
Abstract
Background and aims
Recent studies suggest a potential relationship between rosacea and Helicobacter pylori (H. pylori) infection or small intestinal bacterial overgrowth (SIBO), but there is no firm evidence of an association between rosacea and H. pylori infection or SIBO. We performed a prospective study to assess the prevalence of H. pylori infection and/or SIBO in patients with rosacea and evaluated the effect of H. pylori or SIBO eradication on rosacea.
Methods
We enrolled 90 patients with rosacea from January 2012 to January 2013 and a control group consisting of 90 patients referred to us because of mapping of nevi during the same period. We used the 13C Urea Breath Test and H. pylori stool antigen (HpSA) test to assess H. pylori infection and the glucose breath test to assess SIBO. Patients infected by H. pylori were treated with clarithromycin-containing sequential therapy. Patients positive for SIBO were treated with rifaximin.
Results
We found that 44/90 (48.9%) patients with rosacea and 24/90 (26.7%) control subjects were infected with H. pylori (p = 0.003). Moreover, 9/90 (10%) patients with rosacea and 7/90 (7.8%) subjects in the control group had SIBO (p = 0.6). Within 10 weeks from the end of antibiotic therapy, the skin lesions of rosacea disappeared or decreased markedly in 35/36 (97.2%) patients after eradication of H. pylori and in 3/8 (37.5%) patients who did not eradicate the infection (p < 0.0001). Rosacea skin lesions decreased markedly in 6/7 (85.7%) after eradication of SIBO whereas of the two patients who did not eradicate SIBO, one (50%) showed an improvement in rosacea (p = 0.284).
Conclusions
Prevalence of H. pylori infection was significantly higher in patients with rosacea than control group, whereas SIBO prevalence was comparable between the two groups. Eradication of H. pylori infection led to a significant improvement of skin symptoms in rosacea patients.
Background
Rosacea is a chronic facial dermatosis showing erythema and telangiectasia, associated with recurrent inflammatory episodes characterized by oedema, papules and pustules. Prevalence of rosacea in Europe is highly variable, ranging from less than 1% to more than 20% of the adult population. Rosacea affects mainly adults from the third or fourth decade and is predominant in women, although rhinophyma, characterized by irreversible connective tissue and sebaceous gland hypertrophy, occurs mostly in men.1,2 Rosacea is divided into four different subtypes: erythemato-telangiectatic, papulopustular, phymatous, ocular.3,4 There are four stages of rosacea:
I: frequent flushing, irritation caused by topical preparations
II: facial erythema that becomes more persistent, slight telangiectasias, increased skin sensitivity
III: persistent, spreading erythema, oedema, papules, pustules, enlarged pores, ocular changes
IV: tissue hyperplasia, fibroplasias, rhinophyma) and connective-sebaceous hypertrophy may occur with possible deformation of the affected skin in the late stages.
The aetiology of rosacea remains unknown, however it has been observed in some families with a genetic predisposition. Among the mechanisms involved in the pathogenesis, an important role is recognized for innate immunity, vascular changes, free radicals, ultraviolet radiation and microbial agents. 5
Although etiopathogenesis is not fully known, an element commonly found in patients with rosacea is the presence of gastrointestinal disorders. Several studies suggested a potential relationship between Helicobacter pylori (H. pylori) infection, small intestinal bacterial overgrowth (SIBO) and rosacea but this correlation is controversial.4,6,7 Prevalence of H. pylori infection is 25–30% in general population. 8 Some studies reported a higher (i.e. close to 88%) prevalence of H. pylori infection in patients with rosacea and a number of studies reported improvement of rosacea skin symptoms after H. pylori eradication.7,9,10 However, the correlation between H. pylori infection and rosacea is still debated.
SIBO is defined as unexpected microbial concentration (105 colony-forming units/ml (CFU/ml)) in jejunal aspirate culture. Prevalence of SIBO in the general population is found in 2.5–22% 11 while its prevalence in patients with rosacea has been reported to be as high as 46%. 6 In the same study, eradication of SIBO has been associated with a significant improvement in rosacea skin symptoms. However, as for H. pylori infection, there is no consensus on the association between SIBO and rosacea.
