
Abstract
Introduction:
Visible haematuria (VH) is a very common presentation to the emergency department (ED). In an outpatient setting, 18%−24% of such patients have been shown to have an underlying malignancy. The aim of this study is to determine the malignancy rates of patients presenting acutely to ED and whether the degree of bleeding or presence of clots is a higher risk factor for cancer.
Method:
We retrospectively collected data from adult patients (>18 years) presenting to ED with VH for a six-month period. Diagnostic outcomes after one year were assessed.
Results:
Our study population has 96 patients (male = 77, female = 19) with a mean age of 68 years (SD = 20.2). Twenty-eight patients (29%) had haematuria with clots. Twenty-five patients (26%) had a new diagnosis of malignancy, and 10 had a known diagnosis of malignant disease. Bladder cancer was the most commonly found malignancy, in 17 patients (15 new diagnoses), while prostate cancer was second with 14 cases (six new). Renal cancer two, testicular one and colorectal one accounted for the other new malignancies diagnosed following presentation. All but one patient with cancer were male. Although most malignancies were found in patients over 70 years old, the two youngest patients were in their 30s. The incidence of malignancy appears to increase in patients who have urinary blood clots (58%), p = 0.08.
Conclusion:
A third of patients presenting to ED with VH will have a urological cancer. Patients with VH and clots have a significantly higher incidence of malignancy. We recommend expedited referral of all such patients to a urologist.
Introduction
Haematuria is a frequently encountered presentation in the emergency department (ED).1,2 Presentation of visible or macroscopic haematuria varies, including presence of clots, retention of urine and concurrence of pain. It may be due to a variety of causes, the most serious being underlying malignant pathology.
The positive predictive value (PPV) of visible haematuria (VH) for urological cancer is 10%−22%.3,4 Prospective cohort studies in United Kingdom (UK) protocol-driven haematuria clinics have revealed an incidence of malignant pathology in 19%−24% of patients with VH vs 3.7%−5.2% for non-visible haematuria.5–8 The majority of malignancies found are urothelial carcinoma (UC) of the bladder.
Few studies have been conducted on the incidence of malignancies in patients with VH presenting to ED. We wanted to quantify risk of malignancy in patients presenting to ED with VH and compare to patients presenting through a primary care pathway. We also sought to determine if the severity of VH in the ED, manifested by the presence of clots, has any effect on the incidence of malignancy.
Methods
Selection
This study was performed at Whipps Cross Hospital, a district general hospital in the East of London serving approximately 350,000 people. All patients presenting to the ED with VH from August 2009 to January 2010 inclusive were identified retrospectively using Ascribe’s Symphony Electronic Patient Record system and then verified by documentation in patient records.
Inclusion criteria were patients presenting at ED with a documented principal diagnosis of VH. Inclusive documentation included, ‘visible haematuria’, ‘frank haematuria’, ‘bloody urine’, ‘blood stained urine’, ‘rose urine’, ‘clots’, ‘clot retention’, ‘gross’ and ‘macroscopic haematuria’. Patients under the age of 18 years, patients with microscopic or non-visible haematuria or patients who did not have documented VH were excluded from the study.
The data collection was performed retrospectively. We identified those who had a pre-existing diagnosis of malignancy and cross-checked our results with the urology cancer database at Whipps Cross Hospital Cancer and Histopathology Department. The data were reviewed and correlated with patients’ case notes, electronic records, picture archiving and communication system (PACS) imaging and general practitioner (GP) communication after at least a year in order to confirm accurate data extraction and determine follow-up outcomes.
The degree of haematuria on admission was stratified into VH only or haematuria with documented clots in patient records. Patients presenting to the ED with VH would either be admitted and investigated as in-patients or discharged back to their GP and reviewed by a urologist via the two-week cancer pathway.
Investigations were similar in both pathways and undertaken within the cancer targets timeline. Typically this would have included an ultrasound, intravenous urogram (IVU)/computed tomography (CT) urogram, digital rectal examination (DRE) ± prostate-specific antigen (PSA) and flexible cystoscopy unless the cause of haematuria was obvious, i.e. trauma or where such investigations were inappropriate for individual patients. Patient data were followed up for at least a one-year period and subsequent urological diagnoses in that time frame were included.
Seven patients never attended further urology diagnostics; after review by ED staff only and not needing admission or catheterisation, they were discharged to primary care follow-up. Despite contacting the GP service, no data on these seven were retrievable.
