
Abstract
Male Lower Urinary Tract symptoms (LUTs) and Benign Prostatic Hyperplasia (BPH) provide a significant proportion of the core urologists workload, and will continue to do so for the foreseeable future with an increasingly elderly population. This review sets out to provide an overview of the current understanding around BPH and male LUTs as well as investigations and treatment options.
Keywords
Introduction
In today’s expanding elderly population the significance of benign prostatic hyperplasia (BPH) is becoming more important to the urologist. It has long been established that the prevalence of BPH increases with age, with 50% of men in their 50s and 88% of men in their 80s having histological evidence.1,2
Definitions
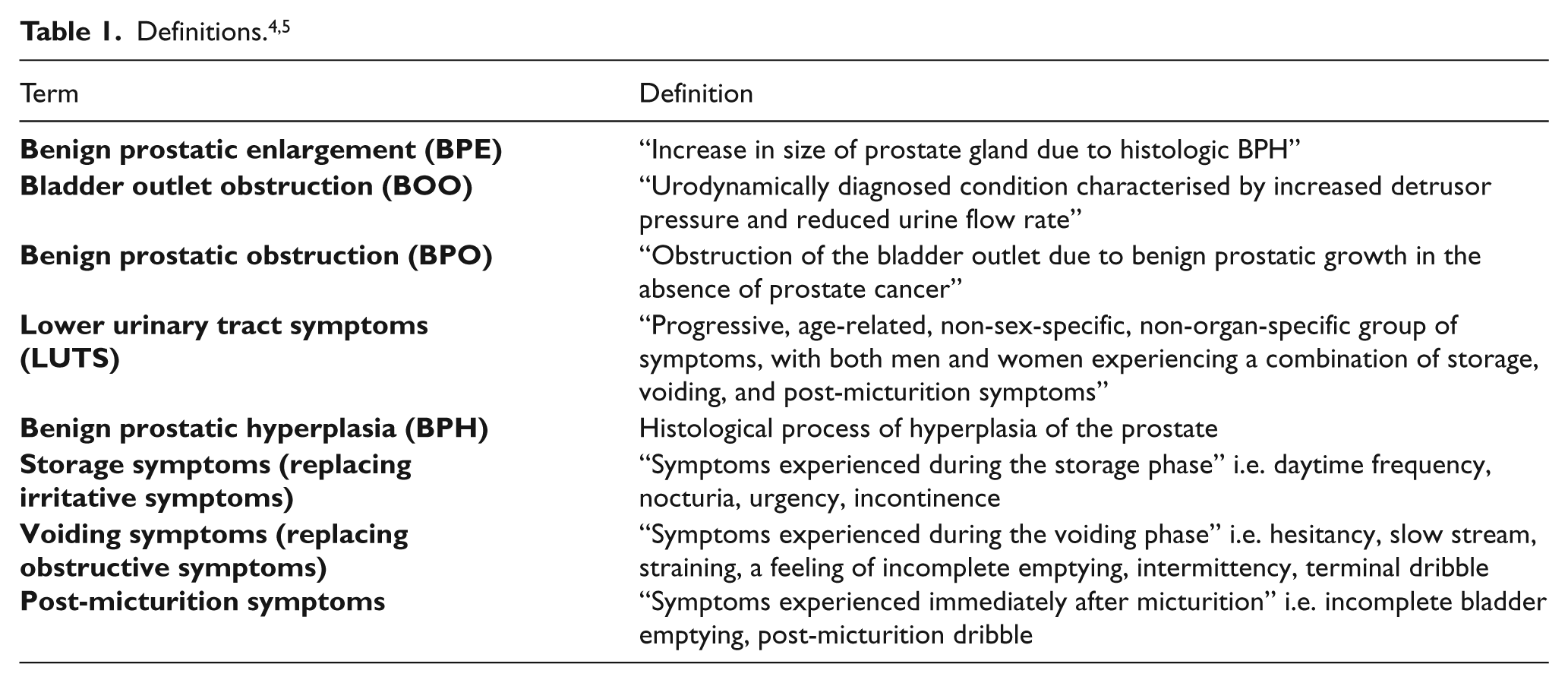
BPH refers to the histological process of hyperplasia of the prostate. The now redundant term prostatism was used broadly to cover the clinical, pathological and pathophysiological elements of BPH and lower urinary tract symptoms (LUTS) and wrongly suggested organ and gender specificity. In response Abrams and Chapple et al., proposed a series of definitions which would more accurately reflect the clinical, pathological and pathophysiological components (Table 1).3,4
Aetiology
It is felt that initially there is an increase in the number of small stromal periurethral and transitional zone glandular nodules secondary to embryonic reawakening.6,7 A second phase is characterised by an increase in larger nodules, and in the stromal-epithelial ratio.7,8
The exact molecular cause behind the development of BPH is not fully understood although a complex interaction of androgens, oestrogens, stromal epithelial interactions, growth factors (epidermal growth factor (EGF), insulin-like growth factor (IGF), keratinocyte growth factor (KGF), transforming growth factor (TGF)-β) and neurotransmitters are implicated). 9 Other risk factors are identified in Table 2.
