
Abstract

BAUS members, SLAUS members and JCU subscribers can earn 3 CPD credits awarded by BAUS by reading this approved CME article and successfully completing the online CME test available at: baus.jcu.membercme.org/key/B44UL8nr8PgCkLFmRRh7SvVR/
Radiation therapy (RT) plays a vital role in multidisciplinary management of urological cancers. RT has a broad spectrum of applications, ranging from treatment with curative intent to the palliation of symptoms from incurable urological cancers. Advances in imaging, radiotherapy planning software and in treatment delivery technology (e.g. linear accelerators, tomotherapy machines, Cyberknife etc.) have led to improvements in radiotherapy over the past decades. Three-dimensional conformal RT allows shaping of the radiation beam to conform better to the tumour contour compared with older techniques. Further advances were made with the advent of intensity-modulated radiotherapy (IMRT) which allows modulation of the radiation fluence across the beam and this, in turn, allows the radiation dose distribution to be ‘shaped’ more closely to the region to be treated. This permits relative sparing of normal tissues and potentially dose escalation to tumour. Precise dose distributions with IMRT plus image guidance for accurate geographical targeting are now an essential part of modern radiation delivery. Moreover, internal RT (brachytherapy) is now established as a cancer therapy option in urology. The ultimate goal of all new innovation is to improve tumour cure rates while reducing toxicity associated with RT. This review aims to provide understanding of radiation principles and evidence for recent clinical practice for urological cancers.
RT principles
For cancer management, ionizing radiation is used. While passing through tissue, ionizing radiation can result in direct damage to DNA, or can result in free radical formation that in turn ‘indirectly’ damages DNA. Such DNA damage may be manifest as single stand breaks (usually repairable due to the complementarity of the strands of the double helix) or as double strand breaks. The latter are more complex to repair and frequently cells undertake ‘error-prone’ repair which results in substantial chromosome aberrations. Such aberrations may not directly affect the metabolic function of the cell, but result in death of both daughter cells on mitosis due to unequal distribution of DNA – what is known as ‘mitotic cell death’.
A number of different particles are available for use in radiotherapy; photon radiation, a high-energy photon beam, is the most common form of radiation used in oncology. Proton therapy is used extensively in the USA in the management of localised prostate cancer. Protons deposit most of their energy at a well-defined depth in tissue (that depth being dependent on the proton energy) allowing relative sparing of structures before and beyond that depth. Electron therapy is less penetrating and is used in the management of more superficial tumour deposits (e.g. palliative treatment of painful rib metastases or skin lesions). Alpha particles (helium nuclei) have also recently gained acceptance in uro-oncology with the advent of alpharadin.
Dose fractionation has long been a central treatment paradigm in radiation oncology. Delivery of the total radiation dose in a number of fractions permits recovery of normal tissues between sessions of RT, while still allowing cumulative damage to the tumour cells.
Two types of RT are commonly used in uro-oncology (a) external beam RT (EBRT) and (b) brachytherapy.
EBRT
EBRT is the most widely used type of RT. In recent years EBRT has improved due to advancement in tumour localisation and modification of radiation beams during therapy. With modern machines, software and imaging, it is now possible to map organs and tumours in four dimensions. 1 IMRT uses multiple treatment beams and multileaf collimation (to shape each beam) and allows the fluence of photons across the field to be non-uniform. This allows for dose escalation to the tumour and/or sparing of normal tissues to minimise collateral damage. Stereotactic body RT (SBRT) is a relatively new approach which aims to treat small tumours in a relatively small number of fractions but with a high dose per fraction (typically >7.5 Gy).
For EBRT, the total dose is often divided into smaller fractions; conventional fractionation describes the situation where the total dose is divided into multiple fractions of 1.8–2.0 Gy per fraction, delivering five fractions per week.
Total radiation dose is not a reliable measure of biological effect when dose-per-fraction or dose-rate is altered. 2 In radiobiology, the linear- quadratic model uses two coefficients (α and β) to describe the dose response relationship. 2 This relationship is calculated by the formula;

where D is the total dose and d is the dose per fraction. The major deficiency with such formula is the lack of precision in determining α/β for the various tissue types, tumour types, and individual variations. However, in clinical practice, these coefficients can be used to calculate the effect of different fractions. In rapidly growing tissues (including many tumours), the α/β ratio is typically around 10 Gy and in tissue with a low cell renewal, the α/β ratio is 3 Gy or lower. Hence, slowly proliferating cells with low α/β ratios are very sensitive to an increased dose per fraction. 2 In recent years, an increasing body of evidence has been developed that suggests the α/β ratio for prostate cancer is around 1.5–2, giving a biological rationale for the move towards hypofractionated treatments in prostate cancer.