Data were collected on the patients’ age, sex, existing urological malignancy diagnoses, new urological diagnoses, urine culture, imaging outcomes and histology.
Analysis
We calculated the incidence of the various urological malignancies in patients presenting with VH to the ED. Chi square analysis was used to determine statistical significance in patients with VH with and without clots.
Results
A total of 109 patients were identified with VH. Six patients were excluded as they were under the age of 18. Seven patients had no urological follow-up and no retrievable data and were excluded. The remaining 96 patients consisted of 77 males and 19 females Their age ranged from 23 to 98 years old with a mean age of 68 years (SD = 20.2). Seventy-two patients (75%) were referred for immediate specialty review with some having inpatient investigations for expediency, while 24 (25%) were discharged from the ED for follow-up via two-week pathway. Twenty-eight patients (29%) had documented presence of clots. Patients were more likely to be admitted if clots were documented 93% vs 68%, p = 0.01.
New diagnosis of cancer was made in 25 patients (26%) subsequent to the haematuria presentation. A pre-existing diagnosis of malignancy accounted for the haematuria in 10 patients (10%). Eight of the 10 pre-existing cancers were prostate cancer. The mean age of patients with a cancer diagnosis was 71.5 years (SD = 15.9). A diagnosis of bladder cancer was the cause of haematuria in 17 patients, whilst prostate cancer was associated with 14 cases. Two renal cell carcinomas, one testicular cancer and one metastatic colonic cancer with vesico-rectal fistula accounted for the remaining four cases (Figure 1).
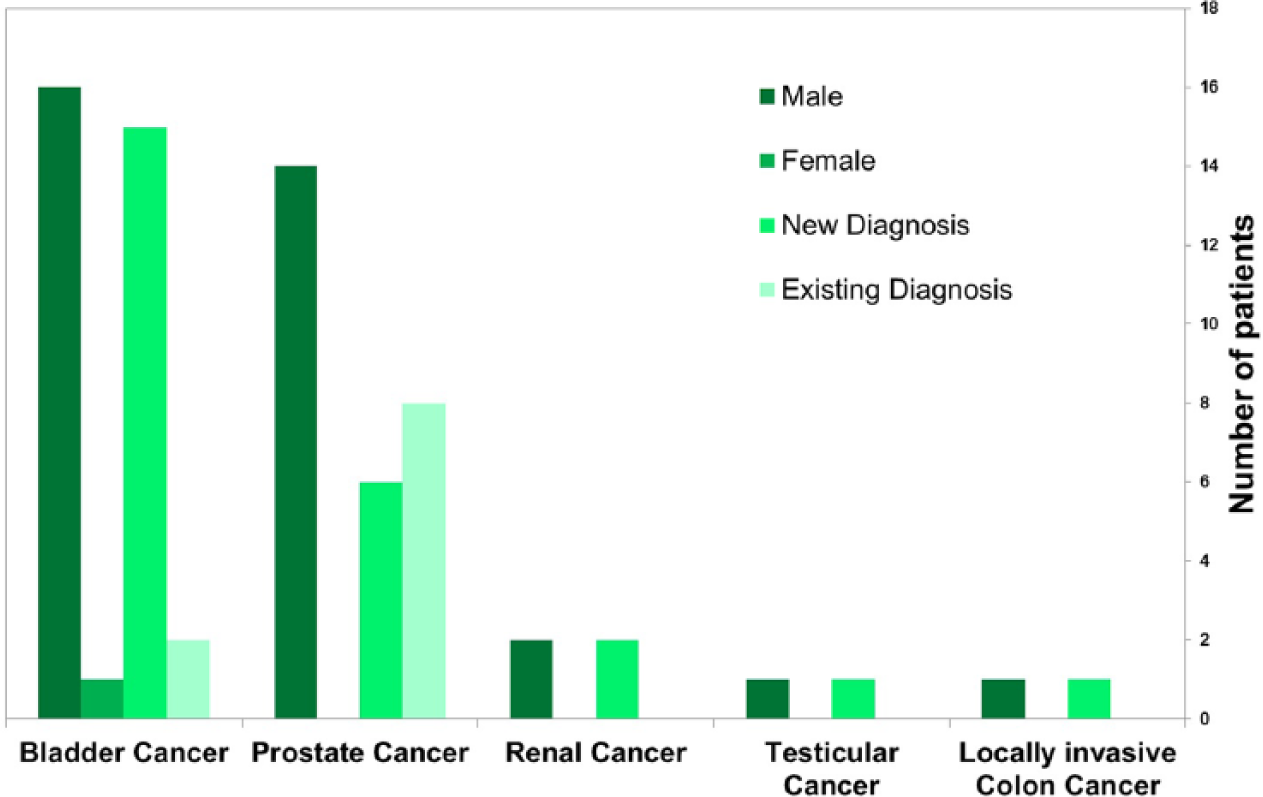
Distribution of cancer diagnoses after presentation with visible haematuria (VH) to emergency department.
