
Abstract
Objective:
To develop a tool, both simple and reliable, for postoperative percutaneous nephrolithotomy (PCNL) stone-free failure prediction.
Materials and methods:
We analysed a sample of 116 patients, who underwent conventional PCNL from 2011 to 2014. Cases with residual stones ⩽ 4 mm in size were regarded as clinically insignificant and ‘stone-free’.
Results:
According to the low-dose computed tomography (CT) scan performed within 24 hours after operation, the patients were stratified as follows: 72 stone-free and 44 with residual stones. Among the analysed variables, three were derived as most important for prediction purposes: an additional stone in a calyx with an acute angle (⩽ 45°), represented by ‘A’; an additional stone in a long calyx (⩾ 10 mm) with a narrow infundibulum (⩽ 8mm), represented by ‘C’; and a stone size that is > 24 mm, represented by ‘S’. These were abbreviated as the ‘ACS’ score. Depending on the absence or presence of each of these three variables, a score of 0 or 1 was assigned. If the ACS score is 0, then the probability of being a stone-free patient was about 88%; however, when the ACS score is 3, then the probability of being stone free was just 8%.
Conclusion:
Use of the ACS score seemed to be a simple and reliable tool for PCNL stone-free failure prediction.
Keywords
Introduction
Since introduction of percutaneous nephrolithotomy (PCNL) into clinical practice in 1941, when Rupel and Brown performed the first nephroscopy, application of this method has undergone steady growth, with the number of PCNLs performed annually in the USA increasing by 47%, between 1999 and 2009.1,2 It is not a secret that reduced achievement of subjective preoperative surgical goals are associated with decreased patient satisfaction; thus, ability to predict the stone-free rate before operation leads to accurate patient counselling, better surgical planning and might serve to obtain better surgical outcomes. 