
Abstract
This year’s British Association of Urological Surgeons (BAUS) Section of Academic Urology Annual Meeting took place on 1–2 December at The Royal College of Surgeons of England in London. Day 1, chaired by Robert Pickard, was dedicated to clinical trials in urology, celebrating our achievements, addressing the challenges, and exploring ways to advance practice through research. Day 2 consisted of presentations of on-going research work taking place across the United Kingdom (UK) and Ireland together with a ‘Dragon’s Den’, where trainees pitched ideas for research projects that could be taken forward by a national urology trainees research collaborative
Purpose of Meeting Day 1
The purpose of Day 1 was to launch the contribution from Urology UK to the Royal College of Surgeons of England (RCSEng) Clinical Research Initiative (https://www.rcseng.ac.uk/surgeons/research/surgical-research/surgical-clinical-trials). This initiative aims to increase surgical clinical research and ensure that the results are translated to improved patient care. Funding of £15,000 has been generously agreed from BAUS, the Trustees of BJU International Ltd, and The Urology Foundation to support the RCSEng clinical research leads; Mark Emberton (oncology) and Robert Pickard (Benign), to increase the number of urologists acting as principal investigators (PIs) for clinical trials and to ensure that all urology patients are offered participation in clinical research.
Presentations
Setting the scene: BAUS
Mark Speakman, president of BAUS, opened the morning. In his introduction he explained that the BAUS Section of Academic Urology was formed in 2007 to promote expansion of high-quality academic urology, to facilitate interactions between academic clinicians in the UK and Ireland and to act as a forum for discussion of clinical research. It has grown to 244 members, including 94 trainees, fulfilling its aim to nurture future academic urologists. He highlighted that BAUS research priorities involved ‘Cinderella’ topics such as pelvic pain and urinary tract infection (UTI) as well as life-threatening disease such as prostate cancer.
Mr Speakman put the research role of BAUS and its Academic Section into historical perspective, reminding us of the debt we owe to natural philosophers of the Age of Enlightenment: Robert Boyle, Humphrey Davy, and Michael Faraday. Not only do we share the same purpose – to reform society using reason, to challenge ideas grounded in tradition and faith, and to advance knowledge through the scientific method – but we also share the same methods, by clearly stating principles, using correct logic to arrive at conclusions, testing the conclusions against evidence, and then revising the principles in the light of that evidence.
Setting the scene: RCSEng
Dion Morton, director of clinical research at RCSEng, addressed the practical aspects of developing a trials culture in surgery and the role of RCSEng in the process. Less than 2% of government research funding goes into surgical areas despite a third of hospital admissions involving surgery. He highlighted the concern that clinical research in surgery is lacking, pointing out there were 10 times fewer active studies across all surgical specialties in 2011 than in cardiology alone! Professor Morton then introduced the new RCS Clinical Research Initiative: collaboration between the RCS, National Institute for Health Research (NIHR), Cancer Research UK and the Rosetrees Trust. This collaboration has established a network of surgical trials units and surgical research champions across the UK to support new studies across all surgical specialities, ensure innovations are introduced quickly and help reduce variation in care. The program is overseen by an independent steering committee (CRISC) chaired by Sir Michael Rawlins. To gain broad leadership, 16 surgical specialty leads have been appointed with the specific remit to develop new trials and establish clinical networks including patients. Prof Morton introduced Mark Emberton and Robert Pickard as the newly appointed specialty leads for urology, and expressed his hope that the recent success in clinical trial funding and completion run both by consultants and trainees in general surgery can be replicated in urology (Figure 1).
A clinical academic career in urology
To explore what makes a successful clinical academic, Mark Emberton chaired a discussion among three clinical academic colleagues: Dr Louise Dickinson, Ms Caroline Moore and Mr Hashim Ahmed. All three pursued research in urology, all three succeeded in it, yet each of them did it in his or her own unique way. Dr Dickinson explained how her experience as one of the first academic clinical fellows (ACF) provided opportunities and an environment for exposure to research during clinical training. Having organised a European Consensus Meeting on magnetic resonance imaging (MRI) for prostate cancer and then coordinated a large, multicentre study of focal high-intensity focused ultrasound (HIFU), she was able to develop academic expertise in a focused area and has pursued it further by starting radiology training following her PhD. Ms Moore confessed that she began with an MD ‘as a mean of obtaining a urology training number’. However, having been awarded her MD and the number, she chose to continue her research and with determined persuasion she created her own clinical lectureship. In contrast, Mr Ahmed decided early on an academic career and followed a more traditional pathway through a research fellow post, a Medical Research Council (MRC) Clinician Doctoral Research Fellowship, to his current MRC Clinician Scientist Award. Yet he too encountered similar difficulties and prejudices juggling the challenges of combining research with surgical training. Mark Emberton reflected that these stories from three different individuals show that whilst there is no one recipe for academic success, core ingredients are scepticism, inquisitiveness and drive for clinical and academic excellence.