Of the 17 cases of bladder cancer in the study, 16 were UC)and one was smal- cell carcinoma. The histological stage for UC found varied, with Ta in eight patients, T1 in three and T2 in five (Figure 2).
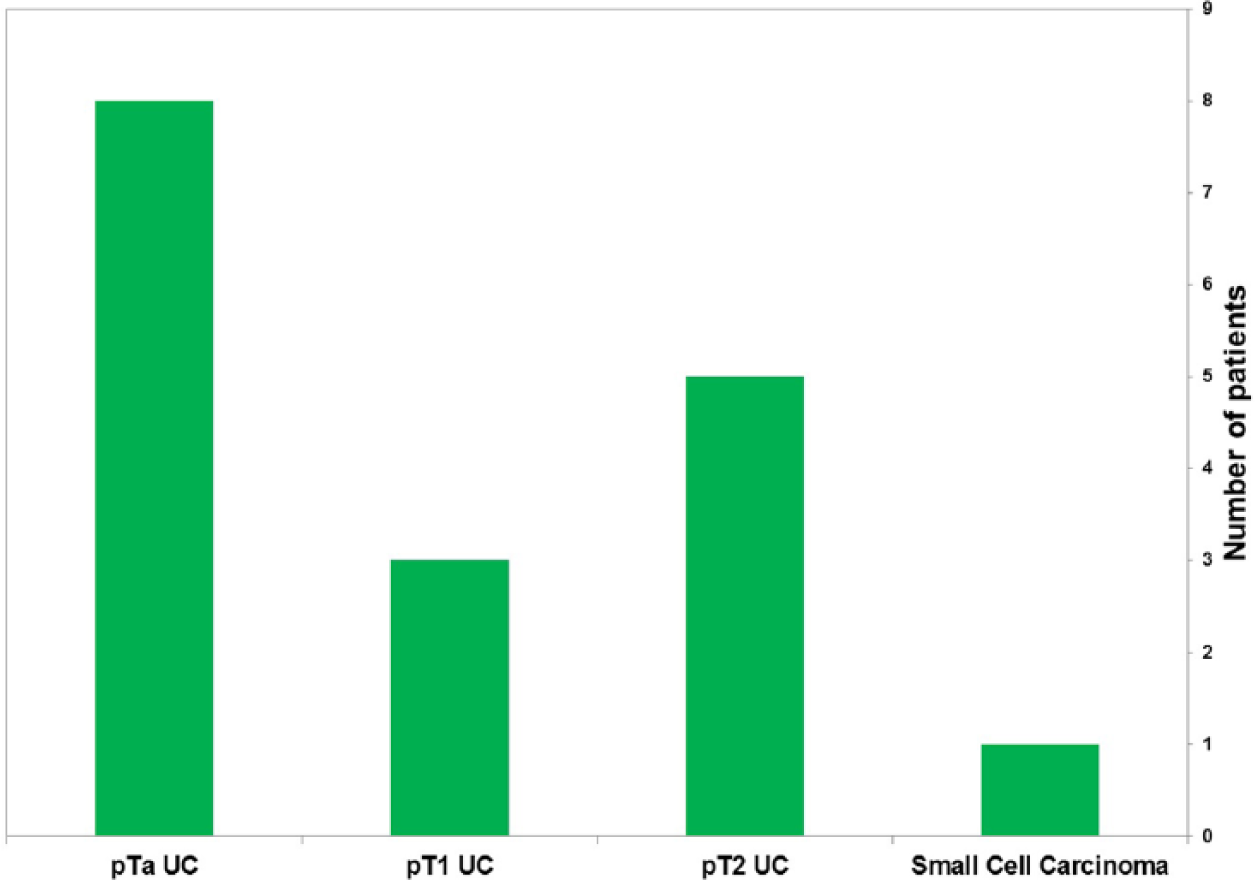
Variation in stage of urothelial carcinoma presenting to emergency department.
