
Abstract
Objectives:
Flexible cystoscopy can cause patients significant psychological distress, especially when utilised in the diagnostic pathway for suspected bladder cancer. We aimed to assess the prevalence of general anxiety and depression, as well as procedure-related worry and pain in patients undergoing local anaesthetic flexible cystoscopy and to determine whether these conditions occur more frequently in subsets of the population.
Patients and methods:
Patients referred for flexible cystoscopy were invited to participate. Patients were asked to complete a questionnaire containing the Hospital Anxiety and Depression Scale (HADS), a worry score and a question regarding the most stressful event in the diagnostic pathway. Following the procedure patients were also asked to complete a pain score.
Results:
A total of 175 patients participated in the study. The prevalence of significant anxiety was 15% and depression 3.5%. This was higher in younger, female and unmarried patients. Procedure-related worry and pain were generally low.
Conclusions:
We found the prevalence of anxiety and depression in patients undergoing flexible cystoscopy to be raised compared to a similar cohort of patients undergoing TRUS-guided prostate biopsy. We have identified subgroups more likely to experience these symptoms and have also identified the sections of the diagnostic pathway that are most likely to cause anxiety and depression. By doing this we can target those patients who are more likely to suffer during the diagnostic process and aim to improve their experience. We can also implement targeted changes to the pathway to reduce the impact it may have on patients’ mental health.
Introduction
Flexible cystoscopy is an important diagnostic tool for the urologist. It is routinely used in an out-patient setting for patients who present with haematuria as well as lower urinary tract symptoms and pelvic pain. Flexible cystoscopy is often the first-line investigation used in the diagnosis of bladder cancer and important for surveillance of patients with known bladder cancer. 1 Anecdotally, many patients undergoing flexible cystoscopy in relation to bladder cancer experience anxiety – either in anticipation of the investigation, during the procedure, or following the procedure in relation to follow-up.
The prevalence of anxiety and depression has previously been studied in relation to the investigation of prostate cancer; Awsare et al. found that some patients suffer significant psychological distress in relation to investigations for prostate cancer requiring targeted mental health support. 2 Stav et al. examined anxiety levels in 100 patients undergoing rigid cystoscopy and found there to be a generally low level of pre-procedure anxiety but noted that younger patients were significantly more anxious than older patients. 3 There is, however, little research investigating the occurrence of psychological distress among patients undergoing flexible cystoscopy in relation to bladder cancer.
Guidelines for the management of patients with cancer in the United Kingdom (UK) have been issued by the National Institute of Clinical Excellence (NICE) 4 and the Department of Health. 5 These guidelines emphasise the importance of offering psychological and social support, as well as spiritual care and financial support to individuals being investigated and treated for cancer. The National Cancer Action Team has published a guide for health care professionals entitled ‘Holistic Needs Assessment for People with Cancer’, which encourages clinicians to look at the patiant’s overall experience during the care pathway. 6 It states that the first step in the holistic management of cancer care is to identify people who are likely to need help and to establish the needs of these patients.
The aims of this study are: to assess the prevalence of pre-existing anxiety and depression; to assess the prevalence of procedure-related worry and pain; to determine whether these conditions occur more frequently in subsets of our cohort according to their gender, age, marital status, employment status and level of education; and to explore which aspects of the diagnostic pathway cause the most distress to patients.
Patients and methods
Patients were recruited from the urology clinics of two large district general hospitals (DGHs) in London between 2002 and 2003. All patients who were listed for flexible cystoscopy, the majority for the investigation of microscopic or macroscopic haematuria, aged over 18 years old and who could read and speak English were eligible to participate in the study.
Patients who accepted the invitation to participate were asked to complete a questionnaire containing the Hospital Anxiety and Depression Scale (HADS), a worry score and a question regarding the most stressful event in the diagnostic pathway. Following the procedure patients were also asked to complete a pain score.