3 A number of approaches to predict the postoperative stone-free rate were developed: STONE nephrolithometry, 4 GUY’s stone score, 3 Staghorn morphometry, 5 the logistic regression model, 6 K1–4 classification, 7 the Nephrolithometric Nomogram proposed by CROES, 8 etc. Although these tools are able to provide predictive value, unfortunately, they are not without drawbacks; being cumbersome in one case and non-reliable in the other cases. Therefore, reliable prognostic tools are needed to counsel patients preoperatively, optimize treatment selection, plan surgery and evaluate outcomes. 8 Our main objective was to develop both a reliable and at the same time simple tool, which could be helpful in routine urological practice.
Materials and methods
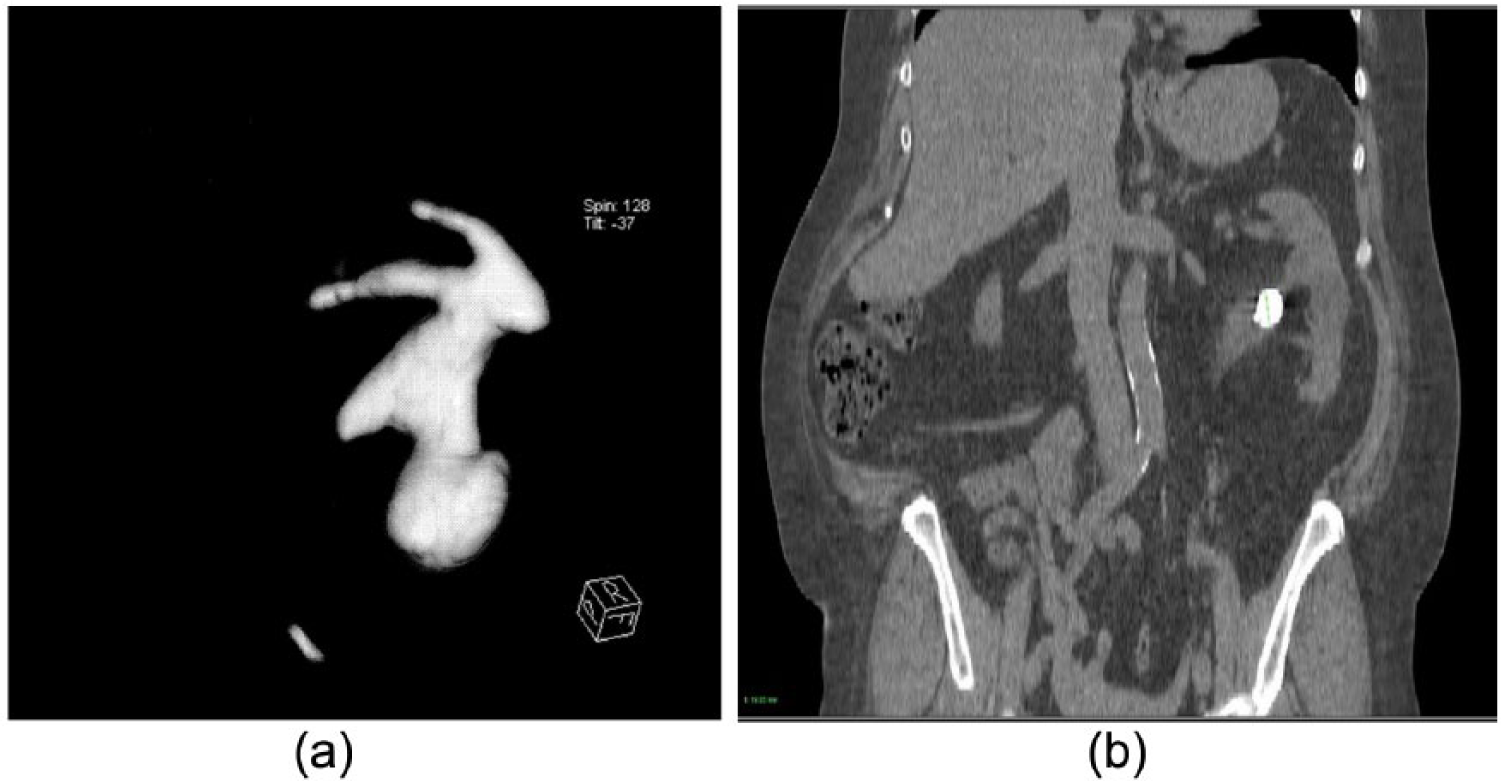
After institutional ethical committee approval, we retrospectively evaluated a sample of 116 patients from 2011 to 2014. The most influential variables affecting the PCNL stone-free rate, according to the publications we extracted from PubMed and Google Scholar, using main keywords such as ‘PCNL’, ‘prediction’, ‘scoring system’, ‘stone-free’ and ‘outcome’ were: age, sex, body mass index (BMI), stone density, operative time, hydronephrosis, laterality, number of tracts, American Society of Anesthesiologists (ASA) grade and number of PCNL sessions. Additionally, three parameters are gained with multiplanar reconstruction of computed tomography (CT) data (Figure 1): A stone in a calyx with an acute angle to the main stone burden, ⩽ 45° (‘Acute Angle’ or ‘A’); a stone in a long calyx (⩾ 10 mm) with narrow infundibulum (⩽ 8 mm), in additional to the main stone burden (‘Complicated Calyx’ or ‘C’) and a ‘Stone Size’ or ‘S’ measured in the longest dimension of that stone’s mass (mm).