Risk factors. 9
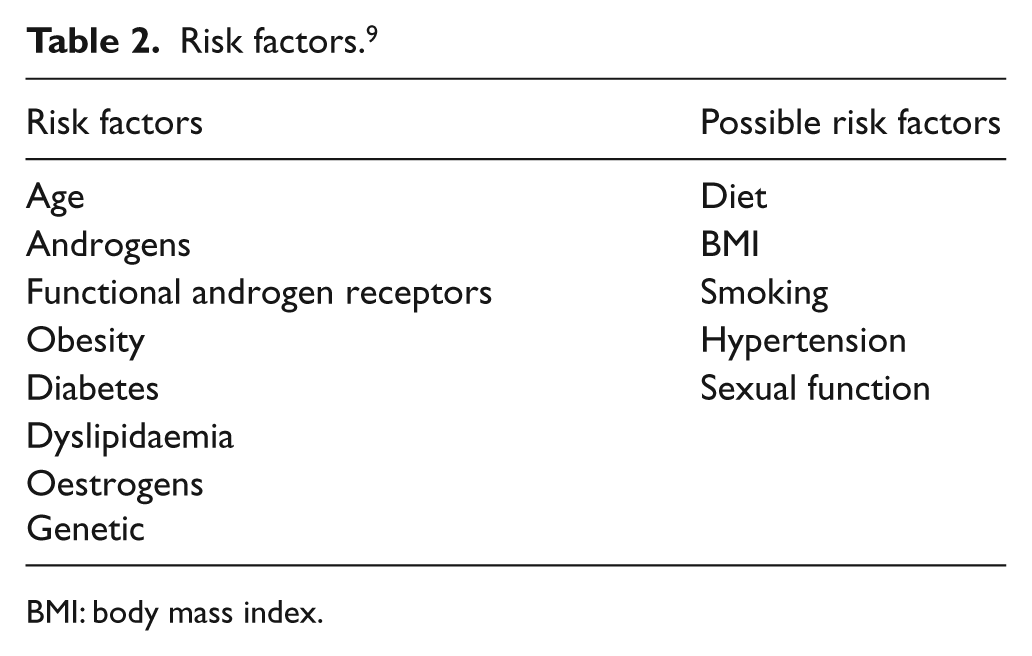
BMI: body mass index.
Approximately 25% of the prostate is composed of smooth muscle under the control of the adrenergic nervous system (α1a receptors) and contributes actively and passively to the pathophysiology of BPH and is the focus of some medical treatments. 10
The portrayal of the clinical manifestations of BPH (LUTS) simply being attributed to a mass effect and tonicity is somewhat simplistic and incorrect. The prostate itself cannot be considered in isolation and changes to the bladder must be considered to fully appreciate the clinical manifestations. Indeed there is an increase in the urethral pressure but this leads to compensatory changes in bladder function which is already affected by age-related changes and neurological degeneration. At first the bladder increases its detrusor action to compensate but over time will hypertrophy, trabeculate, form pseudo-diverticuli and fail, leading to incomplete emptying and a reduced flow. 11
Clinical assessment
The interplay between LUTS, bladder outlet obstruction (BOO) and BPE are illustrated by Hald’s rings. 12 They demonstrate the complex interplay between symptoms and pathology. BPE can be associated with LUTS with or without BOO and BPE can be associated with BOO without having LUTS (see Figure 1). It is the small proportion of patients who occupy the central zone (a) of the diagram who are most likely to derive maximal benefit from intervention. It thus follows that the assessment of LUTS should be broad enough to identify this subgroup of patients.

Hald’s rings. 12
History and examination
LUTS can be broadly grouped into storage symptoms, voiding symptoms, and post-micturition symptoms. Although the predominant type of symptoms can aid in diagnosis, it is worth bearing in mind that the bladder is indeed an “unreliable witness” and consequently further examination and tests must be used as adjuncts to accurate diagnosis and treatment. 13
History must identify the presence of haematuria, urinary tract infection, erectile dysfunction, diabetes, hypotension, fainting and other previous urological conditions including acute urinary retention, or interventions. 14
Medications must be reviewed to identify existing treatment and the use of anticholinergics and α-sympatho-mimetics.