HADS is a tool to assess a patient’s level of anxiety and depression validated for use in out-patient pre-operative settings.7,8 HADS consists of 14 questions in two sections: HADS-A contains seven questions to assess anxiety (score range 0−21) and HADS-D contains seven questions to assess depression (score range 0−21). A score of 11 or more is considered significant as it represents moderate to severe cases. 9
The assessment of worry was conducted using a 10-point visual analogue scale (VAS) included in the pre-procedure questionnaire. Patients were asked to score their level of worry in relation to 1) the upcoming procedure itself and 2) in relation to receiving the results of the investigations in the near future (Figure 1).
Visual analogue scale for the assessment of worry: a) regarding the upcoming procedure; b) regarding receiving the results of the investigation in the near future.
Patients were asked to identify which part of the diagnostic pathway they found to be the single most stressful event. This was performed by selecting a single best answer from a list of 11 options contained within the pre-procedure questionnaire (Figure 2).
Options for the single most stressful event in the diagnostic pathway.
Following the procedure patients were asked to complete a pain score using a 10-point VAS. Pain scores were divided into low pain (0−2) and high pain (3−10).
Statistical analysis
Differences between various socio-demographic groups in mean scores for anxiety, depression, the two worry items and pain were compared using either independent samples t-tests (gender, marital status, employment status) or analysis of variance (age). Statistical differences between lower (≤median) and higher (≥median) pain score groups with regards to mean anxiety and depression scores were assessed using independent samples t-tests. Equality of variance was checked (and relevant modifications made) wherever independent samples t-tests were used.
Ethics
The protocol for the study was reviewed and approved by the Whipps Cross Research and Development department. Prior to their procedure, patients identified for inclusion were given written information about the study and invited to participate.
Results