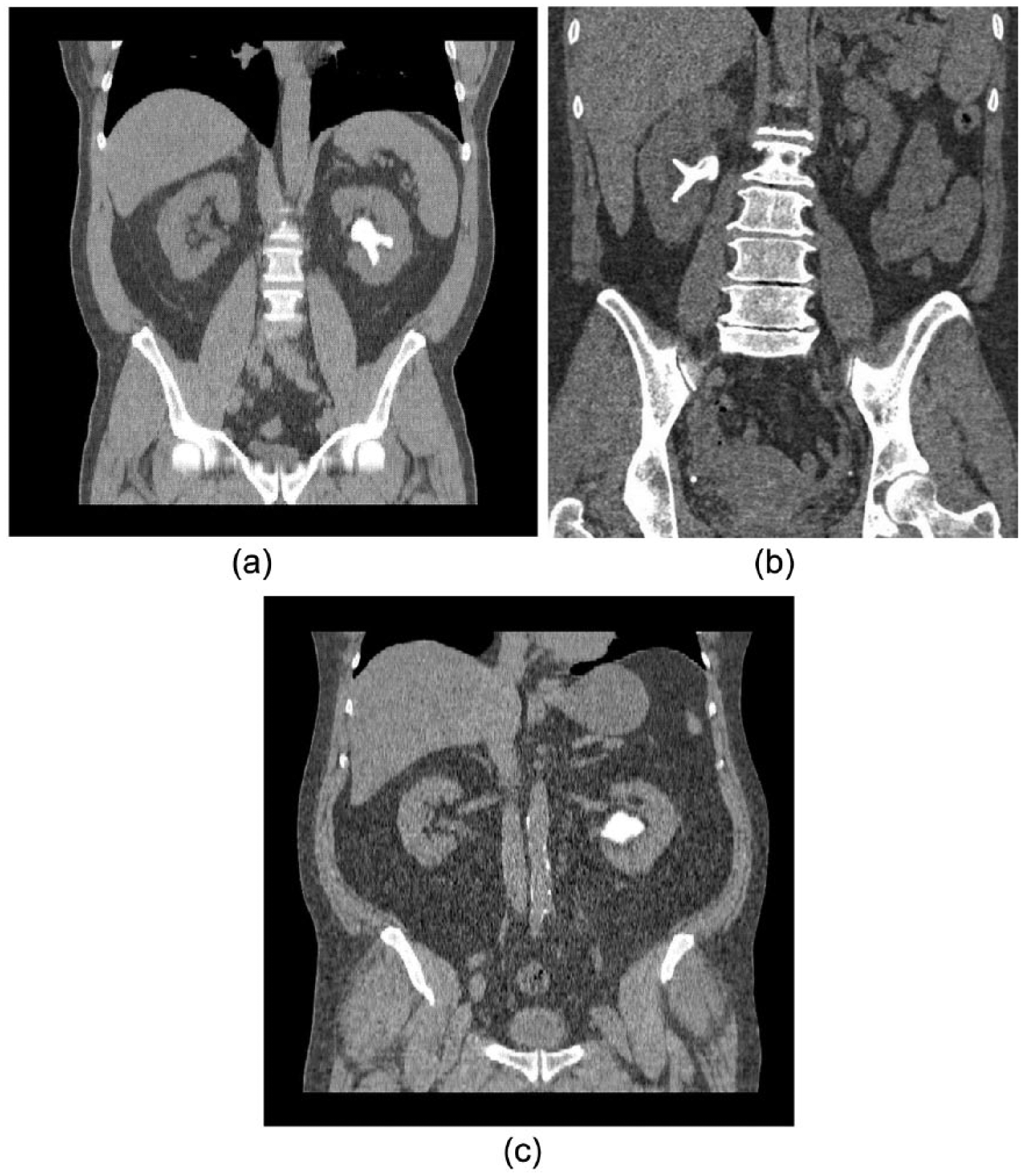
CT-derived parameters for ‘ACS’: (a) for the ‘A’: the acute angle; (b) for the ‘C’: the complicated calyx; and (c) the CT-derived parameter for the ‘S’: the stone size.
All operations were performed by two competent surgeons, according to Jean De la Rosette et al.,
9
with more than 60 cases done by each. Our surgical technique is described elsewhere.
10
We defined stone-free status as either when there was no residual fragment or the residual fragment was
Statistical analysis
Statistical analyses, the Receiver Operation characteristic (ROC) analysis in particular, were performed using software called PAST, 12 MedCalc (http://www.medcalc.org/) and XLStat (http://www.xlstat.com/en/). We realised the calculation of exact Bayesian confidence (credible) intervals for proportions (sensitivity (Se), specificity (Sp), positive predictive value (PPV) and negative predictive value (NPV)) and the MOVER confidence intervals for the ratios of some of them (positive likelihood ratio (LR[+]) and negative likelihood ratio (LR[–])). 13 Statistical significance of the observed effects was tested by P values and confidence intervals (CIs). For expression of the clinical importance of findings, the so-called ‘effect size’ was used.13,14 As measures of the effect size, the area under the ROC-curve (AUC) was used. Values around 0.001 were considered as a critical significance level.
Results
According to the low-dose CT scan performed within 24 hours after the operation, the patients were stratified as follows: 72 patients were rendered as stone free and 44 as stone-free failures. Their demographic and clinical data as well, are presented in Table 1.
Demographic and clinical data.