Fifteen of these patients had a new diagnosis of bladder cancer made subsequent to the haematuria presentation, with two patients having a pre-existing diagnosis.
Conversely, six patients with haematuria had a new diagnosis of prostate cancer, with eight patients having a pre-existing diagnosis. Three patients receiving a new diagnosis were identified by abnormal DRE and high PSA (110, 132 and 568) alone, whilst the further three had prostate biopsy due to suspicious DRE and aberrant PSA. The biopsy results were G3+3, G3+4 and suspicious for prostate cancer without provision of Gleason score. The further eight patients were on active treatment, surgical follow-up or a watchful waiting/active surveillance program for prostate cancer.
The majority of our patients diagnosed with cancer (66%) were aged 70 years and above. Twenty per cent of patients with cancer were in the 40–60 years age group. The two youngest individuals were male and aged 33 and 38 years. They were diagnosed with testicular and bladder cancers, respectively.
Sixty-one patients (64%) had a benign diagnosis. The most common cause is infection of bladder, kidney or prostate, which accounted for 20 cases (21%). Stone disease accounted for 11 cases (12%), benign prostatic bleeding nine (9%), trauma/catheter trauma five (5%), coagulopathy three (3%), surgical complications one and march haematuria one (1%). We were unable to determine the underlying aetiology of VH categorically in 11 patients (12%) (Figure 3).
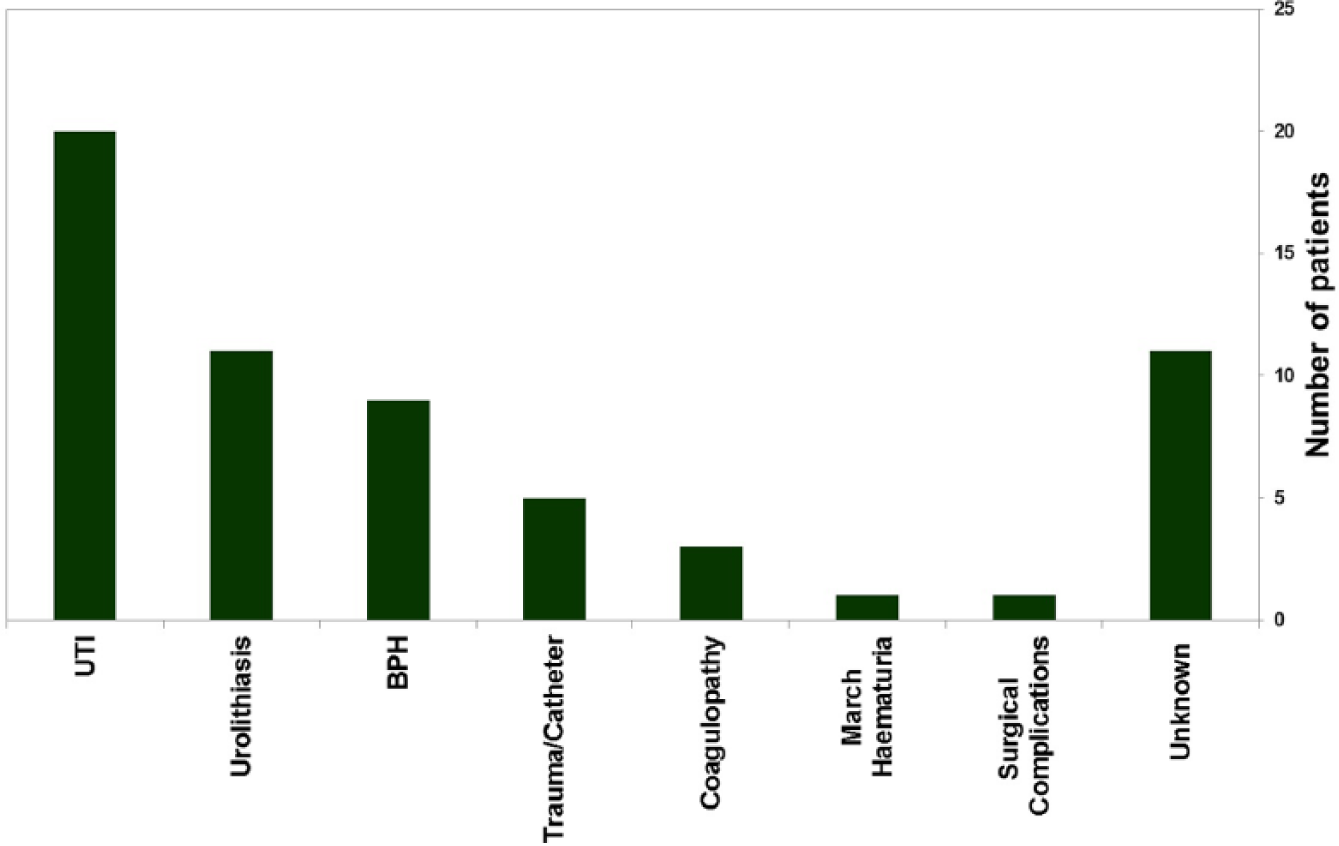
Benign diagnoses of patient presenting with visible haematuria (VH) to emergency department.
