
Abstract

Introduction
Ureteral injuries are uncommon, seen in approximately 3 per 10,000 trauma admissions, and occur more in penetrating than in blunt trauma. The most common associated injury for blunt ureteral trauma is pelvic bone fracture. 1
Blunt trauma patients with ureteral injuries are subject to extreme force applied over the entire body, such as a fall from a height or a high-speed motor-vehicle accident. The great degree of energy imparted to the victim is associated with such uncommon injuries as fractured lumbar processes 2 and thoraco-lumbar spinal dislocation. 3
First case report, August 1995
A nine-year-old pedestrian, knocked down by a car, had pain in the lower back and abdomen and abrasions on the right iliac fossa. X-rays of the cervical spine, chest and pelvis were performed, showing no fractures. An ultrasound scan of the abdomen was performed, showing bilateral pleural fluid and hepatorenal and pelvic fluid with no hepatic or splenic laceration.
A decision was made for follow-up ultrasound scan. Clinical signs of haemorrhage were evident later, and a repeat ultrasound scan was done, showing intra-abdominal haemorrhage. No haematuria was evident.
Laparotomy was performed by an experienced surgeon two hours after the initial presentation: 150 ml of blood was found intra-abdominally with active mesenteric bleeding, which was successfully controlled; no other organ injury was identified. Over the next seven days, there was slow progress with soft tissue swelling and bruising over the right loin. The patient was sent home on day 8.
At outpatient review on day 15, haematoma over the right loin was clinically evident. The patient was admitted for observation, then discharged as the haematoma was thought to be resolving.
On day 31, the patient was referred by his GP with right loin swelling, psoas spasm and hypertension. Ultrasound scan showed a large cystic lesion in relation to the right kidney and a referral to urology was made.
A CT scan was performed on day 32 with findings of urinoma, hydronephrotic kidney and possible upper ureteric injury (Figure 1). Right nephrostomy, antegrade study and drainage of urinoma were performed, with immediate improvement in blood pressure and symptoms (Figure 2).
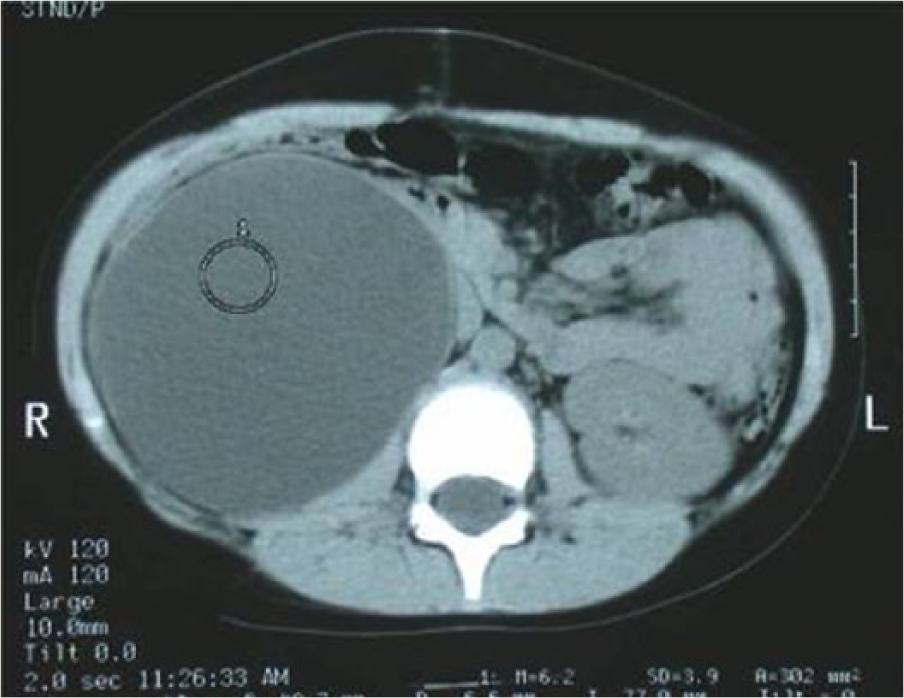
CT showing urinoma. Hydronephrosis was also demonstrated.