A total of 175 patients were recruited: 137 (78.3%) from Whipps Cross University Hospital, London, and 38 (21.7 %) from the Lister Hospital, Stevenage. One hundred and seventy-three patients completed the pre-procedure HADS-A and HADS-D questionnaires; 105 patients completed the two-stage worry score; 121 answered the ‘most stressful event question’; and 76 patients completed the pain score. The mean age of participants was 73 years (SD = 14.78). Of the total, 102 participants were men (58.3%), 60.6% were married/living as married, 59.4% were not in employment. Only five patients had less than a secondary school level of education, thus prohibiting statistical analysis between high and low education groups.
Anxiety and depression (Table 1)
Levels of anxiety and depression are displayed in Table 1. Using a score of ≥11 as the threshold for significant anxiety or depression, a higher prevalence of anxiety (15%) than depression (3.5%) was observed. Scores for anxiety and depression showed significant variation across age and marital status, with younger and unmarried patients experiencing higher levels both of anxiety and depression. Females were significantly more likely to experience anxiety than males, but not depression.
Sociodemographic variables and HADS.
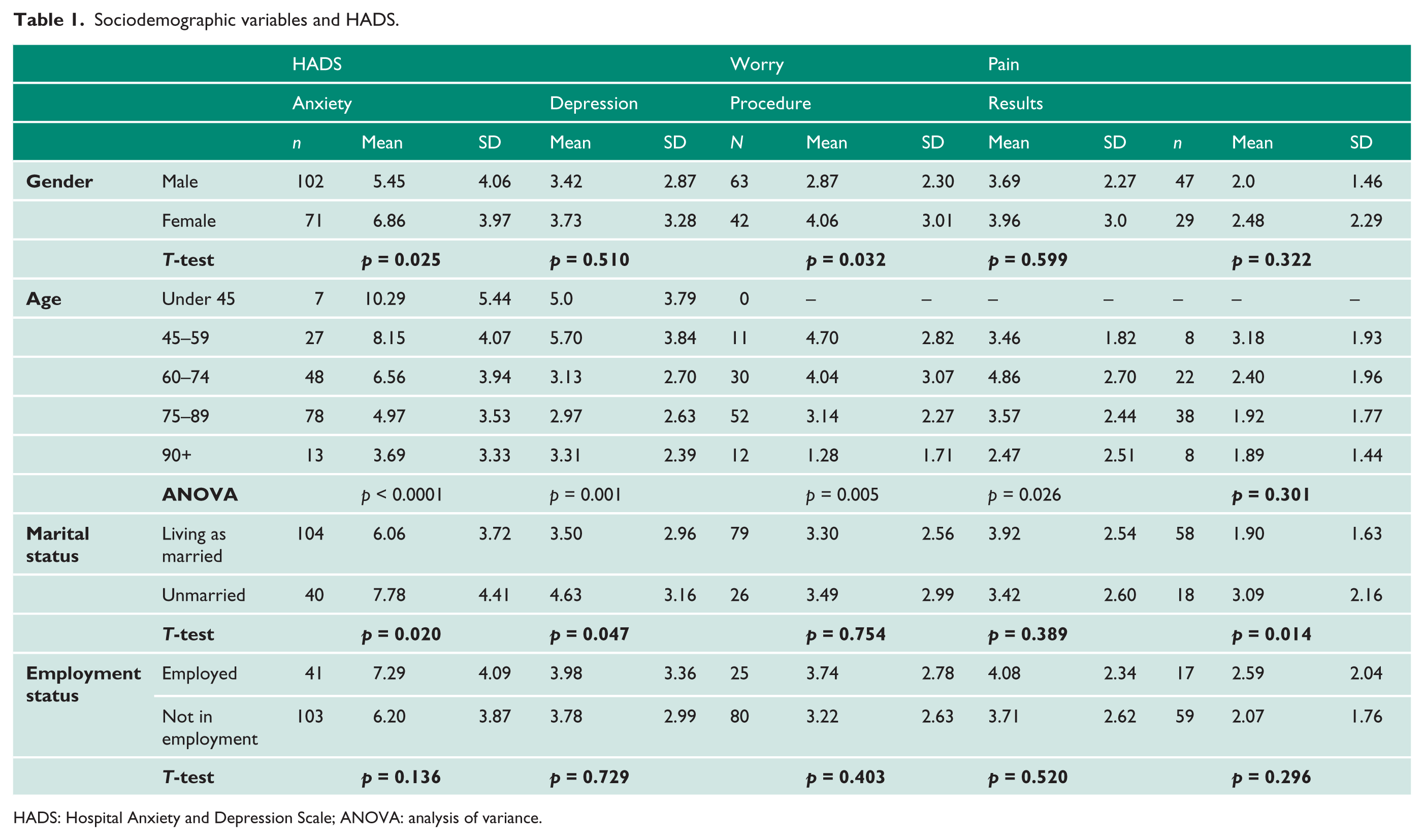
HADS: Hospital Anxiety and Depression Scale; ANOVA: analysis of variance.
Worry (Table 1)
Overall the mean level of worry regarding the procedure (3.35 ± 2.66) and worry regarding the results of the procedure (3.90 ± 2.55) were low. Females experienced higher levels of worry about the procedure than males (p = 0.032), but there were no significant gender differences in worry relating to the results. Levels of worry regarding the procedure declined significantly with increasing age (p = 0.005). There was significant variation in worry regarding the result, with a peak worry level in the 60–74 age group, lower levels in 45–59 and 75–89 age groups and lowest in the >90 group (p = 0.026). Marital and employment status did not appear to affect worry about the procedure or the results.
Pain (Table 1)
Pain scores did not differ between gender, age or employment status. However, patients who were married/living as married reported less pain during the procedure than those who were unmarried (p = 0.014). The median pain score was two. Patients who experienced higher pain levels (pain ≥3) tended to score higher on HADS-D (3.57 ± 2.63) than those who experienced lower pain levels (2.33 ± 2.17; p = 0.03). No significant difference was observed in anxiety scores (HADS-A) for those patients who experienced lower pain (Table 2).
Median split of pain and HADS.