Conducting clinical research as a full-time National Health Service (NHS) clinician
The challenges of achieving results as a research-active NHS consultant were explored by John McGrath and Sam McClinton. They explained that whilst ample opportunities exist, there are multiple hurdles to overcome in to successfully lead clinical research whether NIHR-funded trials, researcher-led studies, or commercial projects. The ethos, experience, credibility and performance of one’s centre, along with navigating the research regulatory arena, can be some of the generic challenges to set up a research unit. Mr McGrath observed that priorities of your employer can easily lie elsewhere and involvement in research can attract criticism, with clinical work always being the trump card. Additionally, local funding can be too small to be meaningful, and the peaks and troughs in funding can be difficult to weather. Research must be a team effort rather than an individual venture, with support from the NHS organisation, patients, and most importantly departmental colleagues being crucial to success. With time always at a premium, Prof McClinton listed ways to make the experience easier and more effective, by being realistic, by planning around one’s own clinical and commitments and source of funding, and by seeking help, both from one’s mentor and the wider team.
Effective research from drawing board to delivery
To conclude the morning talks, Vicki Barber, Rebecca Lewis and Wendy Robson brought together the various points raised throughout the day, focusing on what makes an effective and successful clinical research team. Dr Barber, clinical trials unit manager in Oxford who is supported by the RCS Initiative, introduced the ‘strategies for trial enrolment and participant study’ STEPS, a joint NIHR Human Tissue Authority (HTA)/MRC project which concluded that the three factors successful trials share are: being a cancer or drug trial, having interventions only available inside the trial, and having a dedicated trial manager. A quote from Peter Davidson from the NETSCC emphasised the funder’s perspective, that ‘it is vital that a person leading a trial has good management leadership skills rather than merely energy and scientific curiosity’. Dr Barber encouraged the triallists to seek input from the surgical trials units Prof Morton spoke so keenly about, as an invaluable source of not only expertise, continuity and stability, but also infrastructure, quality assurance, information technology (IT) and statistical input. Ms Lewis, senior trials manager at the Institute of Cancer Research, explained how a collaborative and pragmatic approach to implementation of trial design into clinical care was required. Trials had to fit the scope and paradigm of the current practice and target population, minimising the burden on the patients and teams. Every trial was a learning experience that could be translated to improving running of the next study. Wendy Robson, leader of the urology and renal clinical research team at Freeman Hospital, Newcastle upon Tyne, used real examples to illustrate aspects of trial design that bring either joy or heartsink to an NHS research nurse. The key is a good balance between the needs of the research question and the needs of the patients involved. Effective leadership from the local PI with clearly defined responsibilities and time frames are essential together with clear trial documentation. Things to avoid include lack of flexibility in time points, patient questionnaire overload, burdensome distracting ‘sub-studies’ and data collected ‘because you can’ rather than required for primary analysis. All three speakers emphasised the need for timely, two-way communication between trial designers and those who deliver clinical research to allow completion to time and target and speedy implementation of clinically-relevant results.
Summary
These varied talks emphasised the will and enthusiasm to drive advancement in urology patient care through clinical research and demonstrated that much was already being done. The challenge will be to improve on this platform and spread the message through all UK urology departments.
Discussion group I
Aligning trial design to the clinical problem
Framing the problem
During the afternoon of Day 1, delegates split into two discussion groups. The first discussion led by Mark Emberton centred on trial design and was facilitated by contributions from five invited experts: Dr Clare Relton, Professor John Norrie, Dr Jan van der Meulen, Dr Emma Hall and Dr Susan Dutton. The task was to fit the research design to the ‘value’ of the answer for any given research question with the need to explore alternatives to the ‘gold standard’: the randomised controlled trial (RCT). The opening statement from Prof Emberton that ‘all research comes from a hunch that something isn’t quite right and could be improved’ led the audience to consider examples of challenging research questions.