This study was therefore designed to assess whether H. pylori infection or SIBO might play a pathogenic role in rosacea. The primary endpoint of this study was to assess the prevalence of H. pylori infection and SIBO in rosacea patients compared with control subjects. The secondary endpoint was to evaluate whether eradication of H. pylori infection or SIBO led to any improvement in rosacea skin lesions.
Materials and methods
Population
Sex and age of the two studied groups
Exclusion criteria were age <18 years, pregnancy, every known gastrointestinal disease, every known surgery to the gastrointestinal tract, use of proton pump inhibitors (PPIs), histamine H2 receptor antagonists, antibiotics or non-steroidal anti-inflammatory drugs (NSAIDs) in the last two months. Neither patients with rosacea or control subjects had significant comorbidities. The study was approved by the institutional Ethical Committee of the Second University of Naples. Written informed consent was obtained from all people participating the study.
Gastrointestinal symptoms assessment
All patients on enrolment were asked to complete two questionnaires about gastrointestinal symptoms. The Short-Form Leeds Dyspepsia Questionnaire (SL-LDQ) was used to investigate upper gastrointestinal symptoms. 12 To investigate lower gastrointestinal symptoms we used a structured questionnaire, focusing on the presence of bloating, flatulence, abdominal pain, diarrhoea and constipation. 13 Both questionnaires assessed frequency and severity of each symptom during the last two months.
Dermatologic assessment
All patients underwent a baseline dermatologic assessment and, those who resulted positive at H. pylori or at SIBO testing, were re-evaluated 10 weeks after the end of therapy. Dermatologic assessment was performed by two dermatologists unaware of the H. pylori or SIBO status of patients.
We used the ‘7-Point Static Score' to evaluate rosacea skin lesions, considering total regression of skin lesions when score was equal to 0 and partial regression when score was from 1–4. 6
Evaluation of H. pylori infection
The 13 C Urea Breath Test ( 13 C UBT) and H. pylori stool antigen test (HpSA) were used to evaluate the presence of H. pylori infection. Diagnosis of H. pylori infection was based on positivity to both tests. Tests were performed after at least two months without antibiotics, PPIs, histamine H2 receptor or NSAIDs therapy. Smoking was not allowed for 12 h before the 13 C UBT. The 13 C-UBT was performed after an overnight fast. A baseline breath sample was obtained, and 100 mg of 13 C urea with citric acid (1.4 g) was administered as an aqueous solution (Expirobacter, SOFAR, Milan, Italy). Another breath sample was collected 30 min later. The test was considered positive if the difference between the baseline sample and the 30-min sample exceeded 5.0 parts/1000 of 13 CO2. All breath tests were analysed at the same laboratory by using a single gas isotope ratio mass spectrometer (ABCA, Europe Scientific, Crewe, UK).
HpSA is an enzyme immunoassay test for in vitro qualitative detection of H. pylori antigens in human stool (Premier Platinum HpSA, manufactured by Meridian Diagnostics Inc., USA), and it was performed at the same day on which the patient performed 13 C-UBT. 14
H. pylori-infected subjects were treated with a 10-day clarithromycin-containing sequential therapy (CLA-ST). H. pylori status was re-evaluated by 13 C-UBT performed at six and 10 weeks after completion of therapy. Infection was considered eradicated if patients had a negative test on both occasions.
Evaluation of SIBO
All patients underwent a glucose breath test (G-BT) to assess the presence of SIBO. Patients received neither antibiotics nor laxatives or NSAIDs in the last 30 days before test. To minimise basal H2 excretion, on the day before G-BT was performed, patients were required to eat only boiled rice with no sausage or cheese, and grilled meat or boiled fish, and to drink only non-gaseous water and to fast for at least 12 h prior to the test. Smoking and physical exercise were forbidden for one hour before and during the test. Immediately before the test, a sample of expired air was taken to assay the basal H2 concentrations, after mouth washing with 20 ml of 0.05% chlorhexidine solution. A dose of 50 g glucose, in the form of iso-osmotic solution, was then administered, and samples were taken every 15 min for 2 h, using a two-bag system EXPIRO-Growth H2 (SOFAR SpA, Trezzano Rosa, Milano, Italy). Samples were analysed immediately using a model Quintron Gas Cromatograph (Quintron Instrument Co., Milwaukee, Wisconsin, USA) evaluating both H2 and CH4 levels. The test established the presence of SIBO when the peak, i.e. the increase over the baseline of H2 levels, was more than 12 parts per million (ppm) in a least two readings.13,15
Patients who resulted positive at the test were treated with rifaximin 400 mg every eight hours for 10 days and performed a new test at one and two months after completion of therapy. SIBO was considered eradicated if patients resulted negative at two consecutive SIBO tests performed with one week interval.
