
Abstract
Background:
Recurrent urinary tract infections (UTIs) in women are common despite anatomically normal urinary tracts and are frequently referred to secondary care for further assessment.
Patients and methods:
Clinic letters and pathology reports of 244 women referred to our centre over a 2-year period with uncomplicated recurrent UTIs were reviewed to determine the investigations they underwent in both primary and secondary care.
Results:
A significant proportion of women do not meet the criteria for recurrent UTIs as their infections are not proven on culture. The majority of women undergo both renal tract ultrasound scan (USS) and flexible cystoscopy. Though USS was found to demonstrate relevant pathology, flexible cystoscopy, however, did not reveal any relevant pathology.
Conclusion:
Investigation of women with recurrent uncomplicated UTIs should be done with adequate cultures and renal tract USS.
Keywords
Introduction
Recurrent urinary tract infections (UTIs) in women are common; in general practice, approximately 15% of all community-prescribed antibiotics in the USA are for UTIs. 1 An uncomplicated UTI is one that occurs in a healthy host in the absence of structural or functional abnormalities of the urinary tract. 2 Recurrent UTI is defined as more than three culture-proven UTIs in 12 months. 2 The majority of recurrent UTIs occur among healthy women who have anatomically and physiologically normal urinary tracts. 1 Recurrent infections are thought to be due to re-infection in the majority of cases, rather than a persistent infection. 3
Recommendations from the EAU guidelines are that recurrent UTIs need to be diagnosed by urine culture and post-void residual (PVR) urine should be excluded. 1 However, imaging and cystoscopy are not routinely recommended for evaluation of women with recurrent UTIs, but should be performed in atypical cases. 1
The objective of this study was to determine the investigations women underwent both in primary care and secondary care for uncomplicated UTI.
Methods
All female patients with recurrent UTIs who were seen at the Royal United Hospital, Bath, between January 2010 and December 2012 were identified, using a local shared network folder of patient letters. Women were excluded from further analysis if there were any complicating or 2-week wait referral signs/symptoms identified on review of their clinic letter; that is, visible or non-visible haematuria, loin pain, catheter in situ, previous urological/gynaecological/neurological history, UTI in childhood, palpable bladder or pelvic organ prolapse. Clinic letters, radiology reports and pathology reporting systems were then reviewed for each patient to identify the number of cultures sent and results of those cultures, investigations undertaken by the secondary care team, and the results of those investigations as documented in the clinic letters.
Results
A total of 244 women referred with uncomplicated recurrent UTIs were identified and included in the analysis, with a mean age 54 years (age range 16–95 years). The number of cultures sent to the laboratory in the 12 months prior to urology outpatient appointment ranged from 0 to 16 (mean 4, mode 3). Of these cultures, individual patients had between 0 to 9 culture-proven UTIs (mean 1.7, mode 0) (Figure 1).