Brachytherapy
Sometimes referred to as ‘internal RT’, brachytherapy is a technique that allows the sources of radiation to be placed into or near the tumour. The radiation dose falls off rapidly with increasing distance from the source (according to the inverse square law), potentially reducing the risk of damaging nearby normal tissues. The placement can be permanent or temporary.
Permanent (low dose rate (LDR)) brachytherapy
Commonly used for management of localised prostate cancer (PCa). In this approach, radioactive seeds (e.g. iodine-125 or palladium-103) are placed (usually 40–100) within the prostate via a transperineal approach. The seeds emit low doses of radiation for weeks or months.
Temporary (high dose rate (HDR)) brachytherapy
In this technique, the radiation dose is delivered over a short period of time. Soft catheters are placed and left in the prostate to act as a conduit for radioactive iridium-192 wires (or caesium-137) for 5–15 min. Generally, one to three brief treatments are given over one to two days in the hospital, and the radioactive substance is removed each time. These treatments are often combined with EBRT.
RT in PCa
The choice of appropriate therapy for PCa is dependent on disease factors (risk stratification) and patient factors (age, co-morbidity, life expectancy, International Prostate Symptom Score (IPSS), urine flow studies and quality of life). Both EBRT and brachytherapy are used in the management of PCa. Main indications of RT for PCa are:
As a primary radical treatment for localised PCa
As a part of the primary radical treatment (with hormone therapy) for locally advanced and or high grade PCa.
Post radical prostatectomy – as a salvage therapy
As palliation in metastatic disease
EBRT in PCa
IMRT, with image-guidance RT (IGRT), is the gold standard for EBRT. There are no published randomised controlled trials (RCTs) comparing RT with watchful waiting or active surveillance. However, the result of one of the arms of the ongoing ProtecT study may help to clarify this issue. The combination of RT and androgen deprivation therapy (ADT) has been shown in multiple clinical trials (see below) to prolong overall survival (OS) in men with high-risk PCa compared with either treatment alone.
Localised and locally advanced PCa
Dose-escalated EBRT is established as an option for localised and locally advanced PCa. For localised PCa, RT is used in various regimens depending of risk stratification (Table 1), although no trial has shown an OS advantage with dose escalation. However, several randomised studies have reported that dose escalation (range 74–80 Gy with conventional fractionation) has a significant impact on five-year survival without biochemical relapse.3–5 These trials have generally included patients from several risk groups, and the use of neoadjuvant/adjuvant ADT has been used with variable regimens.3–5 Currently, a minimum dose of ⩾74 Gy with conventional fractionation is recommended for EBRT±hormone therapy. Recently, data from the CHHiP study has been presented, showing that for intermediate and good risk groups, a hypofractionated schedule of EBRT (delivering 60 Gy in 20 fractions over four weeks) using intensity modulated techniques is non-inferior to conventional fractionation of 74 Gy in 37 fractions, and with no significant differences in toxicity. 6
Recommended external beam radiation therapy for localised prostate cancer (PCa)- adopted from European Association of Urology (EAU) guidelines 2015.
