions, and the shared genetic and biological features between mental health conditions and attention-deficit/hyperactivity disorder (ADHD), less is known about the effect of ayahuasca consumption on neurodevelopmental conditions such as attention-deficit/hyperactivity disorder (ADHD). ADHD is described as a ‘persistent’ or on-going pattern of inattention and/or hyperactivity/impulsivity that impairs daily living or typical development (American Psychiatric Association (APA), 2022). Approximately 7% of children experience ADHD (Thomas et al., 2015), and the worldwide prevalence of adult ADHD is 2.8% (Fayyad et al., 2017). Given that variations in serotonergic receptors are associated with the core features of ADHD, namely, inattention and overactivity (Hou et al., 2018), and are impacted by DMT, it would be useful to investigate whether ayahuasca consumption was associated with reduction in ADHD symptoms.
There have been previous studies which found ayahuasca's benefits on personality trait impulsiveness in the context of addiction (Bouso and Riba, 2014; Fernándex et al., 2014; Apud, 2020; Apud et al., 2023), with one study finding no differences in long-term ayahuasca use on trait impulsiveness more generally (Bouso et al., 2012). As for preliminary evidence in other classical psychedelics (e.g., LSD, psilocybin), potential benefits of microdosing (i.e., use of sub-perceptive low doses for therapeutic effects) in alleviating ADHD symptoms have been outlined in a prospective naturalistic study by Haijen et al. (2022), as well as in a bachelor's thesis (Totomanova, 2020). More broadly however, the current literature surrounding microdosing psychedelics has reached little consensus with further research warranted (Ona and Bouso, 2020; Bornemann, 2020), where therapeutic benefits from macro (i.e., moderate to high) doses have been more consistently found for conditions such as anxiety, depression and addiction (Bogenschutz and Ross, 2018). There has been no study to date focusing on the impact of macrodoses of ayahuasca on core features of ADHD, namely, inattention and hyperactivity/impulsivity.
The National Institute for Health and Care Excellence (NICE, 2022) recommend pharmacological interventions as first-line treatment for adults with ADHD. Methylphenidate, which predominantly targets the dopaminergic and norepinephrine systems, is a licensed pharmacological intervention for adults with ADHD. However, the response rate to stimulant medication, like methylphenidate, is variable. For example, ADHD symptom reduction following stimulant medication ranges between 41% and 76% (Reimherr et al., 2007; Spencer et al., 2005), and up to 30% of people do not experience any improvements (Spencer et al., 2004). Therefore, amphetamines, which target dopamine, norepinephrine and serotonin activity (Kuczenski and Segal, 1997), may be more effective in managing ADHD symptomology (Faraone and Buitelaar, 2010), and amphetamines have surpassed prescriptions of methylphenidate in the United States (Safer, 2016).
Aims
This pilot study aimed to explore whether there was an association between ayahuasca use within a traditional shamanic setting and a reduction in self-reported inattention and hyperactivity/impulsivity, the core features of ADHD, in a sample of mostly non-ADHD adults.
Methods
Setting
This study was conducted at the Ayahuasca Foundation in Iquitos, Peru, an ayahuasca retreat and research centre, located in the Amazon rainforest. The primary aim of this establishment is to provide healing through the use of ayahuasca administered legally in a traditional Shipibo setting adapted for tourists. The data was collected as part of a broader research project on the impact of ayahuasca use on mental health (Ruffell et al., 2021), but this pilot paper will focus on inattention and hyperactivity/impulsivity, the core features of ADHD.
Prior to acceptance onto retreats, participants were required to complete an online questionnaire provided by the Ayahuasca Foundation (www.ayahuascafoundation.org), screening for psychiatric and medical history. The Ayahuasca Foundation excludes minors and those with diagnoses of a psychotic condition and/or personality disorder.
Once accepted onto the retreat, each participant was asked to abstain from illicit substances and prescribed medications and to observe dietary restrictions (no red meat, salt, sugar or fat) 2 weeks prior to arrival. Those discovered to be on medication upon arrival, including prescribed ADHD medication, were excluded from attending ceremonies.
Retreats varied in length between 8 days to 4 weeks and the number of ceremonies offered. The 8-day retreat offered five ceremonies, the 2-week offered six, 3-week offered nine and 4-week offered 11. Participants chose for themselves how many ceremonies they wished to attend, which ranged from three to 11. Those who had 8-day retreats joined four (n = 20) or five (n = 8) ceremonies, those with 2-week retreats joined all six ceremonies (n = 5), those with 3-week retreats joined all nine ceremonies (n = 5) and those with 4-week retreats joined 11 (n = 8), eight (n = 1), six (n = 1) or three (n = 1) ceremonies.