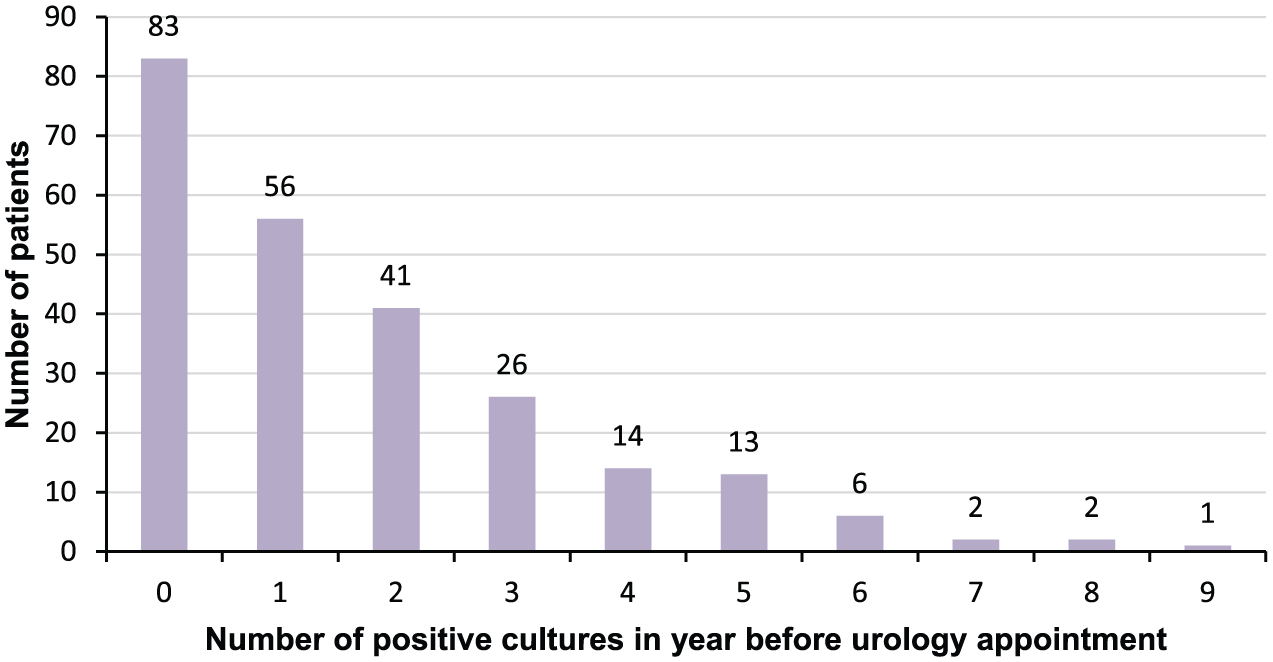
Number of patients with culture-proven UTI(s) in the 12 months prior to first urology outpatient appointment.
Of those patients who had no positive cultures, 27 did not have a single culture sent to the laboratory, 20 only had a single culture sent, 11 had two or more cultures sent which showed no growth and no leucocytes, and the final 25 women had two or more cultures sent, at least two of which had leucocytes but no growth.
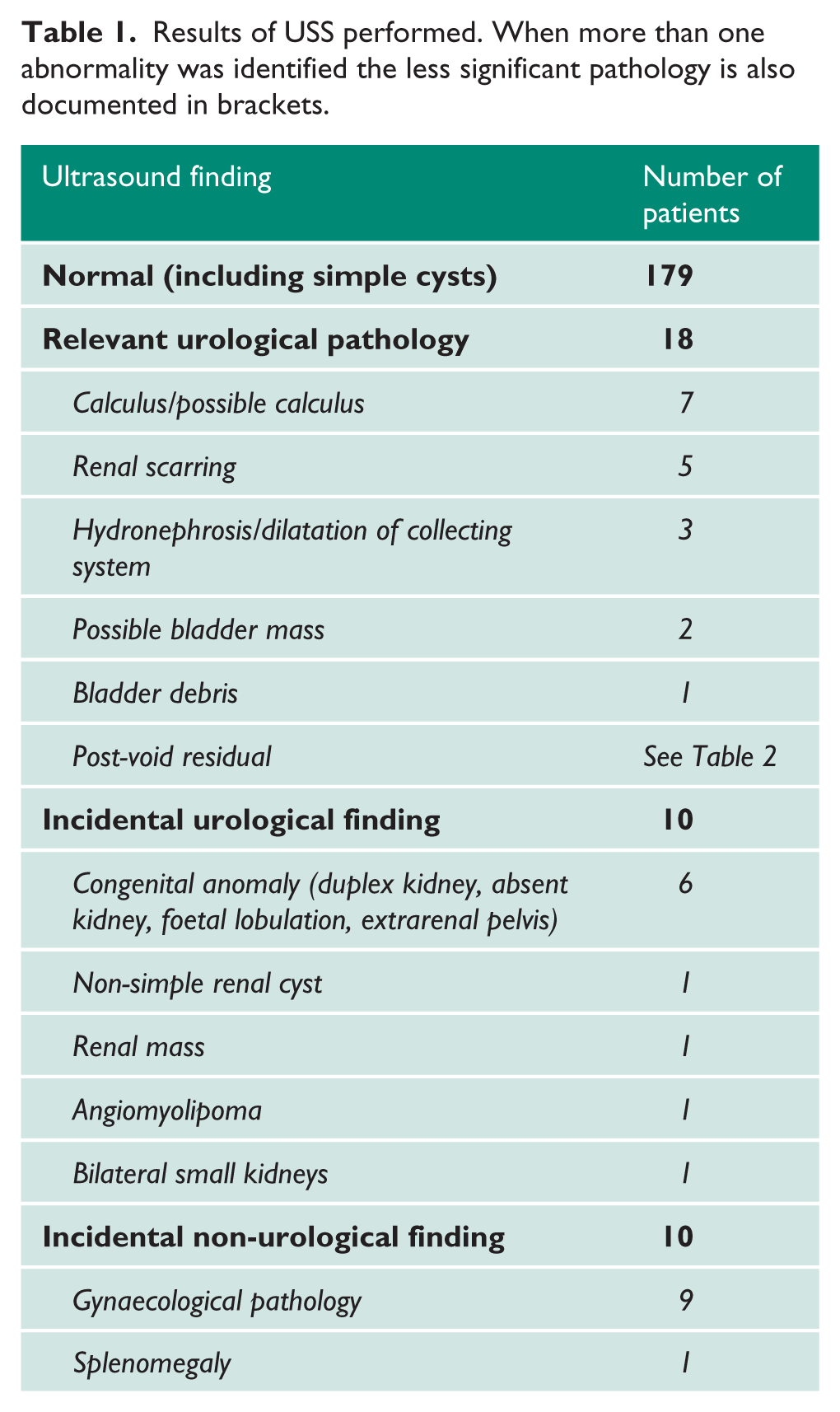
In all, 223 women had an ultrasound scan (USS) performed of the renal tract, one had computed tomography (CT) performed for other reasons and upper tracts were evaluated on this, and 20 had no USS or alternative upper tract imaging performed (including two women who had USS booked but did not attend the appointment). Ultrasound findings are demonstrated in Tables 1 and 2.
Results of USS performed. When more than one abnormality was identified the less significant pathology is also documented in brackets.
Results of post-void residuals performed either at time of urinary tract USS or following flow rate.
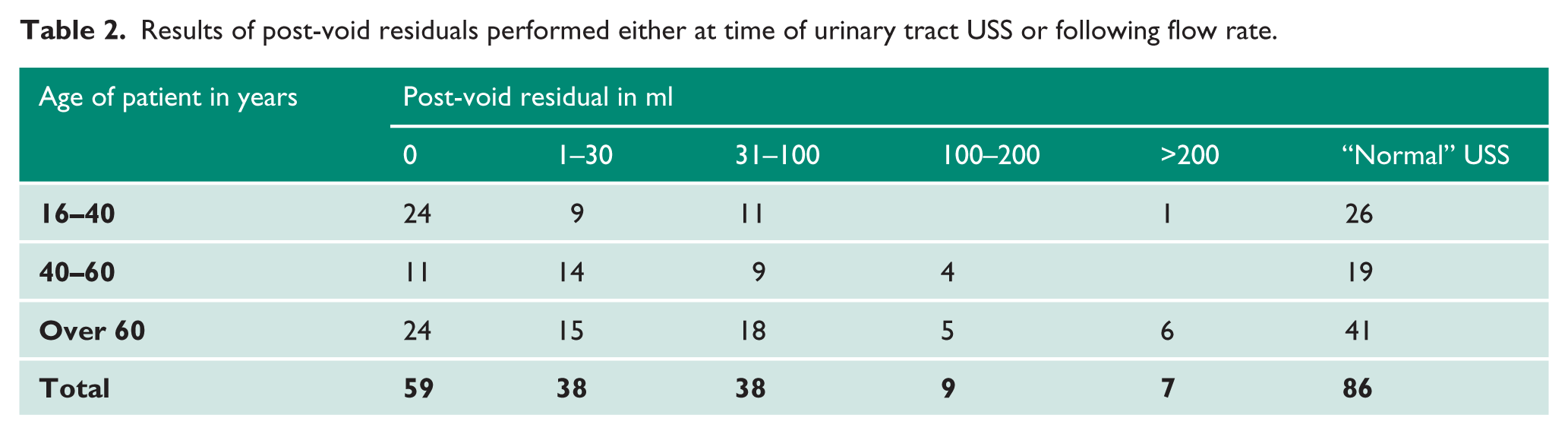