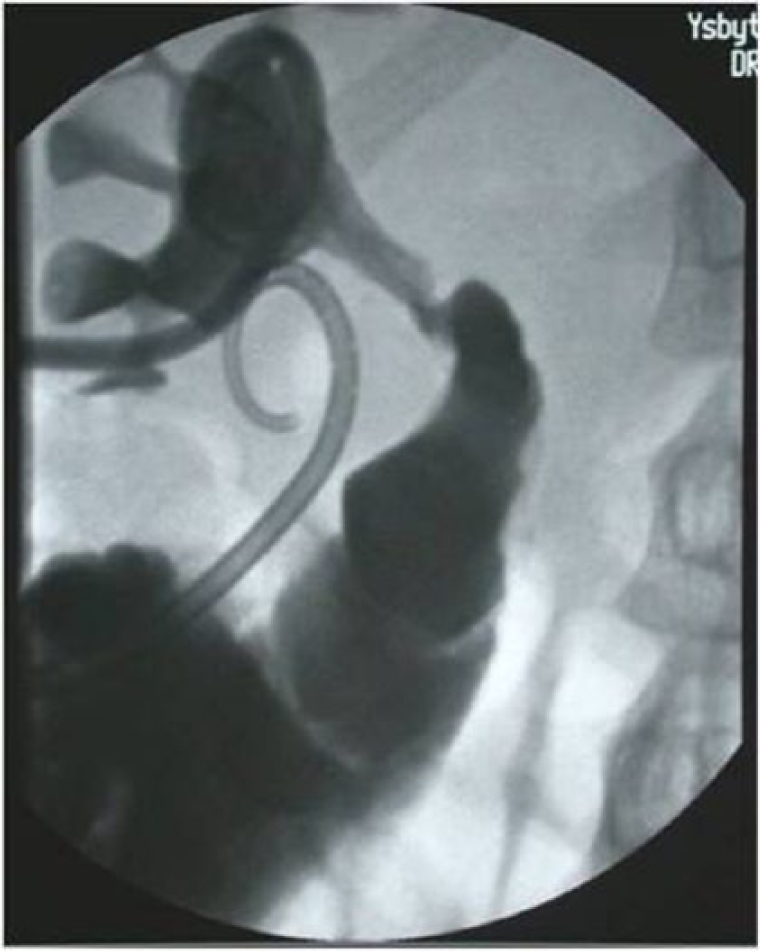
Antegrade study via nephrostomy with contrast flowing into urinoma.
A month later, right retrograde studies were performed, showing a blind-ending ureter with a large gap that was too long to be stented. Exploration of the kidney revealed fibrous tissue over the kidney and a fibrous long gap on the ureter with unhealthy ends; the renal pelvis was scarred up, but there was a good left kidney; hence, right nephrectomy was performed.
Follow up was done for seven years. Renal function remained good and blood pressure normal.
Second case report, January 2014
A 49-year-old male had had a blunt trauma four weeks prior to admission, while abroad, during a fight. He had been investigated for a collection, which was drained. No follow up was done.
The patient was admitted with left loin and left iliac fossa pain and tenderness. He was slightly tachycardic and hypertensive, with a creatinine level of 102, which went up to 114 over the next two days with no haematuria. An ultrasound scan showed a collection adjacent to the left kidney.
CT on day 4 confirmed the findings (Figure 3). Ultrasound-guided drainage was performed on day 5, and a clear urine-like fluid was drained. Analysis of fluid from the collection showed creatinine 2850 mmol/l, and urea 28.8 mmol/l, confirming the nature of the fluid as urine.

CT demonstrating left paranephric collection.
On day 6, a rendezvous procedure was attempted; retrograde ureterography demonstrated transection of the proximal third of the left ureter (Figure 4). A left nephrostomy was placed and contrast flowed freely into the collection adjacent to the left kidney.