Haematuria and clots were documented in 28 patients and had a PPV of 50% for malignancy (Table 1). The presence of clots may increase the risk of malignancy compared to VH alone, p = 0.08 (two-tailed chi square test).
Distribution of new and historic diagnoses against sex and presence of clots.
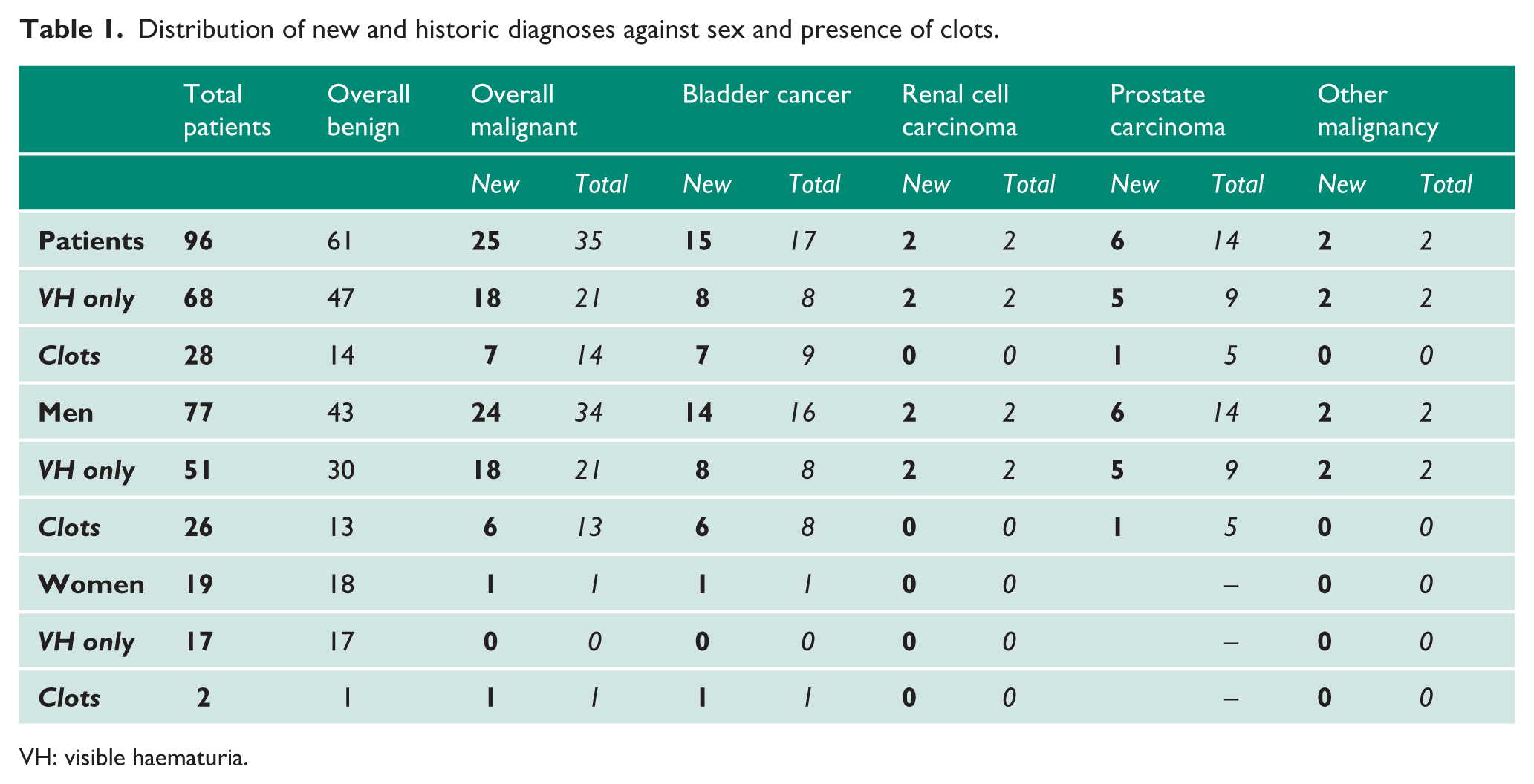
VH: visible haematuria.