A PVR volume was specifically recorded in 151 women, either from USS of the urinary tract by a radiologist/ultrasonographer or in the urology clinic with bladder scanning following flow rates. The range of recorded volumes was from 0 to 841 ml. Of the seven women with a PVR of over 200 ml, three had a PVR between 200 and 300 ml, three had a PVR between 400 and 500 ml, and a single patient had a PVR in excess of this at 841 ml. One of the women with a residual between 400 and 500 ml also had a pelvic mass secondary to gynaecological pathology identified on USS. The PVR volumes are shown in Table 2. There were 93 women for whom no specific PVR was recorded. However, 86 of these women had a USS of the bladder reported as “normal”. Only seven women had no USS and no PVR recorded following flow tests.
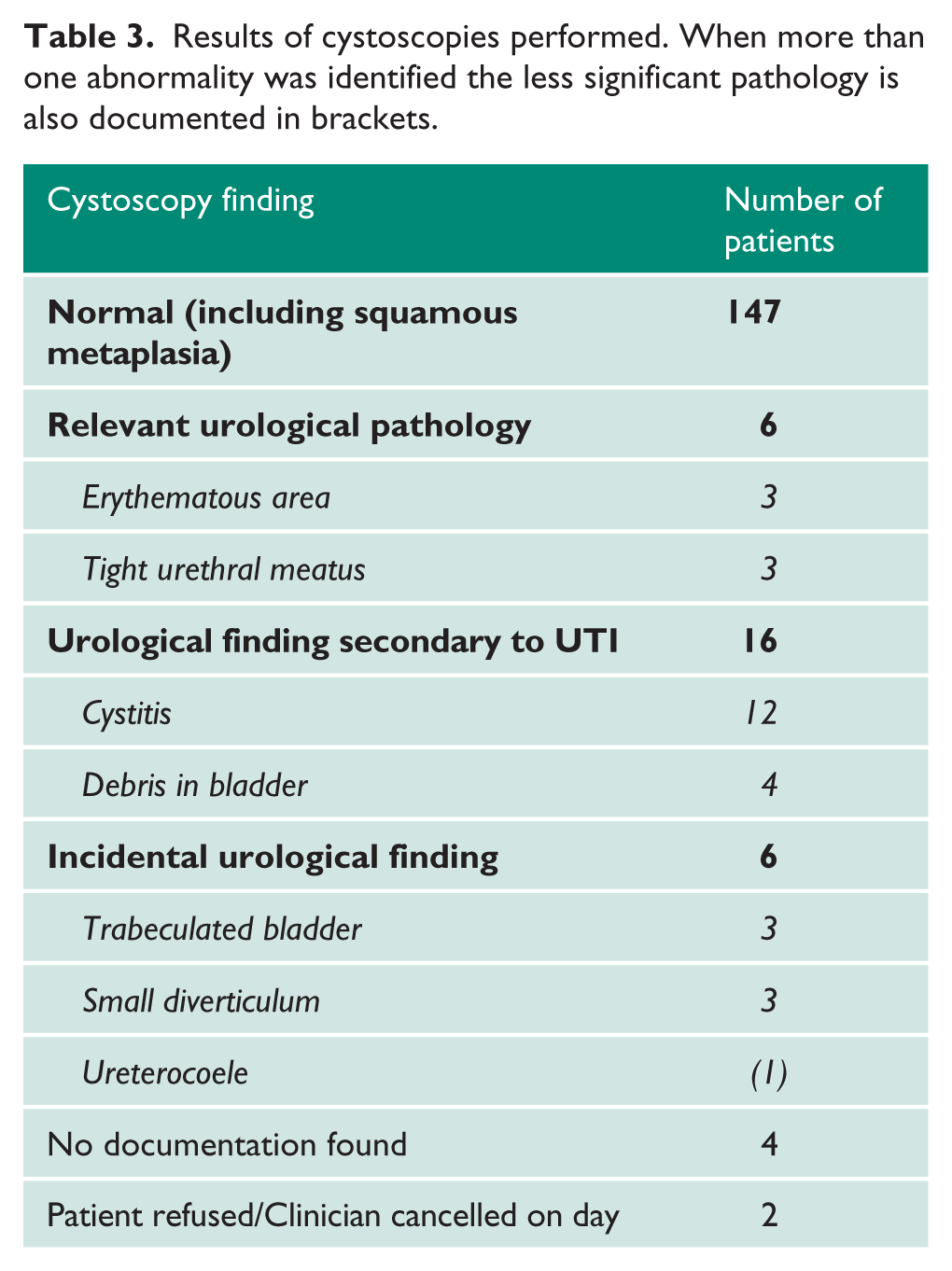
A total of 161 flexible cystoscopies and 19 rigid cystoscopies were performed to investigate the cause of recurrent UTIs (five patients underwent both flexible and rigid cystoscopy). No cystoscopy was carried out in 60 women, a further two had a cystoscopy booked but the appointment was not attended, and an additional two had a cystoscopy offered but the patient declined. Findings of cystoscopy are demonstrated in Table 3. All abnormal areas seen at flexible cystoscopy were booked for a rigid cystoscopy and biopsy, and in all cases the lesion had either resolved or showed inflammation on histology.