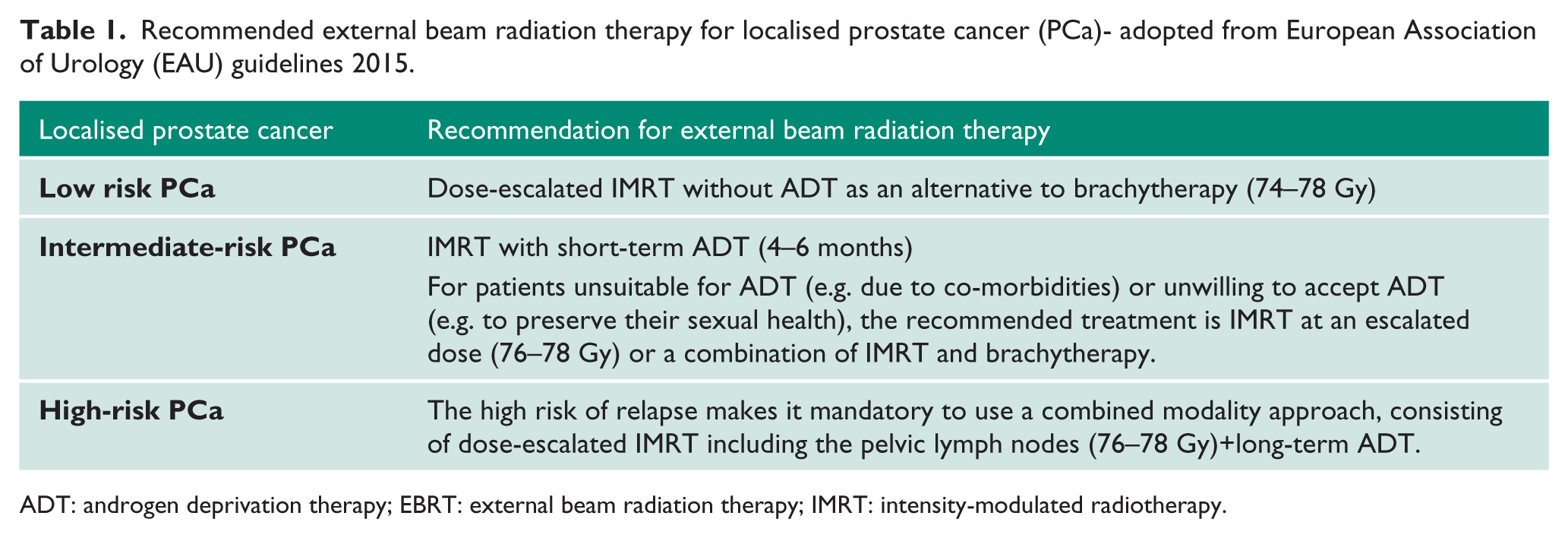
ADT: androgen deprivation therapy; EBRT: external beam radiation therapy; IMRT: intensity-modulated radiotherapy.
Future studies will likely address the issue of radiation dose titration according to risk groups. RT is not without side effects, however, with IMRT/IGRT for dose escalation, severe late side effects (rectal and urinary) are relatively low (2–5%).4,7
The role of EBRT in combination of ADT is well supported by large trials (see below). However, risk stratification plays an important role in determining biochemical failure. The RTOG 94-08 trial compared the combination of EBRT with short-term ADT versus EBRT alone as a treatment for PCa (T1-T2b with prostate-specific antigen (PSA)<20 ng/ml). 8 The results of this trial showed that the combination therapy was superior with improved 10-year disease-specific survival and reduced biochemical recurrence in intermediate and high-risk PCa. However, despite these benefits, 10-year biochemical recurrence in the combination therapy group was still worrisome (28% in intermediate-risk and 31% in high-risk), however the dose of radiation used in this trial (66.6 Gy) would be considered low in the modern era. 8 . For high-risk PCa, long-term ADT is superior as shown by the RTOG 92-02 trial. In this trial high-risk patients (T2c–T4 and PSA<150 ng/ml) were randomised to EBRT combined with either short-term or long-term ADT. Ten-year biochemical failure was 74% in the short-term ADT group and 56% in the long-term ADT group. 9 This high rate of biochemical recurrence is consistent with the possibility of ADT-resistant cell clones within the tumour microenvironment, a hypothesis supported by the positive results for the addition of chemotherapy in the STAMPEDE study in M0 high risk patients. Additionally, the combination of RT with ADT is superior compared with RT alone followed by deferred ADT on relapse, as shown by various phase III randomised trials including EORTC trial 22863.10–12
It is clear from these studies, that ADT improves outcome in intermediate and high risk PCa when added to EBRT. The question of whether adding EBRT to ADT alone in high-risk disease has been answered by two large RCTs (Table 2).13–15
Trials supporting role of combination of radiation therapy (RT) with androgen deprivation therapy (ADT) in locally advanced prostate cancer (PCa).