Design
The design was an exploratory, observational pilot study. The study was approved by the Ayahuasca Foundation (https://www.ayahuascafoundation.org/). All participants who attended the retreat between January and May 2019 were approached for their consent to participate in the study. Participation was voluntary, and participants were not offered any compensation for their participation.
Ethical approval was acquired (#CLESPsy000893 v2.0), and the study is in concordance with the Declaration of Helsinki.
Sample
Of those attending ayahuasca retreats, 49 adults agreed to take part in the study, and 47 provided demographic information. Self-report psychiatric diagnoses were not confirmed with medical records (see Table 1 for participant demographics).
Participant demographics.
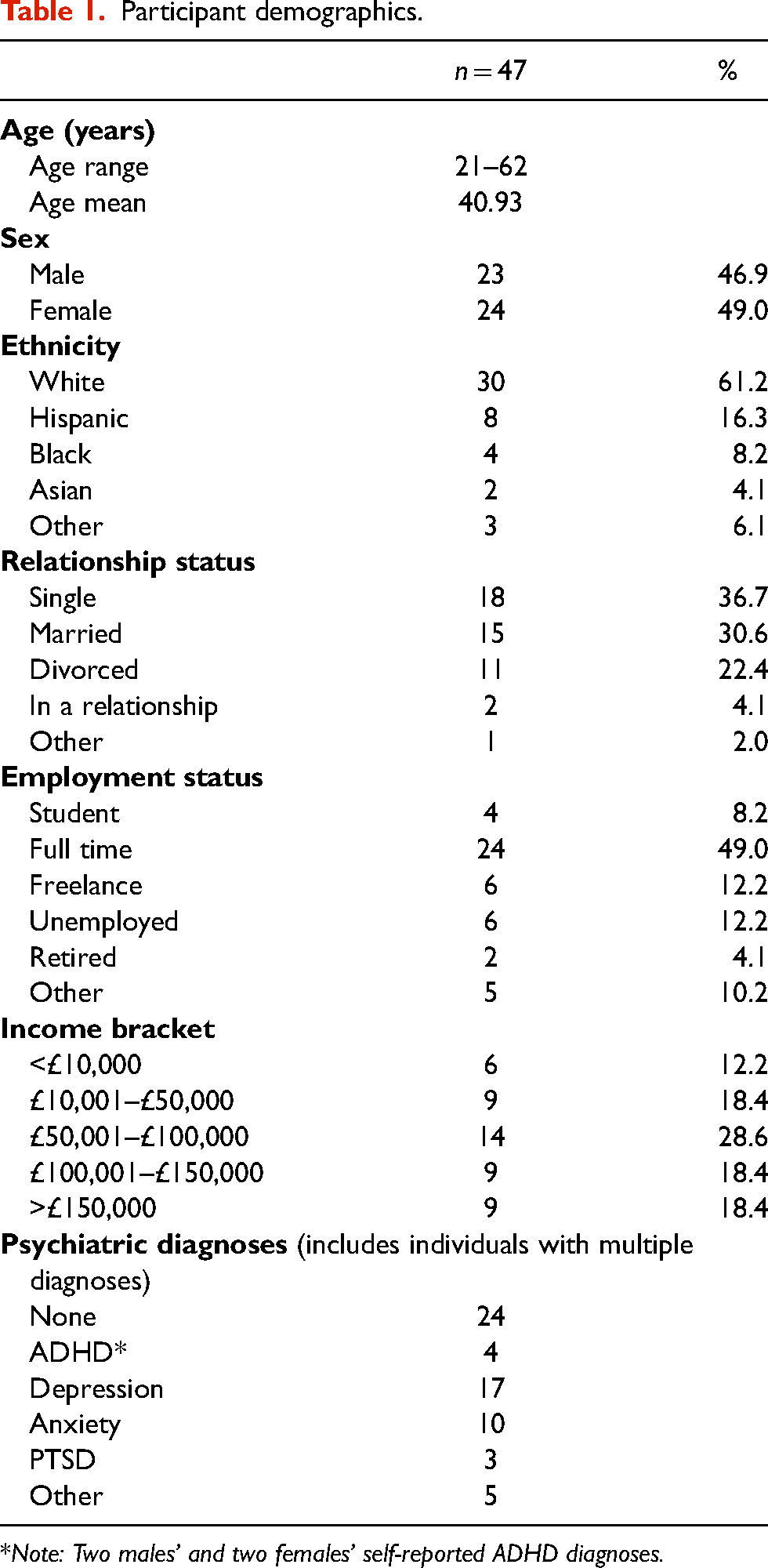
*Note: Two males’ and two females’ self-reported ADHD diagnoses.