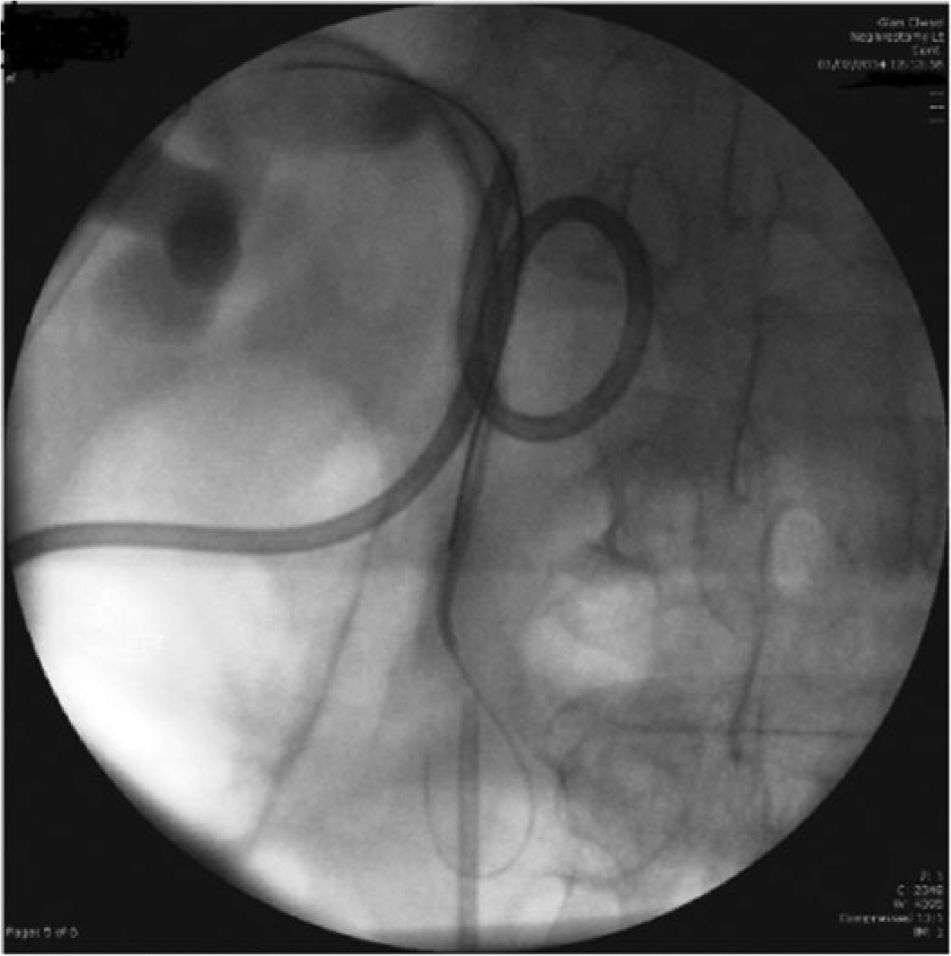
Rendezvous procedure demonstrated transection of the proximal third of the left ureter.
On day 9, exploration of the left ureter and end-to-end repair of the ureteric injury were performed. Both the nephrostomy and the JJ drain were left in. A nephrostogram was performed on day 16 with no significant leakage (Figure 5).