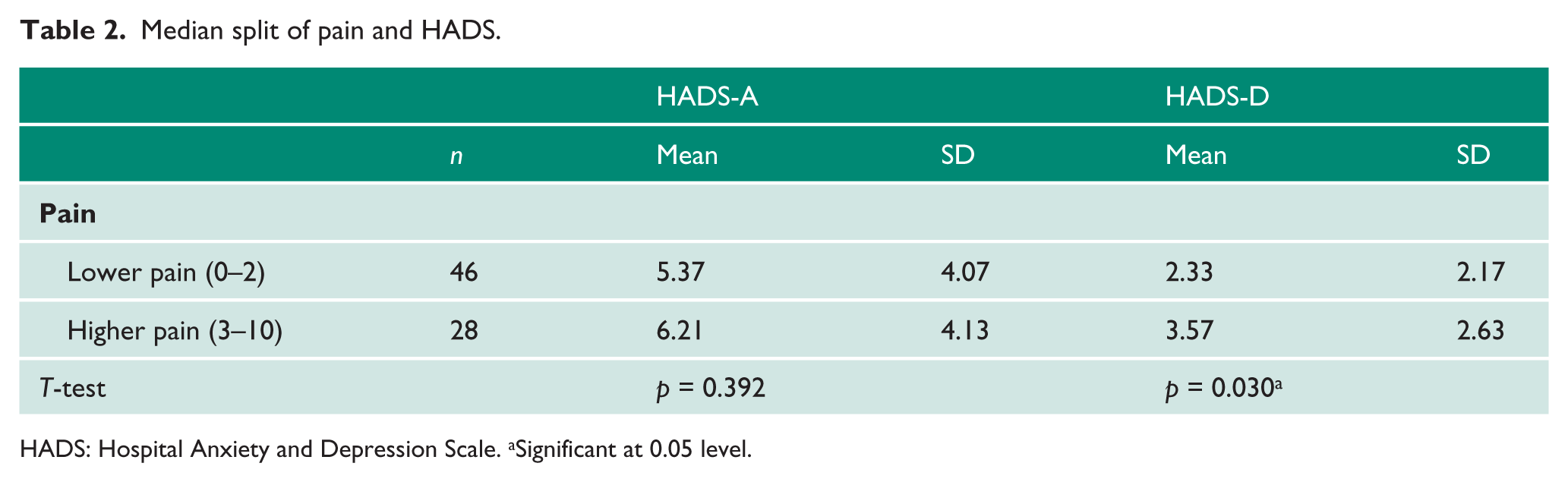
HADS: Hospital Anxiety and Depression Scale. aSignificant at 0.05 level.
Most stressful event (Figure 2)
Patients were asked to state which single component of the diagnostic pathway they found to be the most stressful. Of 121 patients who completed this question, 19 (16%) stated ‘finding out they had to undergo the procedure’, 32 (26%) gave ‘waiting to undergo the procedure’ and 21 (17%) gave ‘undergoing the procedure’ as the single most stressful event. Twenty-five (21%) stated ‘none’.
Discussion
This study demonstrates that out-patient flexible cystoscopy causes psychological distress to a significant number of patients, and that certain groups of patients may be more at risk of distress than others. In particular, female patients suffer higher levels of anxiety than male patients, and females and the 60–74 age group experience the highest levels of procedure-related worry. Unmarried patients and those with higher depression scores experienced higher pain. Over a quarter of patients found waiting to undergo the procedure the most stressful step in the treatment pathway, more than the number who found the actual procedure the most stressful part.
The mean scores of anxiety and depression, as defined by HADS-A and HADS-D, in our population (HADS-A = 6.03, SD = 4.07; HADS-D = 3.55, SD = 3.04) are comparable to those of the general population described by Crawford et al., who administered the HADS to 1792 adult, non-clinical individuals to estimate the prevalence of anxiety and depression in the general population. Crawford et al. found mean HADS-A, HADS-D and total scores of 6.14, 3.68 and 9.82 respectively in this cohort. 10 They also found that females had statistically significantly higher anxiety, depression and total scores compared to males. We have used a threshold of 11 or above to indicate significant levels of anxiety or depression as validated by Snaith and Zigmond to describe moderate to severe symptoms. 9 When this threshold was applied to the non-clinical cohort of Crawford et al., 12.6% of their cohort suffered with moderate or severe anxiety and 3.6% had moderate or severe depression. In our cohort the prevalence of moderate or severe anxiety and depression was 15% and 3.5%, respectively. These data show similar levels of anxiety and depression in our cohort to that of the normal population of Crawford et al. However, the two cohorts differ in their age characteristics, with our population being older with only 4% under the age of 45 whilst, in Crawford’s population, 59% of respondents were aged 18–44.