Measures
Following informed consent, participants completed the Adult ADHD Self-Report Scale (ASRS) (Kessler et al., 2005) prior to their first ceremony and the morning after their final ceremony. The ASRS is a brief screening instrument to identify current ADHD symptoms. The scale contains 18 ADHD symptoms of inattention, hyperactivity and impulsivity according to the DSM IV-TR and DSM-5 (American Psychiatric Association (APA), 2000, 2013). Symptom severity is reported on a 5-point Likert scale (0–4 = never, rarely, sometimes, often, to very often). The ASRS is widely used in both research and clinical practice and has been shown to have good reliability and validity (Brevik et al., 2020). Brevik et al. (2020) reported ASRS normative scores for the ADHD group as 45.0 (12.6) and controls as 23.0 (9.8).
Data analysis
Statistical Package for the Social Sciences (SPSS) version 28 (IBM, 2021) was used to analyse the data. An alpha level of 0.05 was used for all statistical analyses. Paired sample t-tests were conducted to determine whether there were differences in self-reported inattention, hyperactivity and impulsivity pre- and post- ayahuasca ceremonies for the whole group (n = 49).
Analysis of variance was used to determine whether there were differences between male (n = 23) and female (n = 24) self-reported scores. Following this, separate paired sample t-tests were conducted to determine differences in pre- and post-scores for males and females. Additionally, separate analyses of covariance were conducted to determine whether attending a short retreat (8 days) compared with longer retreats (2 weeks, 3 weeks or 4 weeks) or whether attending fewer number of ceremonies (four) compared with a higher number of ceremonies (more than four) impacted on the difference in mean scores for males and females.
Results
For the whole group, significant reductions were identified in inattention, hyperactivity and impulsivity and total scores with medium to large effect sizes (see Table 2).
Pre- and post-ADHD symptomology (n = 49).

Overall, females reported fewer inattentive and hyperactive/impulsive symptoms than males both before and after their ayahuasca retreat. Compared with males, females reported significantly fewer inattentive symptoms prior to taking ayahuasca (F(1,46) = 4.14, p < .05, η2=.084; medium effect) and significantly fewer hyperactive/impulsive (F(1,46) = 4.86, p < .05, η2=.097; medium effect) and total symptoms (F(1,46) = 4.96, p < .05, η2=.099; medium effect) after taking ayahuasca. To put it another way, females reported fewer inattentive symptoms before taking ayahuasca but reported similar levels of inattention compared with males after taking ayahuasca. The reverse is true for hyperactivity/impulsivity and total scores. Females reported similar levels of hyperactive/impulsive symptoms and total symptom scores compared with males before taking ayahuasca but after their retreat reported significantly fewer symptoms than males.
Both males and females self-reported statistically significant reductions in inattentive, hyperactivity/impulsivity and total scores, all with medium to large effect sizes (Cohen, 2013) (see Table 3).
Pre- and post-ADHD symptomology by sex.

Further, analyses of covariance identified that there was no significant difference to reductions in self-reported inattention, hyperactivity and impulsivity for males and females regardless of the length of retreat (short 8-day retreats compared with longer retreats of 2-/3-/4-week retreats) and the number of ceremonies attended (four ceremonies compared with more than four ceremonies) (see Table 4).
Difference in ADHD symptomology by length of retreat and number of ceremonies attended.

Discussion
To the authors knowledge, this is the first study to explicitly examine the association between ayahuasca use and self-reported inattention, hyperactivity and impulsivity, the core features of ADHD. Prior to completing their retreat, males reported more inattention and hyperactivity/impulsivity than females. The main finding from the study is that following the completion of traditional shamanic ayahuasca retreats, self-reported inattention, hyperactivity and impulsivity significantly reduced for both males and females, all with medium to large effect sizes. The length of the retreat and the number of completed ceremonies did not affect the reported change. In other words, similar changes were found whether someone attended shorter or longer retreats. Compared to other samples in the literature (Adler et al., 2019; Brevik et al., 2020), the pre-retreat scores in this study were generally higher compared to ASRS scores of control groups in other studies but lower than that of ADHD groups, and the post-retreat scores were lower than the control scores in the other studies.
Males self-reported a bigger reduction in inattentive symptoms compared with females following their ayahuasca experience, whereas females reported greater reductions in hyperactive/impulsive symptoms compared with males following participation in a traditional ayahuasca retreat. When looking at the four participants with ADHD in the sample, these participants reported elevated pre-retreat ASRS scores similar to that of ADHD groups in other studies (Adler et al., 2019; Brevik et al., 2020). Three of the participants with ADHD reported large reductions in the total ASRS score (reductions of between 8 and 36 points). On the other hand, one participant reported little difference in the ASRS scores. It should be noted, however, that this is a small subsample, and future studies would benefit from exploring ayahuasca use on ADHD symptomatology in a larger group of adults with a diagnosis of ADHD.