Examination should include a thorough examination of the male genitals, digital rectal examination (DRE), estimation of prostate size and focused neurological examination.
Scores
In an attempt to quantify the severity of LUTS there have been a number of scores including the Boyarski score, the Madsen-Iversen score and the widely adopted American Urological Association Symptom Index (AUA-SI) or International Prostate Symptom Score (IPSS). It consists of seven questions which broadly cover storage symptoms (three questions) and voiding-type symptoms (four questions). Each question has five points attributed to it with the rater scoring 0–5, with zero being never and five being affected all the time. The sum of each question then gives a score out of 35. Patients are classified as suffering from mild (0–7), moderate (8–19) or severe (20–35) LUTS. IPSS also incorporates a single question on quality of life (QoL). It has been shown to be consistent and is validated in a wide array of languages. 15 However, its role is limited to the quantification of LUTs and assessment of response to treatment and not diagnosis. Criticism has been levied at the imbalance in questions, biasing towards voiding symptoms and treatments aimed at reducing prostate size and bladder outlet obstruction as well as its inability to attribute each question’s contribution to QoL.
Frequency volume chart
They are simple, cheap and effective and can provide useful information including frequency, total voided volume, functional capacity, fluid intake habits and demonstrate nocturnal polyuria.
Urinalysis
Urinalysis should always be performed to exclude urinary tract infection (UTI) and haematuria, which would require additional investigation.
Uroflowmetry
Uroflowmetry assesses the combination of detrusor force and outflow opening. Alone it is non-specific, and a reduced flow rate or abnormal tracing can be the consequence of a variety of conditions. Further, maximum flow rate (Qmax) values on their own or in series do not correlate well with IPSS score or bladder outlet resistance. 16 Ideally more than one flow rate should be performed and can be considered valid only if the volume voided is greater than 125–150 ml. Following Abrams’ study in 1977 it is felt that a Qmax <15 ml/s is indicative of BPO requiring treatment. 17
Prostate-specific antigen (PSA)
PSA should be used in context of those patients found to have an abnormal DRE. However, PSA seems to correlate with prostate volume as well as likelihood of progression. Crawford et al. demonstrated those with a PSA≥1.6 ng/ml at baseline were at an increased risk of progression. 18
Residual volume
Residual volume measurement can be achieved ultrasonically or by passing a catheter after voiding, the latter being more accurate but invasive. Measurements must be interpreted in series as opposed to a single measurement as there is considerable variation. Persistently high residual volumes imply weak detrusor contraction relative to bladder outflow, which may be secondary to detrusor dysfunction or BOO. What constitutes a significant residual volume is unclear but volumes >50 ml are likely to be significant and >200–300 ml are more likely to have unsatisfactory outcomes following surgery. 19
Pressure flow studies
Although time consuming, invasive and financially expensive, the information that can be gained from pressure flow studies can be extremely useful. LUTS can be attributed to detrusor instability, and the detrusor pressure can be measured to define whether obstruction is present. Nomograms (International Continence Society (ICS) nomogram) can also be employed using the data to show if a patient is unobstructed. The Abrams-Griffiths number which is calculated as Pdet (
Both the European Association of Urology (EAU) and National Institute for Health and Clinical Excellence (NICE) have produced guidelines that rationalise the use of investigations in BPH/ LUTs as outlined in Table 3.