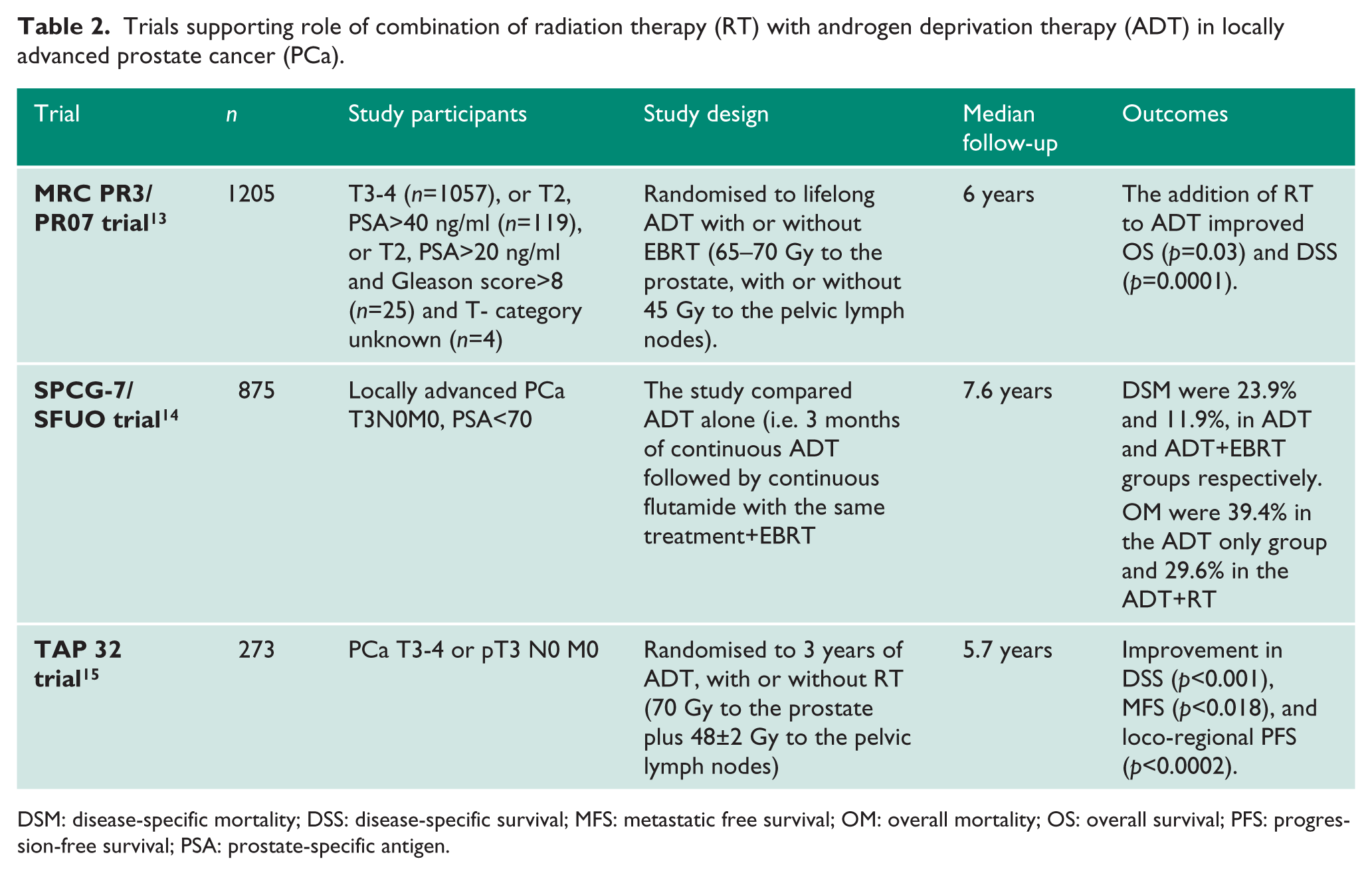
DSM: disease-specific mortality; DSS: disease-specific survival; MFS: metastatic free survival; OM: overall mortality; OS: overall survival; PFS: progression-free survival; PSA: prostate-specific antigen.