Discussion
Haematuria is an extremely common presenting symptom for urological malignancy and many papers have been published regarding its PPV in diagnosing urological cancer.3–10 However, most of the evidence involved patients who were reviewed electively in an outpatient setting. There are scant data assessing the diagnostic value of VH in the emergency setting. A Spanish study looked at admissions from the ED of a specialised urology unit over a 10-month period in 1993. 11 A total of 694 patients were found to have VH. Of these 24.4% were diagnosed with malignancy and 22.2% were lost to follow-up. However, it is difficult to relate this study to a general ED cohort. Our study is the only one that looks exclusively at outcomes of patients presenting to the ED with VH.
Bladder cancer
UC was the most common malignancy associated with presentation of VH (49% of patients with malignancy). This is expected as previous meta-analysis has shown that VH has a pooled sensitivity of 83% for bladder cancer and 66% for upper tract cancers. 3
It has long been known that delay in treatment of bladder cancer has an impact on survival, heightening the necessity for early assessment and intervention.12–14 This has been further emphasised by a large retrospective study by National Cancer Intelligence Network (NCIN) that revealed that 23% of newly diagnosed cancer patients came through as emergency presentations and those presenting at ED had a far worse relative survival. 15 In this study 18% of bladder cancers presented as an emergency presentation, but this was not exclusively in the ED setting. For almost all cancer types, one-year survival rates were much lower for patients presenting as emergencies than for those presenting via other routes. As such, patients presenting to the ED with VH provide an excellent for opportunity for prompt identification and subsequent early treatment of patients with cancer.
A fast-track referral system from the ED or the formation of an ‘emergency urology clinic’ may provide a safety net for high-risk patients, such as those with VH, to avoid unnecessary admissions, particularly in the current stretched system.
Prostate cancer
Haematuria is the most common presentation for bladder cancer, but is less commonly seen as a presenting complaint in prostate cancer. A British study showed that haematuria has a PPV of 1% for prostate cancer among patients in the community. 16 Interestingly, our study showed a significant number of prostate cancer in our cohort of patients with VH. Our study revealed haematuria in the ED did subsequently lead to six new diagnoses of prostate cancer − 6% of the cohort. The NCIN also found new prostate cancer cases had an emergency presentation in 9%. 15 The cause for the high incidence of prostate cancer is not entirely clear, but is likely to be related to more advanced disease; however, further study is suggested. There is no agreed guideline on what constitutes a haematuria screen in an emergency setting. Investigations involving ultrasound kidney, ureter, bladder (KUB), IVU, CT urogram and flexible cystoscopy will not assess the prostate. In view of that, we recommend performing a DRE at least in all patients presenting with haematuria. This is particularly relevant as Singh et al. have shown that there is a higher risk of prostate cancer as a second malignancy in patients diagnosed with bladder cancer after adjusting for diagnostic and treatment biases. 17
Other cancers
Two renal cancers presented with VH. VH was taught as a classical presentation within a ‘triad’ of symptoms for renal cell carcinoma but this is becoming less common as the increased use of imaging leads to earlier detection of smaller renal masses. 18
Testicular cancer was found incidentally, following investigation, in one young male who was known to have human immunodeficiency virus (HIV). One patient with metastatic colo-rectal malignancy had a vesico-colonic fistula presenting with haematuria secondary to lower urinary tract infection (UTI).