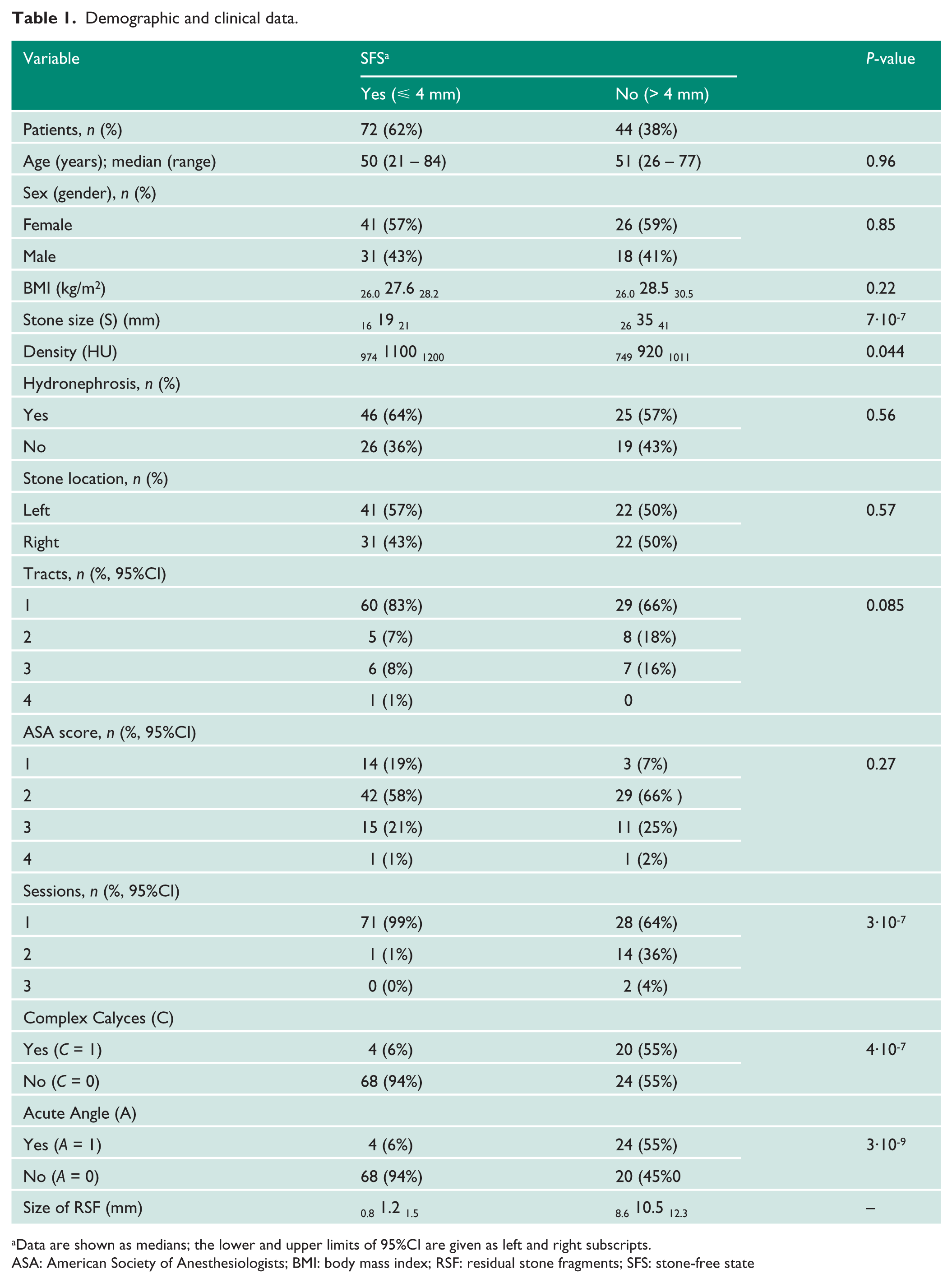
Data are shown as medians; the lower and upper limits of 95%CI are given as left and right subscripts.
ASA: American Society of Anesthesiologists; BMI: body mass index; RSF: residual stone fragments; SFS: stone-free state
Both subgroups appeared to be equal in relation to age, BMI and gender proportions. A score of R = 0 was assigned to the patients with residual fragments ⩽ 4 mm, which were rendered as stone-free; and a score of R = 1 was assigned to the patients with residuals ⩾ 4 mm, whom were rendered as stone-free failures. The AUC = 0.77 (with 95% confidence limits = 0.69–0.86) was achieved, yet for one the most informative characteristics, the stone size (S), with the corresponding cut-off point (COP) = 24 mm (Figure 2(a)).