RT for pelvic lymph nodes
Prophylactic lymph node EBRT in clinically N0 PCa is controversial, with a large RTOG trial suggesting no benefit over RT to the prostate alone.16,17 However, the data relating to the benefits of RT in high-risk disease allowed for, or mandated, the delivery of whole pelvic RT.9,13,14 Similarly, for clinical or pathological node positive disease, the effectiveness of EBRT as a sole modality is poor. 5 However, combination of EBRT+ADT has shown a statistically significant impact on OS, disease-specific survival, metastatic failure and biochemical recurrence. 18 In addition, the data from STAMPEDE trial suggests that pelvic RT could be beneficial for N1 disease. 19
Adjuvant RT after radical prostatectomy
Patients with pT3 pN0 disease have a high risk of local recurrence after radical prostatectomy. Options in these patients are immediate adjuvant RT to the prostate bed,20,21 or clinical and biochemical monitoring followed by salvage RT if the PSA becomes detectable, and ideally before an increase to 0.5 ng/ml. 22 EORTC 22911 trial 20 compared immediate post-operative RT (60 Gy) with delayed RT (70 Gy) in patients (pT3 pN0). The results of this trial showed that the immediate post-operative RT was well tolerated. In addition, immediate post-operative RT significantly improved the 10-year biochemical progression free survival to 60.6% vs 41.1%. Although clinical progression favoured adjuvant RT after five years but, this trend was not sustained after 10 years. However, loco-regional control was better in the long-term follow-up at 10 years after immediate RT.20,21 Furthermore, adjuvant RT seems to be effective even in the setting of an undetectable PSA after RP. 21
For pN1 PCa, ADT+RT is superior to ADT alone. 23 Abdollah et al. 24 compared lymph node positive prostatectomy patients who received either adjuvant ADT alone or ADT+adjuvant RT. They reported reduced eight-year cancer-specific mortality in ADT+adjuvant RT group (7.6% vs 13.8%). 24
Brachytherapy in prostate cancer
Brachytherapy as a single modality is generally used only in men with early stage low-grade PCa. Other factors such as, prostate size, lower urinary tract symptoms and previous prostate surgeries are to be considered before selecting patients for brachytherapy.
LDR brachytherapy
LDR brachytherapy is a safe and effective technique in low-risk PCa. Following are examples of eligibility criteria for patients suitable for brachytherapy;
Stage cT1b-T2a N0, M0
Gleason score <6 (on an adequate number of random biopsies (minimum 10))
Initial PSA<10 ng/ml
Biopsy cores, <50% involved with cancer
Prostate volume <50 cm3
IPSS <12, and Qmax >10 ml/s
No prior transurethral resection of bladder tumour (TURP)
There is no RCT comparing brachytherapy with other curative treatment modalities for PCa. However, non-randomised studies showed that the brachytherapy improves recurrence-free survival.25,26 Importantly, implant dose plays vital role in determining the effect on recurrence rates. 27 Patients receiving a D90 (dose covering 90% of the prostate volume) of >140 Gy can provide a significantly higher biochemical control rate after four years than patients who received <140 Gy (92% vs 68%). 28
HDR brachytherapy
Non-permanent transperineal interstitial prostate brachytherapy using a high dose rate (iridium-192) can be applied with a total dose of 12–20 Gy in 2–4 fractions, combined with fractionated EBRT of 45 Gy. 29 With HDR brachytherapy, the biochemical free survival is comparable to the high-dose EBRT. 30 A single randomised trial of EBRT vs EBRT+HDR brachytherapy has reported that the EBRT+HDR brachytherapy resulted in a significant improvement in the biochemical recurrence free survival. 31 Additionally, there were no differences in the rates of late toxicity. 31 A systematic review of non-randomised trials has suggested better outcomes with EBRT+HDR brachytherapy than brachytherapy alone. 32 Kupelian et al. reported that for localised T1-2 PCa, the five-year biochemical disease free survival was similar for; permanent seed implantation, high-dose (>72 Gy) EBRT, combination brachytherapy+EBRT, and radical prostatectomy. 30
Proton beam therapy in PCa
Proton beam RT seems to be an attractive alternative to photon-beam RT for PCa, as they deposit almost all of their radiation dose at the end of the particle’s path in contrast to photons, which deposit radiation along their path. Additionally, there is also a very sharp fall-off for proton beams beyond their deposition depth. In theory, this should minimise the side effects. Despite this, for PCa RT, superiority of proton therapy is not well established yet.33,34 There is a lack of RCTs to favour the use of proton beam RT in routine clinical practice. Additionally, the high cost of proton beam therapy is a major limiting factor in its widely acceptability. Currently, two proton beam therapy facilities are being built in UK and will be operational in 2018.