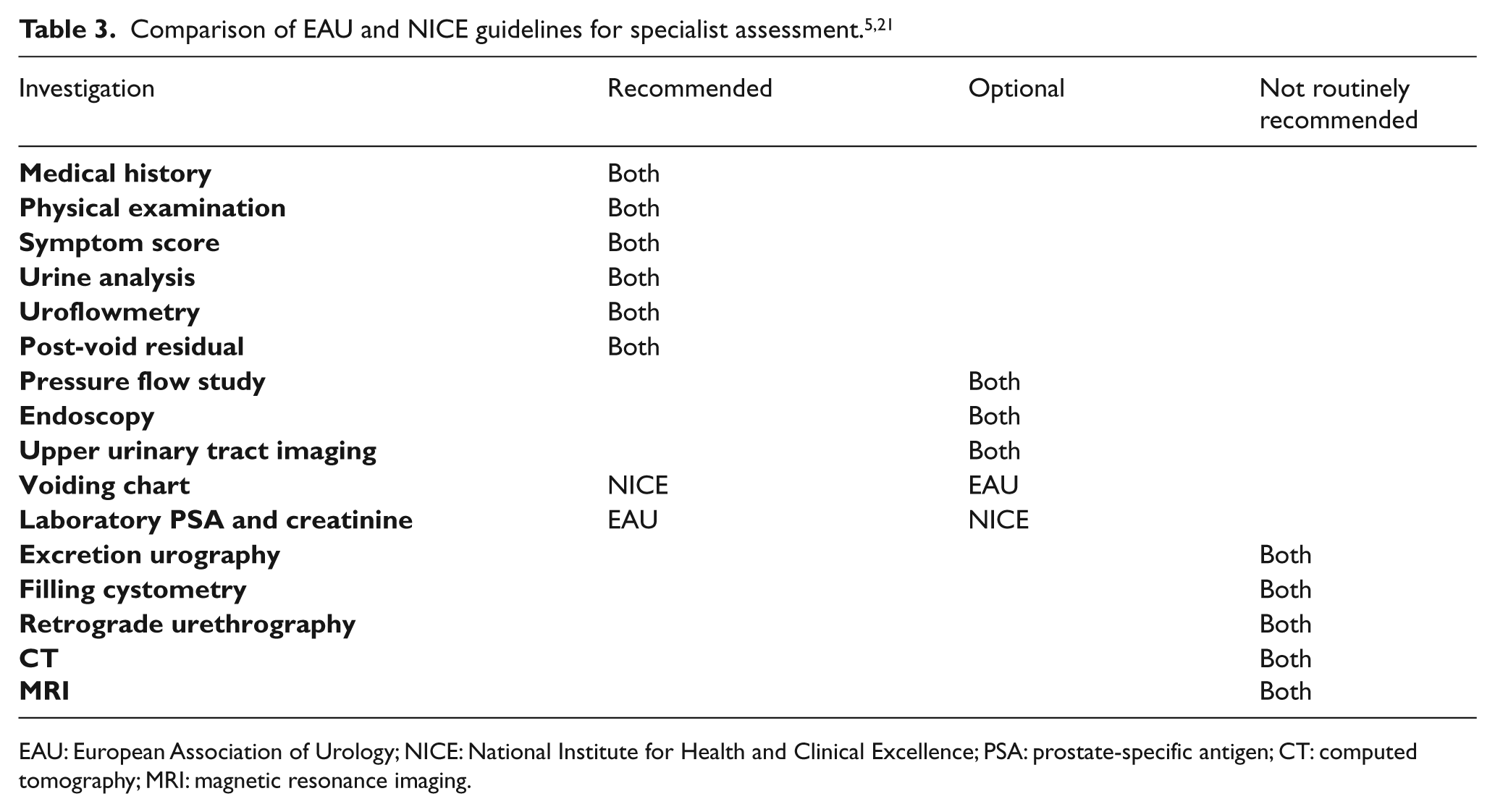
EAU: European Association of Urology; NICE: National Institute for Health and Clinical Excellence; PSA: prostate-specific antigen; CT: computed tomography; MRI: magnetic resonance imaging.
Natural history and complications
The progression of BPH in the untreated patient can only be inferred because of the nature of the disease and the infeasibility of a longitudinal study. Consequently conclusions are derived from placebo arms of long-term interventional studies and hence are subject to inherent biases. A sub-analysis of the Olmstead County Study demonstrated an increase in prostate volume of 1.6% per year on average and an increase in IPSS score of 0.18 symptom units per year on average.22,23
Complications of BPH include renal failure (<2.5%), bladder calculi (0.3–3.4%), infection (<1–12%), incontinence (<1%) and urinary retention (1–2%/yr), all of which have significant impact on the patient.24–29
Acute urinary retention
Urinary retention is a significant complication of BPH. Jacobsen using the Olmsted county data identified that patients in the fourth through seventh decade of life, or an IPSS score >7, or Qmax < 12 ml/sec, or prostate volume > 30 ml, and a post-voided volume (PVR) > 5 oml were all risk factors for acute retention. 30 The annual incidence was 0.7% over the four-year study period. 30
Treatment
Non-surgical
There are a number of conservative strategies aimed at patients demonstrating mild to moderate LUTS. EAU and NICE agree on the education of the patient, reassurance of benign disease and periodic monitoring. Lifestyle advice should also be given and can empower and relieve symptoms without the risks of medical or surgical treatment (see Table 4).
