
Abstract
Introduction
Prostatic abscess is an uncommon diagnosis in the modern antibiotic era, with a reported incidence of approximately 0.5%. 1 Escherichia coli and gram negative organisms are responsible for around 70% of cases; other organisms include Staphylococcus and Pseudomonas species. 2 Panton Valentine leukocidin (PVL) – a highly virulent toxin often present in community-acquired methicillin-resistant Staphylococcus Aureus (MRSA) strains – is rarely found as a cause, with only one published case report to date. 3 We present the first reported case of a PVL-producing methicillin-sensitive Staphylococcus Aureus (MSSA) causing a prostatic abscess.
Case presentation
An 87 year-old Pakistani gentleman with a history of diabetes initially presented to his GP with dysuria and was treated with oral antibiotics for a presumed urinary tract infection. He attended the A&E department 5 days later with persistent dysuria, lower abdominal pain and constipation. On examination his temperature was 38.5°C, he was tachycardic with a tender distended abdomen. Digital rectal examination revealed a tender, slightly fluctuant prostate.
Blood investigations revealed an elevated C-reactive protein (CRP) of 279 and a white cell count of 20.7x10−9/l. Blood cultures revealed a PVL-toxin producing S. Aureus. Computerised tomography with intravenous contrast revealed enlargement of the prostate with low density changes, suggestive of prostatitis with abscess formation.
Despite receiving 72 hours of intravenous antibiotics he continued to spike temperatures. Consequently, an ultrasound-guided transperineal pigtail drain was inserted; 15 ml of purulent fluid was drained, confirming the presence of a methicillin-sensitive PVL-toxin producing S. Aureus. It later transpired that the patient’s 4-year old granddaughter had recently been hospitalised for a PVL-producing S. Aureus necrotising pneumonia and that family members were receiving prophylaxis.
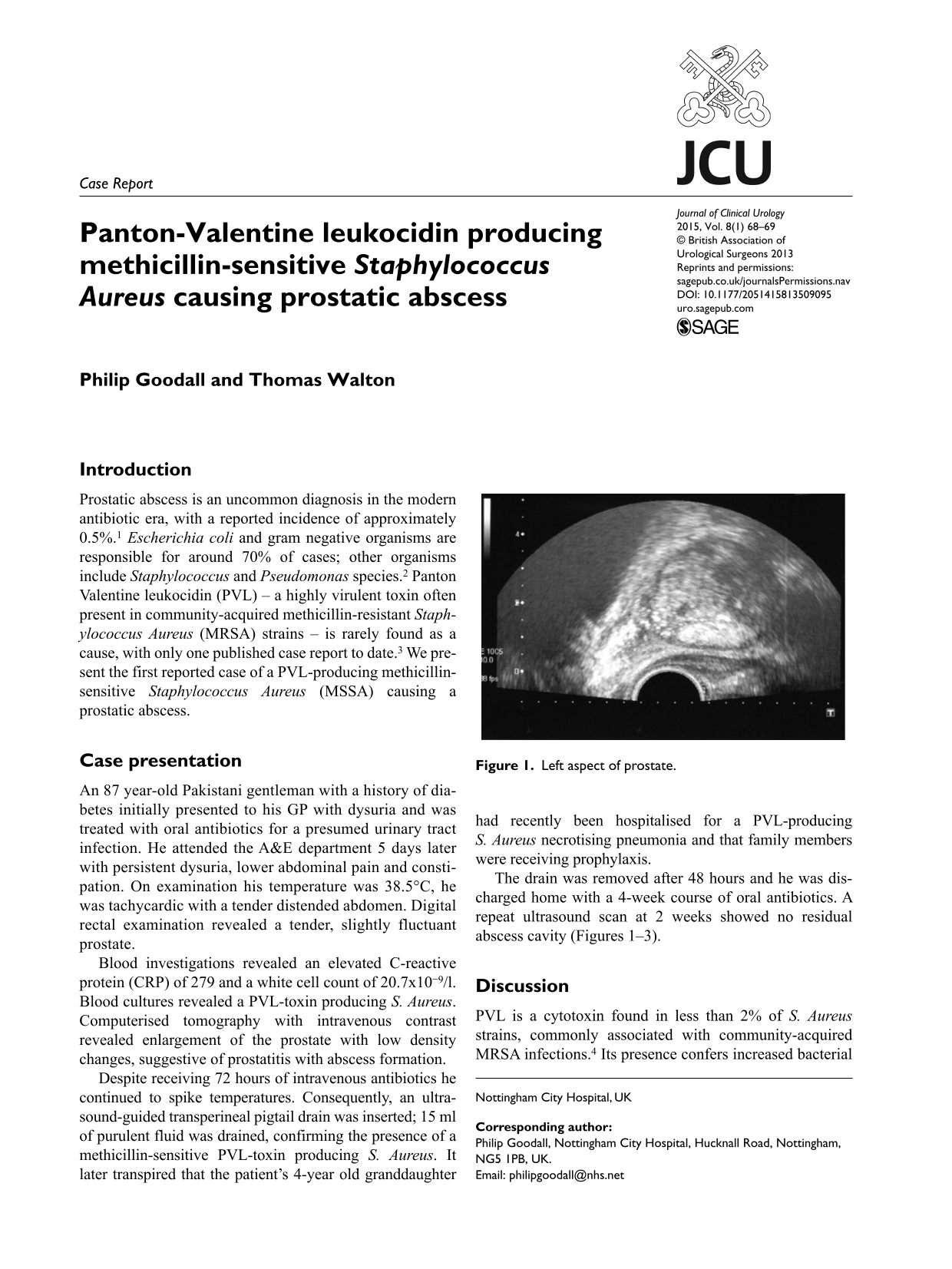
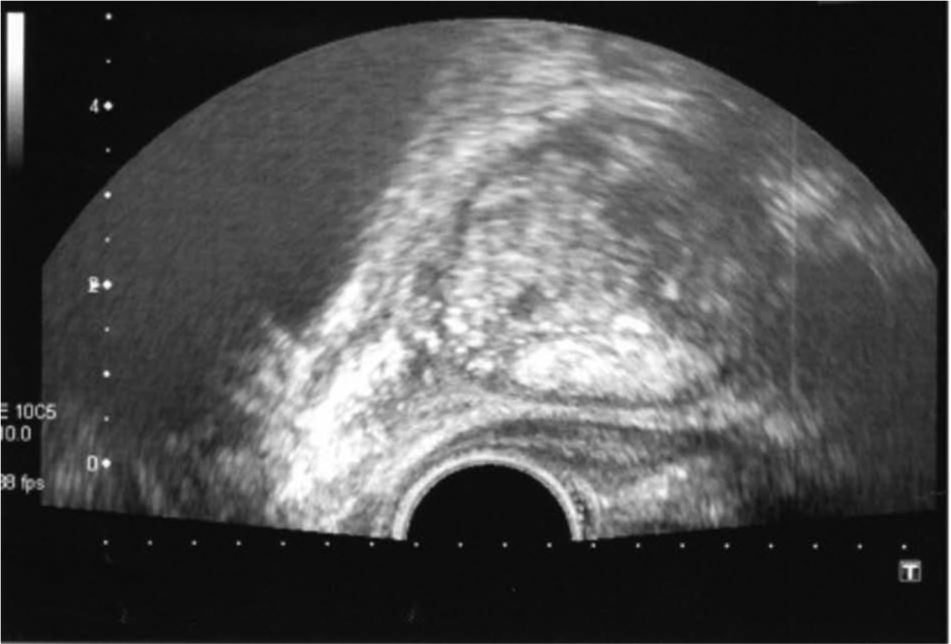
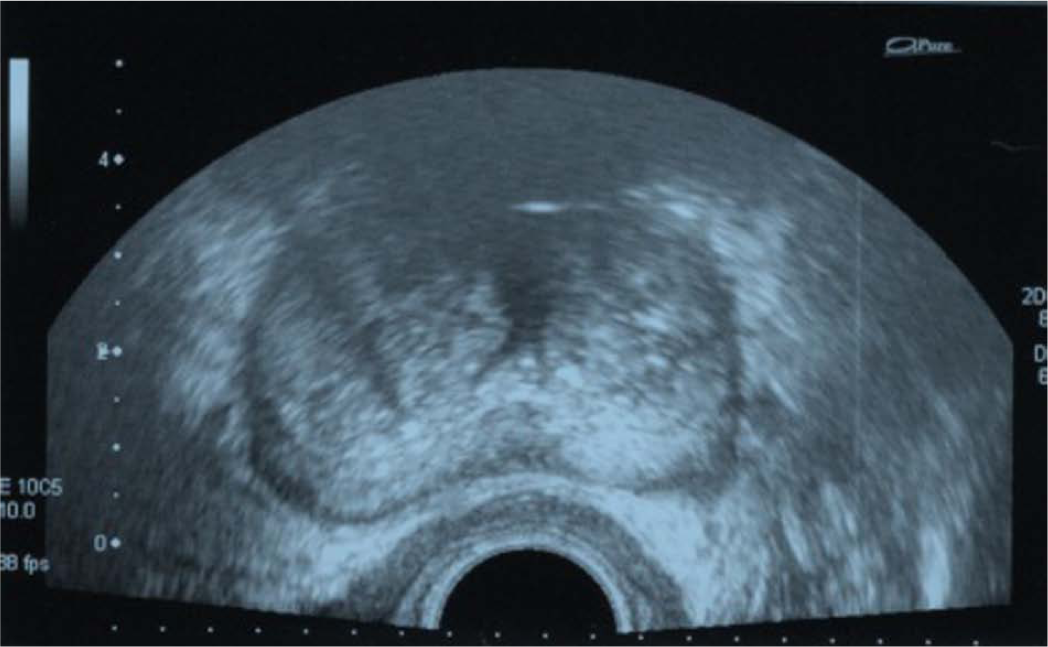
The drain was removed after 48 hours and he was discharged home with a 4-week course of oral antibiotics. A repeat ultrasound scan at 2 weeks showed no residual abscess cavity (Figures 1–3).