RT in urothelial cancer
RT has come in and out of vogue over a number of decades for the radical treatment of muscle invasive bladder cancer (MIBC). However, its effectiveness in controlling pain and bleeding in palliative patients has long been recognised. In addition, RT as a part of multimodality therapy (combines TURBT, chemotherapy and RT) as an alternative to radical cystectomy has been explored and this approach can be a viable alternative option in selected patients. 35 Similar interest has been shown in using RT in the neo-adjuvant or adjuvant setting but historic series have failed to show any conclusive advantages.
Radical RT for MIBC
For MIBC, the target dose for EBRT is typically 64–66 Gy given over 6–7 weeks or 55 Gy in 20 fractions over four weeks. 36 With the evolution of the RT techniques, late major bladder or bowel complications are low (5%). 37 Several good prognostic factors in those undergoing radical RT include good pre-treatment bladder function, unifocal T2 N0 disease, absence of carcinoma in situ (CIS), absence of hydronephrosis and completeness of initial resection of bladder tumour.38,39 A Cochrane analysis from 2002 combined three trials of preoperative radiotherapy followed by cystectomy with radiotherapy alone, and reported a survival benefit for surgery over RT. 40 This has been widely taken to suggest the superiority of surgery over bladder conservation, however, the studies included in this meta-analysis used a lower dose of RT than would currently be considered standard and did not use concurrent radiosensitisers (e.g. mitomycin C and 5FU, cisplatin or carbogen/nicotinamide) and as such this is not a true reflection of current practice. In the MRC Spare trial, an attempt was made to compare chemoradiotherapy with cystectomy in a randomised fashion in patients with tumours that responded to neoadjuvant chemotherapy, but slow recruitment led to the early closure of this study, and the question of the relative superiority of surgery and bladder conservation in appropriately selected patients remains unanswered.
Overall, five-year survival rates in patients with MIBC range between 30–60%, depending on whether they show a complete response following RT while cancer-specific survival rates are between 20–50%.36,41 Combination of chemotherapy with RT can further improve oncological outcomes. Chung et al. reported complete response in 64% patients after EBRT alone, 79% after concurrent chemotherapy and 52% after neoadjuvant chemotherapy. 39
Multimodality bladder preserving treatment
As stated above, there are no completed randomised controlled trials to compare multimodality treatment to radical cystectomy. However, a recent systematic review and meta-analysis of 31 trials has shown an average five-year survival of 56% with 80% of surviving patients not requiring salvage cystectomy. 42 However, in this trial there is much heterogeneity in the specific treatment profiles and patient characteristics making definitive conclusions difficult to draw. There are two common regimens in use presently. In North America following TURBT, EBRT with concurrent radio-sensitizing drugs in a split dose format with interval cystoscopy is more common whereas in the rest of the world a continuous regimen without interim cystoscopy is typical. Frequently used radio-sensitizing agents include cisplatin or mitomycin C+5-fluorouracil. 43 At present there are two broad indications for multimodality therapy. Firstly, multimodality therapy has been offered as an alternative to RT alone in those unfit for cystectomy. Secondly, it has been offered as an alternative to cystectomy in those who wish to preserve their bladders.
Regarding the function of conserved bladders, there is a report on long-term survivors of trimodality bladder conserving treatment performed at the Massachusetts General Hospital. 44 This study showed that of 32 patients assessed, 24 had normally functioning bladders. However, decrease bladder compliance was noted in seven patients. While, bladder hypersensitivity, involuntary detrusor contractions and incontinence were present in two patients. Overall, global health-related quality of life was high with bladder preservation in these patients.