Therapeutic interventions
Patients with H. pylori infection were treated with 10-day CLA-ST (i.e. esomeprazole 40 mg bis in die (b.i.d.) and amoxicillin 1 g b.i.d. for the first five days followed by esomeprazole 40 mg b.i.d. and clarithromycin 500 mg b.i.d. and tinidazole 500 mg b.i.d., for five more days).16,17 Patients with SIBO were treated with rifaximin 400 mg every eight hours for 10 days. 6 Patients with both SIBO and H. pylori infection were treated first for SIBO and then for H. pylori at 4–6 weeks interval from each other. Patients had no topical or systemic therapy for rosacea.
Statistical analysis
A sample size of 86 patients for each study group was calculated for a power of study equal to 90% with alpha error of 0.05, considering that H. pylori infection prevalence is 25–30% in the general population and as high as 88% in patients with rosacea and that 25–50% of patient may improve skin symptoms after eradication. We enrolled, therefore, 90 patients for each group, taking into account possible drop-outs.
Statistical tests employed were Student’s t-test for continuous variables and Pearson uncorrected chi-square for dichotomous variables, odds ratios (ORs) with 95% confidence intervals (CIs) were calculated and a p value < 0.05 was considered significant.
Results
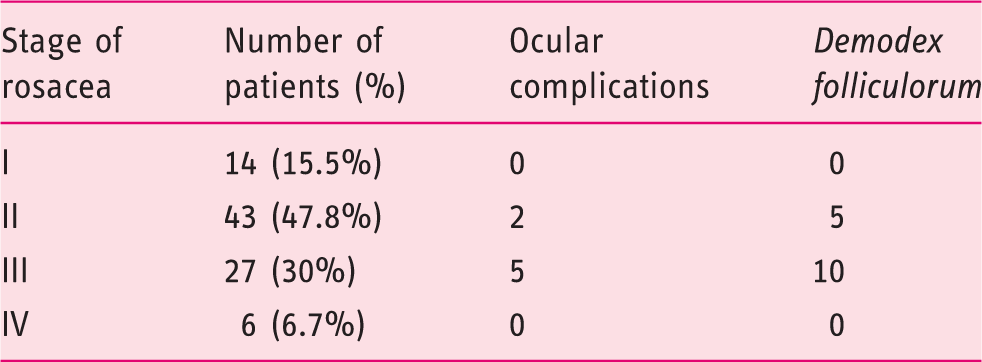
Rosacea patients divided according to the stage of the disease
Prevalence of Helicobacter pylori (Hp) infection and small intestinal bacterial overgrowth (SIBO) in rosacea patients and control subjects

Three rosacea patients were both Hp+/SIBO+.
bOne control patient was both Hp+/SIBO+.
The OR of having rosacea for H pylori-infected subjects was 2.650 (95% CI: 1.414–4.892; p = 0.003), whereas OR for SIBO patients was 1.317 (95% CI: 0.484–3.582; p = 0.794).
The prevalence of upper gastrointestinal symptoms as assessed by the SL-LDQ, showed that 46/90 (51.1%) patients with rosacea had one or more of the following symptoms: indigestion, epigastric pain, nausea, heartburn, regurgitation compared with 22/90 in the control group (24.4%) (data not shown), (OR 3.2, 95% CI: 1.63–6.41, p = 0.0001). Also, 12/90 patients (13.3%) in the rosacea group and 8/90 patients (8.9%) in the control group had one or more of the following lower gastrointestinal tract symptoms: abdominal pain, constipation, diarrhoea, flatulence, bloating (data not shown) (OR 1.57, 95% CI: 0.56–4.49, p = 0.34). In any case, symptoms did not interfere with daily activities. Of the 16 patients with SIBO (nine rosacea patients and seven controls), five had mild lower gastrointestinal symptoms and three had upper gastrointestinal symptoms.