A worked example
To focus discussion, the research question ‘Can extended lymphadenectomy with prostatectomy compared to radical prostatectomy alone improve morbidity and mortality in men with intermediate risk localised prostate cancer?’ was introduced. Defining the study population, standardising the technique for lymphadenectomy and ensuring comparable surgical expertise were listed as some of the design issues the researcher was likely to face. The panel and the audience agreed that setting strict inclusion and exclusion criteria, common practice for regulatory drug trials, led to poor recruitment and selection bias. The trial population would tend to consist of patients likely to gain maximum effect, whilst excluding minorities, those hard to reach, and those at greater risk of harm. This could lead to disparities between the target and populations, resulting in a study result lacking generalisability to routine care. The decision whether to keep the intervention simple, i.e. surgical and controllable, or more generalised, i.e. complex but potentially beneficial to more patients, was another challenge given to the audience. Potential for contamination of the results by requiring treatment by two specialists was suggested as a reason for keeping things simple. It was commented that undertaking single-centre trials of treatments in different populations by different research teams leads to clinical and statistical heterogeneity which hampers meta-analysis of the results and makes translation to clinical care uncertain; much better to have just one large definitive study.
For study outcome measures, the panel and the audience were agreed that ambiguity should be avoided by making the outcomes clear and specific. One-dimensional outcomes were considered rare and unlikely in surgical research, and so the primary outcomes could include morbidity, quality of life, recurrence-free survival and overall survival. End-points should be relevant and acceptable to the patients, something that can be demonstrated by involvement of patient groups in trial design at an early stage. Whilst it was widely acknowledged that failure to recruit to target has implications for the power and generalisability of trial results, the panel questioned whether for many circumstances the existing evidence could be used to answer the research question. The audience pointed out that in the example of lymphadenectomy with radical prostatectomy, data from single-centre case series and small studies were already available. With clinical practice constantly evolving, data from large trials begun 10 years ago may be invalid to current practice. Patients and their circumstances also evolve over time, affecting the clinical decisions made. With progress in care over time often reducing the value of large trial results, new approaches are needed to fit the research design to the ‘value’ and urgency of the answer.
Dr Clare Relton’s example from a systematic review (Ross et al. J Clin Epidemiol 1999; 52: 1143–1156), stating that ‘most common reason given by patients and clinicians for not participating in clinical trials is related to concerns about information and consent’ sparked a discussion on the issues surrounding ethics and consent. She further challenged the audience to the concept of: ‘Random allocation is something “done” to all, whilst random selection ‘happens’ to some’. It was pointed out that unlike patients receiving routine care, patients consenting to participation in clinical trials are fully informed pre-randomisation about treatments they may or may not receive, or that their treatment will be decided by chance. Some members of the audience suggested that patients need to be consented for randomisation only if their allocated treatment was different from usual care, as by prospectively informing people we change the way they act. Mr Jan Nawrocki felt that this is contrary to routine clinical practice, where available options are explained and advice is given on the best course of action. The audience agreed that whilst this is the case in elective circumstances, it may not strictly apply to clinical trials. Mr Nawrocki further remarked on the new General Medical Council (GMC) definition of consent, implying that patients now request treatment and the clinicians consent to provide it. The panel concluded that consent is a marriage of a transaction and a dialogue.
Alternative trial designs
Prof Emberton expanded further on alternative trial designs which could be more suited to the ‘value’ and immediacy of the answer. The examples given by the audience included cluster randomisation, embedding clinical trials into observational registries and cohort studies, and more pragmatic design in line with current practice, such as Zelen’s randomised consent design. The impact of these alternatives was debated, with the audience feeling strongly negative about cluster randomisation, raising further concerns around ethics, patient preferences and consent. When further questioned by Prof Emberton about ways of making it easier to design a publishable study, the audience mentioned adaptive, pragmatic and non-inferior design methods. The panel agreed that in the current constantly evolving world where new markers and treatments emerge regularly, the setting and the objectives of a study may change with time, requiring an adaptive pragmatic design. Recruiting heterogeneous populations and focusing on effectiveness rather than efficacy of the intervention, pragmatic trials have high external validity and can immediately inform practical health care decision making if analysed by an experienced researcher. However, their external validity can be limited to specific health care settings. Prof John Norrie quoted, as an example, a study his team recently published (Brittenden et al. N Engl J Med 2014; 371: 1218), which, although relevant to UK practice, received criticism from the United States (US) audience, who could not extrapolate its findings. Lastly, in studies where use of a superiority trial against a placebo control may be considered unethical, non-inferiority trials were suggested as an alternative, but were heavily criticised by the panel due to large sample requirements and the risk of progression to an inferiority trial.