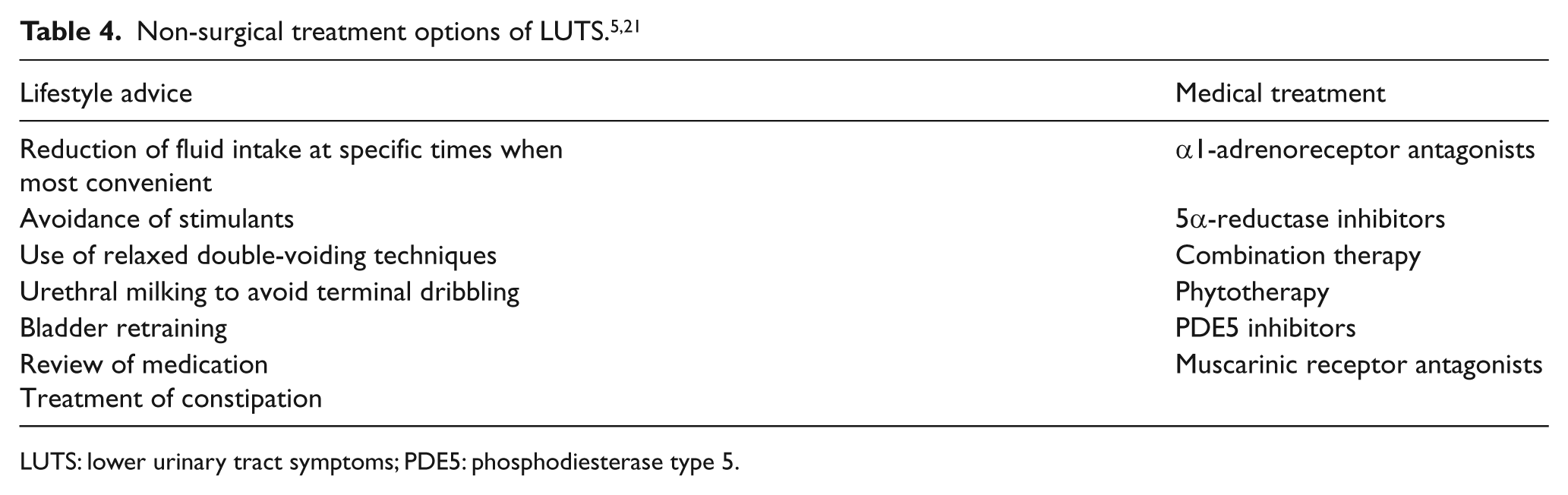
LUTS: lower urinary tract symptoms; PDE5: phosphodiesterase type 5.
Alpha-blockers (ARBs)
Mechanism
There are three forms of α 1 adrenoreceptors: α1a, which is primarily found in the prostate, α1b in blood vessels and α1d in the bladder. Of the α1a type there are at least four different subtypes: a1–4, with a1 being the predominant variant found in the prostate and heart. It was felt that the alpha blockers’ effect was through the antagonism of noradrenaline on the α1a adrenoreceptors in the prostate leading to a reduction in prostatic tone and accordingly bladder outflow obstruction. Unfortunately ARBs have failed to demonstrate a significant change in outflow obstruction on urodynamic studies as well as obstructive LUTS and hence α1-adrenoreceptors outside the prostate are being investigated for their effect.16,31
Efficacy
Evidence provided by Djavan et al. in a meta-analysis suggests that there is little if any difference in the efficacy in terms of IPSS reduction (35–40%) and increased Qmax (15–30%) between different ARBs although tolerability was variable. 32 Improvements are seen in weeks although there is evidence that effects can be seen within hours to days and maintained for at least four years. 29
Side effects
The side effects of ARBs are asthenia, dizziness and orthostatic hypotension, retrograde ejaculation and the recently described intraoperative floppy iris syndrome in cataract surgery. 33
5 alpha reductase Inhibitors (5-ARI)
Mechanism
The effect of testosterone and dihydrotestosterone (DHT) on the prostate and development of BPH has been well documented. The 5α reductase inhibitors (5-ARI) competitively inhibit the 5α-reductase enzyme which converts testosterone to the more active DHT. Finasteride, however, unlike dutasteride, doesn’t reduce DHT to castrate levels as it blocks only the type 2 isoform.