Left aspect of prostate.
Middle aspect of prostate.
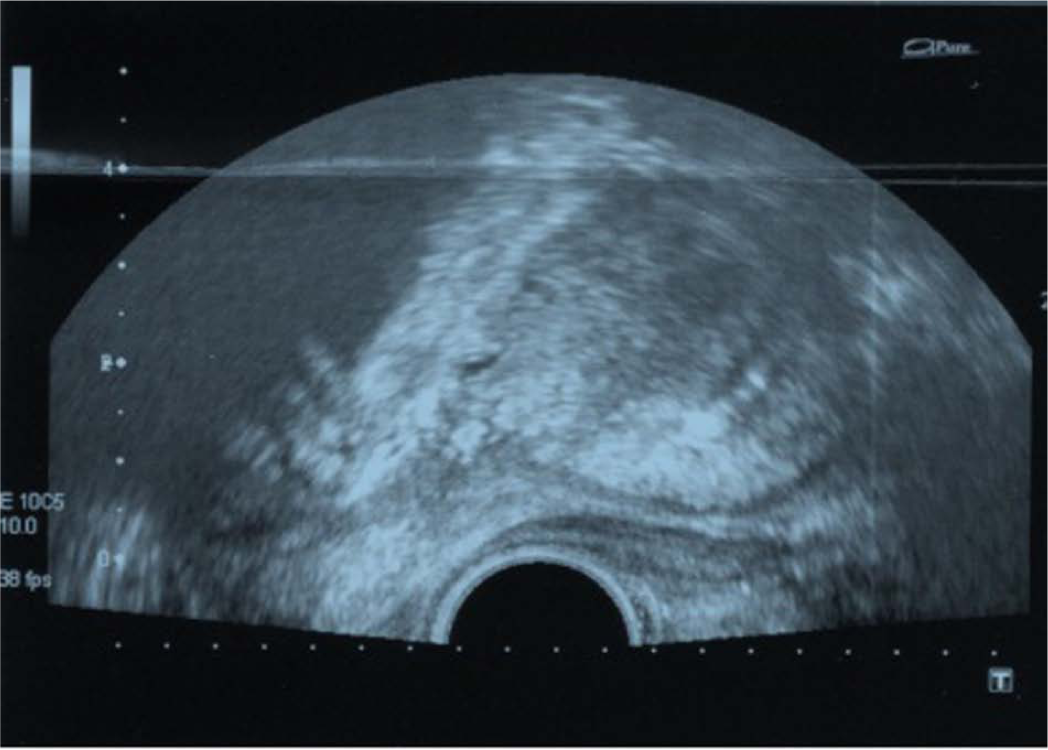
Right aspect of prostate.
Discussion
PVL is a cytotoxin found in less than 2% of S. Aureus strains, commonly associated with community-acquired MRSA infections. 4 Its presence confers increased bacterial virulence, due to an ability to cause leukocyte destruction leading to tissue necrosis. 5 PVL-producing S. Aureus strains are found in cases of significant necrosis, such as necrotising pyogenic skin infections and community-acquired necrotising pneumonia.
Prostatic abscess formation due to a PVL-producing S. Aureus infection has only once been reported in the literature to date. Described by Javeed et al., 3 also in a diabetic patient, the causative organism was a MRSA strain. The clinical presentation was atypical as the features were non-specific with no risk factors to indicate person-to-person transmission. In contrast, our case describes a classical presentation of prostatic abscess caused by a MSSA organism. The predominant feature is that there was a family member with an established PVL-producing staphylococcal infection.
This case highlights that diabetes is an established risk factor. The presence of PVL cytotoxin confers a high risk of person-to-person transmission and severe necrotising infection, mandating aggressive treatment with intravenous antibiotics and potential abscess drainage. Prophylaxis for family members is advisable. Prostate involvement, although rare, should be considered in patients with unusual or persistent urinary or pelvic symptoms.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.