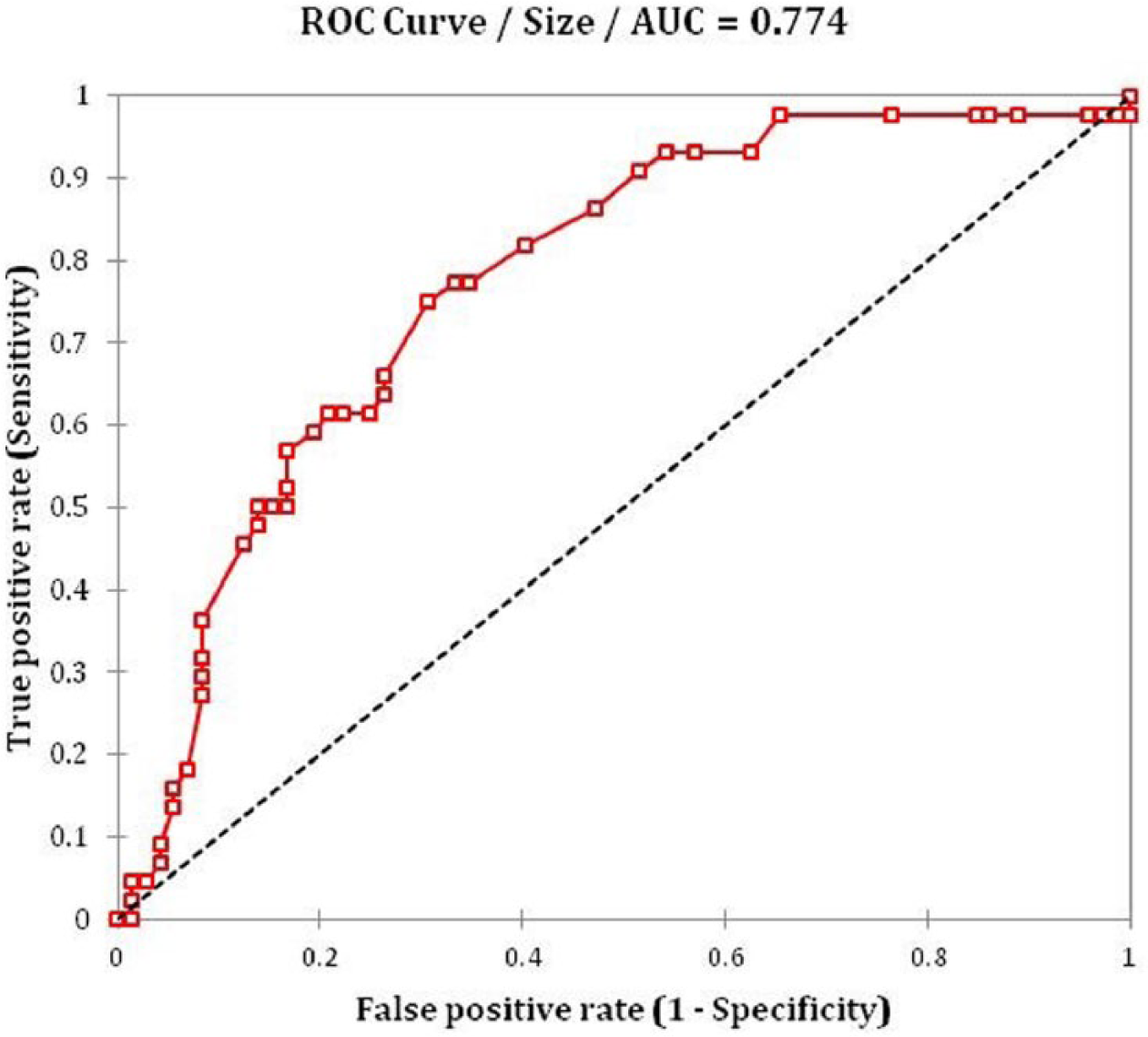
ROC-curve for the Stone Size AUC = 0.69 0.77 0.86 and COP = 24 mm.
Such an AUC value was compatible with AUCs obtained using the nephrolithometric nomogram (AUC = 0.76). 8 For other preoperative variables, AUCs were much less informative (close to uninformative value AUC = 0.5) and are not shown here. So using the cut-off point, we could reduce the ‘Stone size’ or ‘S’ to the following score: S = 0 for stone size ⩽ 24 mm and S = 1 for stone size > 24 mm.
Discrimination and prediction capabilities were improved, when two of the most informative discrete characteristics’ variables were added into account: ‘Acute Angle (A)’ and ‘Complex Calyces (C)’; with the scores 0 and 1, for their absence and presence, respectively.
The ROC-curve obtained from a logistic regression for the combined three parameters, namely ACS, appeared to be more informative. For this curve, AUC = 0.87, with 95% confidence limits from 0.78 to 0.94 (Figure 2(b)): This corresponds with the findings of Z Okunov et al. 4 in a STONE nephrolithometry study.