Results of cystoscopies performed. When more than one abnormality was identified the less significant pathology is also documented in brackets.
Some 20 women underwent a CT scan (six of these were reviewed as part of their recurrent UTI investigations but were done for other indications); of these 20 CT scans, 13 were normal, eight were performed due to abnormalities seen on USS (two for a staghorn calculus, two for possible renal calculi, two for hydronephrosis, one for a renal mass, one for a gynaecological pelvic mass) and only one scan showed a finding not seen on USS, which was that of an incidental pancreatic cyst.
Further investigations were done based on findings of the above investigations, including plain film KUB (three women), MAG3 renogram (two women), DMSA (one woman), ureteroscopy which showed megaureter (one woman) and retrograde pyelography (one woman).
Discussion
Recurrent UTIs are a common presentation to both primary and secondary care. 1 The majority of women who have recurrent UTIs have no predisposing anatomical or functional abnormality of their urinary tract, thereby leading to the low diagnostic yield demonstrated in previous studies.2,3 However, women with recurrent UTIs have been shown to have higher PVR volumes of urine compared with women without UTIs, with up to a quarter of postmenopausal women with recurrent UTIs having significant PVRs.4,5 As such, guidelines, including the EAU guidelines, are that recurrent UTIs need to be diagnosed by a urine culture, and residual urine should be excluded, but imaging and cystoscopy are not routinely recommended. 1
Our results show a significant number of women (35%) are being referred to secondary care without having a single UTI proven on culture, as would be recommended to confirm that a UTI is the cause for the patient’s symptoms and to confirm no adjustment is required to empirical therapy.2,6 This 35% is made up from women who have never had urine sent for culture (34%) and those who have had a number of cultures sent with no growth found on the cultures (66%). Clearly if the former group had cultures sent this may show a UTI, which may include a resistant organism accounting for the recurrent/persistent nature of their symptoms. However, the latter group are being treated and investigated as recurrent UTIs despite evidence to the contrary, when in fact alternative diagnoses may need investigating and treating.