Efficacy
The enlarged Prostate International Comparator Study (EPICs) demonstrated that in those studied (i.e. patients over 50 years old with a Qmax < 15 ml/s, AUA-SI > 12 and prostate volume > 30 ml) over a 12-month period of 5-ARI use, the mean reduction of prostate volume was 26.7 vs. 26.3% for finasteride and dutasteride, respectively (p=0.65). Further there was a reduction of AUA-SI of −5.5 for finasteride and −5.8 with dutasteride (p=0.38). 34
The Proscar Long-term Efficacy and Safety Study (PLESS) (a double-blinded European randomised, placebo-controlled trial, using finasteride 5 mg once daily in men with Qmax < 15 ml/sec, a residual volume of > 150 ml, moderate to severe symptoms and BPE on DRE), found that there was a 55% and 57% relative risk reduction in men requiring surgery and having an episode of acute urinary retention, respectively, in the finasteride arm. 35
Side effects
Side effects include reduced libido, erectile dysfunction and abnormal ejaculation. 36
Combination therapy
There have been a number of studies that have examined the possible benefits and potential difficulties in using combination therapy. Short-term studies (52 weeks) such as the Veterans Affairs Co-operative and the Prospective European Doxazosin and Combination Therapy trial (PREDICT) have demonstrated that although patients on both ARB monotherapy and combination therapy (ARB+5ARI) show a significant improvement in outcome measures, specifically flow rate and symptom scores (IPSS), there is no significant difference between monotherapy or combination therapy.37,38
However, longer-term data from the Medical Therapy of Prostatic Symptoms trial (MTOPs) show that combination therapy significantly reduced the risk of clinical progression when compared with placebo and monotherapy over a mean 4.5-year follow-up. 27 Further post-hoc analysis showed, however, the difference in effect became less significant as prostate volume decreased to a point where there was no statistical difference in prostates < 25 ml in volume. 39
The Combination of Avodart and Tamsulosin trial (COMBAT) aimed to characterise the benefit of combination therapy in larger prostates and recruited men with prostates over 30 ml in size with an IPSS of at least 12. 40 The multicentre double-blinded trial accepted 4844 men ≥ 50 years old and was run for four years. It concluded that combination therapy had a significantly greater improvement in symptom score as well as peak urinary flow rates from baseline than dutasteride or tamsulosin, as well as reducing the relative risk of acute urinary retention (AUR) or BPH-related surgery over four years by 66% compared with tamsulosin monotherapy. Unfortunately those on combination therapy suffered from a higher frequency of adverse events.
Other treatments
Antimuscarinics
In some cases a degree of bladder overactivity may co-exist or masquerade as BOO and as such the standard treatment measures may fail. Several small studies have looked at the concomitant use of antimuscarinics in resistant cases and have demonstrated positive effects. The only placebo-controlled, randomised trial comparing the combination of ARB and antimuscarinics to individual therapy, demonstrated that in isolation the therapies performed less well compared with placebo but in combination showed good efficacy in improving QoL scores. 41 Concerns over precipitating an episode of AUR exist. PVR has been shown to be statistically significantly increased in those on both ARB and an antimuscarinic compared with monotherapy or placebo, although none of the patients in the dual therapy group went on to develop clinical retention. 42
Saw palmetto
Derived from the serenoa repens, saw palmetto is thought to be the active ingredient. Apart from one systematic review and meta-analysis in 1990 by Wilt et al., the general consensus from more recent randomised controlled trials (RCTs) do not support the efficacy of saw palmetto over placebo and hence its exclusion from guidelines. 43
Botulinum toxin
There have been promising small studies examining the use of intraprostatic botulinum toxin use as well as NX-1207 which have shown a reduction in prostate volume and symptom scores. 44 The NICE recommendation is for its use only as part of an RCT.
Surgical treatments
The transurethral resection of the prostate (TURP) continues to be the benchmark treatment of BOO and BPH. In a systematic review, TURP has been shown on average to improve the mean AUA/ IPSS score from 18.8 to 7.2 (−62%) after 12 months post-op as well as improve Qmax by 9.7 ml/s, a mean increase of 120%. 45 Approximately 10–15% of patients within 10 years will require further intervention. 46 The standard workup is similar to that of medical treatment. Contention still exists in the role of urodynamic assessment and although none of the current guidelines recommend pressure flow studies there are certainly patients who merit further characterisation such as patients <50 or >80 years old, those with previous unsuccessful invasive therapy, high post-void residuals (>300 ml) and previous pelvic surgery. Indications and morbidity are listed in Tables 5 and 6.