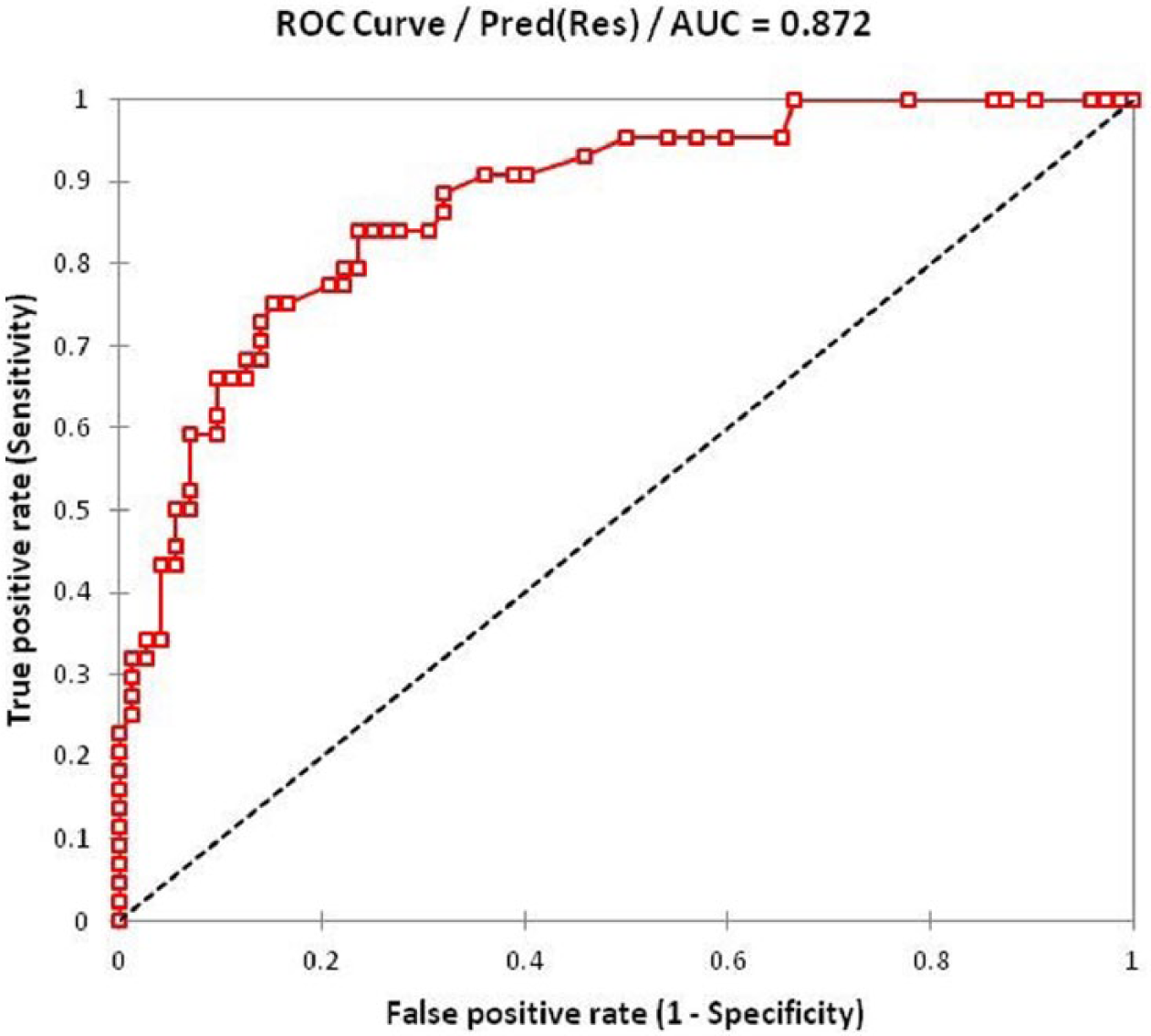
ROC-curve for the combined ACS scores: AUC = 0.78 0.87 0.94.
The distribution of ACS scores between two groups with residual fragments (R = 1) and with clinically insignificant fragments (R = 0) appeared to be, statistically, extremely heterogeneous (P = 3∙10-9); however, this observed heterogeneity was only when all three ACS parameters were present (ACS = 3) or all were absent (ACS = 0). As a result, we were able to create two 2 × 2 contingency tables, called confusion matrices, for these two extreme values of combined ACS scores (Table 2).
Confusion matrices for ACS = 3 (top) and ACS = 0 (bottom).