Pre- and post-cystectomy RT for MIBC
Several old studies looking at pre-cystectomy RT have shown improved outcomes, however these studies have large limitations and it is difficult to draw firm conclusions. 45 In the National Cancer Institute, Egypt, post-cystectomy adjuvant RT is standard treatment for pT2b-4a urothelial cancer. 46 A RCT conducted in this centre has shown near equal oncological outcomes between pre-operative and post-operative RT. 46 However, this study is not directly applicable to Western practice due to the much higher rate of squamous cell carcinoma encountered (46%) among patients in the Egyptian study. Furthermore, 83% of the transitional cell carcinomas (TCCs) in the trial were low grade which is a significantly higher proportion than that typically encountered in the West. 47 European Association of Urology (EAU) guidelines have concluded that whilst pre-operative RT has been shown to down-stage disease after 4–6 weeks, there is no evidence to support improved survival when pre-operative RT is used in the treatment of MIBC.
RT for upper tract urothelial cancer
No role has been demonstrated for RT as a monotherapy for upper tract urothelial carcinoma, however there has been some evidence to suggest its benefit in the adjuvant setting. Most of the studies are old and determining the exact treatment technique can be difficult retrospectively. Typical regimens seemed to involve 40–50 Gy being given in 1.5–2 Gy fractions. Adjuvant RT failed to provide improved OS for all patients with upper tract urothelial tumour. However, for patients with T3/4 disease OS improvement is reported. 48 There has also been interest in giving adjuvant combined chemo-radiotherapy in high-risk patients. A study at Massachusetts General Hospital, displayed improved disease-specific survival when cisplatin was given concurrently to EBRT. 49 However, no current guidelines support the role of RT in upper tract urethelial cancer in the adjuvant setting or otherwise.
RT in testicular cancer
Testicular intraepithelial neoplasia (TIN)
TIN is a progenitor of germ cell tumours. TIN is found in about 4–8% of contralateral testes in patients with unilateral germ cell tumours. 50 Without treatment, TIN will progress to invasive cancer in 50% of cases within five years and likely all of the cases will do so in the long term. 51 Treatment options encompass orchiectomy, local RT of the testis or surveillance. 52 Local RT is highly efficacious in curing TIN. 53 Though hypogonadism occurs in about one-third of patients, RT (20 Gy in 10 fractions) remains the standard form of management of TIN. 54 Patient should be counselled about impaired testosterone production and infertility.
Stage I seminoma
About 15–20% of stage I seminoma patients have subclinical metastatic disease, and will relapse in the retroperitoneum after radical orchidectomy. Seminoma cells are radiosensitive and adjuvant RT reduces relapse rates to <5%. In the past, adjuvant RT to the para-aortic strip or to a ‘dog-leg’ volume had been standard treatment for stage I seminoma. However, surveillance and adjuvant chemotherapy have been shown to give similar results with a five-year disease-specific survival of 99% due to the high chance of salvage in relapsing patients. It has been recognised that RT is associated with increased side effects including cardiovascular disease and secondary malignancies.55,56 Hence, it is recommended that in young patients (<40 years) adjuvant RT should no longer be used, and in practice adjuvant radiotherapy is rarely used now at any age.
Stage II seminoma
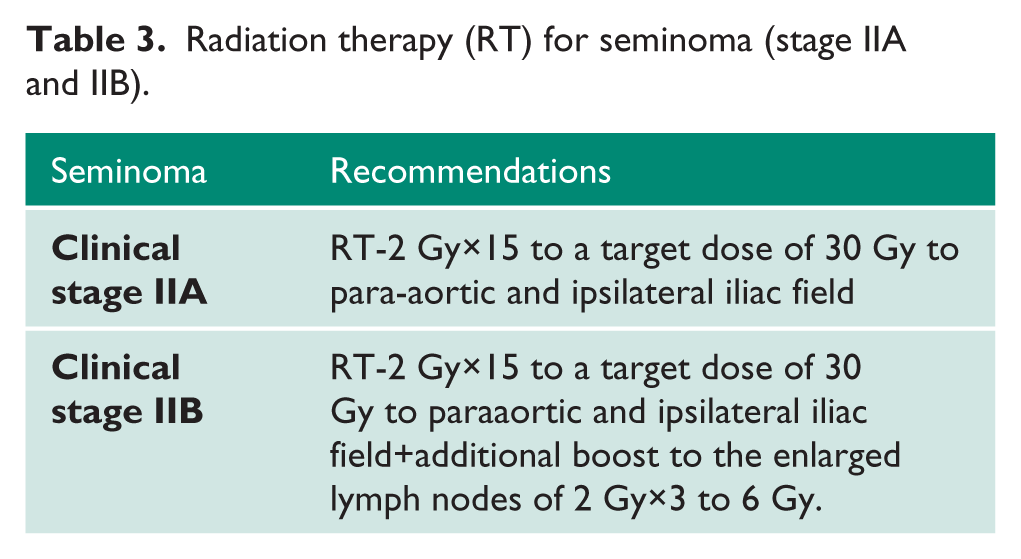
In stage II seminoma, the volume of retroperitoneal disease predicts recurrence rates. In patients treated with RT, the five-year relapse-free rate was 91% in stage IIA/IIB disease compared to 44% in stage IIC disease. RT protocol is different between IIA and IIB seminoma (Table 3). In stage II seminoma, RT includes the gross tumour volume along with the para-aortic and ipsilateral common and external iliac lymph nodes. 57 An alternative approach for stage IIA/B seminoma follows the Royal Marsden Hospital trial of using a single dose of carboplatin (at a dose that results in an area under the curve (AUC) for concentration time of 7 mg/ml) followed by para-aortic nodal RT. 58
Radiation therapy (RT) for seminoma (stage IIA and IIB).