Our findings are consistent with previous studies showing that cystoscopy has a very low diagnostic yield in women presenting with uncomplicated recurrent UTIs, but confirm that despite guidelines advising that neither cystoscopy nor upper tract imaging are required for the investigation of uncomplicated recurrent UTIs, these are still performed in the majority of cases.1,2,7 The few studies which support the use of cystoscopy differ from this one in that they have not excluded patients with risk factors for complicated UTIs, including persistent haematuria or a history of malignancy. These patients account for a large proportion of the subgroup with abnormal cystoscopies.7,8 In our cohort cystoscopy revealed some women had erythematous areas on the bladder mucosa, but further investigation with biopsy showed that all these lesions either resolved or identified inflammation which required no further action.
Ultrasound scan, however, identified a number of pathologies, some of which may contribute to recurrent UTIs and others which were an incidental finding. USS identified all the significant pathology within this series which required further intervention, that is, renal mass, urinary tract calculi and significant PVR. This is in accordance with other studies which have found that false negative results with imaging (namely USS) are infrequent.9,10 In our study the majority of CT scans were appropriately requested to investigate abnormalities seen on USS including renal stone disease, hydronephrosis and a renal mass. There was, however, no clear clinical indication for six CT scans in this cohort. This level of inappropriate radiation exposure cannot be justified in this patient group, and should only be performed with a clear clinical indication.
What constitutes a significant ultrasound PVR in the context of recurrent UTI in women is unclear. In this cohort, accepting the limitation of interpreting a “normal” USS report as meaning a PVR <100 ml, we observed that approximately 7% of women had a PVR greater than 100 ml. A joint report by the International Urogynecological Association and International Continence Society on the terminology for female pelvic floor dysfunction does not set a value for normal PVR and suggests this will depend on the method of measurement. 11 A large study of 1140 women with symptoms of pelvic floor dysfunction found 81% of immediate PVR measured by transvaginal USS were 30 ml or less. They found that residual volumes higher than this were associated with significantly increased risk of recurrent UTIs. They suggest that 30 ml appears to be the appropriate upper limit of a normal PVR, above which recurrent UTIs are seen to increase. 12 A study by Stern et al. has also shown higher PVR in postmenopausal women with recurrent UTIs compared with controls, showing a mean PVR of 33 ml in controls and 70 ml in those with recurrent UTIs. 5 Raz et al. also demonstrated this finding of raised PVR in postmenopausal women with recurrent UTIs where only one control patient had a measured residual volume compared with 28% of the women with recurrent UTIs. 4 Although these studies suggest that women with recurrent UTIs have higher PVRs, the volume at which intervention would reduce the incidence of recurrent UTIs remains to be determined. Clearly the potential benefit, risks and relative impact on quality of life of the introduction of intermittent self-catheterization to manage a PVR needs to be discussed on an individual basis.
Conclusions
As recurrent UTIs are a common presentation in both primary and secondary care, it is important to accurately diagnose and investigate these in the appropriate setting. For women with uncomplicated recurrent UTIs it is important these are accurately diagnosed on culture in the first instance. Our data would support routine USS with assessment of PVR of the urinary tract in women with culture-proven uncomplicated recurrent UTIs; however, routine flexible cystoscopy did not provide any additional clinical information.
Footnotes
Acknowledgements
None.
Conflicting Interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed Consent
Not applicable. Approval was obtained from the audit and research department. As this was a retrospective case note review, ethical approval was not required. All data were anonymised and kept confidential.
Trial Registration
Not applicable.
Guarantor
SRP.
Contributorship
SRP and SDE conceived the study. SRP and NCC researched the literature. SRP, NCC and BM gathered and analysed data. SRP wrote the first draft. All authors reviewed and edited the manuscript.