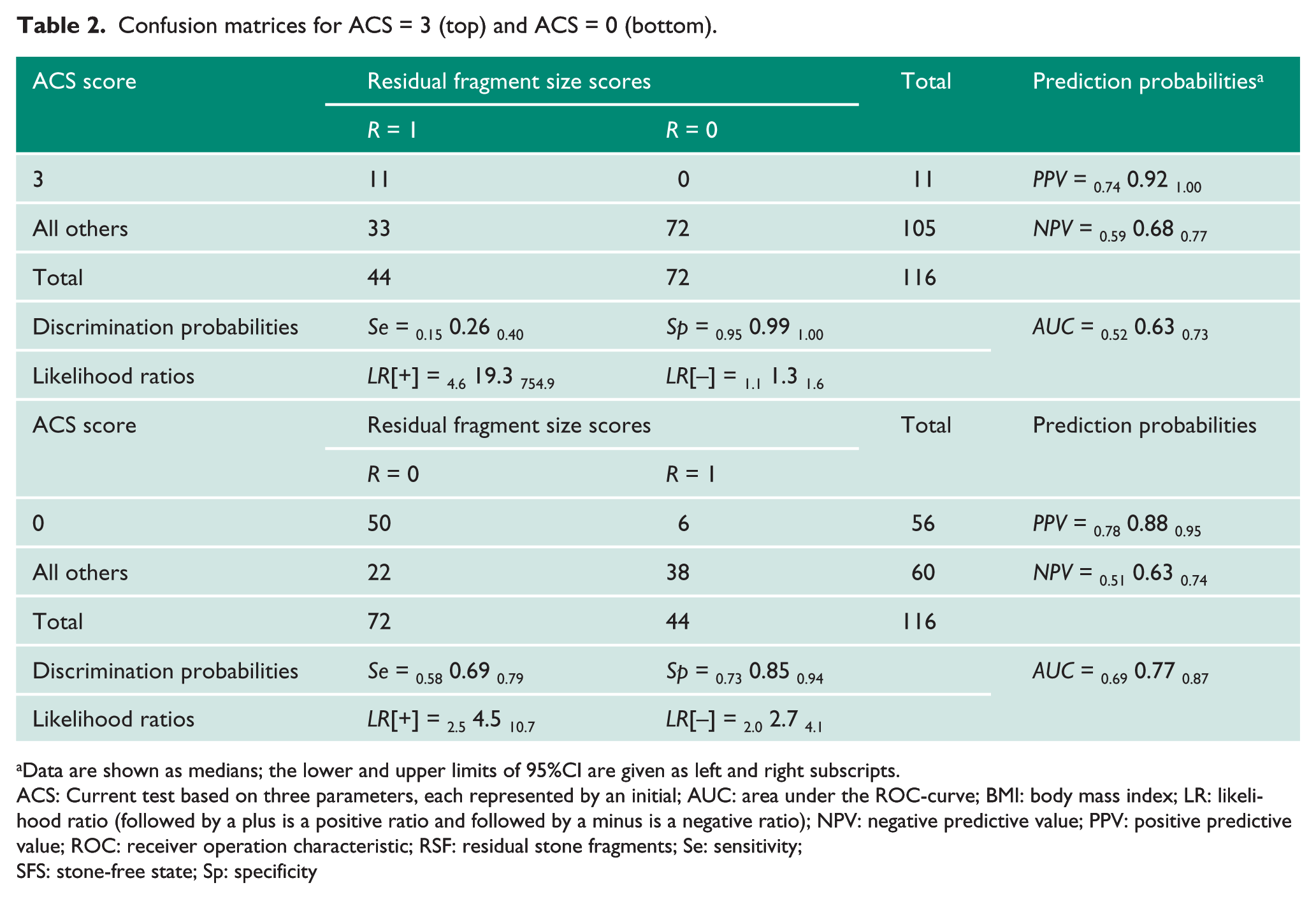
Data are shown as medians; the lower and upper limits of 95%CI are given as left and right subscripts.
ACS: Current test based on three parameters, each represented by an initial; AUC: area under the ROC-curve; BMI: body mass index; LR: likelihood ratio (followed by a plus is a positive ratio and followed by a minus is a negative ratio); NPV: negative predictive value; PPV: positive predictive value; ROC: receiver operation characteristic; RSF: residual stone fragments; Se: sensitivity;
SFS: stone-free state; Sp: specificity
Thus, if the ACS score = 3, then the probability of stone-free failure is about 92% (or probability of being stone free was just 8%); and if the ACS score is 0, then the probability of rendering the patient stone-free is about 88% (Figure 3). The intermediate values of ACS = 1 and ACS = 2 didn’t show any clinical significance.