Dr Relton then introduced the ‘cohort multiple randomised controlled trial’ (cmRCT) design (Relton et al. BMJ 2010; 340: c1066) as an innovative approach that rethinks the nature and infrastructure of pragmatic RCTs, how trial populations are identified, concept of randomisation, and the time and content of information given to the patient. The cmRCTs’ design allows recruitment of large observational cohorts of patients with regularly measured outcomes. This then provides the resource for multiple trials (both concurrent and subsequent) over time, thus saving time and cost. The audience saw the potential of such design, especially in studies where large populations are recruited and suggested that in a study cohort of 20,000, one could collaborate with research groups to formulate 20 different hypotheses and conduct 20 parallel trials. For each trial only some patients from all eligible individuals within the cmRCT cohort are randomly selected and offered the intervention. Direct comparison can be made of the outcomes in the randomly selected patients with others in the cohort having standard care. On recruitment to the cmRCT cohort, patients consent only to being followed up for life, periodically filling in questionnaires, being approached if new recruitment becomes available, and having their biographical data safely stored. Further participation in the ‘nested’ trials then requires additional consent. Prof Emberton felt that the beauty of this method is that everyone carries on doing what they are doing (non-disruptive), few get selected, but all have a chance of being approached giving equity of access. There is a limitation that a standard care comparator is required and this risks non-acceptance and non-compliance among those with high preference against the intervention under test.
Summary
Looking into the future, the audience concluded the session by identifying our main challenge to be the advancement of robust cancer registries, which would reflect changes in patients’ clinical status, e.g. progressing from one stage of disease to another, thus allowing the researchers to identify those potentially eligible for new trials.
Discussion group II
Delivering effective patient recruitment
The second discussion group was chaired by Rob Pickard and looked at various factors that may encourage or prevent recruitment at a local level to clinical trials in urology. Experts with ‘on-the-ground’ experience including presentations from John McGrath, Rebecca Lewis and Wendy Robson, and contributions from Sam McClinton and Rachel Stephenson, helped facilitate the discussion under specific headings.
Local feasibility
Discussion established that it is vital that individual departments make realistic predictions about the numbers of people they are likely to be able to recruit in a specified time period before agreeing to act as a local trial site. It is important to realise that only a relatively small proportion (≈25%) of the total local patient population eligible for the trial is likely to be recruited. This prediction must take into account the local resources available. Delegates both from trial management and clinical research teams agreed it is harmful all round if local feasibility is not established at the start.
Identify support
The NIHR infrastructure provides considerable support across England for all NHS organisations. The main difficulty is accessing it for a specific study. The clinical research team members emphasised the need to engage with the relevant local NIHR clinical network (LCRN) lead. The LCRN also provide training, particularly Good Clinical Practice (GCP). John McGrath pointed out it is important to have buy-in from clinical colleagues that recruitment to trials was a routine part of departmental business.
Local set-up
Trials come with a fair amount of administrative paperwork both in set- up and continuation. The trial managers, clinicians and research teams present emphasised the importance of keeping good records of permissions to carry out the research and continued documentation of progress of the trial locally. All agreed that the headache of inspections and audits is best relieved by proper record keeping from the start.
Identification of eligible patients
Wendy Robson emphasised the importance of mapping out the journey of patients eligible for a trial and working out the best time and place to approach them. This involves collaboration with the clinical team and an easy line of communication with the research nurse. Rapid responsiveness by the research nurse team and ready availability of trial documents for interested patients is also very important. The difficulty of identifying patients who present ‘out of hours’ was highlighted and possible solutions, such as ensuring that on-call medical staff were all GCP trained, discussed.
Recruitment, retention and follow-up
The difficulty of recruiting to trials where the treatment options being tested were already available in the NHS was acknowledged and a number of strategies to ensure that patients were given a fair picture of the uncertainties that generated the need for the trial were put forward. The importance of approaching the patient at the right time and of ensuring that all clinicians were able to express the uncertainty of current practice was emphasised. Another workable option is for clinicians to ‘cross-refer’ patients eligible for a trial to the main clinician to get a consistency of approach. Hand-in-hand with this was the advantage of using various promotional materials to ensure clinicians, support staff and patients maintain awareness of the trial. This is also helped by regular meetings and updates to all involved.