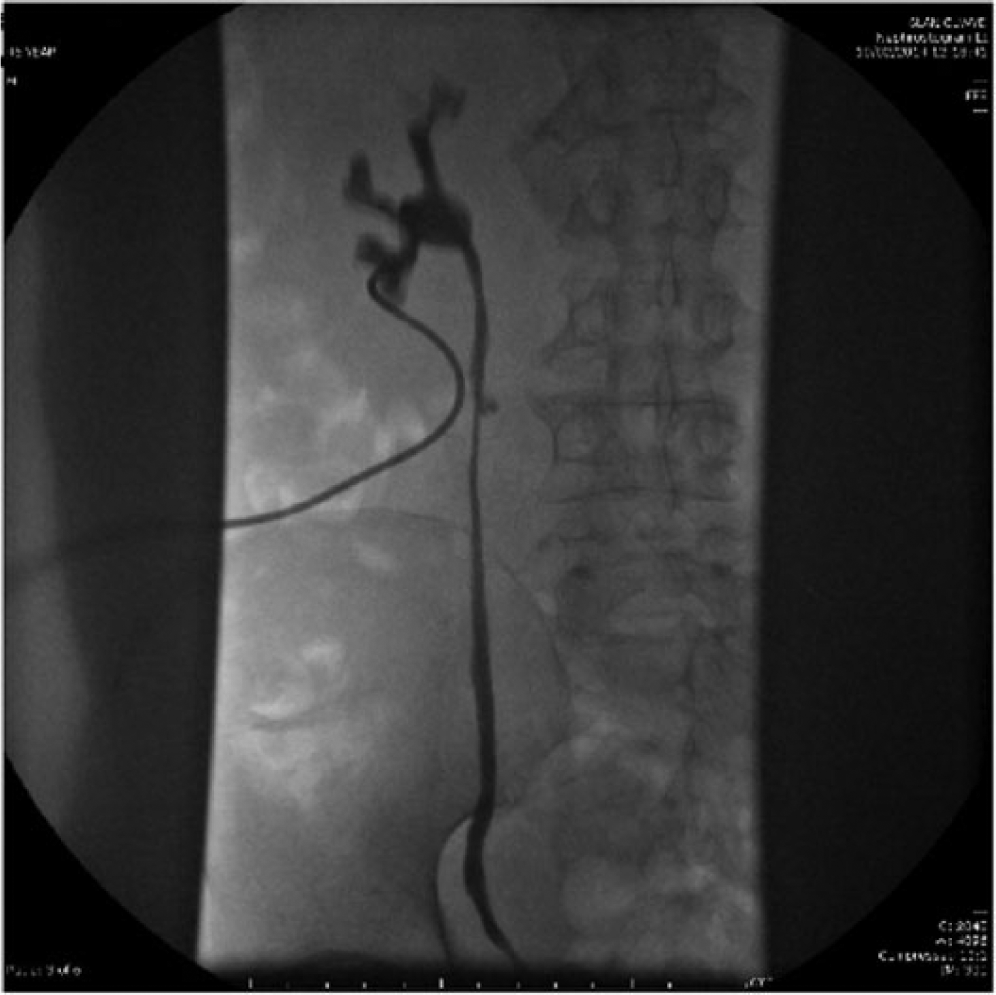
Nephrostogram on day 16 with no significant leakage.
Discussion
Ureteral injuries due to trauma are unusual. However, failure to take this type of injury into consideration can have dire consequences, as complications from missed injuries are a cause of severe morbidity and mortality. 4 The rare entity of ureteropelvic junction disruption consequent to blunt trauma is often missed because the patients do not always exhibit haematuria, and the injury is difficult to palpate during intraoperative manual examination. 5 Because of this, abdominal CT with contrast and delayed images whenever possible 6 is recommended. As we can see, CT scan was not routine for abdominal injury in 1995, and this led to a significant delay in diagnosis and poorer outcome in the first case. Currently, CT scan is well integrated in assessing abdominal trauma and/or suspected upper urinary tract injury; moreover, it is widely available, rendering it more practical.
The upper third of the ureter is more often injured than the middle and lower thirds. Associated injuries are present in 90% of patients; haematuria is absent on urinalysis in 55% of cases. 4 The mainstay of management of ureteral injury is anastomosis. Delay in diagnosis is associated with a worse prognosis. Ureteroureterostomy, with or without indwelling stent, is the surgical procedure of choice of both trauma surgeons and urologists alike. 4 Transureteroureteral anastomosis can also be used, depending on the site and the extent of injury. In distal ureter injuries a Psoas hitch or Boari flap can be employed.
Taking the possibility of blunt ureteric injury into consideration, proper imaging and early repair have a significant effect on improving prognosis.
Footnotes
Acknowledgements
None.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Informed consent for patient information to be published in this article was not obtained because of the time period involved (18 years).
Guarantor
VS.
Contributorship
VS is the surgeon under whose care patients were treated. Other authors are trainees who contributed to the literature search and compilation of the article.