Regression of skin lesions after Helicobacter pylori (Hp) eradication in patients with isolated Hp infection and in patients with combined Hp/small intestinal bacterial overgrowth (SIBO)
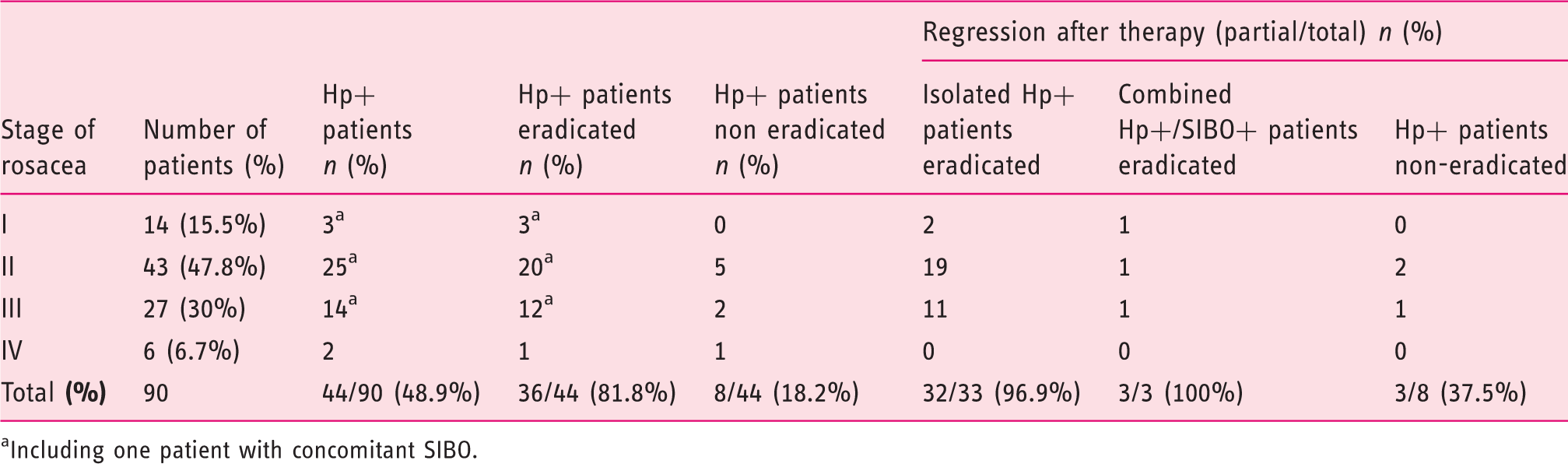
Including one patient with concomitant SIBO.
Regression of skin lesions after small intestinal bacterial overgrowth (SIBO) eradication in patients with isolated SIBO infection and in patients with combined Helicobacter pylori (Hp)/SIBO
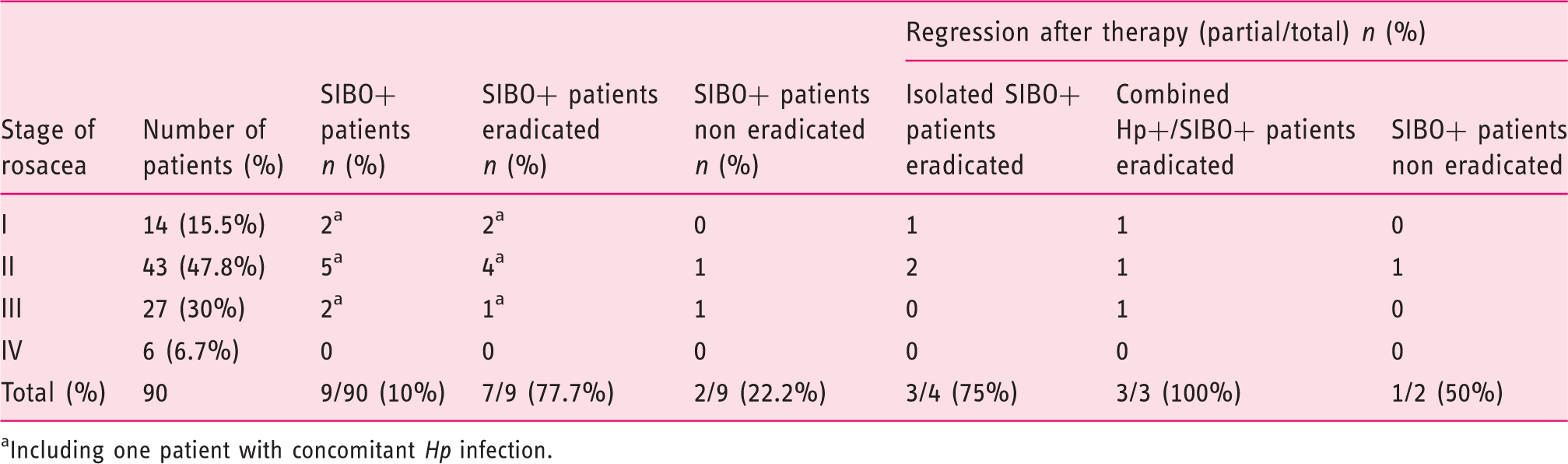
Including one patient with concomitant Hp infection.