Measuring and maintaining activity
All present acknowledged that success in recruitment breeds further success and additionally is the main measure by which NHS organisations and individual departments are judged. High recruitment brings more resources to the NHS organisation through the NIHR accrual-related support and additional LCRN-funded research staff. Unfortunately this extra support may not fully filter down to department level so it is an important part of the PI’s job to help emphasise the importance of success in a recruiting to a particular trial and encourage the team. Friendly competition between units was thought to be helpful but sharing strategies that helped increase recruitment would be best in the longer term.
Summary
The conclusions of the wide-ranging discussion were that successful and satisfying local involvement in multi-centre trials can be achieved, but does require effort, often unsung, and knowing where to get help, advice and support. It was felt that the BAUS website would be a good forum to provide generic advice and points of contact to help individuals and departments new to clinical trial work.
Purpose of meeting Day 2: Tuesday 2 December 2014
Introduction
The second day of the meeting chaired by Mr Vincent Gnanapragasam and Professor Robert Pickard was the BAUS Academic Section of Urology Annual Research Meeting and was a highly successful event. More than 50 delegates took part in an exciting day of presentations and discussions with the inclusion of two new features: the inaugural BAUS Academic Section of Urology Research Prize, and a ‘Dragons’ Den’ style competition for urology trainees seeking to set up collaborative regional or national studies in line with one of the strategies of the RCSEng Clinical Research Initiative.
Summary of the day
More than 40 abstracts were presented and these were all of a high calibre. The top 10 scoring abstracts were selected for podium presentation, while the remainder were presented as posters in three sessions. Podium presentations were judged by a panel of experts and the BAUS 2014 Academic Research Prize was awarded to Alexander Laird from Edinburgh. The presenters of the best posters judged from each of the three ‘poster rounds’ were Marcus Cumberbatch, Robert Foley and Elsie Ellimah Mensah. Many congratulations to these prize winners for their achievement. All the abstracts of the podium and poster presentations are included as part of this report. The ‘Dragons’ Den’-style session was a new feature organised by Ben Lamb, in which trainees were invited to submit ideas for collaborative regional or national audit, service development and research. After extensive debate around the criteria of ‘do-ability’ and maximising trainee involvement, the panel of ‘Surgical Dragons’ declared Taimur Shah as the winner for the project entitled ‘Role of inflammatory markers in ureteric colic and UK Stone Nomogram’.
Concluding remarks
The judges and participants were all highly impressed by the quality of the research being undertaken by the urology trainees and this augurs well for the future of academic research in urology. There was general agreement that this format was encouraging participation and would be taken forward to the next annual meeting and the Academic Section prize and the Dragons’ Den will remain as features.
Abstracts of prize-winning presentations
BAUS 2014 academic research prize winner
‘Best in session’ poster presentations
We found that the presence of the LUZP4 protein in cancer cells is associated with low levels of the ALYREF protein and vice versa. We observed this inverted correlation expression in 80% of the cancer cell lines tested, which included bladder cancers. Furthermore, LUZP4 supports transport of transcripts required for cancer cell growth and tissue invasion, confirmed by a dramatic reduction of cancer cells proliferation upon knockdown of LUZP4 by RNAi.
‘Dragons’ Den’ winner
Creation of a prospective database to assess secondary factors such as Hounsfield units, comorbidities (diabetes), pain score, previous history of stones to eventually create a nomogram.
Paper Session 1: Professor Rob Pickard, Mr Derek Rosario, Mr Richard Bryan and Professor Noel Clarke
Tuesday, 2 December 0920-1105
Paper Session 2: Professor Rob Pickard, Mr Derek Rosario, Mr Richard Bryan and Professor Noel Clarke
Tuesday, 2 December 1145-1330
Importance: If local therapy of the primary tumour in metastatic prostate cancer improved survival, this would herald a paradigm shift in treatment.
Objective: The objective of this research is to determine whether radical therapy locally directed to the primary tumour in men with likely or definite metastatic prostate cancer improves survival.
Design: An observational cohort study of 18,352 men with likely or definite metastatic prostate cancer (PSA > 50) treated by initial radical therapy (radical prostatectomy or radiation therapy) or initial androgen-deprivation therapy, and followed for up to 15 years.
Setting: The PCBaSe dataset provides information on >98% of patient and tumour characteristics of virtually all prostate cancer cases in Sweden diagnosed since 1998. We identified men with PSA > 50 ng/ml, and compared prostate cancer and other-cause mortality between radically treated and androgen-deprivation groups. We matched treatment cohorts for PSA, clinical stage, M-stage, tumour grade, Charlson comorbidity index, age, and year of diagnosis, and repeated comparative effectiveness analyses.
