
Abstract
Objective:
To investigate the accuracy of electronic discharge summaries (EDSs) written for patients who had undergone acute scrotal exploration for suspected testicular torsion.
Methods:
We reviewed the operation notes and EDSs for 169 admissions over a 52-month period where patients had undergone acute scrotal exploration for suspected acute testicular torsion and reviewed the correlation between what was written in these documents, focusing on laterality of pain, operative findings and procedure performed.
Results:
We found that the side of testicular pain was not mentioned in 14.8% of EDSs, the operative findings recorded on the EDS did not correlate to those on the operation notes in 17.2% of cases and the overall procedure performed did not correlate in 35.5% (with most of these relating to the laterality of the operation). The fact that an operative procedure happened at all was not mentioned in 4.7% (n = 8) of the EDSs.
Conclusions:
The information in such an important medical document needs to be accurate, and we advocate that the person performing the operation should initiate the discharge summary process, where EDS use is the norm for discharge. Junior doctors entering urology departments must also be trained on the key information to be included in urological EDSs.
Keywords
Introduction
Acute scrotal pain forms an important part of the emergency urology workload, especially considering the clinical and medico-legal implications of potential testicular torsion and the worst outcome, in the form of testicular loss. The dilemma posed to clinicians who explore the acutely painful scrotum is increased, when assessing patients whom have undergone previous surgery for the same presentation. There is also a variation between operating surgeons in performing orchidopexy in the presence of a normal testis at exploration, with no clear guidance on the issue. The only written information available on previous surgery often comes from electronic discharge summaries (EDSs) prepared by junior doctors, which is a clinical document that used to be dictated by the consultant responsible for the patient’s care. Surprisingly, very little exists in the medical literature about auditing the accuracy of surgical EDSs,1,2 despite the existence of guidelines issued by the Royal College of Surgeons of England on medical record-keeping, which includes guidance for details on discharge. 3
In our institution, EDSs have been in place since 2010. The objectives of this study were to review all those EDSs written for patients who had undergone acute scrotal exploration for suspected testicular torsion and to compare the information recorded in these EDSs against what was written in the operation notes.
Materials and methods
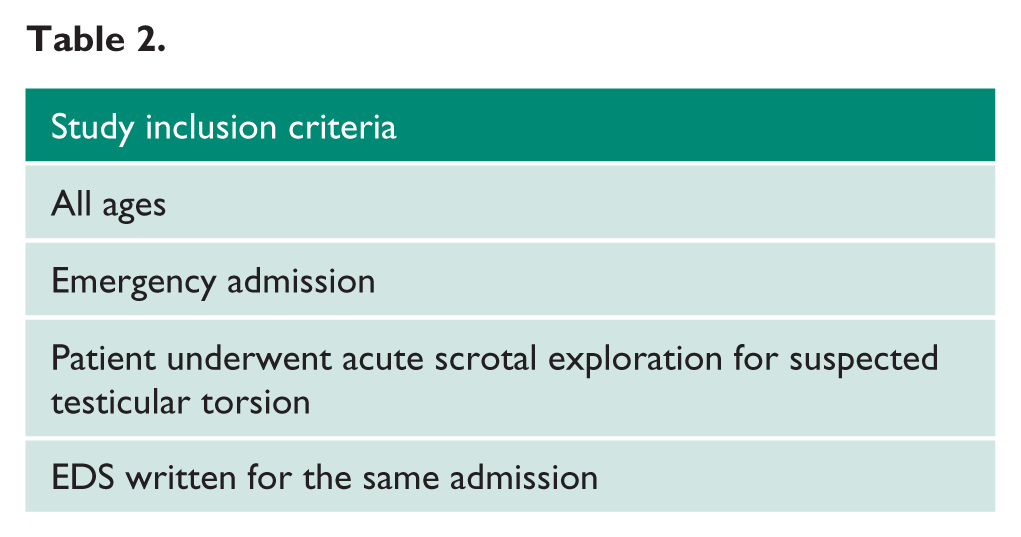
We performed a retrospective review for the period between 1 August 2010 (when the EDSs were first introduced in our institution) and 31 December 2014, registering the project with our institution’s Clinical Effectiveness Department. The Information Department provided a database of all patients whom had undergone scrotal procedures (Table 1), via coding based on the Healthcare Resource Groups Definitions Manual, 4 between the above dates; and the patients’ electronic notes were reviewed, to ascertain if they had fulfilled the inclusion criteria (Table 2). The paper and electronic operation notes for all included patients were reviewed to obtain data on the patients’ hospital identification number, date of surgery, age at the time of surgery, laterality of testicular pain, operative findings and procedures performed at the time of surgery. The EDSs were subsequently analysed to determine the accuracy of the admission history written, as compared to that in the operation notes, focusing on: the laterality of testicular pain, operative findings and procedures performed. The reasons for any discrepancies were noted. All data was entered into and analysed on a Microsoft Excel spread sheet.