All subjects (both rosacea patients and controls) who did not eradicate H. pylori infection were offered a second-line 10-day levofloxacin-containing sequential regimen 16 whereas those patients who did not eradicate SIBO were offered a second-line treatment with metronidazole 250 mg tris in die (t.i.d) for one week. As far as rosacea patients are concerned, both SIBO patients were eradicated of the infection but did not show any improvement in their skin lesions (data not shown). On the contrary, 7/8 H. pylori-infected patients were eradicated of their infection and 6/7 patients showed improvement or further improvement of their skin lesions compared with the evaluation after the first treatment (data not shown).
Discussion
This study suggests that patients with rosacea have a higher prevalence of H. pylori infection compared with controls. Also, eradication of the infection is associated with an improvement in rosacea skin lesions, thus suggesting that H. pylori might be playing a pathogenic role in rosacea.
In our study 44/90 (48.9%) of our patients with rosacea and only 24/90 patients (26.7%) in the control group were infected with H. pylori (p = 0.003), demonstrating a higher prevalence of H. pylori infection in patients with rosacea. We also found that rosacea patients had a significantly higher prevalence of upper gastrointestinal symptoms compared with controls. This is in agreement with a previous report by Szlachcic. 18 This confirms previous reports in favour of a possible pathogenic role of H. pylori in rosacea.7,10 Other studies, however, did not find any significant difference in the prevalence of H. pylori infection between rosacea patients and controls.19–21 This apparent discrepancy might be due to the different method of evaluation of H. pylori infection between these studies and ours (i.e. serology versus 13 C UBT, respectively). To further strengthen a possible pathogenic role of H. pylori in rosacea we evaluated whether eradication of H. pylori infection affected skin lesions of rosacea patients. The eradication rate with sequential therapy in our study was approximately 80%, which is lower than that reported by other Italian studies, 17 but is in agreement with previous report from our group. 22 Eradication of the infection led to a significant improvement in the skin lesions of rosacea patients. In particular, in our study there was a major improvement of rosacea skin symptoms in rosacea stages II and III, with a partial or total regression of skin lesions respectively in 12/14 (85.7%) patients in stage II and in 20/25 (80%) in stage III. Two of these H. pylori-infected patients, one in stage II and one in stage III, had concomitant SIBO, which was successfully eradicated. This difference was not statistically significant. This is in partial agreement with a study by De Miquel et al. who also reported improvement of rosacea skin symptoms after eradication of H. pylori infection. 10 However, in their study the improvement was significantly higher in stage III patients (83.3%), compared with patients in stage II (36.4%). Other studies evaluated whether eradication of H. pylori infection had any effect on rosacea. Several authors demonstrated improvement of rosacea skin lesions after treatment of H. pylori infection.7,9 Other studies could not demonstrate any beneficial effect of H. pylori eradication in patients with rosacea.23,24 Many other authors demonstrated similar results on rosacea skin lesions when an antibiotic treatment of H. pylori infection was compared with placebo because, although antibiotic treatment for H. pylori was successful, eradication of H. pylori did little more than placebo for rosacea.23,24 One may argue that the beneficial effect of H. pylori eradication on rosacea symptoms might be due to non-specific effects of antibiotics rather than H. pylori eradication. However, of the rosacea patients infected with H. pylori who did not eradicate the infection, only 3/8 (37.5%) showed a partial improvement of rosacea skin lesions. This point might have more properly been addressed by treating H. pylori-negative rosacea patients with an eradication regimen, but this would not be ethically acceptable.