Exposures: One group received initial therapy with either radical prostatectomy or radiation therapy, and the other group received initial androgen deprivation.
Main outcomes and measures: We compared competing risks adjusted prostate cancer mortality, calculating crude, traditional (multivariable) adjusted, and propensity score adjusted subdistribution hazard ratios for comparisons between the treatment groups.
Results: Prostate cancer mortality was substantially greater in the androgen-deprivation group compared to the radically treated one, in unmatched (9062/17,602 = 51.5% vs 86/750 = 11.5%, respectively) and matched (177/575 = 30.8% vs 71/575 = 12.3%, respectively) cohorts. Among the matched cohorts, androgen deprivation was associated with a nearly three-fold increase in risk of prostate cancer death compared with locally directed radical therapy (2.87; 95% CI 2.16–3.82). Multiple sensitivity analyses suggested the findings were robust.
Conclusions and relevance: This is the largest and most comprehensive population-based observational study to address the efficacy of radical therapy in men with likely metastatic or micro-metastatic prostate cancer. The results indicate a survival benefit for locally directed radical treatment in men with metastatic prostate cancer and provide a strong rationale to consider a randomised controlled trial in this setting.
Across the TMA, 84% of tumours demonstrated intermediate/high CYR61 expression compared to 62% of normal controls (p < 0.01). Intermediate/high vs. negative/low expression was associated with significantly reduced overall (median 33 vs. >72 months) and cancer-specific (39 vs. >72 months) survival following cystectomy. Expression was an independent predictor of survival, HR 1.493 (p = 0.030, Cox regression).
Posters Round 1: Mr Ghulam Nabi and Professor Jenny Southgate
Tuesday, 2 December 1105-1145
Gene copy number losses and gains were similar throughout the cohort, but using multi-Fisher’s exact test adjusted for multiple comparisons, statistically significant differences were observed in specific loci, between HPV-positive and negative tumours, tumour subtype, grade and nodal status.
Posters Round 2: Professor Sam McClinton and Mr Prasanna Sooriakumaran
Tuesday, 2 December 1330-1430
Introduction: The inhibition of poly(ADP-ribose)polymerase 1 (PARP1) leads to double-stranded breaks (DSBs), and is synthetically lethal in BRCA1/2-deficient cells. We investigate the ability to reproduce this therapeutic effect in prostate cancers which often possess functional BRCA1/2, through the dual inhibition of PARP1 and the DSB-sensor protein, ataxia-telangiectasia-mutated (ATM).
Methods: A dual combination of ATM and PARP1 inhibition using KU55933 and olaparib respectively was compared to their use as single agents or DMSO, in a non-neoplastic immortalised and castrate-resistant prostate cancer (CRPC) cell line (RWPE and C42) across a range of assays: confluence-based proliferation, cell viability, and colony-forming assays; flow-cytometry-based cell cycle analysis; γH2X and RAD51 formation by fluorescence microscopy and Western blot; homologous recombination was measured using a direct-repeat-green-fluorescent-protein reporter assay (Nakanishi, 2011). In vivo drug effects were evaluated by subcuticular C42-LM (luciferin-expressing) xenografts established in NOD-SCID mice; and ex vivo, a novel patient-derived CRPC tissue assay was designed and used with Ki-67/cleaved-caspase-3 immunohistochemical analysis after five days of drug treatments.
Results: The combinatorial effect of PARP1 and ATM inhibition are synthetically lethal in prostate cancer cells, in vivo and ex vivo, with minimal effects in benign prostate cell lines. The combination therapy results in a reduction in γH2X and RAD51 assembly, significantly less homologous recombination and greater G2/M arrest than with each inhibitor alone.
Discussion: We describe a new mechanism of synthetic lethality through which the potentiation of stalled replication forks using PARP inhibition and the abrogation of DSB repair with ATM inhibition results in prostate cancer-selective reduction in growth.
Risk ratios were calculated and comparisons between groups were made with Chi-squared test using SPSS.
The odds of being Black-Caribbean (OR 0.27, CI 0.07–1.07, p = 0.045), Black-African (OR 0.27, CI 0.07–1.07, p = 0.046) or White-British (OR 0.44, CI 0.30–0.66, p < 0.001) were significantly lower among the colic population.
The odds of being Lithuanian or Polish were not statistically significant.