Indications for TURP. 36
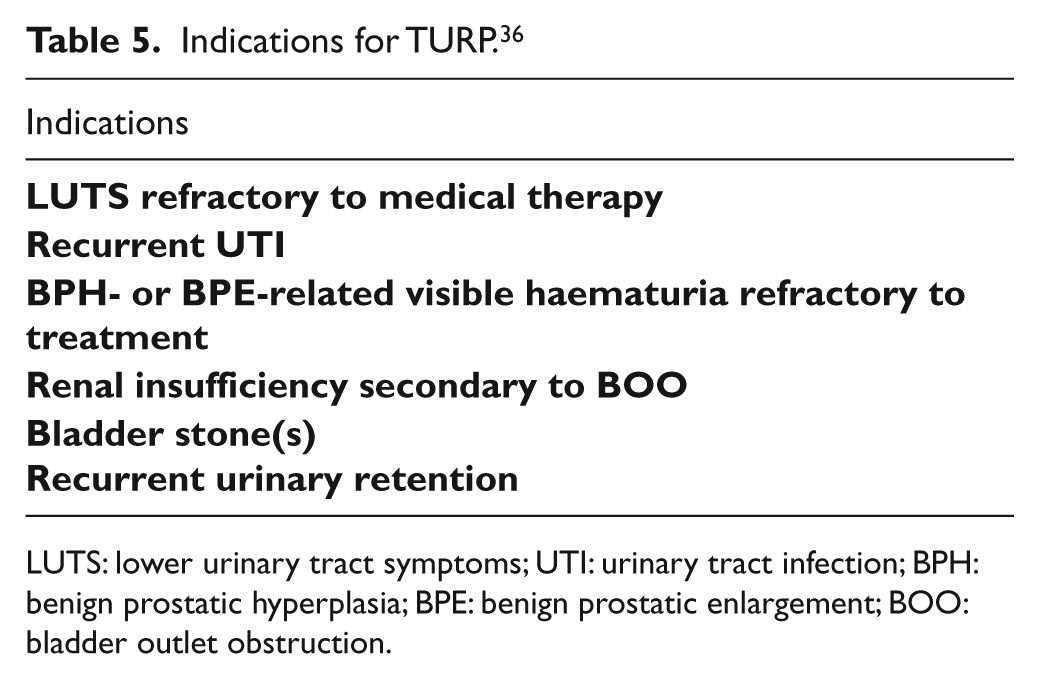
LUTS: lower urinary tract symptoms; UTI: urinary tract infection; BPH: benign prostatic hyperplasia; BPE: benign prostatic enlargement; BOO: bladder outlet obstruction.
Complications of TURP. 47
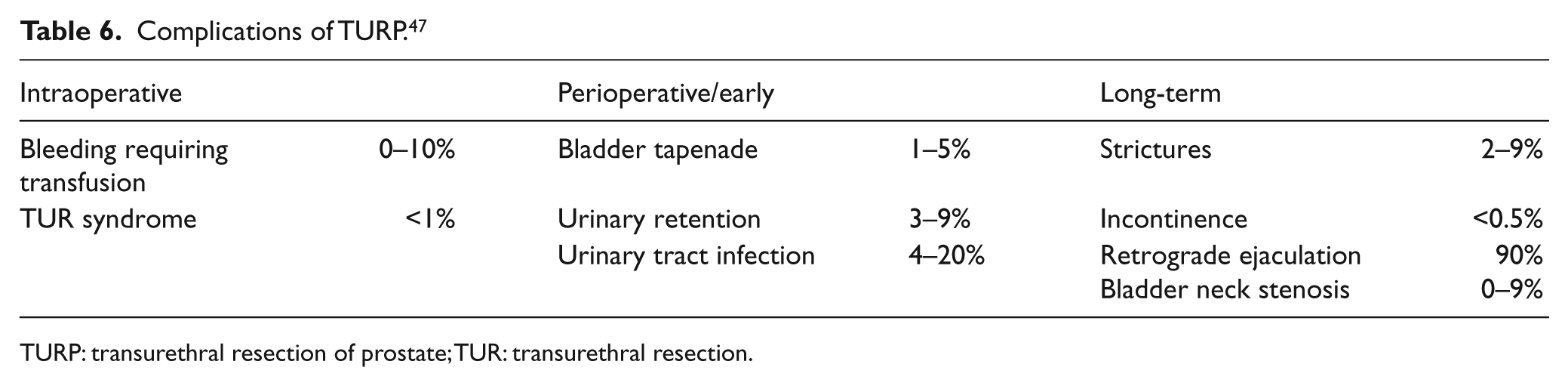
TURP: transurethral resection of prostate; TUR: transurethral resection.