The mechanism whereby H. pylori might be involved in the pathogenesis of rosacea is only hypothetical. H. pylori, besides being the major aetiologic factor of peptic ulcer disease and adenocarcinoma of the distal stomach,25,26 is also implicated in a variety of in skin diseases such as chronic urticaria,27–29 psoriasis,30,31 Schoenlein-Henoch purpura,32,33 alopecia areata, 34 atopic dermatitis,29,35 Sweet syndrome, 36 cutaneous pruritus, 37 nodular prurigo, 38 immune thrombocytopenic purpura, 39 lichen planus 40 and aphthous stomatitis.41,42 Recent studies suggest that rosacea is associated with the generation of reactive oxygen species (ROS) that are released by inflammatory cells such as neutrophils. Exaggerated production of ROS or inadequate antioxidant protection creates a condition known as oxidative stress, which is thought to play an important role in skin cancers, cutaneous aging and in many inflammatory skin diseases. 43 In addition, effective treatment of rosacea with antioxidant drugs, either topical or systemic, 44 suggests that increased ROS activity and/or deficient function of the antioxidant system may play a pathogenic role in this setting. Increased ROS activity and decreased plasma antioxidant compounds, such as ascorbic acid, have been detected in H. pylori-infected patients.45,46 It has also been reported that the reduced circulating levels of vitamin C in H. pylori-infected subjects may contribute to the aetiology of some diseases associated with antioxidant deficiency. 43 Additionally, it has been shown that H. pylori may increase serum or tissue levels of nitric oxide (NO),45,46 which is involved in a number of physiological processes in the skin, including vasodilatation, inflammation and immune modulation. Thus, it has been postulated that NO 47 produced by H. pylori might cause the flushing and erythema associated with rosacea, or that it may have a pathogenic role in the inflammation seen in rosacea.
Based on the results of this study, another infectious condition of the gastrointestinal tract, i.e. SIBO does not seem to be pathogenically related to rosacea. In fact, we did not find any difference in SIBO prevalence between rosacea patients and controls. This is in apparent contrast with a previous report showing a significantly higher SIBO prevalence in patients with rosacea compared with control subjects. 6 One possible explanation is that our study was not powered enough for SIBO. Also, geographic differences in SIBO prevalence and instrument differences may account for this apparent discrepancy. It also should be kept in mind that sensitivity and specificity of G-BT in diagnosing SIBO are 62.5% and 77.8%, respectively, compared to the gold standard which remains culture of intestinal aspirates. 48 To further support the lack of association between SIBO and rosacea, we could not demonstrate any significant difference in the improvement of rosacea between patients who eradicated SIBO and patients who did not. In fact, eradication of SIBO was associated with an improvement in rosacea skin lesions in 3/4 patients with isolated (i.e. non H. pylori-associated) SIBO infection. However, also one of the two patients who did not eradicate SIBO showed skin improvement following rifaximin treatment. This questions whether rifaximin by itself might positively affect rosacea patients by interfering with the intestinal microbiota, independently of SIBO eradication.
In this study the intervention is an antibiotic treatment so, based on our data, we cannot exclude the possibility that the true cause of rosacea is gut bacteria other than H. pylori or those involved in bacterial overgrowth. In order to address this point a study of the gut microbiota should be performed.
In conclusion, based on our data, H. pylori infection seems to play a pathogenic role in rosacea and we postulate that H. pylori infection should be searched for and possibly eradicated in this setting. On the contrary, SIBO does not seem to play a role in rosacea. Whether rifaximin may exert positive effects in patients with rosacea needs further focused studies.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgment
The authors thank Diego Pappalardo for his technical assistance.