Gender
All but one of our patients diagnosed with cancer during the investigative process are male. The only female with cancer was found to have bladder cancer. Males are known to be at a higher risk of urological malignancy as shown by previous studies in haematuria one-stop clinics. 4 In fact, there is a 5:2 male to female ratio for bladder cancer diagnosed in the UK; 19 however, our local cancer database showed a much higher incidence of cancer in females than the national average (1.35:1). 20 We would therefore expect to see more women diagnosed with cancer in the ED in our study, but our results may imply that women are accustomed to accessing primary care. This is backed up by a Danish study, which concluded that men are less likely to seek primary care, but have higher hospitalisation rates and mortality. 21
Males are less likely to seek medical services for a variety of psychosocial, cultural and economic reasons 22 and as a result, they are more commonly diagnosed with cancer in the ED with a higher rate of metastasis. 23 An American public health study showed women were more likely to have public or private health insurance, when controlled for other socio-economic factors, and were more likely to access non-hospital health care. 16 Men’s health awareness campaigns such as ‘Movember’ are currently trying to educate men and reverse this trend. 24
Age
The mean age for patients found with cancer was 71.5 years (SD = 15.9); however, one of the new bladder cancer patients was a male in his 30s. This correlates with other retrospective studies, which have identified UC in young patients. 25 In fact, it has been shown that 10%−20% of men aged <60 years will be found to have a malignancy during the investigative process.5,26,27 British Association of Urological Surgeons (BAUS) guidelines on haematuria have reinforced the fact that all patients regardless of age need to be investigated after a single episode of VH. 28 This is being reinforced by the ‘Blood in the Pee’ campaign, part of the National Health Service (NHS) ‘Clear on Cancer’ initiative to educate patients on symptoms of common cancers. 29
Clots
Many papers have shown that VH is associated with a higher risk of malignancy than microscopic haematuria.4,30 We wanted to determine if the degree of VH, as determined by the presence of clots, has any correlation to the risk of malignancy.
From our study, the incidence of malignancy was higher in patients who had a documented clot haematuria 40% vs 23%, p = 0.08. Although the presence of clots may indicate a brisker rate of bleeding from a malignant tumour, in reality the formation of clots is multifactorial and other factors such as hydration, co-morbidity and medication would also affect clot formation and could be confounding variables. It is, however, supported by the knowledge that VH carries a higher risk of malignancy than microscopic haematuria.
Also the PPV for cancer in our cohort of patients with VH is 24%. This figure is at the higher end of previously reported outcomes (Table 2) in the literature for primary care and outpatient clinic cohorts.3–6 The true incidence of malignancy in our study may be slightly lower as patients with VH and other associated symptoms may have been miscoded, e.g. UTI or vaginal bleeding and hence not identified in our study.