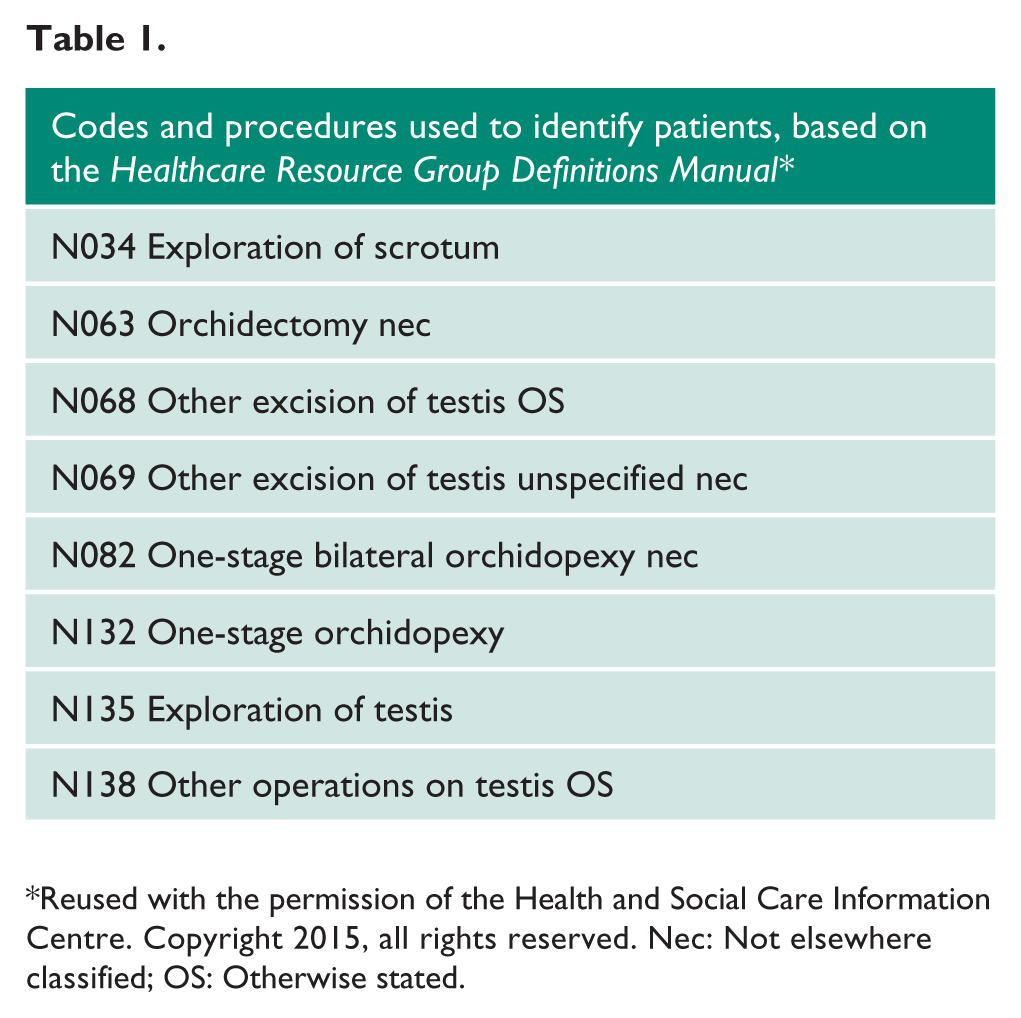
Reused with the permission of the Health and Social Care Information Centre. Copyright 2015, all rights reserved. Nec: Not elsewhere classified; OS: Otherwise stated.
EDS: Electronic discharge summary.
Results
The details of 3164 patients were provided by the Information Department, with the patients’ hospital identification numbers and dates of admission: We had 168 patients fulfil the inclusion criteria, amongst whom there were 169 admissions. The age range was from 3 to 58 years. All admissions occurred over a 52-month period.