Scoring of ACS: (a) All three parameters present: ACS score = 3; and (b) All three parameters absent: The ACS score = 0.
Discussion
Unfortunately, despite the variety of existing tools for PCNL stone-free rate prediction, many of them are not deprived of drawbacks; among others, there are three worth mentioning: The Guy’s score, STONE nephrolithometry and the CROES nomogram, which are, according to a recently-published study, shown to be equally predictive of the stone-free state in patients undergoing PCNL. 15 Guy’s score, as proposed by Thomas et al., 3 evaluating the state of being ‘stone-free’, uses plain radiography, which is substantially less sensitive than CT for detecting calcified stone fragments. The stone-free rates that are reported seem low (62% overall), particularly given the authors’ inclusive definition. This may depend in part on patient selection, the technology that was utilized for treatment (for example, the type of lithotrite), and the provider’s threshold to stage procedures in patients with complex stones, owing to concerns regarding complications. 16
STONE nephrolithometry, developed by Z Okunov, 4 being one of the most comprehensive predicting tools and having much the same AUC as the ACS score, contained points such as the skin-to-stone distance, stone density and presence of hydronephrosis, which were not associated with the presence of residual stones. The CROES nomogram, by a group of authors from CROES, 8 so far has the biggest sample size, gained from 96 centres worldwide and it has the power to detect any statistically-significant differences, having an almost similar AUC with STONE, 15 corroborated with the nomogram’s prior stone treatment; and the case volume per year, was as well making consideration of the stone-free rate be more comprehensive. Nevertheless, the data obtained from such centres is not homogenous, because the centres had different methods to assess both stone-free rates and operative times, 17 and the patients examined for treatment success by Kidney Ureter Bladder (KUB) were also included in the study. This may potentially have resulted in a misinterpretation of some variables, and also given lower predictive capacity.
With the ACS scores provided having an AUC = 0.87, considered as a large effect, we were able to predict the probability of stone-free failure when the main variables are present in 92% of patients; while with having none of those parameters, the stone-free rate could be predicted with 88% probability.
In our study, we did not find any association with stone density, in contrast to some other studies.18,19 Moreover, it was consistent with the findings of the study for CROES nomogram, and perhaps the reason was that stone density does not play any role in facilities having all equipment for efficient stone disintegration and a final pelviocalyceal fiberscope inspection at the end of the PCNL as an obligatory part of the operation.
Hydronephrosis, despite its possible influence on a stone-free rate as has been mentioned in some studies,6,20 did not affect the stone-free rate in our study. The ability of a surgeon to combine both ultrasound (US) and X-ray guidance for gaining access, and a strict adherence to the operative protocol as well, could be a reasonable explanation for this observation.
One of the most important factors was stone size, which is consistent with the other works4,21; and the ROC analysis showed that stone size is able to affect the stone-free state, when it is larger than 24 mm. Unsurprisingly, two other factors, an additional stone in a long calyx (⩾ 10 mm) with narrow infundibulum (⩽ 8 mm) and an additional stone in a calyx with an acute angle ⩽ 45° were shown to be the next most informative, on a discrete analysis, and improved AUC significantly. The explanation seemed quite obvious: The above-mentioned parameters making necessary additional tract creation to achieve complete stone removal are associated with a higher haemorrhage complication rate, and this may influence the stone-free status. 22 Our study had several limitations: First, our study is retrospective in its origin; and second, we did not account for the case volume per year, as it has previously been demonstrated that centres with a volume of cases > 120 per year have superior surgical outcomes. 11 All our PCNL cases’ treatments were performed by competent surgeons, skilled in US- and X-ray-based navigation. Third, we do recognize that despite acceptance by CROES of the size of clinically-insignificant residuals being ⩽ 4 mm, the definition of being stone-free should become much stricter, according to existing reports. 23 Lastly, we did not take into account previous surgical treatment, which can obviously affect the stone-free rate.
Footnotes
Acknowledgements
We are very thankful to Vladimir Khvorov, Mohammed Lezrek, and in particular, Nikita Khromov-Borisov for assistance in statistical analysis, paper revision and the advice given.
Conflicting interests
The Author(s) declare(s) that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Institutional ethics committee has approved this study (Approval no: 2342A).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Guarantor
SP.
Contributorship
NG and SB made all the operations. VG, DS, VO and AP researched the literature. VD, NT, PB and VK were involved in protocol development, the gaining of ethical approval and data analysis. NG and SP wrote the first draft of the manuscript. All authors reviewed and edited the manuscript, and approved the final version of the manuscript.