Comparison of outcomes with major studies in the literature.
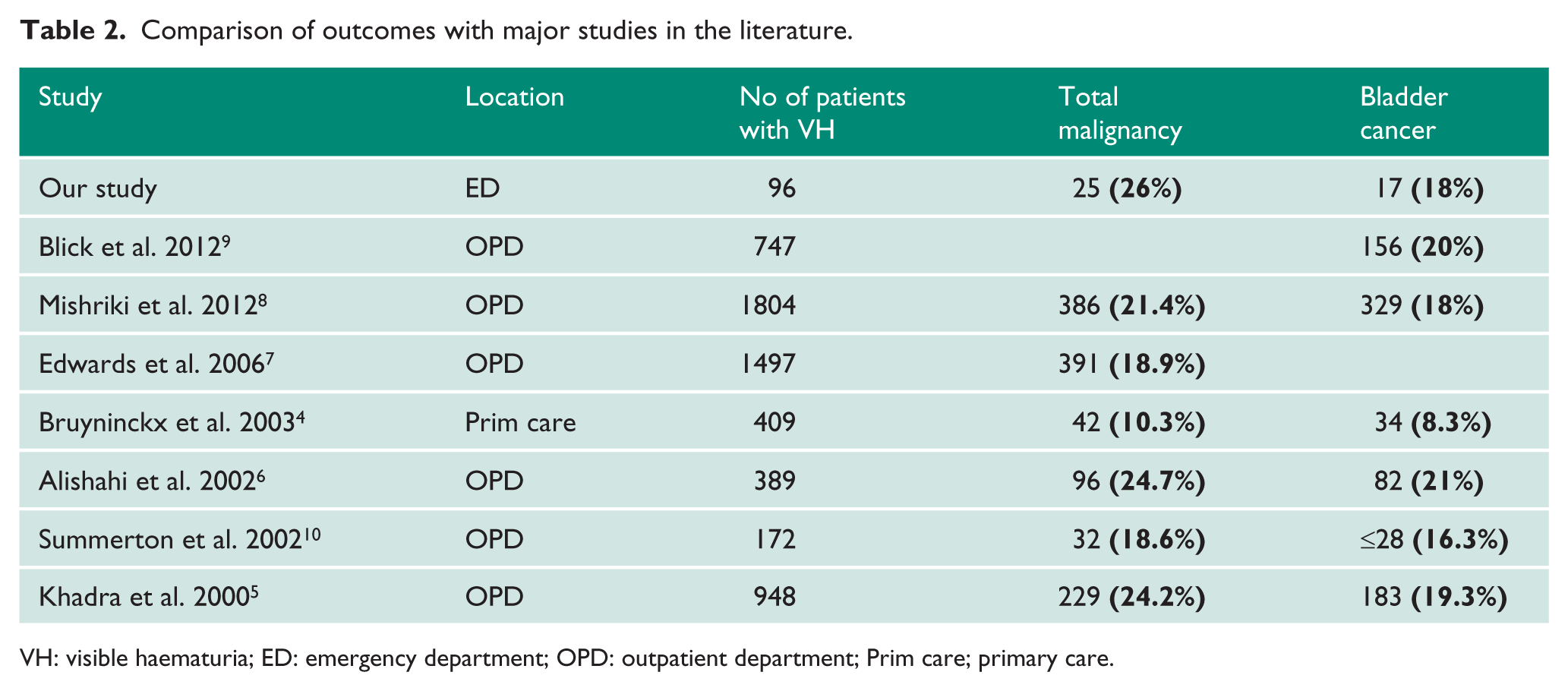
VH: visible haematuria; ED: emergency department; OPD: outpatient department; Prim care; primary care.
Limitations
We recognise that accurate documentation in patient notes may be suboptimal in a retrospective study and the failure to document presence of clots does not exclude their presence. The diversity of presenting pathway unlike a haematuria clinic makes direct comparisons less easy. As patients known to the urology department were not excluded from the study, prior investigations, diagnoses or management made investigation of all patients more heterogeneous. As a retrospective study, end-point of follow-up varied from 12 to 18 months, but was at least one year in all patients except seven who did not receive follow-up. The recruitment process may have missed some patients through miscoding, for example, patients recorded as vaginal bleeding, but who actually had haematuria. Seven patients who did not have urological follow-up may have had subsequent diagnoses made elsewhere that may have affected the results.
The admission rate of patients may appear high, but can be explained by the method of data capture which does not easily differentiate between those patients who were admitted to a dedicated ward for overnight stay and those patients who were sent to a clinical decision unit for specialty review to support increased patient numbers through the ED.
Despite these limitations, this work provides a useful insight into the value of diagnosing VH in the ED and the importance of harnessing this opportunity to investigate these patients. It provides further support to other papers looking at late presentation of various cancer groups via ED and supports the UK Government Health ‘Blood in the Pee’ Campaign to educate the population to recognise potential symptoms of cancer and thus empower them to seek medical care earlier. 30
Conclusion
We conclude that urological cancer is found in significant numbers of patients presenting with VH in the emergency setting and is comparable to those found in the outpatient setting. UC is the most common malignancy found but prostate cancer is also prevalent.
As advised by BAUS for the outpatient setting, we recommend performing a ‘haematuria screen’ for all patients with VH whether as an admitted urology inpatient or via an urgent cancer pathway. We recommend including a DRE as part of the emergency haematuria screen due to the high incidence of prostate cancer and the possibility of concurrent urological cancers. Vaginal examination in women should also be undertaken to exclude cervical and pelvic masses.
Footnotes
Acknowledgements
We would like to thank Ms Paula Allchorne, Bladder Cancer Cancer Nurse Specialist at Whipps Cross Hospital for her help with the study.
Conflicting interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical Approval
This study was registered and approved by the Whipps Cross Hospital Clinical Audit Department.
Guarantor
JSAG
Contributorship
AH and JSAG researched literature and conceived the study. AH and JHG were involved in data collection and analysis. JHG and AH wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.