The side of presenting testicular pain was not mentioned in 25 (14.8%) EDSs. The operative findings recorded in the EDS did not correlate to those on the operation note in 29 (17.2%) cases. Of these, the findings were not mentioned at all in 21 (12.4%) cases, including the 11 cases where a torted testis was discovered. In 60 (35.5%) EDSs, the procedure recorded did not correctly correlate with that on the operation notes, mostly regarding the laterality of surgery not being mentioned in 44 (26.0%) cases. Orchidopexy was performed in a total of 93 cases; and of these, it was not recorded in the EDS only four times. The fact that an operative procedure happened at all was not mentioned in the EDS in a total of eight (4.7%) cases.
Discussion
The intention of creating a discharge summary is to summarise all the key aspects of a patient’s care during a hospital admission, and it is the main form of communication for both primary and secondary care clinicians about inpatient episodes. In surgery, it must include accurate operative details, as the operation notes are often inaccessible to many doctors and available only in the patients’ paper records. Most discharge summaries are scribed by junior doctors, as is the common practice in our department, where they are scribed by Foundation Year One (FY1) and Foundation Year Two (FY2) doctors. Although we expected some errors to be present, given the typical workload of these doctors, we did not anticipate how common some of these inaccuracies would be. Given the medico-legal aspects associated with acute testicular pain, this is clearly an issue that needs to be addressed. Errors in recording operative data on discharge summaries were demonstrated almost as long as 20 years ago 1 ; and this has unfortunately persisted, as evidenced by our findings. Patients do re-present with acute recurrent testicular pain after scrotal exploration; and although there are isolated reports of recurrent torsion despite orchidopexy,5–8 this procedure has been demonstrated to significantly resolve symptoms and prevent future episodes.9,10 Therefore, knowing exactly what has happened before is essential first to make a decision about any further operative interventions (that thus expose the patient to the potential complications of that operation), and then to plan in advance the steps that will be taken at the time of re-exploration.
Our software for writing EDSs has a couple of discrepancies, which did not allow further analysis. Firstly, our EDS software does not record the grade of the doctor who has written the document, only their name; such information would have been useful to gauge if our findings were applicable to all grades, including specialty trainees whom had written some of the above EDSs, but were recognisable only by their recorded name alone when reviewing the documents. The second discrepancy is that the admission diagnosis is not a mandatory field; and therefore, was not included in all of the EDSs. Assessing how often testicular torsion had been recorded as the diagnosis in the presence of a normal testis would have been of value, to assess the doctors’ underlying understanding of acute testicular pain and the diagnostic nature of acute scrotal exploration.
These findings also raise the issue of how much urology is taught in the UK undergraduate medical curriculum, given that the task of writing EDSs is often handed to FY1 doctors, who have just graduated from university. The last survey of undergraduate urology teaching was carried out in 2002, where it was found that urology formed part of the core curriculum in only 37% of the responding medical schools. 11 A follow-up survey of recruitment into the specialty found that less than one-third of urologists were influenced by having undergraduate exposure. 12 Although no such repeat survey may have been performed in the last decade, our work may indicate that there are on-going deficiencies of Foundation doctors, in what urologists perceive to be core knowledge of the specialty. This could in part be due to reduced undergraduate exposure, even if we examined the ability to summarise the care of only one particular urological presentation. Indeed, a study examining EDSs written for all urological admissions may be of benefit, to ascertain whether similar findings occur for all urological presentations and admissions.
Our recommendations in light of these results are that whoever performs a scrotal exploration for suspected testicular torsion should initiate the EDS, given that the operating surgeon is likely to have a greater degree of clinical urological experience, and is therefore more likely to input the important relevant information in the discharge document. The second recommendation is that given the relatively little exposure that medical undergraduates have to urology, individual departments need to take the responsibility for ensuring that junior doctors rotating through and looking after urological patients, for example during on-call shifts, are provided with a proper induction on the key aspects of working within the specialty, including essential documentation, as we have highlighted. Although interventions and training programmes for junior doctors in completing discharge summaries have been evaluated and have demonstrated improvement, regular scrutiny and audit of EDSs must still take place within urology departments, to ensure the on-going quality and provision of feedback to doctors writing these important documents.
Conclusions
EDSs written for acute scrotal explorations performed for suspected testicular torsion have a worrying degree of inaccuracy regarding the exact operative procedure. We advocate that the operating surgeon compose this important medico-legal document, but that urology departments provide formal induction to junior doctors entering urology rotations or jobs where they will be looking after urological patients, including an awareness of essential operative information to be included in the patient discharge summaries.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
None declared.
Ethical approval
Not applicable.
Guarantors
PBS, RD.
Contributorship
PBS conceived the study and was responsible for study design, data collection, analysis and discussion. RD was the consultant with overall responsibility for the study and contributed to the discussion.
Informed consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.