However, over the last 20 years the numbers of alternative surgical treatment options have flourished (Table 7) as clinicians have endeavoured to treat increasingly more complex elderly patients. The introduction of bipolar TURP has improved the safety profile by removing the concern of TUR syndrome. However, the majority of these falls short of the benchmark of TURP and only holmium laser enucleation of the prostate (HoLEP) provides comparable outcomes and longevity. 36
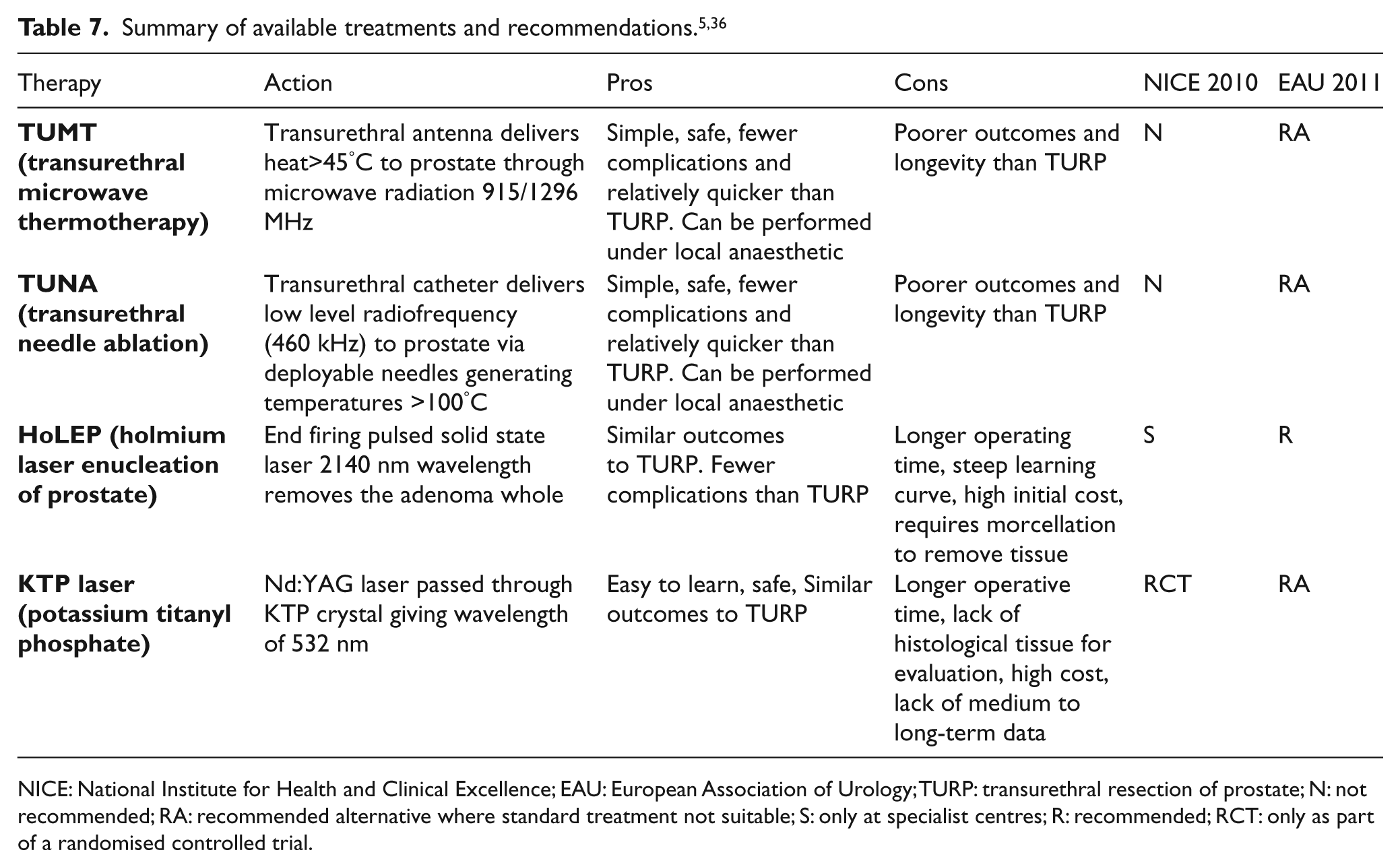
NICE: National Institute for Health and Clinical Excellence; EAU: European Association of Urology; TURP: transurethral resection of prostate; N: not recommended; RA: recommended alternative where standard treatment not suitable; S: only at specialist centres; R: recommended; RCT: only as part of a randomised controlled trial.
Conclusion
BPH is a complex condition with a yet to be fully understood pathophysiology. The diagnosis and treatment of the condition has been refined and are moving to less invasive but effective treatments.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there are no conflicts of interest.
The platform for answering on-line CME questions will be released later in 2013.