Awsare et al. 2 looked at the prevalence of anxiety and depression in patients undergoing transrectal ultrasound (TRUS)-guided biopsy of the prostate. They found the pre-biopsy rates of anxiety and depression to be 7% and 1.4%, respectively, which is much lower than the results described here for patients undergoing flexible cystoscopy (15% and 3.5%, respectively). This may suggest that flexible cystoscopy in the context of the investigation of bladder cancer may cause greater anxiety and depression than TRUS-guided biopsy of the prostate and the potential diagnosis of prostate cancer. The population characteristics of these two groups are well matched in terms of patient ages and the socio-economic background as they come from a similar outer-London DGH population as well as being investigated for urological malignancy; however, the prostate biopsy cohort is a male-only group of patients. Forty one per cent of our cohort were women, a group in which we have shown anxiety and depression to be more prevalent. Further research is needed to discover whether the higher levels of anxiety in flexible cystoscopy patients are related to the perceived invasiveness of the procedure itself.
Further differences between the results of the present study and the TRUS biopsy cohort may be explained by disease-specific factors. Prostate cancer has a higher prevalence in the general population compared to bladder cancer and, due to the more high-profile nature of the disease, patients undergoing TRUS-guided biopsy of the prostate may be better informed compared to those being investigated for bladder cancer, in whom there may be a greater ‘fear of the unknown’. Additionally, for prostate cancer patients, a significant proportion are identified through opportunistic case finding in asymptomatic men, whilst patients undergoing flexible cystoscopy almost invariably have symptoms which might be perceived as being related to a cancer diagnosis.
For patients undergoing flexible cystoscopy, we found that patients who were not married/living as married were also at higher risk of anxiety and depression. The availability of personal home support mechanisms may explain the lower levels of anxiety and depression in patients co-habiting.
Our examination of which aspects of the diagnostic pathway cause the most concern to patient suggests that being told about the procedure, waiting for the procedure and undergoing the procedure itself were the most stressful steps of the diagnostic pathway for the majority of patients. Some of the stress related to anticipation of the procedure might be alleviated by accelerating the diagnostic pathway with innovations such as the two-week wait and the one-stop haematuria clinic. In addition, resources such as improved patient information, targeted counselling by a urologically trained professional or even referral to mental health services may help patients from ‘at risk’ groups.
The findings of this study should be interpreted in light of certain limitations. Self-reported data can be biased, particularly if patients are completing surveys such as this retrospectively. In addition, not every patient completed every part of the questionnaire. Furthermore, the study sample might not be representative of the population in general. Although we have used a population from two distinct sites – one from greater London, and another more suburban – demographic factors may have affected our results and they may differ from populations elsewhere in the UK or overseas. Although the majority of patients in this study were undergoing their first flexible cystoscopy for the investigation of haematuria, some patients may have had previous experience of flexible cystoscopy, which may have affected their experience during this study.
Conclusions
Our study looked at the prevalence of anxiety and depression in patients undergoing flexible cystoscopy and found it to be raised compared to a similar cohort of patients undergoing TRUS-guided biopsy of the prostate. We have identified subgroups more likely to experience these symptoms and have also identified the sections of the diagnostic pathway that are most likely to cause anxiety and depression. The data from this study may provide an opportunity to identify patients who are more likely to suffer from the diagnostic process and aim to improve their experience. Further research is needed to develop and evaluate targeted changes to the pathway to reduce psychological distress in this population.
Footnotes
Acknowledgements
None.
Conflicting interests
None declared.
Funding
None declared.
Ethical approval
Lister Hospital and Whipps Cross R&D and Audit Committee.
Guarantor
JG.
Contributorship
JG for concept and design. JG and SO for questionnaire collection. BL for data analysis and writing TMcN for initial discussions, identification of authors, advice as to progress of study and comments on final drafts. GE for data analysis and writing of paper.