RT in penile cancer
Organ-preserving surgery is the preferred surgical option for penile lesions not involving the urethra. However, RT of the primary tumour is an alternative organ preserving approach for T1-T2 lesions <4 cm in diameter, particularly in surgically unfit patients. RT is not routinely indicated for treatment of nodal disease in penile cancer.
The best results are achieved with brachytherapy with local control rates ranging from 70–90%.59,60 With brachytherapy, no significance deterioration of urinary symptoms and erectile function is reported. 61 For penile cancer, a dose of 60 Gy of EBRT is optimal, combined with a brachytherapy boost or brachytherapy alone.59,60 Penile brachytherapy provide good tumour control rates, acceptable morbidity and functional organ preservation for T1 and T2 penile cancers. 62 Local failure rates are higher with RT compared to partial penectomy, however salvage therapy (e.g. surgery) is still possible in patient who develop recurrence after RT. Patients’ receiving RT for penile cancer should be warned of potential adverse effects. The most common complications include urethral stenosis (20–35%), glans necrosis (10–20%) and late fibrosis of the corpora cavernosa. Radiation to the penile shaft can cause erectile dysfunction. However, in cases where the tumour is confined to the glans, radiation is directed only at the tumour, hence erection is less likely to be compromised. In many cases, the function and appearance of the penis gradually return to normal in the months and years after RT.
RT in renal cell carcinoma (RCC)
RCC is traditionally considered to be a radio-resistant tumour. However, in recent years SBRT has emerged as an important modality in the management of RCC, both in primary settings and in treatment of solitary metastatic disease. 63 In addition, the positive effect might be enhanced when targeted drugs and SBRT are combined. 63 However larger series, randomised trials and long term results are needed to consolidate these initial findings.
Palliative RT in urological cancers
Symptomatic bone metastatic lesions from urological cancer are effectively treated with RT. A single fraction of radiation using a dose of 8 Gy can provide palliation for relief of pain from bone metastases.64,65 Additionally, the single fraction improves patient convenience and was found to be more cost effective compared with fractionated schedules. 65 However, the retreatment rate and pathological fracture rates were higher after single fraction RT. 66
Radiopharmaceuticals are drugs that contain radioactive materials called radioisotopes. These agents emit radiation, mostly in the form of α and β particles that have tumourcidal effect. Strontium 89 treatment has been reported to be effective in ameliorating bone pain associated with metastasis from PCa. 67 In a randomised controlled trial (ALSYMPCA), radium 223 has been shown to result in an overall survival benefit and reduced skeletal-related events when compared with placebo in patients with castration-resistant metastatic PCa with predominantly bony disease (and no visceral metastases). 68
Palliative EBRT is a well-established option for non-resectable bladder tumours. It is effective in controlling haematuria in 59% of patients and control of pain in 73%. 69 Similarly, SBRT is associated with excellent local control and low rates of toxicity for intracranial and extracranial metastatic RCC. 70
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
SA.
Contributorship
SA, PZ and WG researched the literature and wrote the first draft of the manuscript. JR conceived the study and edited the manuscript. GM researched the literature and edited the draft. All authors reviewed and approved the final version of the manuscript.