Progression was defined as either biochemical recurrence using the ASTRO-Phoenix criteria (prostate serum antigen (PSA) >nadir+2 ng/ml) or start of hormone therapy/second-line treatments or development of metastases.
Overall, one-, three- and five-year progression-free survival (PFS) (composite) rates were 71%, 31% and 17%, respectively.
When comparing patients with PSA nadir ⩽0.5 ng/ml, PSA nadir >0.5 and PSA non-responders, a statistically significant difference in PFS was seen (p < 0.05). Three-year PFS in each group was 42%, 15% and 0%, respectively.
Early in the learning curve, between 2005 and 2007, four of 52 (7.5%) developed recto-urethral fistulae. Intervention for bladder outlet obstruction was needed in 28/52 (54%).
Introduction: Robotic-assisted laparoscopic radical prostatectomy (RARP) is a current standard treatment for localised prostate cancer, and treatment failure is defined by biochemical recurrence (BCR). Open prostatectomy series identify positive surgical margins (PSM) as predictors of cancer recurrence. We assess patients with localised prostate cancer treated with RARP across three high-volume institutions, and assess the impact of margin parameters on BCR.
Methods: De-identifiable clinical and pathological data was collected for more than 4000 patients with three or more years follow-up. Three statistical models were employed to evaluate the effect of margin parameters on recurrence: crude rates, traditional multivariable Cox regression and a propensity-adjusted model.
Results: Ten per cent of men with negative margins developed recurrence compared with 37% of men with a PSM (HR = 1.81, 95% CI: 1.47–2.22). Multifocality and length ⩾3 mm carried greater risk of BCR than negative margin cases. Considering only the PSM cohort, multivariable Cox regression revealed only apical margins significantly predicted BCR relative to basal margins (HR = 2.03, 95% CI: 1.01–4.09). In contrast there was no statistically significant difference in BCR rates for postero-lateral margins (HR = 1.62, 95% CI: 0.84–3.11). Propensity-adjusted modelling was used to confirm this smaller effect of postero-lateral margins compared with apical margins.
Conclusions: PSM lengths which are ⩾3 mm, and to a lesser extent multifocality in general, are predictive of BCR. Surprisingly, compared with open prostatectomy series, postero-lateral margins are less likely to result in BCR than apical PSMs.
We aimed to evaluate the utility of repeating semen analysis in patients undergoing bilateral vasectomy.
Posters Round 3: Professor Prokar Dasgupta and Mr Erik Mayer
Tuesday, 2 December 1600-1640
Characteristics of patient group.
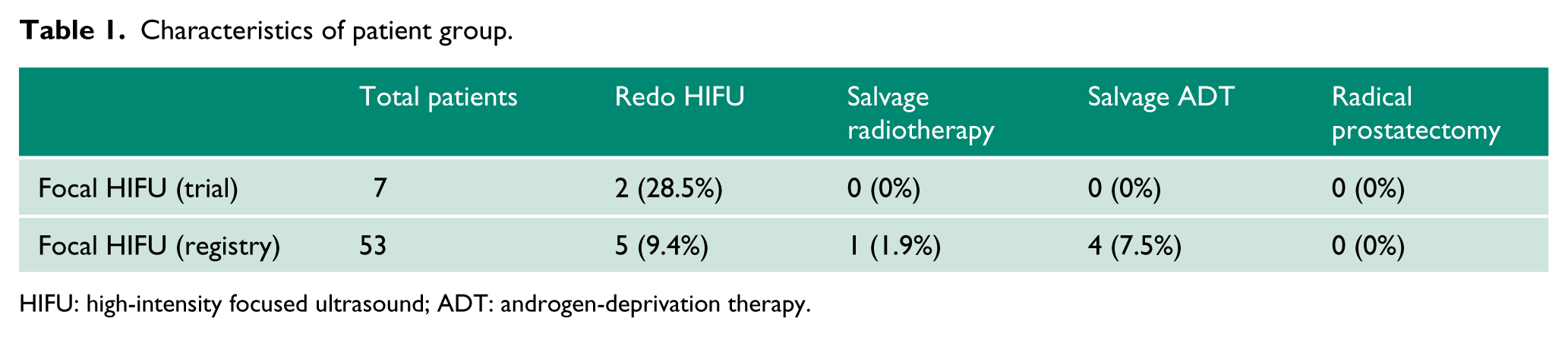
HIFU: high-intensity focused ultrasound; ADT: androgen-deprivation therapy.
Table 2 outlines the complication rates associated with focal HIFU.
Outcomes.