Due to the limitations of this pilot study, the precise mechanisms for change are not known. However, it is possible that DMT's effect on the serotonergic system may have reduced ADHD symptomology (Hou et al., 2018). If this is the case, then it is likely that changes in inattention and hyperactivity/impulsivity are likely to be short-term without engaging in regular ayahuasca ceremonies, similar to what has been found in mental health studies (Santos et al., 2018). However, previous research has also found that psychedelics, such as DMT, stimulate early gene expression that encode transcription factors, which in turn are associated with changes in attention (DeSteno and Schmauss, 2008) and synaptic plasticity (O’Donnovan et al., 1999), suggesting possible structural changes with long-term use. Bouso et al. (2015) found that regular ayahuasca users showed significant differences in cortical thickness in midline structures of the brain and a thinning of the posterior cingulate cortex, an essential node in the default mode network (a network of interacting brain regions that are active when an individual is focused on internal mental-state processes rather than the outside world). Thus, long-term use may lead to long-term changes. Future studies should explore these potential mechanisms of change.
Strengths, limitations and future considerations
The strengths of this study include using a community versus clinical sample and measuring symptoms across the full spectrum of severity. While our sample included a few people with ADHD, it was a small number, and future studies could explore the impact of ayahuasca use on ADHD symptomology in a sample of adults with a diagnosis of ADHD. In addition, the total sample size was comparable with other ayahuasca studies utilising an observational, naturalistic repeated measure design.
However, there are a number of limitations. The absence of a control group prohibits assumptions of causality. Future research should include a control group and a long-term follow-up to infer causality and potential long-term effects of ayahuasca on inattention, hyperactivity and impulsivity. Furthermore, it should be noted that the present group was prone to self-selection and confirmation bias. The generalisability and validity of findings were likely impacted by including only those with the time and financial resource to access the retreat, as well as expectances held related to choosing the treatment, travelling to the jungle and complying with researchers. Future studies in samples representative to the population undergoing randomisation are therefore recommended.
Regarding the ASRS, although it is widely used in both research and clinical practice, it is a brief screening tool for ADHD. Future research may benefit from a more exhaustive measure of ADHD symptomology. The ASRS is also a self-report measure. This requires the participant to have a level of insight into their own differences which can be variable for individuals with ADHD (Mörstedt et al., 2015). Therefore, future research may benefit from a more exhaustive evaluation of ADHD symptoms with the addition of collateral information, such as informant measures.
Equally, this study was of self-reported inattention, hyperactivity and impulsivity, rather than people with diagnoses of ADHD. It is presently unknown whether improvements in ADHD symptoms associated with ayahuasca consumption are mediated through brain systems which are specifically dysregulated in ADHD or whether they reflect indirect or more general effects on cognitive and brain systems involved in mood and anxious arousal.
Furthermore, the context of the delivery of the ayahuasca is particularly important. Ayahuasca was administered within a traditional shamanic ceremonial setting, which had been customised for Western participant groups. Non-pharmacological factors, such as the setting, ceremonial procedure and accompanying supportive appraisal of experience, can lead to placebo effects or indeed non-pharmacological psychotherapeutic effects on mental health outcomes (Uthaug et al., 2021). This emphasises the need for placebo-controlled trials and careful consideration of pharmacological and non-pharmacological components and effects of ayahuasca ceremonies and retreats. Furthermore, the ayahuasca brewing process was not standardised, and therefore the ayahuasca that was administered during ceremonies may have had different levels of DMT. Thus, the findings from this study cannot be generalised beyond the ceremonial context of these specific ayahuasca retreats, the ayahuasca brew that was used and the shaman who presided over it. Further research controlling for DMT levels and different environments, such as clinical versus ceremonial, should be investigated further.
Clinical implications
The recognised benefits of other psychedelic substances, such as methylenedioxymethamphetamine (MDMA) and psilocybin (Carhart-Harris et al., 2021; Mithoefer et al., 2018), have yielded clinical trials for a range of mental health conditions and provided positive outcomes (Feduccia et al., 2018; Vargas et al., 2020). Comparable clinical trials of ayahuasca will help determine its potential value as a pharmacological option and/or as part of an assisted psychotherapy program. Further evidence of the potential benefits of ayahuasca could yield new opportunities for the treatment and management of the core features of ADHD.
Conclusions
This pilot study is the first attempt to explore whether ayahuasca use is associated with reductions in inattention, hyperactivity and impulsivity, the core features of ADHD, in a sample of mostly non-ADHD adults. Although significant reductions were found for both males and females following traditional shamanic ayahuasca ceremonies, further evidence is required to determine causality, mechanisms of change and whether there are long-term effects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Institute for Health and Care Research (grant number CS-2017-17-007).