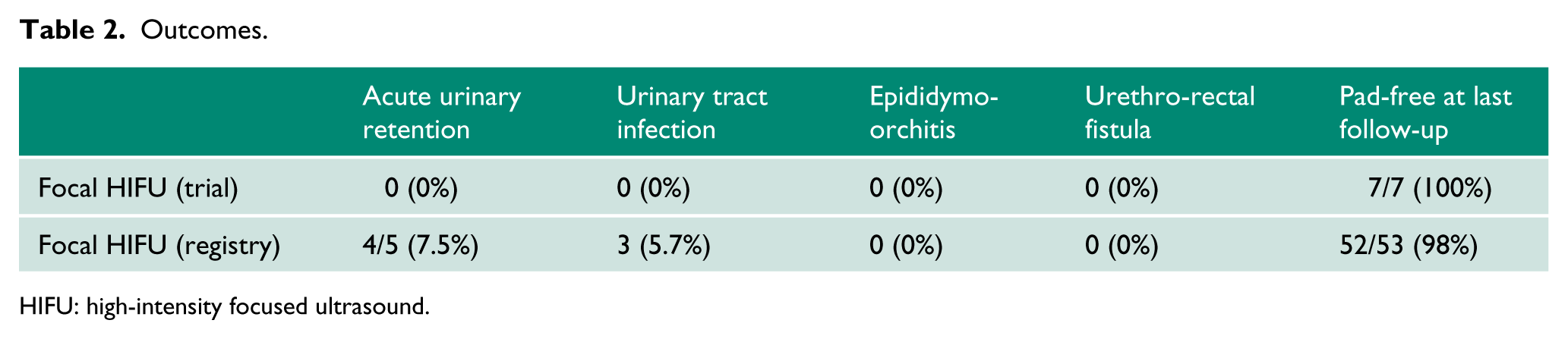
HIFU: high-intensity focused ultrasound.
The objective was to create a consensus statement and guidelines on the initial investigation of a patient with sterile pyuria.
There is a problem in the proper positioning of antegrade ureteric stent with the use of ordinary guide wires. The upper J tip of double J stent is difficult to adjust well in the proper position.
To our knowledge there are no reports mentioning the use of specific types of guide wire except what we have: the straight or J tip guide wire. We designed a special type of guide wire to be circular, floppy and straight ended, which is very helpful for the proper positioning of the upper J tip of ureteric stent.
If the upper J end of the stent with the floppy, circular part of the guide wire inside is in the narrow space as in the upper ureter or in kidney parenchyma, the coiled shape will not occur, thereby indicating the improper positioning of the double J stent.
Dragons Den – Urology’s Got Talent Proposals: Professor Rob Pickard, Mr John Kelly and Mr Tom Pinkney
Tuesday, 2 December 1430-1600
Charing Cross Hospital, Imperial College Healthcare NHS Trust
In modern urological care, ‘forgotten ureteric stents’ still occur, resulting in harm to patients and financial burden to health care systems.
We have developed a novel smartphone application (StentbookTM) to quickly upload stent information on insertion, and log stent removal at a later date, again using the application. StentbookTM triggers an automated email to the clinician and SMS message when a stent is not logged out, in a given timeframe set by the clinician. The application aims to provide a safety net, hopefully minimising the risk of the ‘forgotten stent’, and making the process of entering stent information simple for the clinician, without the need to log into a computer.
The population to be investigated are patients undergoing urological or radiological stent insertion over a six-month period. The intervention proposed is the use of the StentbookTM application. The comparator group will be patients undergoing stent insertion without use of the smartphone application to act as a safety net. The outcome will be the number of overdue or forgotten stents in each group.
Implementing our study at a trainee level across multiple sites will not require additional resources or funding, and if successful may improve patient safety.
Percutaneous nephrosotomy
Endoscopic ureteric stent
No intervention (for example, if patient declined, medically unfit, not clinically appropriate)
Primary outcomes are:
Initial success/failure rate of each procedure (successful placement of percutaneous nephrostomy or ureteric stent)
Improvement of renal function (measured at two weeks following intervention)
Clinical outcome at three months (patient alive or dead)
Secondary outcomes are:
Number of patients requiring further radiological intervention (for example antegrade stent or change of nephrostomy/ureteric stent)
Number of patients undergoing surgery for ureteric obstruction
Numbers of patients requiring palliative care
In pelvic malignancy, patients presenting with acute ureteric obstruction may achieve better renal function with percutaneous nephrostomy compared to ureteric stent placement.